
Abstract
Adverse childhood experiences (ACEs) and mental health issues are highly prevalent in the history of adult offenders, as they affect an individual’s social, psychological, and emotional development and, consequently, their welfare and role in society. The present study explores the relationship between ACEs and mental health in adult offenders. B-on, Psycnet, Pubmed, Scielo, Scopus, and Web of Science databases were systematically searched and selected according to the inclusion and exclusion criteria. Twelve articles were included in the final sample, exploring the relationship between ACEs and mental health in adult inmates. ACEs impact criminal conduct and mental health. The study of those variables is essential to contribute to implementing intervention strategies and crime prevention.
Keywords
Introduction
Adverse childhood experiences (ACEs) are potentially traumatic events that occur during childhood and can be stressful to an individual’s health, which include neglect, physical, emotional, and sexual abuse, living in a dysfunctional household, substance dependence, and having a family member in prison. An unstable family environment, the death of a parent, substance abuse by a close relative, mental illness, or parental separation during childhood, among other potentially traumatic situations, have also been considered risk factors for future criminal behavior (Marques, 2020) as offenders are more likely to have higher rates of adverse childhood experiences than the general population (Basto-Pereira et al., 2016). There is a high prevalence of different types of victimization in offenders (Wemmers et al., 2017; Wojciechowski, 2020), and inmates tend to show more experiences of ACEs than the general population (Almeida & Costa, 2023). Although it is not enhanced how ACEs occurring in childhood influence an individual to commit a crime, these ACEs can have an impact on criminal behavior and mental health (Marques, 2020; Matos, 2019). A recent systematic review showed that having a specific activity routine in unsafe neighborhoods by putting participants close to motivated offenders increases the risk and frequency of victimization and consequently promotes the adaptation of deviant behaviors (Pires & Almeida, 2023).
Mental welfare encompasses how people feel and cope with their daily lives, and there is an increased risk of mental health issues and self-harming behaviors in incarcerated individuals (Marques, 2020). Prison populations have a high prevalence of mental illness (Sirdifield, 2012), and a considerable percentage experience comorbidity of mental health issues and adverse childhood experiences. Studies have shown that those with mental illness have higher re-arrest rates and are more likely to replicate violent behaviors (Skeem et al., 2014). Prisoners often present multiple and complex health needs, and their mental health and well-being can have a negative effect due to experiencing isolation and lack of privacy (Konrad et al., 2007).
There has been an increased rate of self-harm in the male adult prison population in England and Wales, where there were reported over 43,000 incidents in 2018, with a total of 54% within 1,000 incarcerated individuals (Ministry of Justice, 2019). In American jails, suicide is the leading cause of death, which is approximately three times higher rate in jails when compared to the general population (Calli & Jared, 2024). In the European panorama, Portugal is one of the countries with the highest suicide rate. According to the report for 2022 (Aebi et al., 2022), the suicide rates in Portuguese prisons are high, with scores between 5.1% and 25% higher than the European median value.
Researchers suggest that ACEs are also risk factors for poor mental health in adulthood (Marzano et al., 2011). The adverse outcomes of these experiences increase the outcomes according to the number of ACEs types experienced. Therefore, a secure relationship between mental health and ACEs can be identified, along with deviant behaviors leading to criminal justice involvement (Hughes et al., 2017). Additionally, homelessness, low education, being on remand, and serving a life sentence are risk factors for self-harm and suicidal behaviors that influence these rates (Pope, 2018).
James and Glaze (2006) reported that, in 2006, more than half of male and female prisoners expressed mental health issues, and almost 25% of this population had revealed a history of physical or sexual abuse. Within these mental health problems, it is typical to endorse five or more symptoms of major depressive disorder, symptoms of mania, and reporting delusions and hallucinations. The mental illnesses are often unrecognized and untreated (Brooker & Glyn, 2012). Ford et al. (2020) stated that offenders reporting multiple ACEs were more prone to have poor mental health. A survey of incarcerated men revealed that almost half of the sample disclosed a chronic mental illness, and nearly a third revealed lifetime suicide attempts and self-harm. Increased risks of chronic mental illness and suicide attempts were identified in participants who had experienced four or more ACEs during childhood. In contrast, risks were even higher for those who experienced two or more ACEs during childhood. In essence, prisoners who experienced four ACEs or more were 15 times more prone to have lifetime self-harm and 8 times more prone to attempt suicide in prison settings. Inmates who experienced multiple ACEs are more prone to engage in self-harm behavior and mental illness under confinement (Ford et al., 2020).
Offenders also face diverse adversities in mental health services while in an incarcerated environment, where there is a lack of appropriate conditions for those with complex health needs (Bradley, 2009). According to James and Glaze (2006), a small number of prisoners with mental health issues receive mental health treatment at the jail and take prescribed medication. Due to this disproportionately high prevalence of mental disorders among this population, there should be easy access to health care in the criminal justice system (Fazel & Seewald, 2012).
