
Abstract
Autonomy and independence have become crucial elements of end-of-life decision making. Opinions on the latter are, however, strongly contested in public discourses. This contribution analyses arguments in favour of and against a Dutch civil society initiative which promotes the extension of the legislation on euthanasia. The authors investigate Dutch newspapers associated with three groups: religious, liberal and humanist perspectives, and do so by utilising quantitative and qualitative elements from a discourse-analytical perspective, raising the following questions: Which stances can be identified? How do different parties position themselves with regard to a ‘completed life’ and a ‘good death’? To what extent do these positions create demarcations between ‘us’ and ‘them’? The authors show that the debate developed along the lines of three key topoi: the topos of autonomy, the topos of human worth and the topos of embeddedness. The authors thereby identify how the different discursive positions define different visions of dying as ‘legitimate’ and as a proper end to a completed life.
Introduction
In The Loneliness of Dying, Norbert Elias (1985) speaks of the increasingly monadic nature of today’s individuals, emphasising our relation to dying as a thoroughly social one. While traditionally, as Bauman (1992: 15) observes, death had not been a matter of choice but the ‘ultimate humiliation of reason and control’, in late modernity even death has become a site for individualism in which modern subjectivities need to assert themselves (Exley, 2004).
As such, the modalities of self-directed dying have become a contested issue, especially in relation to euthanasia and assisted suicide. In many Western countries, civil society actors demand the right to decide over one’s death. In the United Kingdom groups such as Dignity in Dying advocate for patients’ right to take end-of-life decisions. Although historically a sensitive issue, Germany recently passed legislation for more ‘liberal’ procedures, and even in Catholic Italy, groups have collected signatures to enforce legislation. Other European countries such as Switzerland, the Netherlands, Belgium and Luxembourg have already legalised euthanasia, under various restricting conditions. Consequently, and as self-chosen death becomes part of one’s potential choices in life, debates on what constitutes the good death become crucial issues of public concern.
Against this background, we raise the following questions: how is death constructed in debates about euthanasia, considering present-day images of ideal subjects – and how does this construction reinforce idealised subjectivities? More specifically: how do differently situated ideological camps construct a ‘completed life’ when arguing for/against the right for euthanasia? We take a discourse-analytical perspective and suggest understanding debates on euthanasia as debates over what and who we want and do not want to be.
For this endeavour, we focus on the Dutch debate surrounding the initiative of the civil society group Uit Vrije Wil [Of Free Will]. The initiative seeks to foster emancipation and self-determination of older citizens who should be allowed to decide about their death (Peeters and Sutorius, 2011). Rejecting the often-cited fear of ending one’s life in a care home, its goal is to enable older people who consider their life completed to request euthanasia (Peeters and Sutorius, 2011). To avoid suffering and to die in a dignified way, the currently restricting legal conditions for euthanasia (unbearable suffering with no prospect of improvement) should be removed. In May 2010, the group collected 116,871 signatures, demanding to legalise assisted suicide in cases where the person claims to have lived a ‘completed live’. A parliamentary commission held talks and the parliament finally rejected the initiative. In September 2013 the next round of consultation started and research was commissioned by the Ministry of Health (www.uitvrijewil.nu). In 2016, the initiative Voltooid Leven [Completed Life] was revisited through a concept law, put forward by the liberal party D66, which was followed by further research. Finally, in July 2020, D66 again introduced a concept law to parliament (‘Voorstel van wet houdende toetsing van levenseindebegeleiding van ouderen op verzoek [Proposal for a law on end-of-life support on request for older people]’ (www.uitvrijewil.nu). The initiative that started the debate on the possibilities and conditions of the completed life a decade ago has thus managed to inspire and shape the political discourse profoundly. To understand the voices raised in this discourse, we go back to the public debate in which different ideological positions were first and most clearly, formulated.
To identify the underlying conceptions of the good life and the good death, we examine three distinct ideological responses – loosely based on the tradition of pillarisation of Dutch society (Van Dam, 2015) – to this group’s activism: the liberal, the religious (in our data, this is a Christian Protestant one) and the humanist position. This is not to argue that these positions are entirely homogeneous or cannot overlap at all (as if there has been no pluralisation and liquidisation; see Bauman, 2000), but to point out that these three offer specific grounds from which the aforementioned debate was approached and evaluated. We draw on data from national newspapers from the main period of public debate (2010–2013) and carve out the different ways in which subjectivities are articulated through, first, a keyword analysis (corpus linguistics) and, second, an eclectic discourse-historical analysis (Reisigl and Wodak, 2009).
