
Abstract
While the limits of rational-calculative approaches for healthcare decision-making, alongside institutional forms of ritual, routines and hope employed to deal with these limits, were already described in the 1950s, healthcare professionals’ syncretism of rational and non-rational approaches in their everyday work remains a neglected topic in Northern Europe. Using COVID-19 as an urgent problem for healthcare policy and practice, and a natural ‘breaching experiment’ which disrupts everyday work in ways which help professionals to critically reflect, this article explores how a small, purposive sample of young healthcare professionals in the Netherlands dealt with the uncertainties and risks posed by continued healthcare work amid the pandemic. Analysing qualitative data, collected via longitudinal online interviews among healthcare professionals, the analysis pays particular attention to: concerns, anxieties and risks faced by professionals; understandings and ways of working with(out) protocols; different logics for handling uncertainty in different situations; how different logics (rational, non-rational and ‘in between’ rationalities) are combined in different aspects of their work. A key feature of the analysis is the tensions which emerged within these combined strategies and how these relate to broader tensions in terms of the limits of rationality, economic scarcity, work-life experiences, and evidence versus emotions.
Introduction
Despite an important tradition which has challenged assumptions regarding the rationality of clinical practices (Fox, 2000; Roth, 1957), recent social science approaches to analysing healthcare practices amid uncertainty have often tended to become warped and constrained by a number of unhelpful and simplistic binary assumptions (Derrida, 1976). While anthropologies of health, care and medicines use in the Global South have emphasised the importance of ritual and magical thinking, studies in the Global North have tended to focus on and critique the bureaucratic rationalisation of modern medicine, thus perpetuating a modern-rational versus traditional-magical binary which precludes an attentiveness to rituals, for example, in Northern European healthcare contexts (see Moore, 2020). Where less than rational approaches have been studied, behavioural economics and psychology studies have tended to focus on patients, in contrast to the ‘rational experts’. These approaches sit alongside an attentiveness to the vulnerability of patients, while the vulnerability of the professionals is often neglected within fields of study which have traditionally emphasised their power and authority (see Warner, 2006, for one important exception).
As we will sketch out in the next section, these binaries have been contested in important ways in some classic (e.g. Roth, 1957) and more recent work (Alaszewski, 2015; Horlick-Jones et al., 2007; Zinn, 2016). Some of these assumptions have also been uprooted amid recent media coverage of healthcare work amid the pandemic, creating a natural breaching experiment (Garfinkel, 1967) which helps professionals reflect more critically on how they, and those around them, practise their everyday work. The risks and vulnerabilities faced by (quasi-) professional hospital and care home staff have been highlighted through publication of the numbers and narratives of those who have died from COVID-19. In the Netherlands, as of 9 June 2020, 16,973 health and social care professionals had been diagnosed with the virus with 529 hospitalised and 11 (aged between 45 and 69) having died (Het Parool, 2020).
As with the approach to the pandemic in everyday life more generally, COVID-19 risk governance in Dutch hospitals has been largely shaped by the National Institute for Public Health and Environment (RIVM). Framing government policy in terms of a scientific and evidence-based approach, the Dutch government has largely presented itself as deferring to this expert institution alongside emphasising a wider cultural repertoire appealing to ‘level-headedness’ and shunning ‘symbolic measures’ (Brown, 2020: 5). In ‘following the science’, the centre-right cabinet has, of course, made political decisions in terms of which science, and which expert institutions, to heed. The Netherlands has thus not followed the World Health Organization (WHO) recommendations of extensive testing, tracing and isolation. Instead, between 12 and 23 March 2020 there was a gradual increase in measures, from encouraging people to work from, and stay, home, to closing restaurants, bars and hotels, to cancelling all meetings for education and other events. Although, in a speech on 16 March Prime Minister Rutte referred to ‘herd immunity’, within a week the rhetoric had shifted to an ‘intelligent lockdown’, whereby: . . . people were urged to leave their homes as little as possible and work from home. Furthermore bars, restaurants, schools, gyms and ‘contact professions’ were closed and visiting people in nursing homes was not allowed. Even though people were urged to stay home, they were still allowed to move around freely as long as they kept a distance of 1.5 m to others. This instruction was strictly enforced (within the limits of available police forces) and offenders were fined 390€. (de Haas et al., 2020: 1)
Alongside these public health measures, health services policy focused on building intensive care unit (ICU) capacity across the country, with other non-urgent forms of hospital care being scaled down significantly. The combined policies appeared to have been successful in that ICUs were not overwhelmed; however, as Wallenburg et al. (2020: 1) note, ‘[b]y mid-April, it became clear that the strong focus on hospitals had drawn attention away from nursing homes that now faced a sharp increase in death-rates’. Complaints of limited access to protective equipment were common. Overall, deaths officially recorded as COVID-19 related reached a peak on 2 April, falling steadily afterwards. Schools, alongside various other public facilities, partially reopened from 11 May.
