
Abstract
This study investigated identity (i.e., clinical identity, identity dimensions, and identity styles) and its associations with violent recidivism in forensic psychiatric patients. Using surveys and patient records, correlational analyses showed that all three identity approaches were associated with risk and protective factors linked to violent recidivism. Moreover, regression analyses showed that various identity constructs were associated with reduced self-reliance and higher violation of terms and agreements (disturbed identity and lack of identity), the risk scale (exploration in breadth), and lower impulsivity (information-oriented style). The findings suggest to incorporate identity assessment during the diagnostic phase as well as during treatment, as developing a healthy identity could act as an entrance for the treatment of risk factors and strengthening of protective factors.
Treatment progress and the risk of violent recidivism among each forensic psychiatric patient with TBS (“terbeschikkingstelling” in Dutch, with mandatory psychiatric treatment imposed by a court; Drieschner et al., 2018) is annually monitored by professionals using a structured assessment tool that measures various risk factors. However, despite these measures, violent recidivism still takes place (Drieschner et al., 2018), leading to significant harm for victims and substantial societal costs (Meijer et al., 2020). Hence, there is an ongoing need to address and prevent violent recidivism within the forensic psychiatric field. The current study investigates identity as one of the possible factors associated with both risk and protective factors related to violent recidivism.
One possible factor associated with criminal behavior and recidivism is identity impairment. Although commonly measured risk factors for violent recidivism, such as aggression and substance use, or lack of protective factors such as unemployment or poor social skills, have been well-documented (Spreen et al., 2014), there is growing evidence that identity malfunctioning can also contribute to delinquency, particularly among adolescents (Klimstra et al., 2011; Meeus et al., 2012). However, research on identity in relation to delinquent behavior in convicted adult forensic psychiatric patients remains limited and nascent. Investigating the relationship between identity and both risk and protective factors could enhance our understanding of how identity-related factors can contribute to the prediction and prevention of violent recidivism in forensic psychiatric patients. Various theories emphasize the importance of identity in recidivism (Bogaerts et al., 2021; Maruna, 2001, 2004; Paternoster & Bushway, 2009). For instance, the identity theory of desistance developed by Paternoster and Bushway (2009) noted that individuals possessing a well-developed identity (i.e., having a coherent sense of self, including their values, beliefs, goals, and roles in life) are more likely to stop criminal behavior than those without a well-developed identity. According to this theory, identity serves as both a motivation and a direction for behavior. A person’s actions are seen as expressions of one’s self-identity, people intentionally behave in ways that are consistent with who they think they are. Thus, (criminal) behavior is interpreted as an expression of someone’s identity. As individuals develop a new identity incongruent with a criminal lifestyle, they become motivated to align their actions with this revised self-concept, consequently distancing themselves from criminality. This transformation is accompanied by shifts in self-perception, values and beliefs, leading to the adoption of prosocial behavior. Paternoster and Bushway (2009) additionally propose that interventions should focus on helping individuals in constructing a new identity aligned with pro-social norms. However, this theory offers limited insights into identity styles, dimensions, and processes, which are emphasized in this study. Given the complexity of identity as a mechanism, specific aspects will be further explained to theoretically frame our research.
Identity represents an important developmental process throughout life (Arnett, 2000; Erikson, 1968). Individuals with a maladaptive identity have difficulties seeing themselves as unique, and often experience emotional dysregulation and unclear boundaries between themselves and others (American Psychiatric Association [APA], 2022). In recent decades, identity has gained an important role in diagnosing personality disorders (PDs; Bender et al., 2011), particularly within the framework of the Alternative Model of Personality Disorders presented in the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5, Section III; APA, 2013). In the context of forensic patients, research on identity impairments is often linked to borderline and antisocial PD (Tressová et al., 2024), which consequently emerge as the most prevalent PDs in forensic patients (De Ruiter & Greeven, 2000; Van der Veeken et al., 2018).
Although identity development occurs across the lifespan (Arnett, 2000; Erikson, 1968), it is noteworthy that identity research has mainly focused on adolescents and emerging adults in the general population (e.g., Klimstra et al., 2011), with comparatively less attention given to adults and forensic patients (Fadjukoff & Kroger, 2016). Identity malfunctioning is associated with behavioral problems and can trigger certain risk factors associated with aggression and recidivism (Schwartz et al., 2009), issues commonly observed in forensic psychiatric patients (Tressová et al., 2024). However, to our knowledge, no research has investigated the relationship between identity and specific risk and protective factors of aggression and recidivism. Despite decades of research on recidivism-related risk and protective factors, identity has not been recognized as a significant factor in risk assessment and has consequently been overlooked in the treatment of this population (Bogaerts et al., 2020; Jankovic et al., 2021). Currently, it remains unclear how identity (malfunctioning) is associated to risk and protective factors, and how it may contribute to violent recidivism. Therefore, the current study investigates the association between identity and both risk and protective factors related to violent recidivism in adult forensic psychiatric patients, considering identity through three different conceptualizations (clinically relevant identity, identity dimensions, and identity styles).
Identity from Three Different Conceptualizations
Identity refers to an individual’s sense of uniqueness and self-sameness (Erikson, 1950). Individuals with an integrated identity can distinguish between the self and others, while showing continuity in their interactions with the social world. Over the past 50 years, various conceptualizations of identity have been explored (Erikson, 1950, 1968). A first conceptualization focuses on clinically relevant identity functioning, delineated across three domains (Kaufman et al., 2015). First, an integrated or consolidated identity is characterized by a coherent and long-lasting set of values, goals, and commitments that define who a person is (Schwartz et al., 2009). Second, disturbed identity is characterized by a lack of direction in life and commitments across various life domains. Third, extreme identity malfunctioning and feelings of emptiness is manifested as a lack of identity (Erikson, 1958; Kernberg, 2006). Research among adolescents showed that individuals with an integrated identity generally show fewer delinquent behaviors and externalizing problems than individuals with a disturbed identity or a lack of identity (Schwartz et al., 2009). However, the association between identity malfunctioning and violent recidivism among forensic psychiatric patients requires further research.