Reviewing dying
Old age is often comprehended through a ‘deficit paradigm’ (Coupland et al., 1991), emphasising limitations and vulnerabilities of older people. This gets more explicit in the depiction of the latest stage in old age, which has been conceptualised as the ‘social imaginary of the 4th age’ (Higgs and Gilleard, 2015). Like other social imaginaries, the 4th age is needed for society to uphold an ideal of personhood. The collectively imagined 4th age functions as period that encompasses all the fears associated with old age and, at the same time, allows demarcation of an active period for older people, characterised by choice, autonomy and self-expression (Higgs and Gilleard, 2015: 14). The societal image pictures people in the latest life stages being limited in their agency, human intimacy or social exchange. Due to frailty, abjection and dependence on care the 4th age is a social vision that captures imaginaries of a position people fear and desperately want to avoid. Public perceptions mark the meaning of a good, proper, active life and thus by extension, the rejected, undesirable state.
Borgstrom (2015) demonstrates the significance of the construction of a ‘good death’, ideally at home, whereby the focus shifts more explicitly onto matters of choice and control. In line with increasing consumerism (Collyer et al., 2015; Kirby et al., 2015), ‘choice’ is constructed as a solution to individual and societal challenges (Schwarz, 2018). The ability to choose, Borgstrom (2015: 705) argues, is perceived to ‘represent a “good death”, quality of care, and to some extent, the value of personhood’. The underlying assumption is that choice and the ability to plan one’s life until and beyond death (Raddon and Ciupa, 2011) reconfirm personhood and reject the coinciding of biological and social death. However, contrary to this idealised image, individual choices are not merely expressions of personal desire but represent socially constituted expectations and constructions (Collyer et al., 2015).
The emphasis on choice and individualism is influenced by cultural forces that have reconfigured the dying process (Broom and Kirby, 2013). In countries where euthanasia has been normalised, the aim of a choice biography can lead to the recognition of a ‘completed life’ and related organised death (Wijngaarden et al., 2014). Thus, euthanasia ‘emerges as an ultimate symbol of control – the lack of which, for many people, is unbearable’ (Johnstone, 2013: 175).
Unsurprisingly, debates over euthanasia are deeply polarised (Johnstone, 2013) and groups in society engage in discursive struggles over the definition of the issue, its causal interpretation and moral evaluation. One of these actors is the right-to-die movement (McInerney, 2006: 654). Debates have been observed in many countries, including France (Teisseyre et al., 2005), Germany (Jordan, 2011), the United Kingdom (O’Neill et al., 2003) and Australia (Eliott and Olver, 2008). Of course, religious beliefs, socio-demographic factors and national traditions affect such debates, something particularly visible in Belgium (Cohen et al., 2012).
In the Netherlands euthanasia has long been debated by civil society, resulting in established policies and regulations. As Green-Pedersen (2007: 274) argues, euthanasia became a political issue along pre-existing conflict lines between secular and non-secular parties. However, over time, euthanasia has been ‘normalised’ (Norwood, 2007), now seen as one amongst many end-of-life options. Medical technology and health care, changing societal attitudes and individualisation have characterised the context of these debates (Weyers, 2006). Overall, the legal framework in the Netherlands is relatively transparent (Onwuteaka-Philipsen et al., 2012) – though this has not harmonised levels of acceptance of end-of-life decision making (Rietjens et al., 2005). To end one’s life, one must confirm suffering and the loss of dignity. Euthanasia and/or assisted suicide become contributors to a socially acceptable end of life (Van Baarsen, 2009): ‘It is thus not self-determination as such but the combination of the request and the suffering that constitutes the situation in which termination of life is considered justifiable’ (Weyers, 2006: 811).
The year 2010 saw the rise of a new campaign called Voltooid Leven [Completed Life], which seeks to ‘making self-determination of life’s end’ the central focus (Wijngaarden et al., 2014). If a one feels alienated from oneself and the world and feels detached from one’s life (Wijngaarden et al., 2015), why, within such an imaginary, should one’s ‘free will’ not decide over one’s life?
We now turn our attention to how this civil society actor’s intervention has tried to reconstruct modern subjectivities via the issue of dying.
