
Abstract
Adverse childhood experiences (ACEs) have long-term impacts. This study explores the association between ACEs, emotional regulation difficulties (ERD), and substance use (SU); the differences between the general and prison populations regarding ACEs, ERD, and SU; and the predictors of ERD and SU. The sample comprises 203 participants (143 French general population and 60 French prisoners). Participants from the general population reported higher bullying victimization, while prisoners showed higher ACEs. Age, education level, growing up with an incarcerated household member, and SU are predictors of ERD. Sex, the presence of a partner, community and collective violence, and difficulty in adopting goal-oriented behavior are predictors of SU. This study highlights the need for early interventions to reduce ERD, SU, and criminal trajectories.
Keywords
Introduction
Adverse Childhood Experiences (ACEs) are generally defined as stressful and potentially traumatic events that occur during childhood and adolescence before age 18 (Felitti et al., 1998). They have been shown to have negative consequences for the health and well-being of individuals (e.g., Anda et al., 2006; Nelson et al., 2020). The ACE concept introduced by Felitti et al. (1998) includes experiences such as child abuse (emotional, physical, and sexual), neglect (emotional and physical), and home or family dysfunction (substance use, mental health problems, criminal behavior, domestic violence, divorce, or separation). Later, more experiences, such as violence outside the home (bullying, community violence, collective violence), have been included in the concept of ACE (Tarquinio et al., 2023).
Over the past two decades, several studies have also found associations between the number of exposures to ACEs and disorders later in life (e.g., Nelson et al., 2020; Poole et al., 2018; Wang et al., 2022). In France, a study of 2,174 adults showed that 25.6% of the participants reported having at least one ACE, and 8.5% reported having two or more (Hughes et al., 2021). The literature points out that ACEs have a short and long-term impact on physical and mental health, with various serious problems being found in adulthood (Tarquinio et al., 2023). For example, the loss of a parent during childhood has lasting consequences, influencing an individual’s psychological and emotional well-being, social relationships, and overall life satisfaction in adulthood (Sebastian et al., 2024). Research found a relationship between ACEs and disrupted neurodevelopment, social, emotional, and cognitive impairment, serious health problems (disease, disability, early death), as well as health risk behaviors (e.g., Anda et al., 2006; Zarei et al., 2021) such as substance use (SU) and/or criminal behaviors (Basto-Pereira et al., 2022; He et al., 2022).
Individuals with four or more ACEs are seven times more likely to be incarcerated (Compassion Prison Project [CPJ], 2024). Indeed, it has been shown that exposure to adverse experiences can cause permanent damage to the developing brain and alter the functioning of the immune, neurological, and endocrine systems in an individual, as well as alter the molecular and genetic makeup of a child (Boullier & Blair, 2018). This underlying phenomenon can be explained by one of the body’s most important systems, the stress response system, which becomes active when we experience stress. This activation heightens our alertness, increases heart rate, and elevates levels of stress hormones (e.g., adrenaline and cortisol) (Chu, 2022). Therefore, the body is prepared to react. The stress response is, at first, adaptive, allowing the body to cope with the challenges faced by internal or external stressors. However, when exposure to a stressor is perceived as intense, repeated, or prolonged, this response can become maladaptive and detrimental to physiology (Russell & Lightman, 2019). Stress experienced in childhood can lead to changes in the hypothalamic-pituitary-adrenal axis, structural changes in the brain, and alterations in the expression of genes in the mesolimbic dopaminergic reward pathway linked to the development of addiction (Enoch, 2011). Recent studies showed that ACEs affect individuals’ empathy (Antunes et al., 2021) and attachment in adulthood (Almeida & Costa, 2023).
ACEs and Emotional Regulation
Research has shown alterations in brain regions such as the amygdala and hippocampus (involved in emotions), changes in the prefrontal cortex (the attention area), decision-making, and self-control (Bryan, 2019; Gupta et al., 2011). These brain changes could result in emotional distress and emotional regulation difficulties (ERD). Other studies suggested that children who experienced ACEs showed various outcomes in adulthood associated with emotion regulation and coping strategies (e.g., Lavi et al., 2019; Miu et al., 2022). ACEs have also been linked with difficulties with impulse control (Rudenstine et al., 2019).
Gross’s process model of emotion regulation (Gross & Thompson, 2007) explains how individuals regulate their emotions, that is, how they modify, maintain, or suppress them to adapt to different situations. Emotion regulation involves controlling when and how, and the intensity and valence (positive/negative) of the emotion felt and expressed (Gross, 2002). ACEs have been linked to dysfunctional limitations in emotion regulation that persist throughout life, such as using fewer emotion regulation strategies, higher levels of nonacceptance of one’s negative emotions, and reduced emotional clarity (Gratz & Roemer, 2004).
ACEs within the household could signify unstable and invalidating caregiving environments during early development, and consequently, this disruption may hinder the formation of healthy emotion regulation skills (Burns et al., 2010; Morelen et al., 2016). ACEs, particularly recurrent trauma, interfere with the development of adequate emotional regulation and interpersonal abilities (Burns et al., 2010). In addition, they experience ERD, aggression, reduced social competence, and rejection by peers (Shields et al., 2001). ACEs can influence how a person perceives, interprets, and responds to emotional situations throughout life (Miu et al., 2022). ERD can often lead individuals to seek alternative coping mechanisms, such as SU, to manage overwhelming feelings (Weiss et al., 2022).
ACEs, Emotional Regulation, and Substance Use
ACEs significantly impact brain development, particularly on the hypothalamic-pituitary-adrenal axis (HPA), which regulates responses to stress (Nishi, 2020). Over-exposure to stress in childhood can lead to hyperactivity of this axis, making the individual more vulnerable to stress in adulthood (Van Bodegom et al., 2017). ACEs may also influence the way the nucleus accumbens (a set of neurons located within the prosencephalic cortical area) responds to stimuli (Teicher et al., 2016), which may predispose individuals to seek external rewards (such as SU) to compensate for under- or over-reactivity of the pleasure and reward systems (Michaels et al., 2021), attenuating negative emotions (Weiss et al., 2022). According to the theory of self-medication (Khantzian, 1997), psychoactive substances might be used as a form of self-medication to alleviate the effects of ACEs or distressing emotions or to regulate feelings when they are lacking or disordered as an attempt at self-regulation (Dassieu, 2019; Weiss et al., 2022).