A second conceptualization pertains to the underlying processes of identity development that are divided into five identity dimensions (Luyckx et al., 2006): exploration in breadth (looking for new commitments), exploration in depth (evaluation of current commitments), ruminative exploration (endlessly worrying over possible choices in life, without coming to a satisfying solution), commitment making (the degree to which commitments in a certain life domain are made) and identification with commitment (the degree to which commitments contribute to a sense of self and provide certainty in life). These dimensions are associated with various indicators of maladjustment (e.g., Mercer et al., 2017; Morsunbul, 2015; Schwartz et al., 2011). Individuals who experience ruminative exploration often fail to complete the process of exploration and to make commitments (Luyckx, Schwartz, Berzonsky, et al., 2008). Therefore, ruminative exploration is negatively associated with the identity dimensions of commitment making and identification with commitment (e.g., Beyers & Luyckx, 2016; Luyckx et al., 2013; Luyckx, Schwartz, Berzonsky, et al., 2008). High levels of ruminative exploration and low levels of commitments are related to aggression and delinquency among adolescents in the general population (Beyers & Luyckx, 2016; Klimstra et al., 2011; Luyckx et al., 2006; Morsunbul, 2015; Schwartz et al., 2009). Exploration in breadth and exploration in depth, as well as both commitment dimensions, are seen as adaptive dimensions of identity (Luyckx, Schwartz, Berzonsky, et al., 2008).
The third identity conceptualization focuses on identity styles (Berzonsky, 1989, 1990) that represents different approaches to identity-exploration tasks and the processing of identity-relevant information. There are three different identity styles: information-oriented, normative, and diffuse-avoidant. Information-oriented individuals make well-informed decisions by actively seeking, processing, and using identity-relevant information through self-reflection, leading to a well-integrated identity (Berzonsky, 1990). Individuals with a normative identity style passively adhere to the expectations and prescriptions of significant others, adopting and affirming others’ values and prescriptions. This can finally result in rigid and conservative commitments (Berzonsky, 1990). The normative identity style also has been found to be positively associated with physical and relational aggression (Smits et al., 2011). Research has shown that strong commitments are most likely to be formed by individuals with the information-oriented or normative identity style (Berzonsky & Niemeyer, 1994). However, individuals who prefer the information-oriented style deliberate over various alternatives before making commitments, while those with the normative style base their commitments on the influence of others without extensive consideration. Finally, individuals with a diffuse-avoidant identity style lack problem-focused coping strategies and mainly use emotion-focused and avoidant coping strategies (Berzonsky, 1992; Seaton & Beaumont, 2008). They often postpone personal decisions until compelled by circumstances, resulting in a loosely integrated identity (Berzonsky, 1990). This style is associated with low prosocial behavior and elevated aggression in non-clinical emerging adults (Smits et al., 2011).
In sum, several subdomains within the diverse conceptualizations of identity, including (1) clinically relevant identity domains, (2) underlying dimensional processes of identity development, and (3) identity styles have shown associations with externalizing problems, low prosocial behavior, delinquent behavior, and aggression, primarily within community and non-forensic clinical samples (Beyers & Luyckx, 2016; Klimstra et al., 2011; Luyckx et al., 2006; Morsunbul, 2015; Schwartz et al., 2009, Smits et al., 2011). Consequently, it is crucial to investigate how these identity constructs relate to aggression-related risk factors in forensic patients, as they may serve as buffer against aggression and recidivism. Hence, a first step to provide valuable insights into the interplay between identity and aggression involves illuminating both risk and protective factors for violent recidivism.
Risk and Protective Factors for Violent Recidivism
Risk factors for criminal behavior and recidivism can be attributed to the central eight, originally situated within the general personality and cognitive social learning (GPCSL) model of criminal conduct (Andrews & Bonta, 2016). The central eight refers to the eight key criminogenic factors that predict recidivism. Apart from the static risk factor “criminal history,” all other factors are dynamic and potentially changeable in two directions (e.g., one can stop using drugs or increase drug abuse) (Andrews & Bonta, 2016; Heffernan & Ward, 2019). Dynamic risk factors are important from a treatment and rehabilitation perspective because a decrease in these factors is associated with a reduced likelihood of future recidivism (Andrews & Bonta, 2016; Smith et al., 2009).
Dynamic risk and protective factors can be classified within two prominent models for offender treatment. The Risk Need Responsivity (RNR) model, derived from the GPCSL theory, consists of general responsivity, which employs cognitive social learning methods to influence behavior, and specific responsivity, which emphasizes tailoring treatment to individual patient characteristics, based on three principles (e.g., Andrews & Bonta, 2016): (1) the risk principle (matching the level and intensity of treatment to the offender’s risk of recidivism), (2) the needs principle (targeting criminogenic needs in treatment, e.g., the Central Eight), and (3) the responsivity principle (considering offender characteristics, such as learning style during treatment) (Andrews & Bonta, 2016). Treatment following the RNR principles has been shown to reduce the risk of recidivism by 17% compared to offenders not treated according to the RNR principles (Andrews & Bonta, 2016). In addition to the RNR model, the Good Lives Model (GLM) can be seen as a complementary approach. The GLM is a strengths-based approach that emphasizes protective factors, such as skills and competences of offenders (Höing et al., 2013; Ward & Brown, 2004; Ward et al., 2007). Thus, the aim of GLM is not to tackle the risk factors themselves, but to increase the protective factors so that offenders can learn to deal with these risk factors.
The factors that should be targeted in offender treatment are also referred to as the Central Eight. These have also influenced different risk assessment tools used to predict future recidivism and monitor treatment progress (Jankovic et al., 2021). One widely recognized and extensively used risk assessment tool is the Historical, Clinical, Risk Management-20 Violence Risk Assessment Guide (HCR-20 V3; Douglas & Skeem, 2005). In Dutch forensic psychiatry and the prison system, the Historical Clinical Future-Revised (Historisch Klinisch Toekomst, HKT-R; Spreen et al., 2014) is the most commonly used instrument. Administered at least annually, the HKT-R assesses the risk level and changes in the risk of violent recidivism compared to previous assessments. Comprising historical, clinical, and future factors, the HKT-R yields a higher total score for increased risk of violent recidivism. While historical factors are static, clinical and future factors are changeable and serve as treatment goals (Spreen et al., 2014). Dynamic HKT-R factors can be divided into risk and protective factors. Risk factors, such as impulsivity, heighten the risk of recidivism, while protective factors, such as self-control, mitigate the risk of recidivism (Andrews & Bonta, 2016; Heffernan & Ward, 2019).