Data and method
This article analyses knowledge production and contestation surrounding activism by the Dutch civil society group Uit Vrije Wil [Of Free Will]. After we had familiarised ourselves with the group by considering its webpage (www.uitvrijewil.nu) and book (Peeters and Sutorius, 2011), our systematic analysis of voices focused on media texts representing liberal positions, religious ones and ones we call humanist. We are interested in claims along the lines of relatively distinct ideological camps, thus sampling the investigated material around the three factions, representing ideal-type positions (see Fitzpatrick, 2008). Speaking of ideal types does not deny that identities have become more fluid, something sociology has long related to religion too. Instead of simply claiming the decline of religion (or its replacement by spiritual revolutions; see Partridge, 2004), research has argued that religion too has become liquid. De Groot (2008) examines liquid religious praxis (inside, at the border of and beyond the religious sphere), arguing for a persistent, yet different, relevance of religion as offering possibilities to belong. The discursive struggle we analyse can similarly be read as reasserting (religious) community or, more critically put, as policing the boundaries of the respective communities. Thus, while (not just religious) identities are fluid to some extent, we do argue that core convictions can be identified (see also Fitzpatrick, 2008).
In these ideal-type positions the liberal perspective centres on the individual, its autonomy and its capacity for rational action. The religious camp views life as a gift from God which, as such, is sacred and must be preserved. The humanist perspective too values life in itself and criticises social norms and welfare systems which fail to provide sufficient care. Whilst thus partly resembling religious voices, humanists lack the reference to a supreme being.
To gain access to these voices, we collected data between 2010 and 2013 from Dutch national newspapers (while we did include all newspapers in our search, the debate only marginally reached tabloids). As mentioned above, the political debate on those issues is still ongoing; we limited our analysis to these initial years, however, as it was those first negotiations in which the public debate took shape and in which different ideological positions were first and most clearly formulated. Using the newspaper archive LexisNexis (www.lexisnexis.nl/) we identified all contributions mentioning ‘Uit Vrije Wil’ [Of Free Will] and/or ‘Voltooid Leven’ [Completed Life] anywhere in the text. After eliminating duplicates or irrelevant articles, we ended up with 154 contributions. During an initial content analysis of all texts collected, each one of them was categorised as giving voice to primarily a liberal, a religious or a humanist position. This led to the establishment of three corpora, according to the three ideological camps. Representing liberal voices, we collected 42 texts (39,011 words) which were published in NRC Handelsblad, NRC Next, Volkskrant, Trouw and Het Parool; representing religious voices, we collected 62 articles (44,035 words), published in Reformatorisch Dagblad and Nederlands Dagblad; and representing humanist voices, we collected 50 texts (42,379 words), published in Trouw, AD, NRC, NRC Next, Volkskrant, Het Parool, Nederlands Dagblad, Reformatorisch Dagblad, De Telegraaf and De Pers. Not the primary ideological orientation of newspapers defined our corpora, but every single article was coded. The three corpora are relatively similar in size and there is some diversity in terms of newspapers giving voice to different positions (with the exception of the religious position).
The data were analysed adopting the discourse-historical approach in critical discourse studies (CDS). We understand discourse as comprised of, first, context-dependent semiotic practices; second, as socially constituted as well as socially constitutive; third, as macro-topic-related; and, fourth, as pluri-perspective and argumentative (Reisigl and Wodak, 2009: 89). CDS investigates the ways in which texts and discourses promote representations of actions, events, objects and processes. Our analytical procedure starts by drawing on quantitative corpus linguistics (CL) to identify key lexis which enables us to conduct the in-depth analysis at significant points. Utilising the programme WordSmith 6.0 through the use of keyword analysis, our aim is to identify key lexis in the discursive construction of a ‘good death’ by the proponents of this debate. This enables us to see the degree to which a word is more common in one corpus than in a comparison (reference) corpus. Thus, we look for the keywords in what we call the liberal corpus vis-a-vis the religious corpus and so forth (see Table 1; see also, for example, Subtirelu and Baker, 2018).
Keyword analysis concerning the three corpora (words are ranked according to their keyness score [log-likelihood], all words displayed are present in at least 20% of texts of the respective corpus [the number of texts in presented in parentheses]).