Within this context we explore how a small, purposive sample of healthcare professionals (N = 6) working in hospitals in the Netherlands experienced and adapted to uncertainty in their everyday work. We do this by analysing qualitative data collected from 21 in-depth interviews collected at three or four time points with each participant, between April and early June 2020. These data thus provide important insights into how uncertainties and risks pertaining to the SARS-CoV-2 virus, and the COVID-19 disease which results from this virus, were handled. The interruption of medicine-as-usual also means these data provide us with a more reflexive set of considerations into the nature of medical practice and how professionals handle uncertainty within this.
Conceptualising how professionals experience and handle uncertainty
From her early research in the 1950s, Renée Fox has emphasised the centrality of uncertainty to medical work, as well as the ‘social, cultural, emotional, and moral and spiritual meaning of uncertainty for professionals’ and professional groups (Fox, 2000: 410). Fox’s classic study, of how medical students and trainees were socialised into handling medical uncertainty, notes various ways in which uncertainty is encountered – from gradually establishing whether the uncertainties trainees face are related to the early stage of their career, personal limitations, or those pertaining to the field, doctors also must come to grapple with ‘critical problems of meaning, and “ponderably imponderable” questions about the “whys” and the mysteries of life and death that are at once integral to medicine and that transcend it’ (Fox, 2000: 410). In this sense medicine is as much craft as science, whereby good care-giving requires ‘reflective awareness of physicians’ structural and symbolic power, and is displayed as discerning, empowering improvisations in critical situations, based on empathy and willingness to learn from patients’ (Schei, 2006: 393).
Fox, alongside contemporaries such as Donald Light (1979), observed several different and complementary ways of coping with the various unknowns/unknowables. These ranged from more intellectual-rational approaches such as probabilistic understandings, diagnostic techniques and the use of experience, judgement and a personal philosophy in developing prognoses and treatment strategies, to a gradual process of emotional detachment and cognitive bracketing away of uncertainty, and then the use of particular configurations of dark and ironic humour (Fox, 2000: 411; Light, 1979).
These understandings emphasise the collective, socialised and ritual form of these coping strategies (see also Douglas, 1966, 1992), with Fox quoting her colleague and mentor Parsons in acknowledging the ‘ritualised optimism’ or hope inherent to modern American medicine (see also Good, 2001). Whereas Parsons considered that the ‘scientific tradition of modern medicine “may preclude outright magic”’ (Fox, 2000: 410), another sociologist of the 1950s went further to argue that, in the handling of contagion (tubercle bacilli) in the American hospital where he did his ethnographic fieldwork, uncertainty was often handled through ritualised formats of ‘irrational practices that can properly be called “magic”’ (Roth, 1957: 310). This could most visibly be observed in the inconsistent use of facemasks.
The question of why an attentiveness to magical and non-rational practices in handling uncertainty largely (if not entirely) disappeared from medical sociology for the half century after Fox’s and Roth’s key works is beyond the scope of this article. The binary-thinking briefly sketched in the Introduction arguably provides at least part of the answer. But more recent work at the meeting points of medical social sociology, anthropology and the sociology of risk and uncertainty have begun to re-emphasise the role of rituals (Armstrong-Hough, 2015; Burgess and Horii, 2012; Lohm et al., 2020; Moore, 2020), hope (Baldwin, 2019; Brown and Flores, 2011; Good, 2001), and a much wider range of ‘logics’ (Mol, 2002: 91; Zinn, 2016) by which professionals handle uncertainty.
Some of this work reflects longer running considerations of how people in everyday life handle uncertainty amid a late- or reflexive-modernity characterised by the uprooting of traditions, the questioning of knowledge and expertise, and a heightened awareness of human-made risks (Giddens, 1990). Building on this important base, more recent work has made especially striking contributions in terms of challenging the lay–expert divide (Wynne, 1996) and acknowledging the similarities in how patients and professionals handle uncertainty (Zinn, 2016), exploring how these approaches tend to pragmatically combine multiple different logics (Horlick-Jones et al., 2007; Zinn, 2016), and emphasising that most approaches to uncertainty combine rational with non-rational or ritual features (Alaszewski, 2015).
There is much less empirical work on how professionals cope with serious upheavals of their working conditions, such as those changes brought about by pandemics. Studies which do exist (e.g. Chan et al., 2016, on the impact of the SARS epidemic on healthcare professionals) tend to be more psychiatric in nature, using quantitative survey data to describe higher levels of fear, anxiety, mistrust and damaging effects on intimate and family relations. Studies of fateful moments and biographical disruption following Giddens (1990) and Bury (1982) among patients and wider populations also emphasise the coping which emerges over time, such as through rebuilding routines (Giddens, 1990), narratives and reworking roles in social networks (Bury, 1982).