In forensic risk assessment and treatment, consideration of both risk and protective factors is important when assessing the risk of recidivism and making decisions, such as regarding unguided leave or unconditional release (Douglas & Skeem, 2005; Kepfisz et al., 2016). Although identity in offenders could potentially be considered as a dynamic risk or protective factor, there is limited knowledge of the relationship between clinically relevant identity domains, underlying dimensional processes of identity development, and identity styles on the one hand, and risk and protective factors of violent recidivism on the other. The specific risk factors associated with identity characteristics in forensic patients remain unclear. Therefore, further research is needed to better understand this relationship and to develop effective interventions aimed at identity development, reducing risk factors, and enhancing protective factors in forensic patients.
The Current Study
The aim of the current study is to investigate the importance of three different identity conceptualizations (clinical and dimensional identity approach, and identity styles) for risk and protective factors of violent recidivism in adult forensic psychiatric patients.
First, we will investigate the associations between the clinical and dimensional identity approach, and identity styles on the one hand, and risk and protective factors for violent recidivism on the other. Drawing on previous research (e.g., Beyers & Luyckx, 2016; Klimstra et al., 2011), from a clinical identity perspective, we expect that higher levels of disturbed identity and a lack of identity, and lower levels of consolidated identity will be positively associated with risk factors and negatively associated with protective factors (Kernberg, 2006; Schwartz et al., 2009). Regarding identity dimensions, we expect that higher levels of ruminative exploration and lower levels of exploration in breadth, exploration in depth, and both commitment dimensions (commitment making and identification with commitment) will be positively linked to risk factors and negatively linked to protective factors. Regarding identity styles, we hypothesize that lower levels of the informational identity style and higher levels of the normative and diffuse-avoidant style will be positively associated with risk factors and negatively with protective factors (Smits et al, 2011).
Second, we will investigate the predictive contributions of each identity conceptualization separately for the risk and protective factors for violent recidivism to gain insight into which identity conceptualization and what kind of specific construct within each conceptualization will have the strongest predictive contribution. We hypothesize that low levels of consolidated identity, high levels of disturbed identity and lack of identity (from the clinical approach), low levels of exploration in breadth, exploration in depth, both commitment dimensions (commitment making and identification with commitment), and high levels of ruminative exploration (from the dimensional approach), as well as low levels of the information-oriented style, and high levels of the normative and diffuse-avoidant style (from the identity style approach) will predict higher scores on risk factors and lower scores on protective factors for violent recidivism.
Method
Participants and Procedure
The present study is part of a larger longitudinal project entitled “Identity, implicit schemes and self-regulation in forensic psychiatry.” Ethical approval was obtained from the Ethics Review Board of Tilburg University (EC-2017.45). Seventy-five male patients participated in this study. These patients stayed in three forensic psychiatric centers (FPCs) in the Netherlands (Rotterdam) and Belgium (Ghent and Antwerp). This cross-sectional study relies on data collected in different waves. For the statistical analyses related to the clinical identity and dimensional identity measurements, the first wave was used (N = 75). For the identity styles measurement, the second (patients in Belgium) and fourth wave (patients in the Netherlands) were used (N = 57). Patients in the FPC in the Netherlands committed crimes with a minimum sentence of 4 years, for which they were given a TBS order. TBS in the Netherlands is a mandatory admission to a high-security FPC with compulsory psychiatric treatment imposed by a court on those who have committed a serious crime because of severe mental disorder(s). The primary goals are to protect society and reintegrate these patients into society. Due to a mental disorder and high risk of recidivism, patients were declared partially or fully unaccountable for their offence (van Marle, 2002). All Belgian patients were deemed completely irresponsible for their offenses due to their mental state. They received an internment measure from the court because of the risk of recidivism (Jeandarme et al., 2016). The group of Dutch and Belgian patients is similar to those found “not guilty by reason of insanity” or “guilty but mentally ill” in the United States, though legal and treatment systems differ.
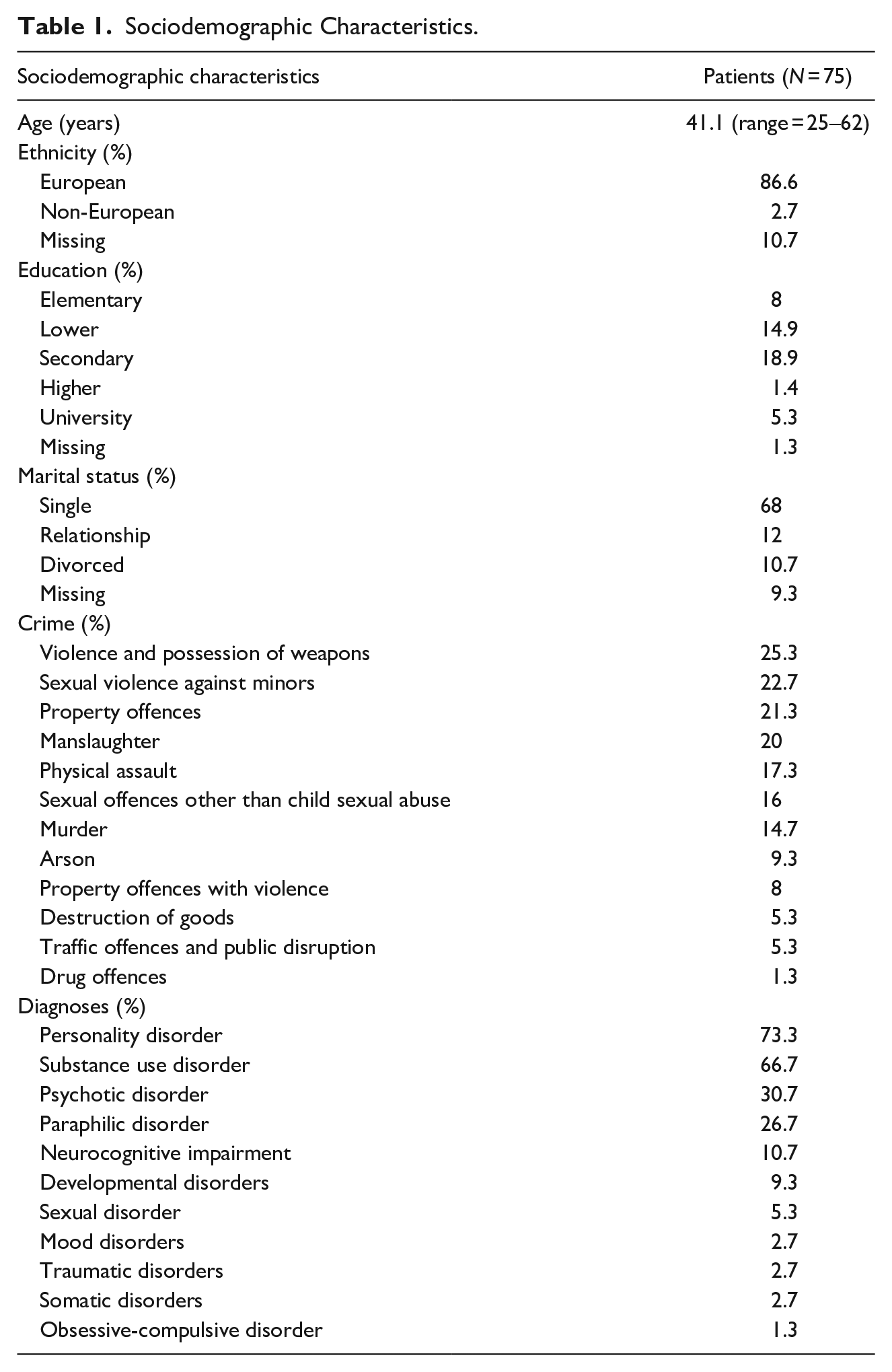
Most of the patients were either Belgian (61.3%) or Dutch (22.7%). A majority was single (68%) and completed secondary school (50.7%). The mean age at the first data collection point was 41.12 years old (SD = 10.11; range = 25–62).