ACEs can disrupt brain development and create deficits in the individual’s ability to cope with stressful or emotional situations, such as reduced cognitive flexibility (Kalia et al., 2021), poor self-regulation, and maladaptive coping strategies. These deficits can lead to an increase in SU or dependence, beginning in adolescence and continuing into adulthood (Sebalo et al., 2023; Trossman et al., 2021).
While some neurobiological and cognitive factors may explain the link between ACEs and SU, the socio-environmental factors also help to explain this relationship (Grummitt et al., 2021). ACEs increase the likelihood that a child will engage in SU if they experience at least one of these adverse experiences (Hughes et al., 2017), and the risk of developing SU in adulthood is even higher if the parents have a history of SU (Owais et al., 2021). Furthermore, if growing up with an SU parent increases the risk of the child becoming involved in these addictive behaviors, it also increases the risk for children to accumulate ACEs. Parents who actively use alcohol and other drugs often experience diminished parenting abilities (e.g., less supervision, more conflict), which further intensifies the already high-risk environment within the family (Neger & Prinz, 2015). Parental monitoring and parenting style were also found to be associated with the child’s later use of substances (Neppl et al., 2020).
ACEs, ERD, and SU in the Prison Population
Research has demonstrated that ACEs have lasting effects on both physical and mental health, leading to various challenges in adulthood, such as ERD and SU disorders (Grummitt et al., 2022; Poole et al., 2018) and aggression in adulthood (Almeida et al., 2024). This phenomenon is mainly present in prison populations (Crick et al., 2023). Numerous studies highlight that ACEs are an important risk factor for future antisocial behavior (Almeida et al., 2024; Basto-Pereira et al., 2022; Pires & Almeida, 2023). While 64% of the general U.S. population has encountered at least one ACE (Swedo et al., 2023), the percentage among the prison population (PP) is approximately 98%, with more than three-quarters reporting four or more ACEs (CPJ, 2024). Comparably, childhood adversity in individuals in the criminal justice system has been linked to more severe offenses and a higher likelihood of reoffending (Weber & Lynch, 2021).
When examining ACEs linked with criminal behavior, studies focus on juvenile offenders (e.g., Pires & Almeida, 2023) or adult offenders (e.g., Almeida & Costa, 2023). For example, sexual abuse in childhood elevates the risk of delinquency, violent behavior, and sexual offending (Kozak et al., 2018; Papalia et al., 2018). Due to intergenerational crime cycles, researchers estimate that 65% of individuals with a parent in prison as a child are likely to commit an offense at some stage in their lives (Murray & Farrington, 2008). Indeed, these results have been corroborated by the recent Compassion Prison Project (2024) study, showing that compared to the general population (GP), prisoners have 45% of a family prison history in childhood (vs. 8% for the GP). A systematic review including 49,163 prisoners found that ACEs can lead to antisocial behavior, and the low bonds between child and parents are associated with delinquency, as well as disruptive social learning models, where anger and aggression are seen as adequate coping mechanisms (Bowen et al., 2018).
Even though community violence (e.g., violence in the neighborhood) and collective violence (e.g., war) are understudied, an unsafe environment or a life-threatening situation can turn into a traumatic experience for a child or an adolescent, with lifelong consequences (Wyrick & Atkinson, 2021), being a risk factor for delinquency and criminal behavior in adulthood (Pickens et al., 2016). Experiencing violence outside the home is frequently reported among male offenders (Prasad et al., 2022). Among adolescents involved in the justice system, studies indicate a high rate of exposure to community violence and violent traumas (Loughran & Reid, 2019), which is a risk factor for reoffending in adulthood (Weber & Lynch, 2021).
Emotion regulation has also been studied as a link between ACEs and criminal or delinquent behavior. Indeed, ACEs can lead to psychological dysfunction and cognitive deficits such as social behavior, emotion processing, and emotional regulation (Bowen et al., 2018; Pflugradt et al., 2018). In adolescents with multiple ACEs, a lack of self-control was linked to early involvement in delinquent behaviors (Jackson et al., 2023). Offenders with higher levels of anger are more likely to commit violent offenses and are more prone to have ACEs (Ramirez et al., 2015). Studies with prisoners revealed that negative emotions were correlated with physical aggression and criminal behavior (Garofalo & Velotti, 2017). Lower levels of self-esteem, greater levels of emotional nonacceptance of one’s negative emotions, and the presence of hostility, as well as ERD, are related to physical aggression and anger (Garofalo et al., 2016). The lack of emotional awareness (or inattention to emotional responses) and limited access to emotion regulation strategies are associated with poorer anger control, with the use of more aggression and hostility (Velotti et al., 2017).
Some research has been conducted concerning the prevalence of SU in the PP, revealing high rates of SU among prisoners (e.g., Fazel et al., 2017; Kinyanjui & Atwoli, 2013). Studies demonstrate that approximately 65% of the PP in the USA has an active SU (National Institute on Drug Abuse, 2020). Concerning the type of illicit SU in prison, studies indicate that cannabis is largely reported, followed by sedatives or sleeping pills and amphetamines (Bukten et al., 2020; Carpentier et al., 2018). Regarding licit SU in prison, it is mentioned in only a small number of studies, whereas tobacco use ranges between 4% and 90%, according to a review of 59 studies worldwide (Carpentier et al., 2018). ACEs are associated with substance misuse in both genders of prisoners (Bowen et al., 2018). ACEs linked with SU have also been found to be a strong predictor of reoffending (Weber & Lynch, 2021). ACEs lead to psychological dysfunction, and SU can be used as a coping mechanism, as well as maladaptive antisocial behavior, leading to an interaction with the judicial system (Crick et al., 2023). Besides that, other studies found that imprisonment would create or exacerbate drug addiction, both during incarceration and upon release (Volkow, 2021; Western et al., 2019).
Regarding the literature review, this study aims to: (a) explore the association between ACEs, ERD, and SU; (b) compare the results of ACEs, ERD, and SU among French prisoners and the French general population; and (c) assess the predictors of ERD and SU in adulthood.
Method
Participants
The sample includes 203 adult participants, 129 women (63.5%) and 74 men (36.5%), aged between 18 and 92 (M = 28.4, SD = 11.5). Of the total sample, 143 (70.4%) belong to the French general population (GP). The remaining 60 (29.6%) participants were French individuals incarcerated in France.