In emphasising commonalities between how people in everyday life, and experts in their everyday work, cope with uncertainty and vulnerability, Zinn (2016) provides a number of useful insights which help us go further to explore specific ways in which rational and non-rational strategies are syncretised. Zinn also draws our attention to the centrality of strategies such as emotions, heuristics (rules of thumb) and trust which he sees as combining rational and non-rational elements (see also Möllering, 2001: 410). Emotions, as with many of these logics for ‘heading into the unknown’, form a response to vulnerability and uncertainty but, moreover, a way of negotiating and continuing forward amid these conditions (Zinn, 2016). More recent work on how professionals handle risk and uncertainty following Zinn’s (2016) emphasis on multiple strategies also emphasise the common experience of tensions resulting from organisational approaches to risk (Brown and Gale, 2018). In the analysis below we explore various ways in which experiences of vulnerability and uncertainty amid COVID-19, and ways of coping and making decisions, relate to one another. But first we outline the study itself.
Methodology
We used a short-term longitudinal research design using interviews and a participant-generated photo-voice approach (Henwood, 2019). Data were collected between April and early June 2020 in the Netherlands. Participants were purposefully recruited through the social network of the first author, both through word of mouth and by distributing the information letter in various hospitals in the Netherlands. Recruitment was challenging, due to the pressure that healthcare professionals were experiencing, as well as the longitudinal design which required a greater commitment from participants. Each of the six participants was interviewed fortnightly three or four times. In total, 21 semi-structured interviews were carried out, lasting between 15 minutes and 1 hour (mean duration = 43 minutes).
Interviews were conducted online to make sure no risk was posed to interviewer and interviewees at time of the SARS-CoV-2 virus outbreak. We have used pseudonyms to protect the privacy of respondents. Five participants worked at different regional hospitals, while Maaike worked at a nursing home. The participants are briefly described in Table 1.
Participant characteristics.
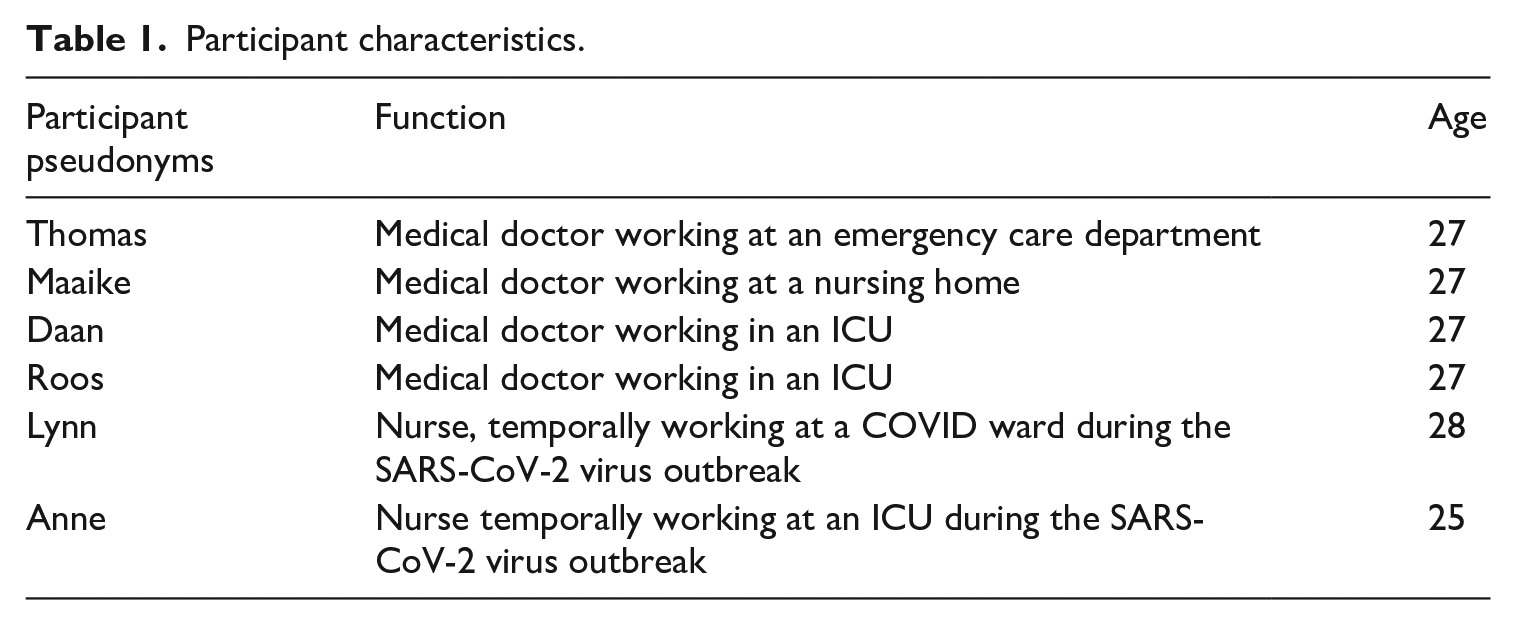
The interviews explored experiences of these young physicians and nurses providing care at the time of the SARS-CoV-2 outbreak in the Netherlands. All interviews started with open-ended questions about daily work. The disruptions to their clinical routines due to COVID-19 was immediately mentioned by all participants, becoming important themes. In the interviews, attention was focused on care practices and the uncertainties healthcare professionals faced. Approaches to handling these uncertainties were specifically enquired into. Participants were asked to take photographs of different aspects in their work – of course protecting the privacy of patients and other colleagues. These photographs provided insight into the (material) context at hospitals and were considered especially helpful in stimulating the exploration of participants’ (new) routines in the interviews (Henwood, 2019). The interviews were recorded and transcribed in full, following the consent given by each participant. The research was carried out within the research ethics framework of the Medical Anthropology and Sociology graduate study programme at the University of Amsterdam.