The most common index crimes committed by the patients were violence and possession of weapons (25.3%), sexual violence against minors (22.7%), property offences (21.3%), and manslaughter (20%) (see Table 1 for an overview). These percentages do not sum to 100% because some patients were convicted of multiple offences at the same time. Common diagnoses were PD (73.3%), substance use disorder (66.7%), psychotic disorder (30.7%), and paraphilic disorder (26.7%) (Table 1). Many patients had comorbid disorders.
Sociodemographic Characteristics.
Prior to data collection, the heads of treatment at the FPCs informed all patients about the study. Patients received an information letter and attended an information session where the goals and procedures of the research were explained. Two weeks later, participants signed an informed consent, allowing the use of their electronic patient data (e.g., diagnoses and crimes), and completed multiple surveys. Participation was voluntary, and participants could withdraw at any time without providing a reason and without any consequences. Collected data were kept confidential and were not shared with practitioners or third parties. During the assessment, participants had unlimited time to complete the computerized self-report questionnaires, with a short break to minimize unwanted response effects. A research assistant was available to answer any questions. Patients received a €10 reward after each assessment.
Measures
The Self-Concept and Identity Measure (SCIM)
Clinical identity was assessed with the SCIM (Kaufman et al., 2015). This self-report questionnaire consists of three scales that assess consolidated identity (eight items; “I know who I am”), disturbed identity (11 items; “I imitate other people instead of being myself”), and lack of identity (six items; “I no longer know who I am”). All 25 items were rated on a seven-point Likert scale ranging from 1 (completely disagree) to 7 (completely agree). Participants could also select the “I don’t know” option. Past research showed reliable and structurally valid test scores (Kaufman et al., 2015). In the present study, the scales of the SCIM showed poor (.52, consolidated identity) and good (.82, disturbed identity and .83, lack of identity) Cronbach’s alpha values. These results correspond with the reliability results found in the study of Kaufman et al. (2015) where consolidated identity also showed the lowest Cronbach’s alpha values. For further investigation of reliability, also an average inter-item correlation was calculated and considered acceptable in the range of .15 to .50 (Clark & Watson, 1995). An average inter-item correlation for consolidated identity showed a value of .12 and was considered unacceptable, since it did not fall between .15 and .50. No further analyses were performed with this consolidated identity scale due to poor reliability.
The Dimensions of Identity Development Scale (DIDS)
The DIDS (Luyckx, Schwartz, Goossens, et al., 2008) is a self-report questionnaire measuring five dimensions of identity development: exploration in breadth (“I think about different things I might do in the future”), exploration in depth (“I think about the future plans I already made”), ruminative exploration (“I am doubtful about what I really want to achieve in life.”), commitment making (“I have plans for what I am going to do in the future”), and identification with commitment (“My plans for the future match with my true interests and values”), each measured by five items. All 25 items were rated on a 5-point Likert scale ranging from 1 (completely untrue) to 5 (completely true). The DIDS has good validity and reliability (Luyckx, Schwartz, Berzonsky, et al., 2008; Luyckx, Schwartz, Goossens, et al., 2008). In the present study, Cronbach’s alpha values of the DIDS scales ranged from acceptable (.79, exploration in depth) to excellent (.90, commitment making).
The Identity Style Inventory (ISI-4)
The ISI-4 (Smits et al., 2008) is a self-report questionnaire assessing identity styles: the information-oriented style (seven items; “When facing a life decision, I try to analyze the situation in order to understand it”), the normative style (eight items; “I strive to achieve the goals my family and friends hold for me”), and the diffuse-avoidant style (nine items; ”Many times, by not concerning myself with personal problems, they work themselves out”). All 24 items were scored on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The ISI-4 showed good reliability and validity (Smits et al., 2008). Cronbach’s alpha values of the ISI-4 in the current study ranged from acceptable (.74, information-oriented style) to good (.86, diffuse-avoidant style).