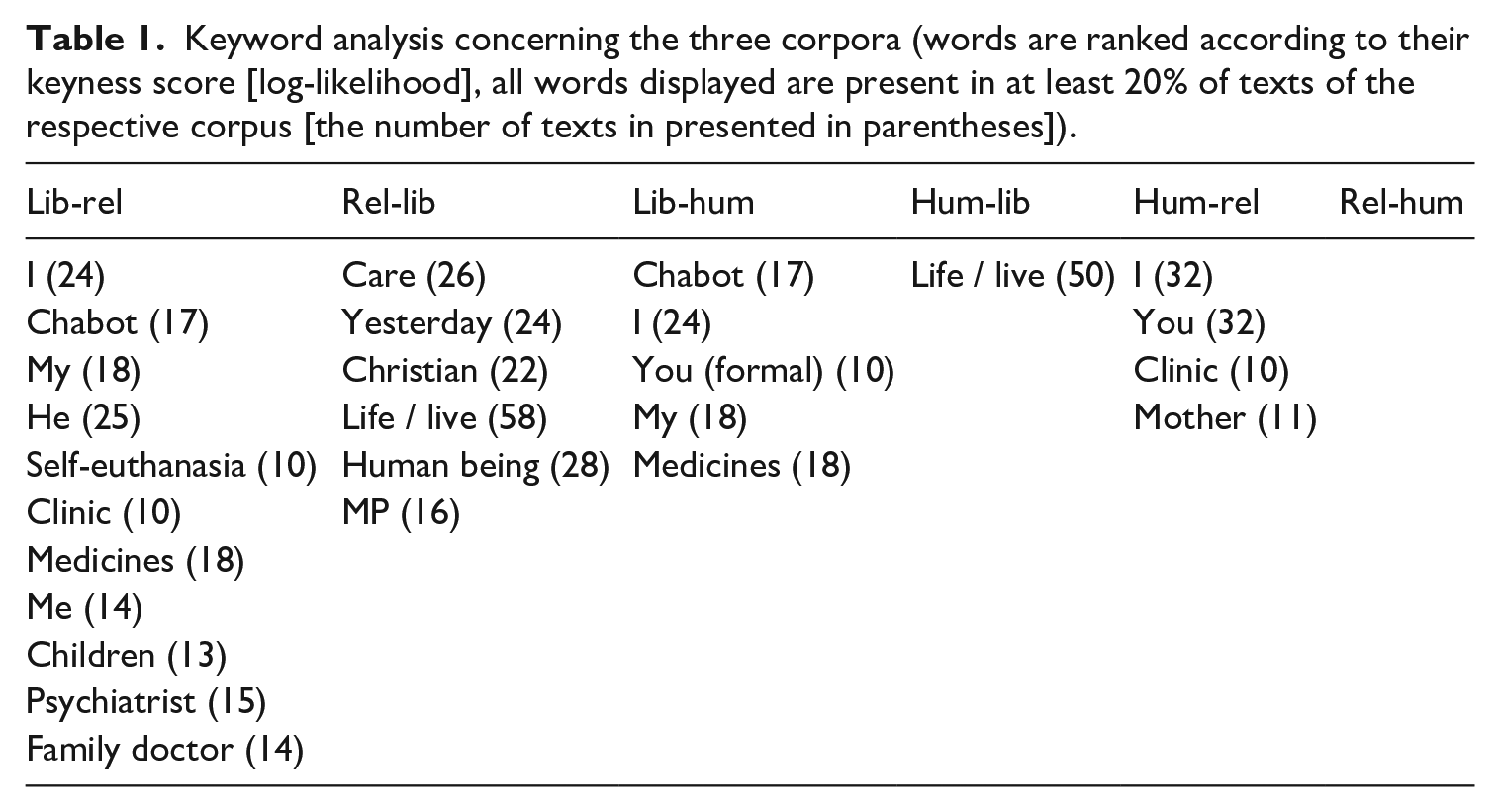
We start this analysis by considering the aforementioned keywords which provided an initial, computer-assisted indication of different foci characterising the three, distinct corpora. Here, we consider only those words that are key in the respective corpora, and which appear in at least 20% of texts in the respective corpus. Second, the data are analysed in detail with a focus on discursive macro-strategies, referring to more or less conscious acts which serve purposes or help to achieve goals (Forchtner and Schneickert, 2016; Reisigl and Wodak, 2009: 94). We focus specifically on nomination (how actors, events, objects and processes are referred to), predication (what characteristics are attributed to them) and perspectivisation (from where involvement is expressed), and argumentation strategies (realised through conclusion rules which justify claims and legitimise standpoints). Conclusion rules (‘if-then’), known as ‘topoi’, connect the argument to the claim. They are formal or content-related warrants that, while being rarely explicitly stated, justify the transition from the arguments to the conclusion (Reisigl and Wodak, 2009: 102). As such, we analyse the key representations and arguments via which ‘others’ are systematically delegitimised through ‘negative other-representation, acts of blaming, scapegoating, marginalising, excluding, attacking the moral character of some individual or group, . . . attacking the rationality and sanity of the other’ and inverted attempts to legitimise the self (Chilton, 2004: 46ff.).