The interviews were carried out in Dutch by the first author, who is also a medical doctor. On the one hand this provided familiarity with the context and resulted in open interviews, by which participants felt safer among ‘one of their own’. On the other hand, this familiarity could also result in assumptions about the experiences of the participants which were self-evident, or where professionals felt they had to prove themselves or their clinical knowledge (Bourdieu, 1999: 611, 613). These power dynamics and their shaping of interview narratives were discussed and critically considered as part of the analysis process, and brought in at each of the three stages of qualitative thematic coding – open, axial and selective. Aided by the use of AtlasTi, in the axial coding phase emerging themes were compared chronologically and across participants. In the selective coding phase, the relation between themes were further scrutinised, paying particular attention to changes over time for specific participants. Below we show quotations which have been chosen to capture the most common themes emerging in the analysis as well as the themes which appeared to be most salient to grasping the changing experiences of healthcare professionals across the two-month period of the interviews. While the photos gave important insights which facilitated the interviews, and enabled greater insight into the materiality of the participants’ work in the absence (and impossibility) of observations, we do not include these data here. The photos are discussed in more detail in another publication and are not shared here to respect the participants’ privacy.
Findings
The imposition of uncertainty and change over time
The initial interviews took place in early April. This was two to three weeks after the start of the ‘intelligent lockdown’ and around the time of the peak mortality in the Netherlands on 2 April. At this point in time, participants shared two main common concerns: firstly regarding the total level of infections and whether hospitals had sufficient capacity (beds and staff), and secondly regarding their own approaches to providing care while ensuring infection control and not contracting the virus.
Uncertainties over hospitalisation rates and ICU capacity
It is important to note that the timing of the pandemic’s impact varied across the different Dutch regions in which the participants worked. While the virus was much more widespread, and spread much earlier, in the southern province of Brabant, the northernmost province of Groningen continued to experience low rates of infections, partly by complementing Dutch government and RIVM guidelines with a local public health approach which was much closer to the test, trace and isolate approach of the WHO. Yet participants’ concerns appeared to transcend these regional variations, with a doctor in Groningen stating: But the uncertainty also relates to this, in how far it [the virus] will spread around here [province of Groningen]. And how great the outbreak will be. And can the Netherlands manage with its [limited number of] intensive care beds. And I think that was really nerve wracking. And if you have that uncertainty, yeah, uncertainty over how it would spread. But as time passes, then you have a better idea of how severe things will get. And uncertainty too over how the illness develops, how it plays out [in individual prognoses]. I think things were so new, people hadn’t got their heads around it – a few weeks back. (Daan, early April)
That these concerns transcended local characteristics may, especially in relation to ICU capacity, have been a reflection of national media preoccupations which, in turn, were shaped by reporting from regions elsewhere in Europe (around Bergamo, Italy, for example), where services had been overwhelmed. In this sense these worries reflected concerns expressed by many in wider society and appear to be as much driven by media reporting as by first-hand observations. However, these potentially negative futures were described by participants as likely to impact on them far more directly: Because, for me, it was more anxiety about what was coming and whether we [as an organisation] could cope. Would it become total chaos with patients lying in the wards and in the corridors? In the end it wasn’t even that bad. We did not have to work so hard and the things we saw were not so intense. (Roos, early May)
Managing risk of infection for oneself
Alongside the pressures of being overwhelmed by caring for sick others, a further important source of anxiety was risk to self through infection, particularly in terms of how best to follow protocols while using protective equipment which, at least earlier on, was in short supply: . . . imagine that you have a [care home] patient who has it [COVID-19]. I have come in [to the patient room]. It is quite a faff to do this in a good way, to ensure you don’t touch anything; to be careful to hang back and keep your distance. And then to put everything on without touching the outside [of the garments]. Then you just look forward to just taking everything off, [putting it] in one bag and then you’re done. Then you feel a bit safer. I don’t know, maybe that is just a feeling, you know. But that’s how I find it, I would rather things were different. Anyway, that’s not the way it is, because we just don’t have enough equipment. (Maaike, early April)
For this doctor based in a care home, the concerns of treating people who were sick (and thus infectious) with COVID-19 were not only the difficulty of giving care while wearing appropriate protective equipment and trying to keep one’s distance, but also in having to ‘recycle’ the same equipment throughout the day. Similarly, hospital-based Thomas had taken a photo of a washing line of facemasks to characterise his daily experiences. As he described further in the next interview: The issue with these facemasks, for example . . . until last week it was the agreement, due to the scarcity . . . that doctors and nurses would use one each per day. And then, it’s like we have a long washing line with hooks where you can hang up your mask, separately from those of others. (Thomas, early April)
The rationing of personal protective equipment (PPE) was a source of uncertainty in at least two important senses. Firstly, as we saw in the first of these two quotations above, professionals worried and felt unsure about their safety. Secondly, as we see briefly here but which we will return to in a later section, the impossibility of using PPE in a rational-calculative manner – in terms of what was safe according to the evidence-base – raised uncertainties of how, then, PPE should best be used.