Historical-Clinical-Future-Revised (HKT-R)
The HKT-R (Bogaerts et al., 2018; Spreen et al., 2014) is a structured risk assessment tool to measure the risk of future violent recidivism among forensic psychiatric patients. It is composed of historical, clinical, and future domain factors, with higher scores indicating a higher risk of recidivism. In the present study, only the clinical domain was included because it reflects a patient’s psychopathology over the past 12 months and consists of dynamic factors important for treatment. Since the historical factors are not reversible and future factors relate to the situation after release, we did not include these factors in our analyses. The clinical domain consists of 14 factors. The HKT-R data were analyzed at four levels: (1) the total clinical score of the HKT-R, (2), the risk and protective scales separately, (3) the protective awareness and protective skills subscales derived from the protective scale, and (4) the 14 individual factors of the HKT-R clinical scale. First, we created the clinical scale based on the 14 HKT-R factors, indicating that participants with higher sum scores showed a higher risk of recidivism, thus meaning they exhibited higher levels of risk factors and lower levels of protective factors. Then, the risk scale (psychotic symptoms, addiction, impulsivity, antisocial behavior, hostility, violation of terms and agreements, influence of risky network members) and protective scale (problem insight, social skills, self-reliance, cooperation with treatment, responsibility for the offence, coping skills, labor skills) were computed. The seven factors of the protective scale were reversed (i.e., 0 = no protection, 4 = high protection), while the scores on the risk factors remained the same (i.e., 0 = no risk, 4 = high risk) (Bogaerts et al., 2020). Next, to validate the factor structure of the risk and protective scales, a principal component factor analyses with a varimax rotation (Varimax with Kaiser Normalization) was conducted separately on these two scales. Factor analyses showed a two-factor solution for the protective scale (Supplementary table 1) and therefore it was split into a protective awareness subscale (problem insight, treatment compliance, and taking responsibility for the index offense), and a protective skills subscale (self-reliance, social skills, coping skills, and labor skills), aligning with the study of Jankovic et al. (2021). The Cronbach’s alphas in the current study showed values ranging from poor (.58, protective skills subscale), questionable (.68, protective scale), acceptable (.70, protective awareness subscale, .76, risk scale) to good (.80, clinical scale). Average inter-item correlations for the protective awareness subscale and protective skills subscale were .45 and .27, respectively. Since these correlations fall between .15 and .50 (Clark & Watson, 1995), both subscales were included in further analyses. Unlike in the study of Jankovic et al. (2021), an exploratory factor analysis yielded a two-factor solution for the risk scale as well (Supplementary table 2). However, the Cronbach alpha for one of the subscales showed to be unacceptable (α = .38). Moreover, the average inter-item correlations for these subscales were .03 and .76, which did not fall within the acceptable range of .15 and .50 (Clark & Watson, 1995). Therefore, the two factor solution for the risk scale was not included in further analyses.
Statistical Analyses
An a priori power analysis with G*Power 3.1 was performed to calculate the necessary sample size (Faul et al., 2007) with a large effect size (f2 = .35), an alpha of .05, two-tailed testing, power of .95, and a maximum of three (the scales of SCIM and ISI) or five predictors (the scales of DIDS). The results showed that 54 (a maximum of three predictors) and 63 participants (a maximum of five predictors) were needed to achieve a power of .95. Therefore, 57 (statistical analyses related to ISI) and 75 participants (statistical analyses related to SCIM and DIDS) were sufficient. All statistical analyses were performed using SPSS 26. Since the data collection was computerized using Qualtrics, there were no missing values. However, 61 participants selected the option “I do not know” in the SCIM, so these responses were coded as missing. Outliers were inspected using boxplots (27 in total) and included in further analyses to maintain heterogenity. Multicollinearity was checked using correlations with r ≥ .70 indicating multicollinearity. A histogram and scatterplot were used to check the assumptions of homoscedasticity and normality. Due to the presence of outliers and violations of the assumptions of multicollinearity and normality, Spearman’s Rho correlations were used to investigate associations between identity conceptualizations and both risk and protective factors for violent recidivism. Finally, to test the predictive contributions of identity conceptualizations for risk and protective factors at the four operationalization levels of the HKT-R, multiple regression analyses with bootstrapping were performed separately for the DIDS, SCIM, and ISI. Effect estimates were derived from bias-corrected 95% bootstrap confidence intervals, using 2,000 bootstrap resamples. If the overall model was significant, the confidence intervals were interpreted.
Results
Spearman’s Rho Correlations between Identity (SCIM, DIDS, and ISI) and HKT-R
Table 2 presents the results of the Spearman’s Rho analyses investigating the associations between the identity constructs and the HKT-R. Concerning the associations between SCIM and HKT-R, disturbed identity was negatively associated with protective skills and self-reliance. Lack of identity positively correlated with the risk scale and violation of terms and agreements, while displaying a negative correlation with self-reliance.
Bivariate Spearman’s Rho Correlations Between SCIM, DIDS, ISI, and HKT-R.