There is a higher frequency of psychiatric issues in older prisoners, compared to the younger ones, with comorbid mental illnesses, including psychoses, dementia, depression, and a psychiatric disorder. This includes psychotic and mood disorders, substance use, personality, and neurodevelopmental disorders. It is suggested that these results may be a consequence of the prison environment and the traumatic and stressful experiences (Haesen et al., 2019). In their study, Ignatyev et al. (2019) identified that more than half of inmates had one mental health problem. Among those, a high percentage has shown three or more mental disorders, with antisocial and borderline personality disorders and anxiety disorders. A cross-sectional review of the Mental Health in the Prison Population has shown the pervasiveness of mental disorders within incarcerated individuals. Offenders reported a high rate of major depressive disorder, anxiety disorders, and a risk of suicide. Comorbidities are also frequent; nearly half of the sample presented two or more substance abuse or psychiatric disorders. This sample was compared to a general population sample, demonstrating a significantly higher prevalence of mental health disorders in an offender population (Fovet et al., 2020). Other studies indicate that inmates, compared to the general population, have higher values of substance abuse (Pflugradt et al., 2017), mental illness (Tyler et al., 2019), and higher levels of emotional lability (Almeida et al., 2024).
Although there are studies that present outcomes of ACEs in the inmate population or the general population, comparative studies between these populations are scarce. Studies about mental health highlighted that there is often a high range of offenders who experience mental illnesses and are not given the proper healthcare access treatment while on probation (Fazel & Seewald, 2012). Mental health care for individuals incarcerated is a challenge. One primary factor is the limited resources within prisons, leading to a shortage of mental health professionals, insufficient funding for programs, and inadequate staff training (Weil, 2015). Compounding this problem, the pervasive stigma surrounding mental health issues arises, both within society and specifically within correctional settings. This stigma can result in a lack of awareness and understanding of the prevalence and severity of mental health conditions among inmates, further contributing to the insufficient attention and care they receive (Lamb & Weinberger, 2001). The high rates of incarceration of individuals with pre-existing mental health conditions exacerbate the demand for mental health services within prisons. Screening and assessment processes during intake may also be insufficient, leading to undiagnosed or untreated mental health issues. A lack of continuity in mental health care is often experienced by inmates transitioning between prisons or upon release (Priebe et al., 2008). Furthermore, the punitive nature of correctional systems historically places a greater emphasis on punishment than rehabilitation, potentially neglecting the mental health needs of those in custody and perpetuating a cycle of reoffending (Lamb & Weinberger, 2001).
Thus, this systematic review aimed to analyze and synthesize the literature, exploring the relationship between ACEs and mental health in adult offenders. The objective is to conduct a comprehensive synthesis of existing research, seeking not only to identify patterns and correlations but also to extract actionable insights that can significantly impact the development of targeted intervention strategies. Through a meticulous analysis of selected articles, our synthesis endeavors to provide a robust foundation of knowledge. This foundation is poised to inform various facets of the field, including shaping the trajectory of future research endeavors, guiding the formulation of evidence-based policies, and influencing the design of practical interventions. By explicitly addressing the intricacies of ACEs and mental health among adult inmates, our systematic review seeks to advance scholarly discourse and empower practitioners, policymakers, and researchers with valuable insights that can drive positive change in criminology and mental health. By addressing this gap in the literature, it aspires to provide valuable knowledge that can guide future research, policy development, and practical interventions in the field.
Method
Eligibility Criteria
The present systematic review includes studies that incorporate samples of incarcerated adults. The studies included were published between 2007 and 2022. This systematic review considers the ACEs definition by most of the researchers, including experiencing emotional abuse, sexual abuse, physical neglect, low family economy, living in a dysfunctional family, witnessing violence, and the presence of a convicted family member (Wolff & Caravaca Sánchez, 2020). Studies also explored the definition of mental illness, whereas most research presented a common aspect of these individual’s health and life experiences (e.g., Ford et al., 2020; Hilton et al., 2019; Messina, 2022). We included studies: (1) published in English; (2) with a sample equal to or higher than 18 years of age (age of adulthood in some countries); and (3) that analyzed the link between ACEs and mental health in samples of offenders.
Information Sources and Search Strategy
Scientific articles were searched through six databases: B-on, PsycNet, Pubmed, Scielo, Scopus, and Web of Science with the terms “(offender or inmate or prisoner or incarcerated)” AND “(adverse childhood experiences or ACE),” AND “(mental health or mental illness or mental disorder or psychiatric illness).” The research results in 370 articles.