The GP’s participants range in age from 18 to 92 (M = 26.9, SD = 11.5), including 26 males (18.2%) and 117 females (81.8%). Most were single (n = 124, 86.7%). Most participants indicated having a master’s degree (n = 56, 39.2%), followed by graduation (n = 47, 32.9%).
The age of the participants of the PP sample ranges from 18 to 65 (M = 32, SD = 11.1), including 48 males (80%) and 12 females (20%). Most of them are single (n = 53, 88.3%). The predominant education level is up to 12th grade (n = 54, 90%). Most of the participants have a judicial background (n = 45, 75%) with a prison history (n = 41, 68.3%), and 16 (26.7%) of them are recidivists. Concerning the penal facts, the majority serve prison sentences for personal injury (n = 20, 33.3%), followed by drug-related offenses (n = 12, 20%), followed by damaged property (n = 8, 13.3%). Five (8.3%) of the inmates were imprisoned for terrorist criminal association, and equally for traffic offenses. Six (10%) participants did not answer this question.
Measures
The Sociodemographic Questionnaire: The questionnaire evaluated sociodemographic factors such as sex, age, nationality, partner presence, education level, judicial background, and prison history. It also included questions regarding penal facts.
The Adverse Childhood Experiences International Questionnaire (ACE-IQ; World Health Organization, 2011; French version: Tarquinio et al., 2023) is a 29-item measure to assess ACEs. It refers to potentially traumatic events that occur in childhood (0–18). The instrument assesses thirteen ACEs categorized into three principal groups: child maltreatment (5 items; α = .50), family dysfunction (5 items; α = .67), and violence outside the home (3 items; α = .47). Response options for each item can be assessed on a dichotomous (i.e., yes/no), or 5-point Likert scale ranging from “always” to “never” (always; most of the time; sometimes; rarely; never), or a 4-point Likert scale ranging from “many times” to “never” (many times; a few times; once; never). The final scoring system can be either binary (score 1 for yes or no, depending on the question) or frequency (score 1 for once/many times or never, depending on the question). The frequency scoring system was used for the current study, and the final score ranges between 0 and 13. Internal consistency was demonstrated with an alpha coefficient of .73 for the frequency scoring of the overall questionnaire. Internal consistency Cronbach’s α has shown a coefficient of .86 for the whole questionnaire and each of its subscales: physical neglect (α = .77), domestic violence (α = .77), emotional violence (α = .66), physical violence (α = .56), sexual violence (α = .90), community violence (α = .87), collective violence (α = .75). The emotional neglect subscale was excluded from this study, because it revealed a low Cronbach’s coefficient (α = .50), as was the death/separation/divorce of parent’s subscale (α = .34).
The Difficulty in Emotion Regulation Scale (DERS-F; Gratz & Roemer, 2004; French version: Dan-Glauser & Scherer, 2013) is a 36-question comprehensive instrument that measures emotion regulation problems. The scale is divided into six factors: nonacceptance of emotional response, or the tendency to have an adverse secondary or non-accepting reaction to one’s own distress (α = .87), difficulties in adopting goal-directed behaviors, or the difficulty in concentrating and/or accomplishing tasks when experiencing negative emotions (α = .90), difficulties in controlling impulsive behaviors, or the difficulty remaining in control of one’s behavior when experiencing negative emotions (α = .87), lack of emotional awareness, which signifies the inattention to emotional responses (α = .80), limited access to emotion regulation strategies (α = .87), and lack of emotional identification or clarity, which reflects the extent to which an individual knows and is clear about his or her emotions (α = .74). Response options for each item can be assessed by a 5-point Likert scale, ranging from “almost never” to “almost always” (almost never; sometimes; half of the time; most of the time; almost always) which indicates the frequency of the behavior described in each item. Scores are presented as a total score and a score for each of the six subscales. Higher scores suggest more problems with emotion regulation. Internal consistency Cronbach’s α of the overall scale is high (α = .92). For the current study, internal consistency was demonstrated with an alpha coefficient of .93 for the overall scale and subscale of nonacceptance (α = .88), goals (α = .82), impulse (α = .85), awareness (α = .79), strategies (α = .88), and clarity (α = .78).
The Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST Questionnaire; WHO ASSIST Working Group, 2002; French version: Khan et al., 2011) is an eight-question questionnaire that identifies SU such as tobacco, alcohol, cannabis, cocaine, amphetamine-type stimulants, sedatives and sleeping pills, hallucinogens, inhalants, opiates, and other drugs. Response options for each question can be assessed on a dichotomous (yes/no), 3-point frequency scale ranging from “never” to “daily or almost daily,” or a 5-point frequency scale ranging from “never” to “yes, in the past 3 months.” The questionnaire has a high internal consistency for the total score with a Cronbach coefficient of .91. For the current study, the internal consistency was demonstrated with an alpha coefficient of .87.
Procedure
The data were collected from the GP using an online protocol distributed via social media (e.g., Facebook, Instagram, and LinkedIn). All participants accepted electronic informed consent.
To collect data from prisoners, authorization was requested from the Direction Interrégionale des Services Pénitentiaires (DISP). Each district chief of the prison center was then contacted to explain the study’s objectives, methodology, and data collection organization. All participants at the prison center were informed about the survey by prison staff or through flyers on the notice board, which had been approved by staff in advance. Voluntary participants sent letters to confirm their participation and have therefore been notified to participate in the study, individually or collectively. Data collection primarily occurred in groups, except for vulnerable prisoners and those in solitary confinement, who required individual data collection. All participants were informed about the nature of the study and signed an informed consent form, a separate document stating they could withdraw from the study without prejudice. The self-report protocol was completed using a paper-and-pencil format. To ensure participant anonymity, everyone placed their filled protocol into a neutral envelope that they sealed themselves. This sealed, neutral envelope was then placed into a larger kraft envelope containing the other sealed envelopes from the other participants. The kraft envelope was opened only at the end of the data collection process. This method of ensuring participant anonymity is inspired by secret ballot voting, in which each voter’s choice in an election or referendum remains anonymous both during and after voting. For technical reasons, kraft envelopes were used as the ballot box. The prison sample included adults serving sentences for various crimes at a prison center in southern France (e.g., sexual crimes such as rape and pimping; terrorist criminal association; property offenses such as violent robbery and theft; personal injuries including domestic violence, assaults, and homicide; drug-related offenses; traffic offenses) offenses). All the study participants were adult French nationals who could read and write French. The ethical issues underlying data collection were strictly respected, including participants’ anonymity. The study followed the ethical principles in the Declaration of Helsinki (World Medical Association, 2024) and was approved by the University’s Ethics Committee.