Worries changing over time
In the later interviews among our small cohort, worries had shifted noticeably. As the numbers of infections, hospital admissions and fatalities gradually shrunk throughout April and into May, so did capacity cease to be a concern for people. Once more, driven by experiences elsewhere and as reported in the media, the growing concern and uncertainty related to the potential for a second wave and when this would arrive.
So it seems to me that things have got calmer again, There are also fewer junior doctors who have been assigned to us. And that is good as there is just one ICU again. The supplementary [COVID-ICU] is closed, so you don’t need personnel there anymore either. But yeah, the question remains of course, will there be a second wave? And when will it arrive? Will it come in a couple of weeks after the [lockdown distancing] measures are relaxed? (Daan, mid-April)
For Anne, an ICU nurse, during her interview in early May she described having less uncertainty over whether a second wave would come, the uncertainty remained however as to when.
Everyone concerns themselves with whether there will be a second wave. Everyone where I work says they’re convinced that there will be a second wave. But the question is when? And everyone is concerned about that. But it’s far from an all consuming topic. (Anne, early May)
This last quote reflects a wider tendency across the small cohort and the changing nature of the interviews over the research period. The foci and core preoccupations gradually shifted as the initial concerns around overwhelmed hospitals faded. Meanwhile discussions of anxiety and worry gradually eased in a more general sense, as the participants appeared to adjust and cope more effectively, and/or where supplies of PPE improved over time. We turn to various forms of coping with uncertainty in the next section.
Different forms of coping, more or less awkwardly . . .
Coping with uncertainty regarding a second peak
As noted in the previous section, the main uncertainty and source of worry stated in the earlier interviews with the participants was that of hospitals, particularly ICUs, becoming overwhelmed by acutely ill patients. Gradually, as noted already, these worries were allayed by empirical evidence; what these professionals saw with their eyes. But in many instances these understandings of the present were also projected into the future, based on ‘trust’ or ‘confidence’ (Luhmann, 1988) in the organisational infrastructure within which they worked.
Yes, I found [all those thoughts and questions regarding not knowing what to expect] very nerve wracking. I noticed that that brought a lot of nervous tension with it. But these days that [feeling] has reduced, right. We see that things are gradually improving and returning to normal. [Fewer] new admissions. And because somewhere I have trust that we have this really well organised. We are ready for it. And so it is not that I could come to work and that everything just descends into chaos. (Roos, mid-April)
This perspective, partly driven by having seen that things had gone better than feared with the first main peak, also appeared to gradually allay the concerns noted above regarding a second peak. Again, this appeared to gradually take place over time. In one of the last interviews: MvdM: Yeah, and you said the second peak is going to happen anyway, but we don’t really know yet how big it would be. And the uncertainty around that, what does that do to you? Is that a tricky topic [for you]? Daan: Well not very much. I think, I think we already know it, we know what to do I think. Yes, maybe I think it should be a little peak. I don’t worry much about that. (Daan, end of May)
Another coping strategy (Zinn, 2016) for the uncertainty regarding a second wave was hope – which we see implicitly above in Daan’s tentative expectations for a small second peak. Some participants referred to hopes that the Dutch population more generally would be better prepared in terms of hand washing, distancing and so on and that this would help ‘flatten’ a second peak. Others, meanwhile, focused their hopes on a return to normal hours, with this hope, in turn, founded on a tentative hope that there would not be a second peak: I really want to know whether there will be a second peak. I hope not . . . I hope we can go back to normal working hours. Yeah, I think that mostly, normal working hours. But you don’t know [what will happen] right. (Roos, mid-April)
But these hopes related to clinical futures, as we see here, were often fragile. Such fragile hopes were expressed alongside participants’ hopes, and disappointments, for their lives more generally: You can do so little, you can barely sit outside a bar or all those normal things, yeah. Also, at the beginning, you hoped that things would very quickly pass, but now it is clear things are going to last a lot longer, and that there are going to be no ‘events’ [festivals, etc.] and that makes your outlook a bit dull. (Maaike, early May)
Early hopes that life would return to normal were thus disappointed, with a realisation that life would remain rather ‘dull’ for the foreseeable future. As time went on, participants referred to modest ways in which they coped with this part of the wider COVID-19 experiences, with small aspects of their social and family lives returning more to normal: I am more inclined to go outside, and I am less strict about the 1.5 distancing. I have visited my parents again. My parents have no health problems whatsoever, they are really healthy and 60 [years old]. But still, in the beginning I felt a bit awkward about it and now less so. Which I don’t think is a good thing I am doing. Because I think more people in the Netherlands are acting like this and therefore we can expect a second wave, and I am part of all this. (Lynn, early May)
In this sense forms of coping with everyday life outside of work also heightened some of the concerns about a second peak. Tensions thus became apparent in the coping narratives of these professionals, not least between how they felt and coped with their clinical work and how they handled uncertainty in their lives outside the hospital. As we will see below, tensions were an important feature of coping narratives.