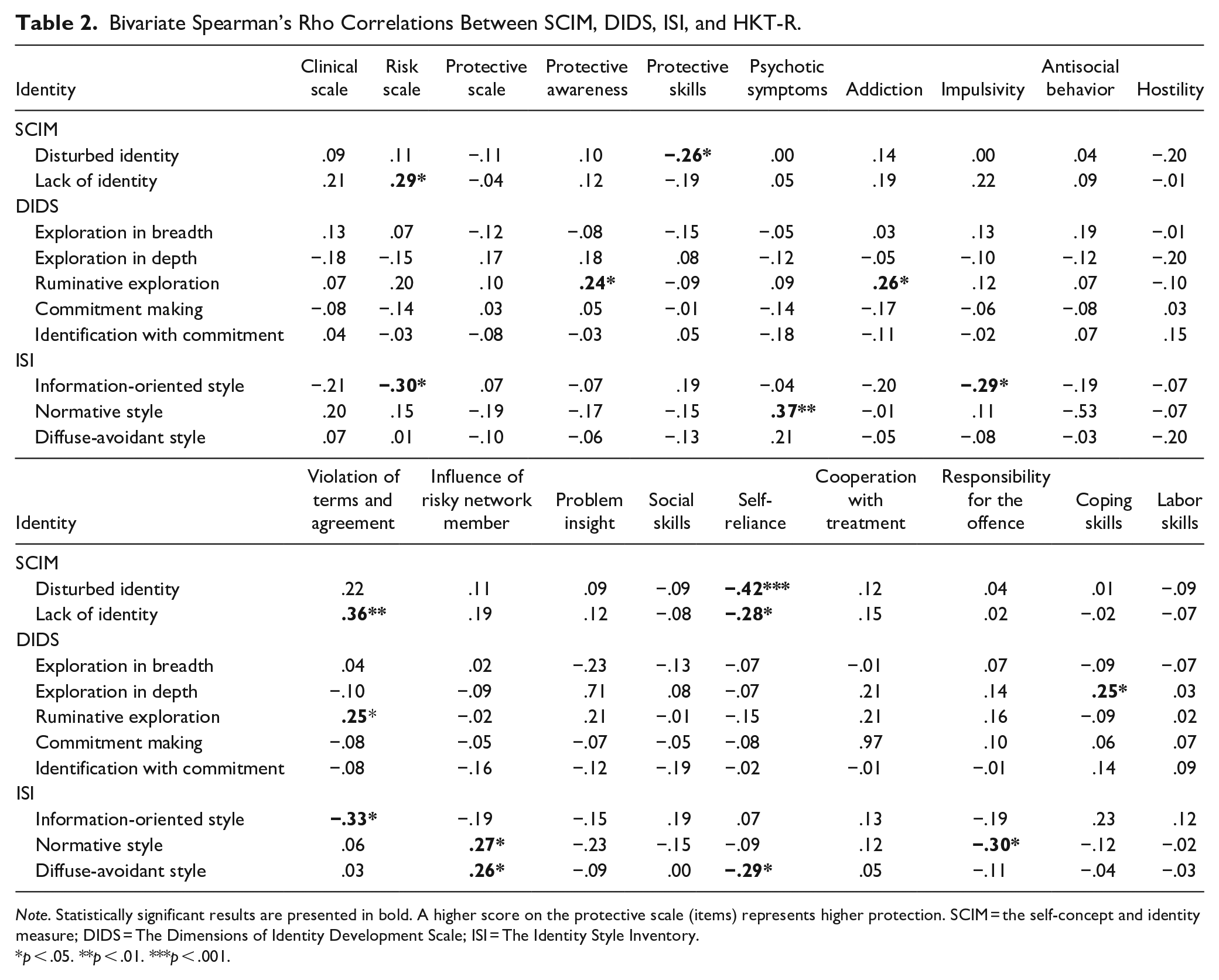
Note. Statistically significant results are presented in bold. A higher score on the protective scale (items) represents higher protection. SCIM = the self-concept and identity measure; DIDS = The Dimensions of Identity Development Scale; ISI = The Identity Style Inventory.
p < .05. **p < .01. ***p < .001.
Regarding the associations between DIDS and HKT-R, exploration in depth was positively associated with coping skills. Ruminative exploration was positively associated with the protective awareness subscale, addiction, and violation of terms and agreements.
Correlational analyses between ISI and HKT-R showed that the information-oriented style was negatively associated with the risk scale, impulsivity, and violation of terms and agreements. The normative style showed positive associations with psychotic symptoms and influence of risky network members, and a negative association with responsibility for the offence. The diffuse-avoidant style was positively associated with influence of risky network members and negatively with self-reliance. No other statistically significant results were found.
Multiple Linear Regression Analyses with Bootstrapping of Identity (SCIM, DIDS, and ISI) Predicting HKT-R
A multiple linear regression with bootstrapping was conducted to predict the HKT-R from identity constructs (per conceptualization) (see Table 3). Only statistically significant models were reported. Regression analysis using the SCIM resulted in a significant model for predicting the protective factor self-reliance, R2 = .20, F(2, 72) = 9.03, p < .001. Only disturbed identity (controlling for lack of identity) negatively predicted self-reliance (β = −.40 [−.66, −.13]). Also the model predicting the risk factor violation of terms and agreements was significant, R2 = .12, F(2, 72) = 4.69, p < .05. Only lack of identity (controlling for disturbed identity) significantly predicted violation of terms and agreements (β = .36 [.03, .67]).
Multiple Linear Regression Analyses With Bootstrapping of SCIM, DIDS, and ISI Predicting HKT-R.
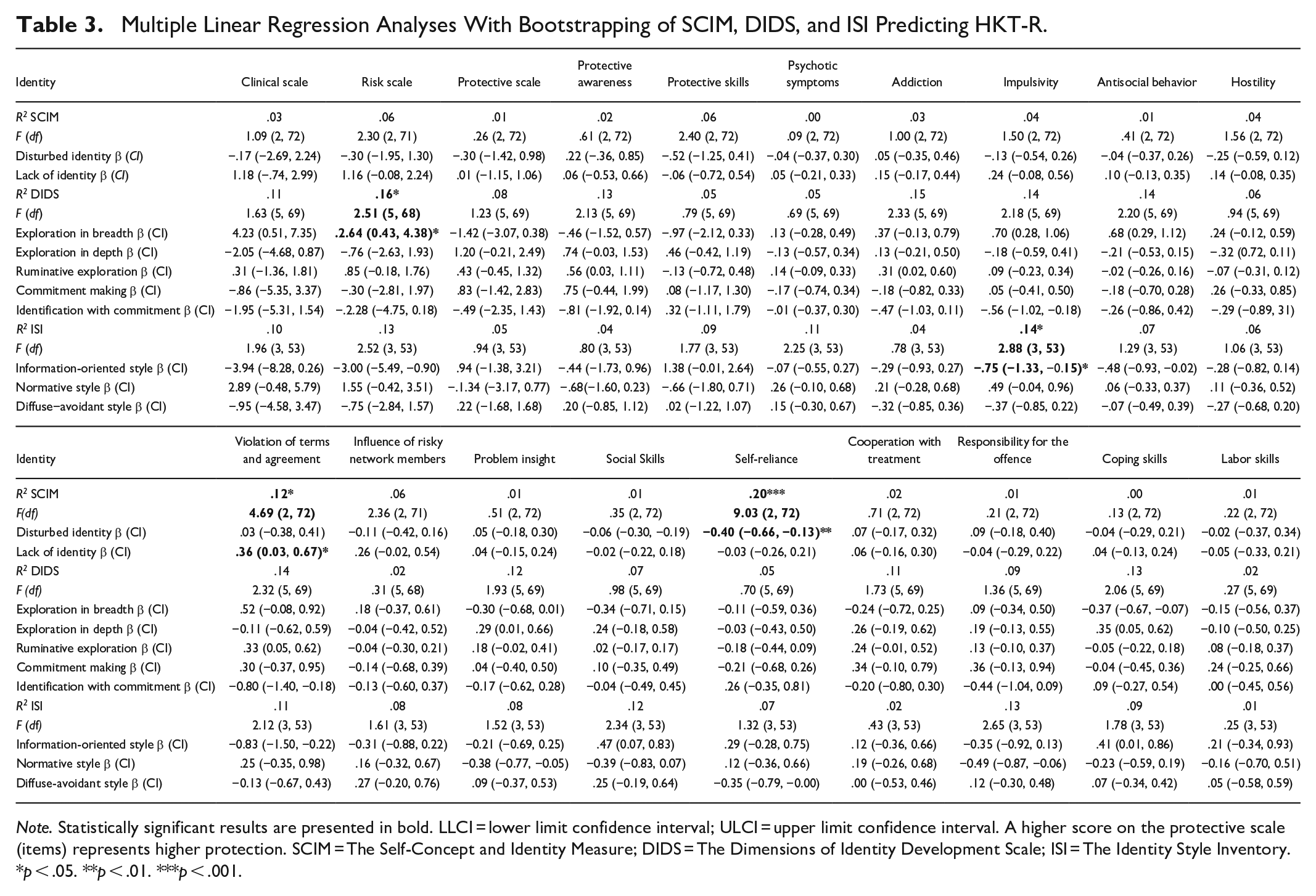
Note. Statistically significant results are presented in bold. LLCI = lower limit confidence interval; ULCI = upper limit confidence interval. A higher score on the protective scale (items) represents higher protection. SCIM = The Self-Concept and Identity Measure; DIDS = The Dimensions of Identity Development Scale; ISI = The Identity Style Inventory.