Statistical Analysis
The data was analyzed using the IBM Statistical Version SPSS v.29 program. First, Pearson correlations were performed between the scales and subscales to verify the relationship between the variables. Correlation values are assessed by r (.8 as large, .5 as medium, and .2 as small) and direction (positive/negative), as well as significance, which is assessed by “p” (p < .05 or p < .01) (Sullivan & Feinn, 2012). Then, ANCOVA tests were performed to examine differences between the GP and PP for each scale and subscale used in this study. Finally, multiple linear regressions were conducted to analyze the predictors of ERD and SU.
Results
Correlation Analysis
The results in the GP show small but significant correlations between some different instrument subscales (Table 1). Significant positive correlations are observed between the subscale ACE Total and the DERS subscales Nonacceptance of emotional response, Strategies, and DERS Total, which means that exposure to ACEs is associated with increased emotional regulation difficulties (ERD) in adulthood, particularly in accepting negative emotions and implementing effective strategies to regulate emotions. The subscale ACE Home Mental Health shows a positive correlation with DERS Nonacceptance and a negative correlation with DERS Awareness. This means that living with a mentally ill household member in childhood is associated with more difficulties in accepting one’s emotional response, but less difficulties with emotional awareness (the attention to emotional responses) in adulthood. ACE Emotional violence shows positive correlations with the DERS subscales Nonacceptance, Goals, Impulse, Strategies, and DERS Total, which means that exposure to emotional violence in childhood is associated with ERD in adulthood, particularly a greater nonacceptance of one’s emotional response, more challenges in adopting goal-directed behaviors, more difficulties in controlling impulsive behaviors and more limited access to emotion regulation strategies. ACE Sexual violence shows positive correlations with DERS Nonacceptance, DERS Strategies, and DERS Total, which means that suffering from sexual violence in childhood is also associated with ERD, in particular, a greater nonacceptance of one’s emotional response and more limited access to emotion regulation strategies in adulthood. Positive correlations exist between the ACE subscale of Bullying and the DERS subscales of Nonacceptance, Goals, Impulse, Strategies, Clarity, and DERS Total. This means that exposure to bullying in childhood is associated with more general ERD in adulthood, specifically a greater nonacceptance of one’s emotional response, more problems in adopting goal-directed behaviors, more difficulties in controlling impulsive behaviors, more limited access to emotion regulation strategies, and more lack of emotional identification or clarity. There are positive correlations between the ASSIST questionnaire and the ACE subscales Community violence, Collective violence, and ACE Total, meaning that exposure to ACEs is associated with more substance use in adulthood, particularly exposure to community violence and collective violence. The ASSIST questionnaire also shows positive correlations with the DERS subscales Nonacceptance, Goals, Impulse, Strategies, Clarity, and DERS Total. This means that ERD is associated with more substance use for individuals who experience the nonacceptance of one’s emotional response, difficulties in adopting goal-directed behaviors, difficulties in controlling impulsive behaviors, limited access to emotion regulation strategies, and lack of emotional identification or clarity.
Pearson’s Correlations Between the ACE, DERS, and ASSIST in the General Population (n = 143).
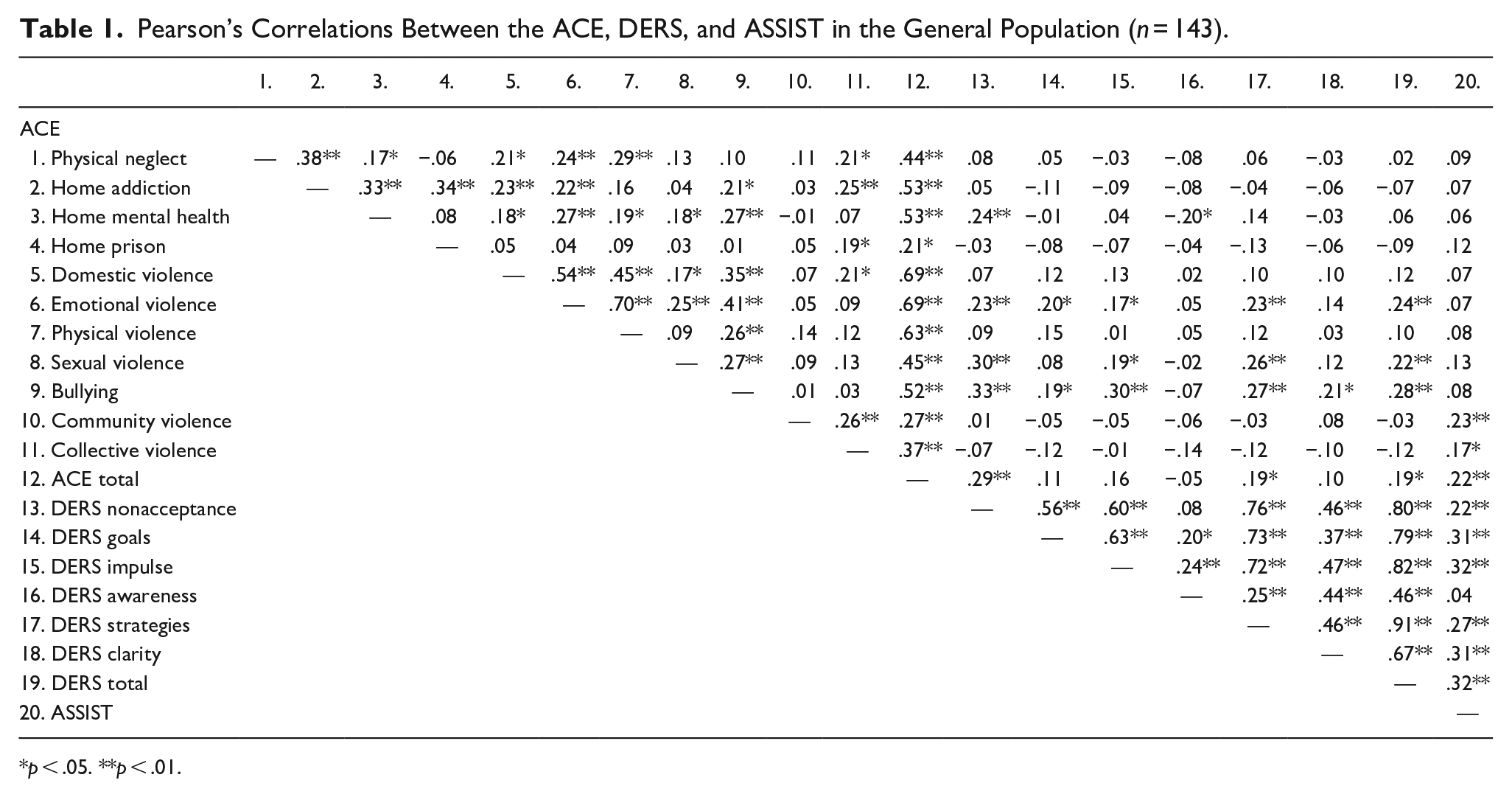
p < .05. **p < .01.