Analysis: The struggle over free will and the good death
We begin our analysis of the debate by considering how the three camps diverge through a CL entry-level analysis of keywords of each of the six possible combinations.
The first column, for example, refers to those words that appear statistically significantly more often in the liberal than in the religious corpus, while the second column shows the words that appear more often in the religious corpus. Looking at the concordance lines in which these items feature, we see that the use of ‘I’ and ‘My’ is due to direct speech and reference to personal stories (e.g. my mother). ‘My’ refers to experiences with dying family members but also the formulation of ‘my’ wish and ideal of how to live and die. In the liberal corpus the psychiatrist Boudewijn Chabot plays a highly prominent role as one of the main proponents of assisted suicide. ‘Clinic’ refers to the planned clinics for euthanasia while ‘medicine’ points to how euthanasia is and can be carried out. Family doctors feature prominently as those who should assist people with their wish to die.
Religious sources very diligently report on news, events and decisions in the context of the initiative. Hence, ‘yesterday’ and ‘MP’ feature prominently. Additionally these contributions stress ‘human being’, referring abstractly (in contrast to liberals) to the person that allegedly wants to die. The reference to ‘Christian’ (what Christians want and how they view the issue) is not surprising while ‘life’ is usually put in inverted commas as in ‘clear with life’ and ‘completed life’ or as description of attacks on unwanted life. ‘Care’ is positively referred to, e.g. in palliative care, but also when cuts in care are criticised and better care is demanded.
Also in humanist sources ‘life’ features prominently, mainly debating the question of what constitutes a good or completed life. The personal pronouns ‘I’ and ‘you’ point to a personalised conversation with the readers. Personal stories are also present through family stories about one’s ‘mother’.
This entry-level analysis provides a first sketch of the contested field. The three positions mainly diverge from each other vis-a-vis the autonomy of the subject versus its proper care, the latter two defining the two outer poles of the discursive arena. Utilising Alexander’s (2006) conceptional framework for the civil sphere, we linked his categorisation of subjects/motives/institutions to our initial inductive insights. That is, moving back and forth between the inductive and deductive, we structure our analysis around, first, who is the main subject position? Second, what is the main theme of discussion and conflict? Third, how, i.e. under which institutional arrangements, should the issue be primarily treated and solved? These three dimensions are: older people, autonomy and care. This is not to say that ‘the old’, autonomy and care are the only ‘answers’ given to who, what and how – though they are clearly the most dominant ones as visible in the dominance of concepts such as elderly, 70-plus, 70-plussers; freedom, voluntary, right of self-determination, self, oneself; and care, doctor, help, clinic, KNMG (the Royal Dutch Medical Association) in our corpus. In terms of argumentation schemes, these three dimensions structure contestation through the utilisation of three different topoi which justify the liberal, religious and humanist position. We could name these three the topos of autonomy (‘if humans are autonomous, then they should be allowed to autonomously decide about their completed life and its end’), the topos of human worth (‘if humans are created by God, then they should be enabled to live a completed life until the end’) and the topos of embeddedness (‘if humans are part of an I–We dialectic, then they should be enabled to experience fulfilment until the end’). In the following qualitative analysis, we delve deeper into these perspectives.
Contested elderly
In this section, we turn to the subjects who are debated. Above we identified ‘the old’ as the main subject position under question (in contrast to, e.g., doctors or politicians).
In explicit reaction to negative perceptions of older people in public discourses (in which the old are often being caricatured as passive, vulnerable and dependent; see Weicht, 2013) the liberal perspective performs a counterweight to such negative stereotypes. Liberal contributions in our corpus articulate older people as active subjects in charge – or at least with a right to be in charge of their destiny. They are autonomous and self-reliant; they are active in judging and describing their life as completed; and they have earned themselves the right to decide to die. In turn, however, ‘the old’ are portrayed as victims of laws and regulations and hence request and deserve public debates. More outspoken than earlier generations, they are presented in the historical context of emancipation movements. They are characterised as not willing to depend on care in institutions as passive recipients. An example of the liberal position towards the old in this debate is put forward by the Amsterdam daily Het Parool:
The story starts with a typical temporal code (before/after) which emphasises the woman’s continuous desire for independent and rational decision making. Indeed, the ‘87 years old Mrs. C. van der Zee’ is constructed as active (‘she has had’, ‘she’s afraid’, ‘she knew’) and thus as a being who can be legitimately put in charge of her life. Care is constructed as a failing, ignorant practice that is not listening to the individual’s demands. The failure is one of the nation. The older person is independent and autonomous, he/she should have the right to self-determine his/her life – something which is juxtaposed with a gloomy outlook if that right is not exercised.