Coping with uncertainty around infection control
As noted in the first findings section, the other main concern expressed by participants, especially in earlier interviews, was that regarding infection control. As apparent in the excerpts below, uncertainties around this topic related to the uncertainty of being infected, as well as the uncertainty and frequent adjustments on policies on protocols around PPE: MvdM: And what do you think about this [changed policy with regard to lower quality face masks]? How’s that been for you? Thomas: Yes it is [about] adjusting. But on the other hand I find it, like, it makes sense and it is understandable that it has been this way. You just don’t know how it [really] is. Uhm, that we now still have to find out a bit how the virus works and [how it] doesn’t work. And I am not surprised that the guidelines change so often. (Thomas, early April)
But in the same interview Thomas also expressed doubts regarding infection control protocols because of the scarcity of materials.
Because things change every day . . . for example the story of those face masks and that now lower quality ones are also sufficient, I think that is an admission of weakness. And, you know, if there was no scarcity, they would have just said wear an FFP2 [high quality mask]. It feels like [they say] a lesser degree of protection is also sufficient because they don’t have them. And then I think, a bit, I have questions whether that is correct. And not only me, other people too. (Thomas, early April)
While we saw above that some participants expressed trust in the organisation in terms of its capacity to handle patients with COVID-19, especially were a second peak to develop, this is not to say that there were no questions or concerns regarding the handling of all aspects of healthcare delivery – not least due to the incoherence of infection control policy, as forced by mask shortages, for example. But despite these doubts as expressed in the preceding quote, this same participant appeared to continue to trust. When interviewed several weeks later, this time regarding the stopping of the requirement of covering their hair, this professional asserted: I only know that, for us, at a particular moment the decision was made not to [wear hairnets] any more. And indeed I followed this [new protocol]. [The way I] think about it, ‘ok, someone must have done a study and decided that it wasn’t necessary, and I assume that if it was a possible means of infection, then we would have hairnets. So I take it that it has been well looked into [researched], and that it evidently isn’t a big risk not to have a hairnet. (Thomas, end of May).
In spite of earlier doubts, and concerns that protocols were at least partially driven by what PPE was available, rather than what evidence was available, here the same participant describes ‘assuming’ that the decision around hairnets was evidence based. But seemingly there remained a small level of doubt, implicit in the way this narrative is presented.
As noted in the wider conceptual (Möllering, 2001) and empirical literatures (Brown, 2009), trust has often been found to be experienced as awkward, whereby uncertainty was bracketed off in a partial and pragmatic manner: I think that you just don’t have the time not to trust, and to go and check up on things. (Daan, mid-April)
Indeed, despite Thomas referring to his ‘assuming’ that hairnets were stopped on evidence-based grounds, as he said in the same interview: . . . it is still not one hundred per cent sure if it helps to wear a hairnet or not. (Thomas, end of May)
We explore these tensions and pragmatic forms of coping further in the following section.
The development of routines, rituals and their inherent tensions over time
We have shown above that infection control was one the key foci of uncertainty and vulnerability that participants encountered in their day-to-day work. Protocols for the wearing and use of clothing and PPE were a core way in which these risks and uncertainties were handled, though we have noted various tensions in the forming of these everyday policies. In this section we now move to explore the embodied practices of infection control in more depth, not least their symbolic, spatial and affective dynamics and tensions.
Accounts from different hospitals described a fairly common policy by which non-ICU wards were divided into ‘clean’ and ‘dirty’ sections, with possible SARS-CoV-2 and COVID-19 cases being cared for in the latter. Corona ICUs became locked wards, wherein the rooms themselves were understood as ‘dirty’ while the corridors were ‘clean’. Patients were not taken along corridors to shower or use the toilet in order to maintain these ‘clean’ spaces.