p < .05. **p < .01. ***p < .001.
Regarding the DIDS, the model predicting the risk factors scale was significant, R2 = .16, F(5, 68) = 2.52, p < .05. Only exploration in breadth (controlling for the other four dimensions) showed to positively predict the risk factors scale (β = 2.64 [.43, 4.38]).
Regression analysis using the ISI showed a significant model for predicting the risk factor impulsivity, R2 = .14, F(3, 53) = 2.88, p < .05. Only the information-oriented style (controlling for the other two styles) negatively predicted impulsivity (β = −.75 [−1.33, −.15]). No other statistically significant results were found.
Discussion
The aim of the present study was to investigate the importance of three different identity conceptualizations (clinical and dimensional identity approach, and identity styles) for risk and protective factors of violent recidivism in adult forensic psychiatric patients. First, we statistically analyzed the associations between the clinical and dimensional identity approach, and identity styles on the one hand, and risk and protective factors for violent recidivism on the other. From a clinical identity perspective, we hypothesized that high levels of disturbed identity and a lack of identity, as well as low levels of consolidated identity, would be positively associated with risk factors and negatively associated with protective factors (Kernberg, 2006; Schwartz et al., 2009). In line with this hypothesis, we found that disturbed identity was negatively associated with protective skills. Both disturbed identity and lack of identity were negatively associated with the protective factor self-reliance. Additionally, lack of identity correlated positively with the risk scale and the risk factor violation of terms and agreements. Due to the low Cronbach’s alpha of the consolidated identity scale, we could not test the hypothesis regarding this scale and its association with HKT-R. Nevertheless, our results suggest that disturbances in clinical identity functioning are associated with increased risk factors for violent recidivism and reduced protective factors. These factors are important factors for successful reintegration into society and reducing the likelihood of recidivism (Andrews & Bonta, 2016; Heffernan & Ward, 2019).
Regarding identity dimensions, we hypothesized that high levels of ruminative exploration and low levels of exploration in breadth, exploration in depth, and both commitment dimensions (commitment making and identification with commitment) would be positively associated to risk factors and negatively associated to protective factors. The results showed that exploration in depth was indeed positively associated with the protective factor coping skills. Furthermore, ruminative exploration showed positive associations with the risk factors addiction and violation of terms and agreements, consistent with previous research (Klimstra et al., 2011; Luyckx, Schwartz, Berzonsky, et al., 2008; Schwartz et al., 2009). Unexpectedly, ruminative exploration, typically seen as a maladaptive identity dimension (Luyckx, Schwartz, Berzonsky, et al., 2008), was also positively associated with the protective awareness scale. Given that ruminative exploration involves overthinking various options (Luyckx et al., 2006), it is possible that forensic patients high in ruminative exploration may develop more awareness and insight into their own identity-related challenges in developing and maintaining a stable and coherent identity (Schwartz et al., 2013). This heightened awareness could potentially lead to a better understanding of the consequences of their actions and a willingness to engage in protective behavior or at least avoid engaging in risk behavior. However, all correlations concerning the dimensional approach were weak and should be interpreted with caution, as there might be other determinants at play.
With regard to identity styles, we hypothesized that low levels of the information-oriented style and high levels of the normative and diffuse-avoidant style would be positively associated with risk factors and negatively associated with protective factors related to violent recidivism. Our analyses confirmed this hypothesis. The information-oriented style was negatively associated with the risk scale and the risk factors impulsivity and violation of terms and agreements. Moreover, the normative style showed positive associations with the risk factors psychotic symptoms and influence of risky network-members, and a negative association with the protective factor responsibility for the offence. The diffuse-avoidant style was positively associated with the risk factor influence of risky network-members and negatively with the protective factor self-reliance. As expected according to previous research (Berzonsky, 1990; Smits et al., 2011), patients who adopt an information-oriented style tend to have lower scores on risk factors, which consequently reduces their risk of recidivism. Conversely, patients with primarily normative and diffuse-avoidant styles show difficulties in taking responsibility for their offenses and in completing essential daily tasks independently. Additionally, they are more vulnerable to negative external influences, which compromises their ability to resist peer pressure and increases their risk of engaging in risky behavior and recidivism.