Religious voices too point to the affected subjects and their plight, which, however, are represented very differently. First, the old are represented as suffering and lonely and not feeling connected to society anymore. We – society – need to protect and take care of this group, which are valuable from the start to the end of life. Religious voices present older people as marginalised victims of the citizens’ initiative which puts them under pressure to end their lives. As life has been given by God, many non-believers are losing sense and meaning which should give rise to spiritual practices. This rendering of the social is visible in the following excerpt: Salden [director of Catholic organisation for the elderly] feels that the discussion on help with self-euthanasia stands in contrast with the cuts on care for
This passage illustrates a critical perspective on contemporary culture and the lack of support. Talking about ‘people’, this continuously nominates the subject in general and relational terms. At the same time, the article questions the very premises of the liberal argument, i.e. the individual’s autonomy, and aims for shifting the grounds of the entire debate by stressing a different concept of the person. Such ‘ideal’ subjectivities would precisely not be ‘isolated islands’, would not understand themselves as a detached individual autonomously deciding over their fate in light of their agency (‘what you can or can’t do’). Rather, they would view themselves as embedded within networks of significance (‘family, children, acquaintances’) through which life becomes meaningful. The conclusion rule signifies that older people suffer due to the image of the individual person, which should thus be changed.
Humanists share many aspects of the religious critique, focusing, however, on the inner-worldly embeddedness of individuals. Individuals are always part of social groups and as such interdependent instead of isolated. The following extract illustrates this: The problem for these
This extract illustrates the interdependence of individuals and, thus, their necessarily vulnerable nature – in particular in the case of the old who are depressed, feel insecure and lonely (especially in care homes). The initiative and its idea of the old is criticised as too individualistic since it does not take the social environment into account. In consequence, it is this environment (‘retrenchment in care and the lacking social support’) which is criticised. It is, according to this analysis, not the autonomous individual who naturally feels that life is useless and that they are often confronted with and are portrayed as causes for enormous costs. Instead, such feelings emerge due to a lack of people who care and support the creation of meaning in life. Instead of letting ‘our elderly’ make decisions in a bad context, the latter needs to be changed through more care which will help them to accept suffering as part of life.
Contested autonomy
Like the articulation of the subject (older people), the proclaimed aim of life and its connection to personhood is also contested. As noted, the ideal of independence penetrates all levels of modern society (Weicht, 2011). While autonomy emphasises its progressive function vis-a-vis traditional settings, becoming dependent is, in turn, associated with being a burden on others. Discourses on care for older people have difficulty in moving beyond the utopic thrall of independence since the latter represents what is considered a good life. All three perspectives feature debates on the concept of autonomy, while they are differing in its significance for a completed life.
The liberal perspective views life as personal belonging. Individuals should determine their own lives and must have the right to take destiny into their own hands. As people can make rational choices, the state should not interfere but take self-determination seriously. Society should allow citizens to end their lives whenever they wish to. Laws and regulations are restricting people’s autonomy and a thorough liberation process is required to break this taboo and thereby end the religious monopoly on morality. Liberal perspectives see euthanasia as an inevitable step in the process of increasing self-determination and emancipation. This is documented in the following extract from NRC Next (10/02/2010): . . . it is recognised that some elderly have a
The active individual is emphasised – semantic intensification (‘real’) making the dichotomy even more pronounced – which, by being able to make his/her own choices, leaves behind an oppressive past. Having the choice becomes the symbol of self-determination and through that the ideal and goal itself (Borgstrom, 2015). Control is positioned against an ‘unplanned death’ (Raddon and Ciupa, 2011) and this control, enabled through the choices available, is furthermore seen as protecting one’s dignity (Johnstone, 2013: 145). Allowing choices should thus become the goal of policy making.
While there is certainly diversity to the religious position at large (i.e. beyond our newspaper-focused analysis), we find that religious voices, in contrast to liberal ones, oppose viewing autonomy as the guiding category in thinking about dying. Indeed, explicit references to life being given by God, which implies a duty to live this life, are frequent. Moreover, Christians view dependency not simply as part of human existence but as state in life that is at least as crucial as autonomy. Accordingly, self-determination is not understood as an absolute truth but a philosophical term subordinate to human dignity. When self-determination becomes the highest value, it does in fact conceal that actions always have consequences which are never restricted to individuals. The right for self-determination turns into duty and those who do not adhere to it are viewed as weak. Autonomous freedom and self-determination are part of a cold, juridical side of ethics and instruments of (health) care should not be (mis)used for such a notion.