Lynn described the everyday working protocols in her Corona ward and how, in front of each room: . . . on the left side, [you have] the dirty side, and on the righthand side the clean side. On the clean side you put your clothes on. There are the clean things so you didn’t touch anything there if you had touched anything with Corona. So there you took your suit, your gloves, your facemask, your [protective] glasses. And there you had to place your glasses once you had scrubbed them clean. And then on the other [dirty] side you took your suit off. There you had to put your used apron, your surgical mask, so it could all be [cleaned and] reused. And you have a white tray hanging there. You put your glasses in there. (Lynn, early June)
Lynn went on to explain how the clarity and consistency of these systematised routines and boundary-making, or rituals, in relation to dirt (Douglas, 1966) ‘ensured the safety’ of her and her colleagues. She contrasted her ‘well organised’ ward with another ward where many professionals had tested positive for SARS-CoV-2 and got sick: And on that other ward, where everything went wrong, there they just didn’t follow [the safety protocols]. There the dirty and clean got mixed up. Then it went wrong. And now, [on my ward] I can just say ‘this is clean and this is dirty’. I found it very clear and good. So there I felt safe as an employee. So I really like that.
While Lynn described feeling reassured by the stringent following of protocols and demarcation of spaces, at least on her COVID-19 ward, another nurse, Anne, also temporarily working on a different ward (COVID-19-ICU), referred to the less consistent following of protocols – either due to people forgetting, especially when they were busy, or due to the sheer impossibilities of following requirements, due to space: You can of course say that people need to keep 1.5 metres from each other when working but that’s just not possible. The team office is just not big enough. So they may have these nice plans but they simply don’t work. So, in the beginning, in the first weeks, people tried to take [the 1.5 metre protocol] into account but in the hospital, really everyone occasionally walks [closer] past someone else. It can’t be otherwise. (Anne, end of May)
So despite some accounts that asserted that strictly following the protocols gave a sense of safety and reassurance, all six participants referred to various ways in which they themselves, or others, bent the rules – either in the hospital or in their social contacts outside of work (similar to Roth, 1957).
Such accounts of becoming more pragmatic with protocols became more common as the weeks went by. Lynn, who we quoted above as describing the importance of strict adherence to protocols in the workplace, was the same participant who we earlier quoted as describing how she gradually started visiting her parents. She went on to rationalise this in more scientific terms, invoking understandings of aerosol dispersal: I also think that, if someone doesn’t cough, or sneeze next to me . . . then I don’t think that the 1.5 metre [public health rule in the Netherlands] is going to do anything. Then it doesn’t matter whether that person is 1.5 metres or 30 centimetres away from me, because it [the coronavirus] travels through aerosols but if you don’t sneeze, cough or have a runny nose, then these [dangerous] aerosols won’t come to me. (Lynn, early June)
In this excerpt we see Lynn grappling with awkward tensions emerging within and between her accounts of her following protocol in the hospital versus her behaviour outside. She appealed to rational-scientific accounts to rationalise her safety practices but the tensions endure – not least because by early June it was commonly understood that the virus could be spread by non-symptomatic carriers.
Alongside these tensions amid attempts to rationalise, participants also provided insights into tensions between the practices themselves – which they felt could be rationally justified – and underlying feelings about these same practices. We saw in the first findings section how Thomas described the need to hang up his facemask due to equipment shortages. As he elaborated: But they [the masks] are hanging close to each other [15–20 centimetres]. But on the other hand people can’t come within 1.5 metres of each other, because they are speaking, or there are aerosols and such. While the idea is that with a facemask that doesn’t happen, they [the masks] don’t speak, there is no movement. But deep down you feel ‘those masks are close together’. (Thomas, end of May)
Here we see multiple logics conflicting with one another. Thomas knew that the underlying reason for hanging up the masks was not scientific-rational but practical – his hospital simply did not have enough of them. The practice of hanging up masks could still be rationally justified as safe, at least within an account focusing on aerosol movement. Yet from a more affective logic, Thomas felt a jarring between the thorough routines of strict protective measures (disinfecting his hands, putting on protective clothing) and the rather improvised line with the facemasks. He noted elsewhere in the interviews that it was quite difficult to only touch the elastic cords/bands of the facemasks and that people probably put on the wrong facemask by mistake.