The results in the PP demonstrate small but significant correlations between some different instrument subscales (Table 2). A positive correlation is observed between the ACE Total and the DERS Nonacceptance of one’s emotional response, which means that ACEs are associated with a greater tendency to have an adverse secondary reaction or not to accept one’s distress in adulthood. Pearson’s correlations analysis demonstrates negative correlations between the ACE subscale of Home Prison and the DERS subscales of Strategies and Clarity. This means that growing up with an incarcerated household member is associated with less difficulty implementing effective strategies to regulate emotions and less lack of emotional identification or emotional clarity in adulthood. Finally, the data indicate positive correlations between the ASSIST questionnaire and the ACE subscales of Community violence, Collective violence, and ACE Total for the PP. This means that exposure to ACEs, particularly exposure to community violence and collective violence, is associated with greater substance use in adulthood.
Pearson’s Correlations Between the ACE, DERS, and ASSIST in the Prison Population (n = 60).
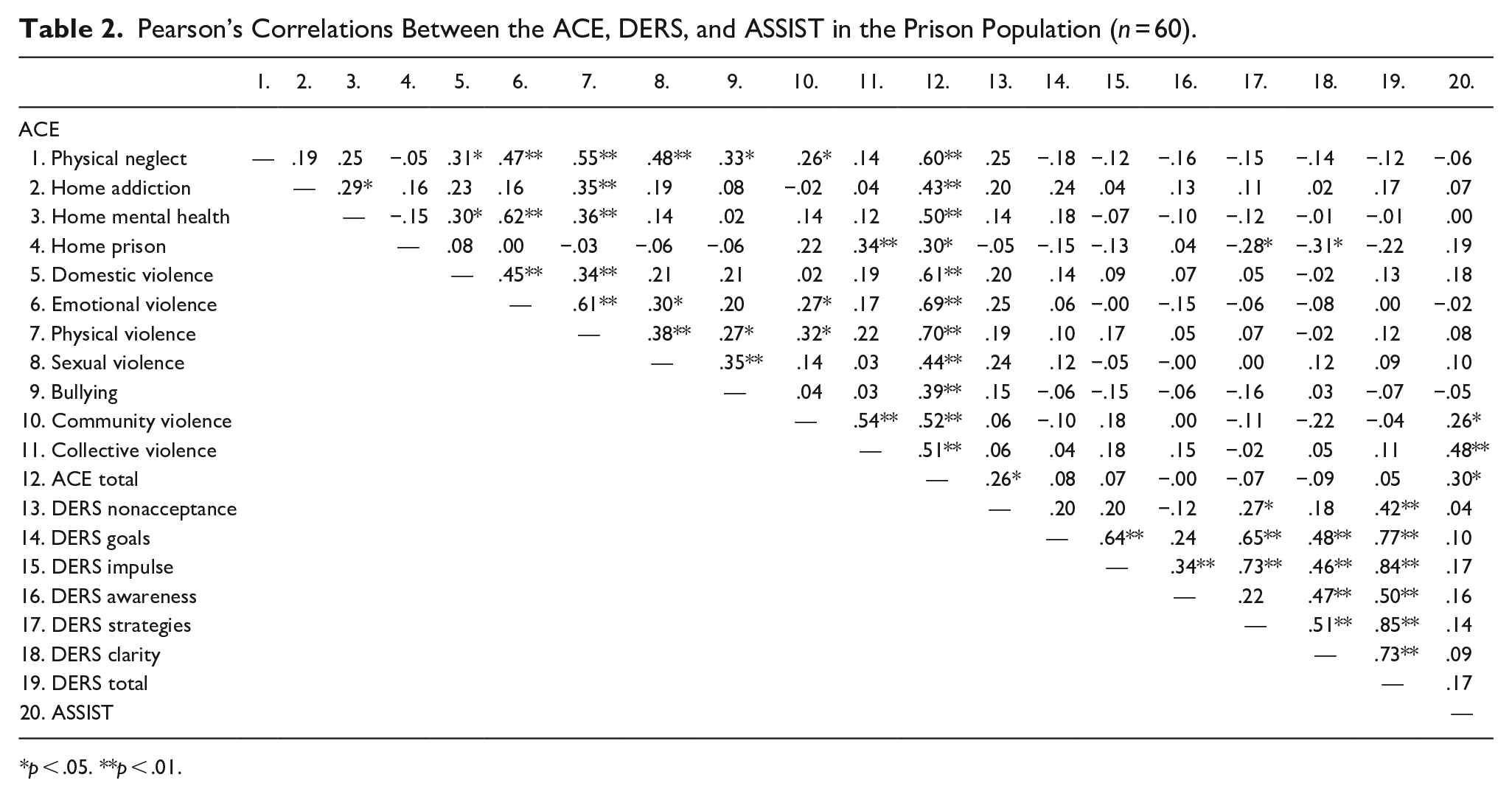
p < .05. **p < .01.