More important than
Dependency is, first, linked to an eternal being which, in turn, justifies the claim that dependency is a human condition par excellence. Second, strict autonomy is a misguided illusion and should therefore never be a principle for (social) policies. The liberal focus on autonomy is viewed as being an ideological value for the wealthy middle classes (see Krag, 2014).
Humanists too view life as not being restricted to monads but as being all about complex sets of actors who are dependent on each other. This forms an essential part of being human and self-determination is consequently seen as arrogant and egoistic. Nevertheless, these arguments are never as absolute as they are in the case of religious voices. The notion of self-determination takes a concrete character rather than remaining abstract as in the liberal tradition: self-determination requires to take responsibility for oneself – but this always happens within a social context constituted by others. In cases where responsibility and awareness are lacking, self-determination can turn into subjugation because of society’s pressure, leading to situations in which the lives of people who cannot express themselves anymore are described as meaningless. As such, self-determination is gone when others decide that someone with serious impairments should rather not be there anymore. Therefore, self-determination always entails the danger of a slippery slope: discussions might start with self-determination but end with a threat on vulnerable people.
Our human dignity does
This third perspective thus contests the values put forward by the liberal perspective by emphasising humans’ relational nature – but without reference to a higher being. The relational constitution of life extends to questions of self-determination and care (Borgstrom, 2015; Collyer et al., 2015) while challenging individualist and, arguably, consumerist perspectives on (health) care (Kirby et al., 2015).
Contesting care
After identifying the who (the elderly) and the why (the focus on autonomy) we turn to the institutional context of care. The significance of relationships arising from caring for and caring about other people makes care the ultimate contested ground on which questions of self-determination, individual decision making and the definition of the good life are negotiated.
From the liberal perspective, care is viewed as a necessary element for dignified dying. Even palliative care is understood within the framework of helping to die, as euthanasia practised outside caring institutions would be barbaric. Those who favour a traditional understanding of palliative care, i.e. one which only attempts to ease the pain, are considered to act solely based on religious convictions. The argumentation strategy continues that new forms of care need to be developed. This for example means the creation of clinics which people can visit when they have made their decision to die. Care, in such a context, is also placed in the hands of professionals, which should ease the burden for relatives.
According to the NVVE it is high time for attention for people with a serious wish to die who now are
The liberal position presents itself as having the courage to ask difficult questions in relation to whether all care is possible and desirable. The issue of costs is explicitly raised. Traditional care which only seeks to lighten the situation is not seen as solving the issue. In this sense the meaning of care is extended by explicitly introducing the aim of choice. A self-chosen and self-orchestrated death is contrasted with shameful, stigmatised deaths in (care) institutions (Králova, 2015) where dependency and vulnerability challenge the social norms of a good life (Greco, 2009). The liberal arguments of rationality, control and choice are thus meant to provide an alternative form of palliative care which provides comfort and control against a projection of horrible suffering (Norwood, 2007: 164). This avoidance of suffering is additionally highlighted by the idea of learning the lessons from the past (see Forchtner, 2016), as the issue of abortion clinics is seen as comparable.
Such a comparison is not acceptable for the religious perspective for which palliative care signifies love and compassion with the vulnerable. Accordingly, Christians answer to the wish to die with more attention to the individual, with more care. Palliative care, including the easing of pain and loving, compassionate care, are defined as Christian practices. Good, ‘warm’ high quality care takes up the fight for life and enables a dignified end of life. If such questions are taken up, religious actors state, the demand for euthanasia would decline.
. . . it’s often difficult to determine whether there really is no medical cause for a wish to die. In these cases thorough (medical) help
If a certain quality and kind of care can serve as an alternative to the wish to die, the subsequent question arises, why should more attention be paid to euthanasia rather than improving or changing the delivery of care and giving meaning? It is in this context that financial constraints and cuts in psychological care are mentioned. The religious perspective advocates the financial and conceptual strengthening of palliative care as part of basic insurance schemes. Societal willingness to provide proper care is seen as a benchmark to judge the quality of a society and positive valorisation (‘beautiful and difficult work of carers’). In the context of intergenerational care individuals should be able to experience and express warm values such as solidarity, friendship, love, respect and loyalty instead of what is considered cold and hard reactions attached to the wish to die. This coldness, ironically characterised as ‘secular compassion’, is seen as fundamentally different to Christian-inspired compassion. This is further specified when elderly care is described as frightening for some, as attention and help, i.e. care, is much more demanding than receiving an injection. Actors within care institutions thus must be capable of being attentive to other human beings. Doctors, for example, should be selected according to qualities such as empathy and care, mirroring the ideal of those sitting next to the suffering, holding his or her hand.