Second, we investigated the predictive contributions of each identity conceptualization for the risk and protective factors related to violent recidivism. The analyses confirmed our hypotheses for all three identity conceptualizations (Smits et al, 2011). For clinical identity, the results showed that patients experiencing disturbances in their identity might exhibit reduced self-reliance, potentially undermining their ability to cope with stressors and resist engaging in criminal behavior. Moreover, lack of identity predicted the risk factor violation of terms and agreements, highlighting the importance of addressing maladaptive identity in interventions aimed at reducing the risk of violent recidivism. Regarding identity dimensions, exploration in breadth showed to positively predict the risk scale, indicating that patients who engage in broad exploration of identity may be more prone to various risk factors associated with recidivism. From the identity styles perspective, the information-oriented style showed to negatively predict impulsivity. This suggest that patients who adopt an information-oriented approach may show greater self-control and thoughtfulness in their decision-making processes, thus reducing impulsive behavior that could otherwise increase the risk of violent recidivism. In summary, all three identity conceptualizations (i.e., clinical identity, identity dimensions, and identity styles) demonstrated significant predictive contributions to various risk and protective factors leading to or preventing violent recidivism. Furthermore, the clinical identity conceptualization made the strongest predictive contribution to risk and protective factors, due to its largest effect sizes and most significant results.
Although we only found a limited number of significant associations, and most of them were weak, certain risk and protective factors emerged as particularly important in their associations with identity. These factors, such as the influence of risky networks and impulsivity as risk factors, and self-reliance as a protective factor, consistently showed significant associations with various identity scales. Notable, the risk factor violation of terms and agreement showed associations across all three identity approaches. Therefore, identity may play a crucial role for some factors compared to others, while its impact on other factors may be less pronounced. Moreover, the results of this study might suggest that individuals with a certain identity style are more susceptible to peer influences and have difficulty regulating their impulses, and therefore may be more likely to engage in risky or impulsive behaviors as a result. Furthermore, based on our results we might assume that patients with identity impairments may struggle to comply with their treatment’s terms and conditions, increasing the likelihood of violating these agreements. On the other hand, we might assume that individuals with a strong sense of identity may be more capable to rely on themselves and make healthier choices, which can decrease their likelihood of recidivism. More research is needed to investigate these assumptions.
This study has several limitations. First, the sample size may limit the detection of smaller effects. Second, some subscales demonstrated poor reliability, so findings should be interpreted with caution. Third, the cross-sectional research design hindered us to draw conclusions about the direction of effects between identity and both risk and protective factors. Finally, the inclusion of only male participants means that the findings cannot be generalized to female forensic psychiatric patients. Future research should include female forensic patients as well as patients from forensic institutions with different security levels to allow for comparisons across these groups.
Despite its limitations, this study is, to our knowledge, among the first to explore the relationship between identity and the risk and protective factors associated with violent recidivism in a forensic psychiatric sample. The inclusion of this sample is a significant strength of this study because forensic psychiatric patients are generally difficult to reach due to their mental illness. Moreover, we successfully included three various identity perspectives, with all risk and protective factors analyzed separately. This approach provides a detailed view of the associations between identity and both risk and protective factors related to violent recidivism. Furthermore, the HKT-R data were analyzed at four levels (the total clinical score of the HKT-R, the risk and protective scales separately, the protective awareness and protective skills subscales derived from the protective scale, and the 14 individual factors of the HKT-R clinical scale). It is advisable to analyze the HKT-R data at multiple levels, as our findings indicate that significant results are predominantly observed at the individual factor (i.e., item) level, such as impulsivity, rather than within broader composite scales, such as the risk scale.
Although with caution, the findings of this study underscore the importance of integrating identity assessment during both the diagnostic phase and treatment. Given that identity has been shown to be associated with certain risk and protective factors, it could be helpful for clinical practitioners working with forensic patients to regularly assess the patient’s current identity state. Based on the findings of the study, therapeutic interventions should focus on aspects of identity that influence the risk of violent recidivism. Developing a healthier identity may help address risk factors and strengthen protective factors. For example, patients with identity disturbances could benefit from interventions aimed at consolidating their self-concept and strengthening self-reliance (Oyserman et al., 2012). Treatments that support healthy identity development may reduce risk factors such as violating terms and agreements. Additionally, patients with high levels of ruminative exploration might benefit from interventions that limit excessive rumination and encourage more adaptive coping strategies (Aldao et al., 2010). This approach could help patients manage their behavior more effectively and enhance protective factors, such as self-reliance, reducing the likelihood of future violent behavior. This knowledge can help clinicians not only in identifying potential risks related to offense-driven behavior, but also in tailoring treatment to the individual needs of each patient aligning with the responsivity principle of the RNR model. Interventions should be adapted to specific difficulties in developing a healthy identity. For instance, patients with high ruminative exploration may require more individualized strategies to manage excessive overthinking than those with a more consolidated identity. Furthermore, addressing identity disturbances, such as helping patients develop a stable sense of self, may target dynamic risk factors like impulsivity and non-compliance with conditions (Lutz et al., 2022). Customizing interventions in this way enhances the likelihood that patients will respond effectively to treatment (Andrews & Bonta, 2016).
In conclusion, clinical identity, identity dimensions as well as identity styles show associations with risk and protective factors linked to violent recidivism. Forensic patients with disturbed identity or lack of identity, and those exploring broad possibilities and looking for new commitments, showed higher levels of risk factors and lower levels of protective factors. Individuals with an information-oriented style demonstrated better self-control and thoughtful decision-making, which was associated with lower risk of impulsive behavior and violent recidivism. Specific risk factors, such as the influence of risky networks, impulsivity, and violation of terms and agreement, and the specific protective factor self-reliance may be more strongly associated with certain aspects of identity than others. Moreover, the clinical identity conceptualization had the strongest contribution in predicting risk and protective factors linked to violent recidivism. In addition, it is recommended to analyze HKT-R data at multiple levels, as our findings suggest that significant results are primarily found at the individual factor level, rather than within broader composite scales. Given the associations found between identity and risk/protective factors, forensic institutions might consider integrating structured identity assessments into routine diagnostics and treatment to better tailor interventions. However, as the findings are preliminary and effects sizes were small, further research is necessary before implementing definitive policy changes.
Supplemental Material
sj-docx-1-cad-10.1177_00111287251346142 – Supplemental material for The Associations Between Identity and Both Risk and Protective Factors Related to Violent Recidivism in Adult Forensic Psychiatric Patients
Supplemental material, sj-docx-1-cad-10.1177_00111287251346142 for The Associations Between Identity and Both Risk and Protective Factors Related to Violent Recidivism in Adult Forensic Psychiatric Patients by Deni Tressová, Elien De Caluwé and Stefan Bogaerts in Crime & Delinquency
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Ethics Review Board of Tilburg University (EC-2017.45). All participants provided written informed consent.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.