Group Difference
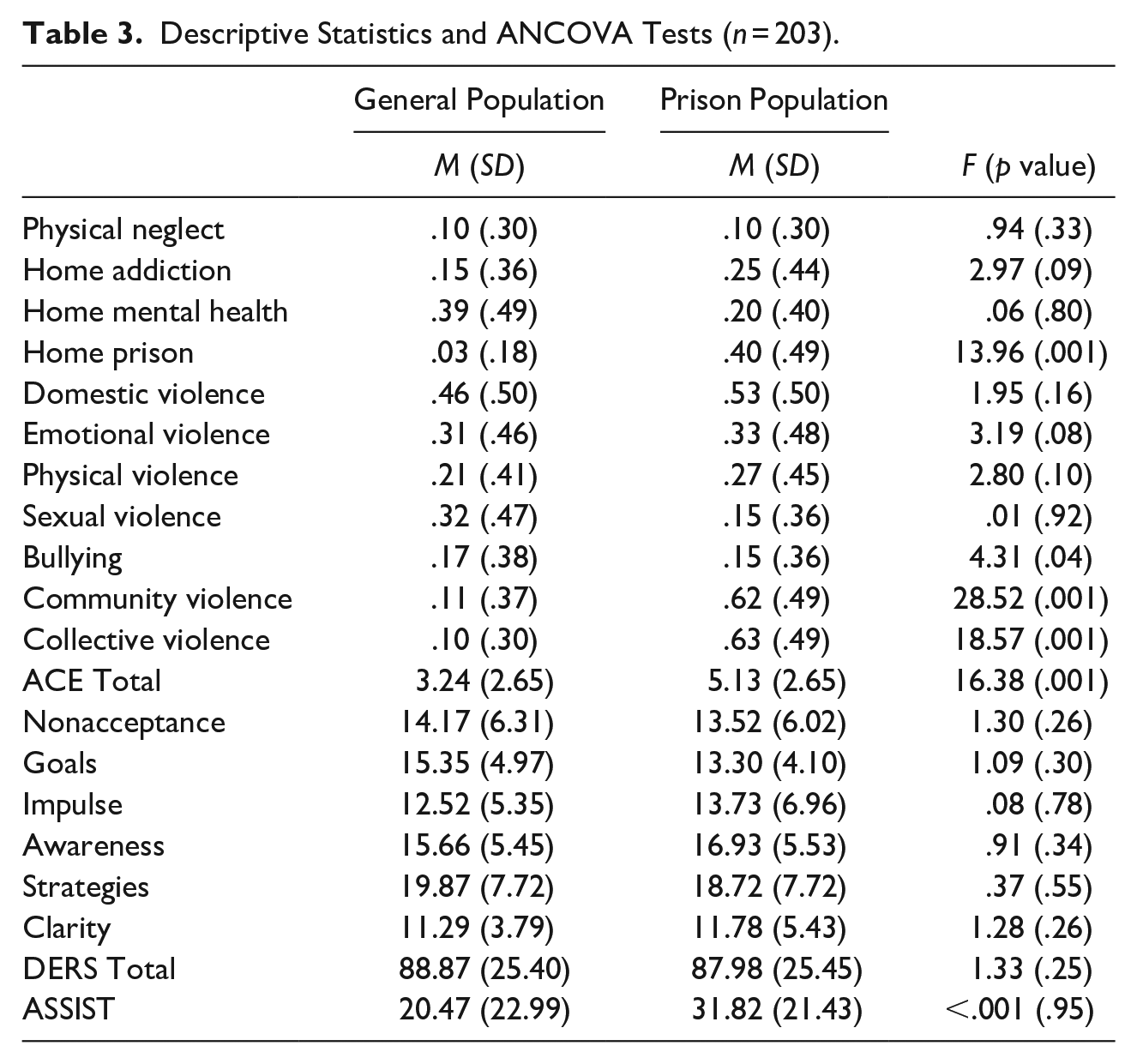
ANCOVA was conducted to compare the GP and PP samples (Table 3) while controlling for sex, age, the presence of a partner, and education level. Results showed that the GP participants experienced more bullying in childhood than the PP participants. The sample of individuals in prison scored significantly higher than the GP sample regarding the existence of an incarcerated household member in childhood, exposure to community violence, exposure to collective violence, and the total ACEs.
Descriptive Statistics and ANCOVA Tests (n = 203).
Regression Analysis
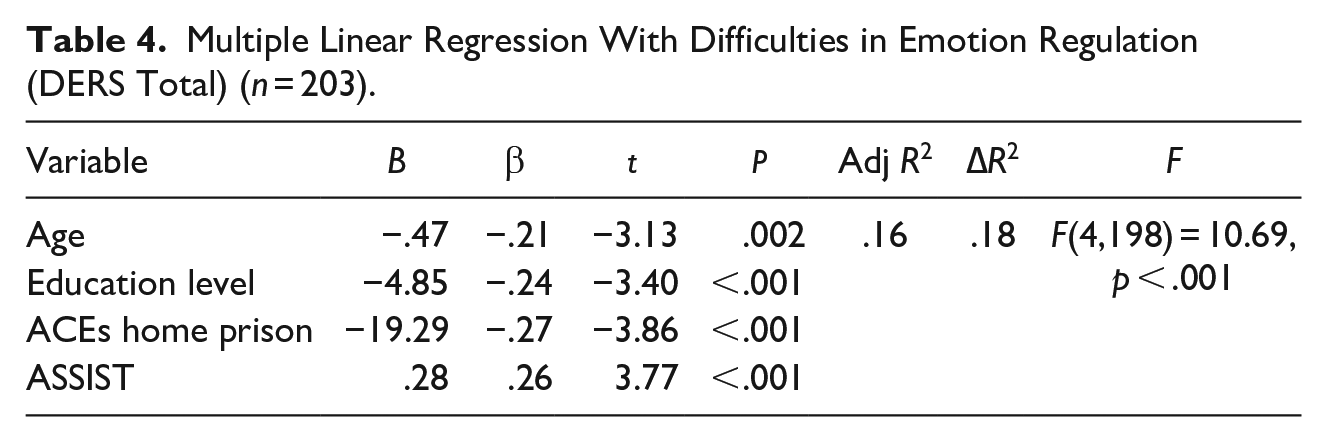
The explanatory model of ERD using a multiple linear regression showed that the model is significant [F (4,198) = 10.69, p < .001]. Durbin-Watson was 1.91, and VIF was < 2. The sex, presence of a partner or not, physical neglect, growing up with a drug-addicted household member, growing up with a mentally ill household member, exposure to domestic violence, emotional violence, physical violence, sexual violence, and bullying were not significant. For this reason, we performed a new model with significant paths. The model explains 16% of the variance of ERD. Age (β = −.21, p = .002), education level (β = −.24, p < .001), growing up with an incarcerated household member (β = −.27, p < .001), and SU (β = .26, p < .001) are significant predictors of ERD in adulthood (Table 4).
Multiple Linear Regression With Difficulties in Emotion Regulation (DERS Total) (n = 203).