In this way, wider organisational-policy and economic-supply tensions, shaped in turn by underlying legitimation and rationality tensions in the realm of policy-making and economics (Habermas, 1976), could be seen to become manifest in the individual narratives and experiences of healthcare professionals. Attempts to resolve these tensions often proved unsuccessful, leading most participants’ narratives to sooner or later resort to non-rational logics such as faith in rituals around spatial and symbolic boundaries (Douglas, 1966), hopes in safe futures (Good, 2001; Brown et al., 2015) and fatalism (Douglas, 1992): . . . I think, yeah, if I am going to get sick then so be it, yeah, then I will see it happen. [But] I am not such a pessimist. (Anne, end of June)
Even Thomas who, of the six participants, adopted the most calculative-rationalised narrative style, drifted nevertheless towards fatalism at particular moments: And yeah, that, so occasionally someone from the care staff is going to get sick . . . or that is, alas, unavoidable. Then I think, we just have to accept that. (Thomas, early April)
Discussion
Our findings thus build on and extend work which notes the combining of different (non) rational-calculative strategies (Zinn, 2016), particularly by paying attention to the tensions that emerge amid these ‘bricolages’ (Brown and Gale, 2018; Horlick-Jones et al., 2007). Rather than explaining these away, our post-formal (Brown et al., 2015) approach focuses on these tensions as manifestations of more deeply rooted crises in terms of political-economy of healthcare and evidence-based practice, balancing a clinical working identity with lives outside of the hospital, and rules of thinking and acting as a scientific expert versus rules of feeling as a caring professional (Hochschild, 1979).
Our longitudinal approach not only allowed us to explore how uncertainties receded and/or emerged over time but also how coping developed through this tumultuous period via experience, confidence in the organisational system, hopes, and the development of routines around safety protocols. The data analysis we have presented above reflects a recent tradition (Horlick-Jones et al., 2007; Zinn, 2016) by remaining attentive to multiple strategies – rational, non-rational and ‘in-between’ (Zinn, 2016) – working alongside one another. While some participants seemingly sought to present highly rationalised accounts, the limits of rationality were strongly apparent in all six accounts and all participants effectively syncretised rational-calculative and non-rational approaches (Alaszewski, 2015).
These syncretised approaches took different forms, with more calculative evidence-based strategies being combined with: a differentiation between safety-consciousness at work and more ‘relaxed’ approaches outside the hospital; fatalism regarding the potential of contracting COVID-19 (Douglas, 1992); and/or a faith in the highly routinised boundary distinctions between cleanliness and dirt (Douglas, 1966), and between wards where these routines were followed well and ‘other’ wards which were more chaotic (Douglas, 1992). Roth’s (1957) classic study of magic and ritual in contagion control was chiefly based on a hospital ethnography rich in observational data. COVID-19 safety measures made such a study impossible, alas, but using in-depth longitudinal interviews and photo voice nevertheless enabled insights into the ‘inconsistencies’ (p. 310) and pragmatic rule-bending of infection control activities in relation to various objects and people.
The ways in which rules were followed differently at different points in time, across different spaces and by different professions, as driven by busyness and PPE shortages, echoed Roth’s findings that practices were often shaped ‘more on convenience and ease of administration than on rationally deduced probabilities’ (1957: 310). As with Roth’s hospital ethnography, the participants in our study were aware of these inconsistencies or tensions, and struggled with them. Yet their partial commitment to particular routines and practices, especially as these pertained to the handling of meaningful objects with the goal of bringing particular futures into being, also reflects Roth’s work on the power of ritual (or even magic) for handling residual uncertainty which emerged at the limits of rationality (1957: 312–314).
It is important to acknowledge that the small study sample of young professionals, alongside the use of interviews and a participant generated photo voice approach, inevitably shaped the data. Although similar tensions in crises - in terms of political-economy of healthcare, evidence-based practices, and economic scarcity in the context of COVID-19 - are experienced in most European contexts, such as the UK, healthcare professionals in other healthcare systems may have had different experiences of vulnerability and coping amid uncertainty during the COVID-19 pandemic.
Conclusion
The study findings presented above give important insights into a small, purposive sample of Dutch healthcare professionals’ narratives of their experiences of, and coping amid, uncertainty during the Corona pandemic. Small-n, very in-depth designs are more common within an interpretative-phenomenological tradition focused on sense-making and lifeworlds and our design makes a novel contribution to the COVID-19 and wider sociology of risk and uncertainty literatures by enabling an attentiveness to changing understandings of, and approaches to, uncertainty by professionals over time (following Henwood, 2019). Moreover, because of the way COVID-19 has undermined medicine-as-normal, the data collected in this study arguably provide important insights into wider tendencies of, and experiences amid, modern medical practices – not least those pertaining to risk and uncertainty. The prevalence of rituals, hope and other non-rational approaches to coping with uncertainty and risk is striking here, in particular because many of these phenomena have remained neglected, certainly among studies of healthcare practices in Northern Europe. While some approaches, such as hope (Good, 2001), have received quite some critical attention, the combining of multiple approaches and the tensions emerging here require further investigation; amid COVID-19 care and more widely. Such studies may benefit from embracing a post-formal attentiveness to tensions, and a reflexivity towards the binaries we noted at the start of the article. Our research furthermore points to the added value of multiple follow-up interviews within a longitudinal design, as a means of tracing evolving experiences and understandings of uncertainty, vulnerability and coping over time.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.