Similarly, the humanistic perspective on care identifies the existing problem in the lack of fitting forms of care. The lack of palliative care causes loneliness or depression, both indicators for institutions lacking proper care. The reality of care homes is described as harsh and in contrast to the need for a dignified existence. To deal with these issues, care needs to be strengthened and further developed. Attention is given to the negative effects of the introduction of market logics into care-settings which, ultimately, make old age being understood as a cost factor. Retrenchment and cuts in (health) care are thus seen as the core problem. Additionally, the improvement of care through social participation of the old and a stronger focus on the creation of meaning are essential areas of change.
Research shows that the wish to be allowed to die in the near future is common with older people. Understandable if they can’t travel anymore and can’t look after the grandchildren anymore. Old age is considered a blessing but many very old go to bed with the wish to not having to wake up anymore. And
This extract describes how doctors in clinics are inhibited to engage in meaningful relationships with older people. Underlying is a powerful discursive dichotomy of individual freedom on the one hand and meaningful relationships on the other. Relationships form the main focus of the humanist perspective in that the individual is recurrently framed through his/her relationships. What is formulated in those positions is an integration of care and autonomy in the sense of a relational autonomy (Ellis, 2004), ‘where the self is viewed as situated in a matrix of relationships’ (Kittay, 2007: 66). Norwood (2007) argues that the possibility to openly talk about euthanasia provides people the opportunity to engage with their close relations more honestly since the practice of euthanasia is not an individual decision but is profoundly influenced by conversations with one’s loved ones. Humanists in these discourses do not deny the widespread wish for end-of-life measures; they criticise, however, that these debates are stimulated by the limited resources and the ‘normalisation’ of the wish to die through an uncritical and unreflective debate.
Conclusion
In this contribution we have investigated how the discourse on euthanasia and assisted suicide shape modern subjectivities and how the construction of the latter leads to reinterpretations of a completed life and the good death. By distinguishing three ideological positions (liberal, religious, humanist), we demonstrated how argumentation strategies (about the good/bad and the right/wrong) are inherently linked to processes of demarcation between the self and the other. In this, one’s understanding of what constitutes a good life can be linked to one’s perspective on the good death.
Drawing on insights from the preliminary quantitative analysis we examined the discourse via its three key dimensions, responding to the who, the what and the how. That is, we showed different constructions of the subject group (older people); different understandings of the aim of public policies (autonomy); and, finally, differences in the design of policies which are seen as answer to the challenges (care). These differences are based on divergent definitions of the individual and the good life, as well as definitions of society and care. Undoubtedly, articulations of these positions are at time heterogeneous, but our analysis has illustrated clear differences in the initial discursive organisation of this debate.
Analysing the opposing positions on subjectivity, individual autonomy, and care, we subsequently identified three consequential main topoi that depict the three positions of the discursive struggles: through the topos of autonomy, the liberal perspective centres on the individual who ought to have the right for self-determination, control and choice. End-of life questions form an important part of taking independence and autonomy seriously. Religious perspectives can be summarised through the topos of human worth, which directs attention onto the sanctity of human life. Because life and the human being have value in themselves, any debate on prematurely ending this life are considered an assault on the worth of human beings. Finally, humanists employ the topos of embeddeness, which concentrates its discursive contributions on the fact that human beings are inherently relational, and that individual autonomy must therefore always be understood as embedded in the very relational contexts.
Importantly, while our methodological approach is based on the differentiation of three identified perspectives, our aim is not to synthetically demarcate respective groups. Rather, we seek to distinguish ideological perspectives that, however, can be held by different actors. Nevertheless, the contested field of end-of-life decision making brought forward opposing positions which draw heavily on demarcation approaches.
While legal negotiations are ongoing in the Dutch political arena, we demonstrated that the discourse on the initiative to extend the euthanasia laws goes beyond a simple legal debate. The identification of the opposing argumentation strategies displayed how broader societal questions are renegotiated. These include questions of the good life, the relationship between the individual and society and objectives of care policies. Our analysis confirmed that individualism and autonomy are key elements in how people imagine euthanasia. And yet, voices also point to fear and loneliness, thus indicating a lack of recognition, of being wanted and valued.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.