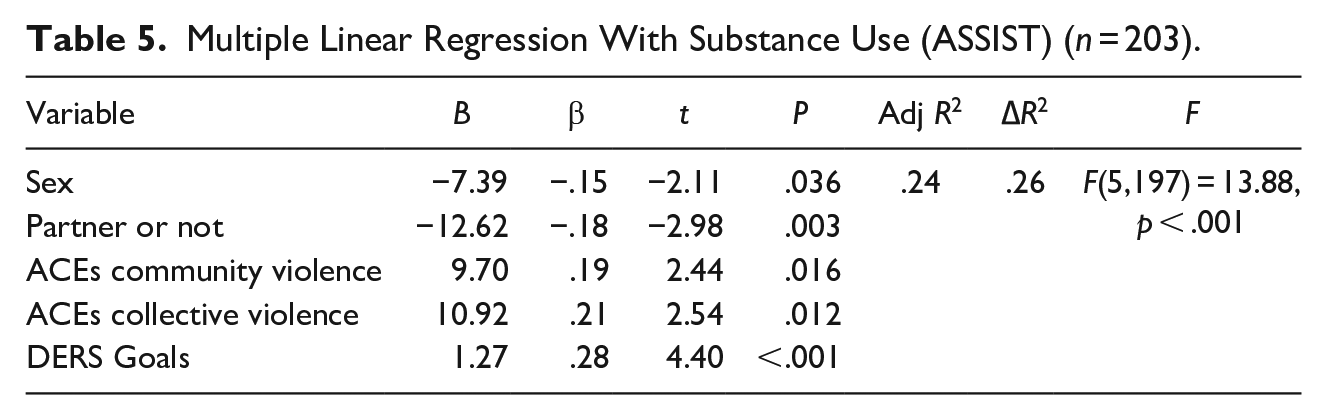
The explanatory model of SU using a multiple linear regression showed that the model is significant [F (5,197) = 13.88, p < .001]. Durbin-Watson was 1.84, and VIF was < 2. The age, education level, physical neglect, growing up with a drug-addicted household member, growing up with a mentally ill household member, growing up with an incarcerated household member, exposure to domestic violence, emotional violence, physical violence, sexual violence, bullying, nonacceptance of negative emotional response, difficulties in controlling impulsive behaviors, lack of emotional awareness, limited access to emotion regulation strategies, and lack of emotional identification or clarity were not significant. For this reason, we performed a new model with only significant paths. The model explains 24% of the variance of SU. Sex (β = −.15, p = .036), absence of a partner (β = −.18, p = .003), exposure to community violence (β = .19, p = .016), exposure to collective violence (β = .21, p = .012), and difficulty engaging in goal-directed behavior when experiencing negative emotions (β = .28, p < .001) are significant predictors of SU in adulthood (Table 5).
Multiple Linear Regression With Substance Use (ASSIST) (n = 203).
Discussion
Many associations have been observed between the ACE subscales, the DERS subscales, and the ASSIST questionnaire. In participants from the GP, living with a mentally ill household member in childhood was associated with more difficulties in accepting one’s emotional response (or the tendency to have an adverse secondary reaction to one’s distress) and more emotional awareness, which represents attention to emotional responses. The results align with previous research (Schumacher & Bassal, 2011) since a person who lives with a mentally ill relative takes the role of a caregiver, who is often emotionally affected by the situation of the sick relative and the surrounding duties. Also, for participants in the GP, our results indicated that exposure to emotional violence in childhood was associated with difficulties in emotional regulation. Namely, participants of this research who experienced emotional violence show greater nonacceptance of emotional response (Gratz et al., 2007) and more difficulties in adopting goal-directed behaviors, meaning difficulty in concentrating and/or accomplishing tasks when experiencing negative emotions (Oshri et al., 2015), more difficulties in controlling impulsive behaviors, or the difficulty remaining in control of one’s behavior when experiencing negative emotions (Liu, 2019), and more limited access to emotion regulation strategies (Gratz & Roemer, 2004). These findings show that abuse and dysfunction within the household may indicate an insecure caregiving environment during early development, which can impair the emergence of healthy emotion regulation skills (Burns et al., 2010).
Suffering from sexual violence in childhood was associated with more ERD among the GP, which corroborates previous research regarding the more limited access to emotion regulation strategies (Fernández-García et al., 2023). Specifically, more nonacceptance of the emotional response was found, in agreement with Gratz et al. (2007). An association between child sexual abuse and difficulties in controlling impulsive behaviors was also found in our study and corroborates the research of Liu (2019). The effects of ACEs may persist throughout life, especially in the absence of care, whether psychotherapeutic or judicial (Sadlier, 2021).
In the GP, suffering from bullying in childhood was associated with more ERD in adulthood, which matches previous findings (Adrian et al., 2019), specifically the greater lack of emotional identification or clarity, which reflects the extent to which an individual knows and is clear about his or her emotions (Levantini et al., 2023). Bonds with peers represent a continuation of the attachment to the family, and social relationships are essential to the proper functioning of a human being. Such impaired social interaction and unsafe environments can lead to ERD (Bäker et al., 2023).
Overall, more ACEs in the GP were associated with more ERD, which aligns with previous studies (Miu et al., 2022) that point out more limited access to emotion regulation strategies (Gratz & Roemer, 2004). The link between ACEs and ERD has demonstrated that maltreatment leads to maladaptive social learning (Miu et al., 2022), harmful parenting practices (Morelen et al., 2016), and affective lability (Almeida et al., 2023). On the other hand, among prisoners, there were significant negative correlations between ACE and ERD. Those who experienced growing up with an incarcerated household member in childhood experience less limited access to emotion regulation strategies and less lack of identification or emotional clarity. Additionally, our outcomes also show that growing up with an incarcerated household member in childhood showed decreased ERD, and no differences were identified regarding ERD between the GP and the PP. These results are not in line with previous findings (Di Piazza et al., 2017) and may be explained because those who are exposed to more complex emotional situations and more intense trauma experiences, like prisoners (Almeida & Costa, 2023), may develop post-traumatic growth—a capacity to triggers for positive change facing traumatic experiences—which could lead to an emotional adjustment (Tedeschi & Calhoun, 2004). Moreover, those who have grown up with incarcerated parents may receive external support from Social Services or family members (Miller, 2007), which can help develop emotional regulation.
More ACEs were associated with greater SU, corroborating previous research (Crick et al., 2023). Specifically, more community and collective violence was associated with more SU, both in the GP and in the PP. This could provide a clue to understanding that SU may be a maladaptive coping mechanism for dealing with ACEs (Sebalo et al., 2023). Those who have been exposed to trauma are particularly vulnerable to developing SU disorders (Jacobsen et al., 2001). Psychoactive substances might be used as a form of self-medication to alleviate the effects of trauma as an attempt at self-regulation (Dassieu, 2019). Also, in both samples, the SU was associated with more ERD, corroborating the study by Weiss et al. (2022). More SU was associated with more difficulties in controlling impulsive behaviors (Kale et al., 2018), more lack of emotional clarity (Stellern et al., 2023), and more limited access to emotion regulation strategies (Weiss et al., 2022). Individuals struggling with regulating emotions might be more disposed to SU to cope with or escape negative emotional states (Baker et al., 2004).
Concerning the group differences, our results showed that the GP participants scored significantly higher exposure to bullying as victims. The study of Renda et al. (2011) indicates that youth who engage in bullying as perpetrators are at a significantly higher risk of developing antisocial behaviors later in life. Involvement in bullying was not only related to increased aggression and social impairment but also predicted a greater likelihood of future interactions with law enforcement or the judicial system.
The results of this study demonstrate differences between the GP and the PP regarding the incarceration of a household member in childhood, as observed in previous studies (CPJ, 2024). In addition, families affected by imprisonment often face more difficult living conditions (e.g., precarity and social isolation), which can lead to children engaging in risky and antisocial behavior (Bowen et al., 2018). Regarding exposure to community violence and collective violence in childhood, PP also scored higher. Male offenders frequently report this type of adverse childhood experience outside the home, and it is almost twice as often in recidivist violent offenders (Prasad et al., 2022). Witnessing violence strengthens this belief, leading them to see aggression as a justified method for handling conflicts (Cooley-Strickland et al., 2009). Our results showed that PP scored significantly higher regarding the number of ACEs. Indeed, ACEs cause long-term impacts on physical and mental health, leading to various issues in adulthood (Almeida et al., 2023, 2024; Grummitt et al., 2022) and increasing criminal behavior (Almeida & Costa, 2023).
Regarding SU, the results of this research did not emphasize a statistical difference between the GP and the PP, which does not corroborate previous findings (Bronson et al., 2017). This inconsistency may be due to the carceral context and limited substance access. Another explanation lies in the fact that prisoners tend to potentially under-report their drug use for fear of punitive measures from the institution.
Our study’s results indicated that age impacts emotional regulation. Chaudhary et al. (2023) demonstrated that ERD diminishes with age. They suggest that aging leads to changes in cognitive and affective functions, accompanied by decreased reactivity to intense emotional stimuli and/or improved emotional regulation. Education level also affects emotional regulation, suggesting that the higher the level of education, the lower the ERD. Those with more studies often face high academic demands that can generate significant stress, and they implement emotional regulation strategies to prevent the emotional and mental exhaustion associated with these pressures (Supervía & Robres, 2021).
The results of our study indicate that sex affects SU, as highlighted in the studies by Fonseca et al. (2021). The authors point to a higher prevalence among men, although this may vary according to culture. In general, men often have easier access to substances, but there is no clear consensus on the specific types of drugs consumed by each gender. In addition, gender-specific biological, psychological, and social factors may influence the development, persistence, and treatment of SU disorders (Fonseca et al., 2021). The results of the current study also showed that the absence of a partner is a predictor of SU. It is recognized that SU is often linked to interpersonal dynamics, particularly in a social context such as peer influence, which can increase SU (Mbatia, 2023).
Limitations
This study presents some limitations that must be acknowledged. One of them is that the sample of the PP is smaller than the GP sample, and we have an over-representation of men among the PP and women in the GP sample, which may influence the results. Moreover, for the PP sample, some responses may be altered due to the potential fear of being honest about SU reporting. Furthermore, the prison context can alter results, as prison conditions (such as isolation or deprivation of liberty) change how prisoners manage their emotions. Another limitation is that the online study has no control over the environment in which participants respond. In addition, the self-report format of the ACE-IQ questionnaire does not allow for a deeper exploration of the issues. This limitation could be overcome through interviews with the participants. The self-report format of the DERS-F and ASSIST questionnaires may cause bias regarding the person’s awareness of their difficulties or problems, and it should be considered in future research. Finally, since the study is cross-sectional, it is subject to the associated biases.
Conclusion
This study enhances our understanding of the relationship between adverse childhood experiences (ACEs) and their impact on emotional regulation difficulties (ERD) and substance use (SU) in adulthood, contributing to the fields of psychology, health, and criminal justice. Based on our findings, it is essential to raise awareness about ACEs, develop early interventions for violence, and promote psychological support in schools and communities to mitigate the likelihood of adverse outcomes in adulthood. Professionals can improve the detection of at-risk people by focusing on vulnerability factors. Programs such as anger management training (Tryastuti, 2021) may help prevent emotional issues in children who have experienced this type of victimization. Schools and communities must recognize the importance of identifying children suffering from all forms of abuse and referring them to appropriate support services.
It is also essential to strengthen mental health services in prisons by incorporating psycho-educational and resilience-building components (Alleaume et al., 2023) to help prisoners better understand and cope with their past experiences. Cognitive-behavioral therapy that focuses on ACEs, emotional regulation, and addiction should also be prioritized (Graziani & Romo, 2013). Psychologists, educators, and probation officers require training to recognize the signs of ACEs, allowing them to provide the best possible support and guidance to vulnerable individuals. To effectively address collective and community violence, a comprehensive strategy is necessary, integrating prevention, intervention, rehabilitation, and long-term support. This approach requires collaboration among local communities, governments, and civil society. Key initiatives may include fostering dialogue and cooperation to alleviate social tensions (through collective projects and/or sports) and training community leaders and mediators for conflict management (Marlière & Fontaine, 2011).
Footnotes
Acknowledgements
The authors would like to express their gratitude to all the participants who voluntarily provided information for this study, the DISP, and the French national prisons who consented to participate.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CiiEM has provided support through Project 10.54499/UIDB/04585/2020, funded by FCT (Foundation for Science and Technology).
Ethical Approval
The Egas Moniz School of Health & Science Ethics Committee approved the research (N. 1413).