Data Management and Selection
The selection process of the articles comprised in this study is shown in Figure 1. Articles were reviewed in the following order: title, abstract, and full text. Three hundred seventy articles were identified through the database search. After removing duplicated articles, 220 were established. Posteriorly, titles and abstracts were screened, which led to a total of 19 articles. The inclusion criteria previously stated were implemented in these articles, resulting in the final 12 articles. Data extraction contained: (1) adolescent population samples; (2) non-offending samples; (3) not measuring adverse childhood experiences and mental health; (4) not being written in English; and (5) not being a scientific article.
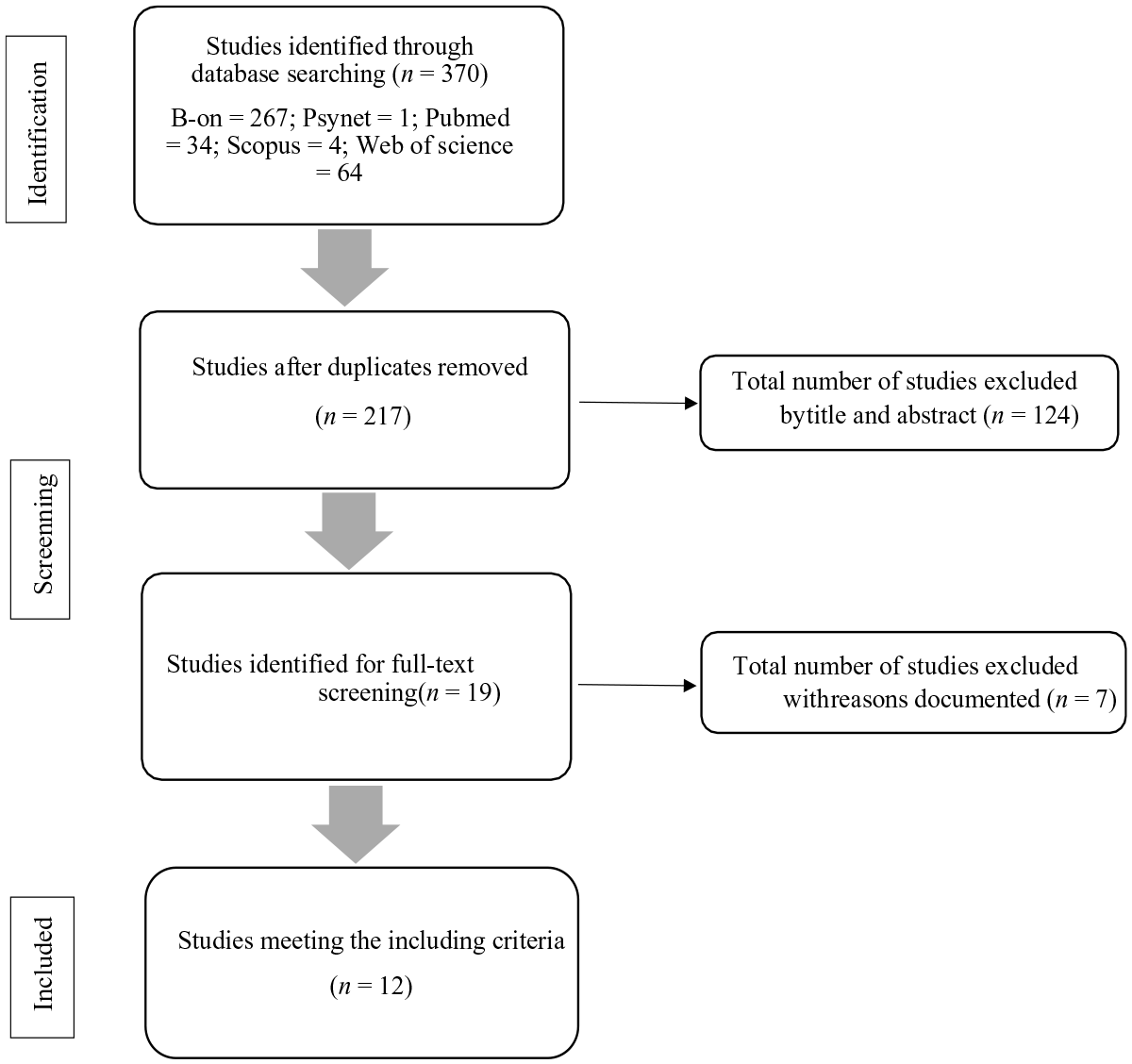
Flow diagram of the studies selection.
The authors independently extracted data from articles that meet the inclusion criteria. Discrepancies were discussed until a mutual agreement. The reliability of the agreement between the authors was assessed based on the standard criteria of Cohen’s kappa statistic. Interpretation of the kappa statistic (κ) for the inter-rater agreement was: <.20 (slight), .21 to .40 (fair), .41 to .60 (moderate), .61 to .80 (good), and >.81 (excellent; McHugh, 2012). The reliability of the agreement between the authors is excellent (.83).
Results
Study Sample
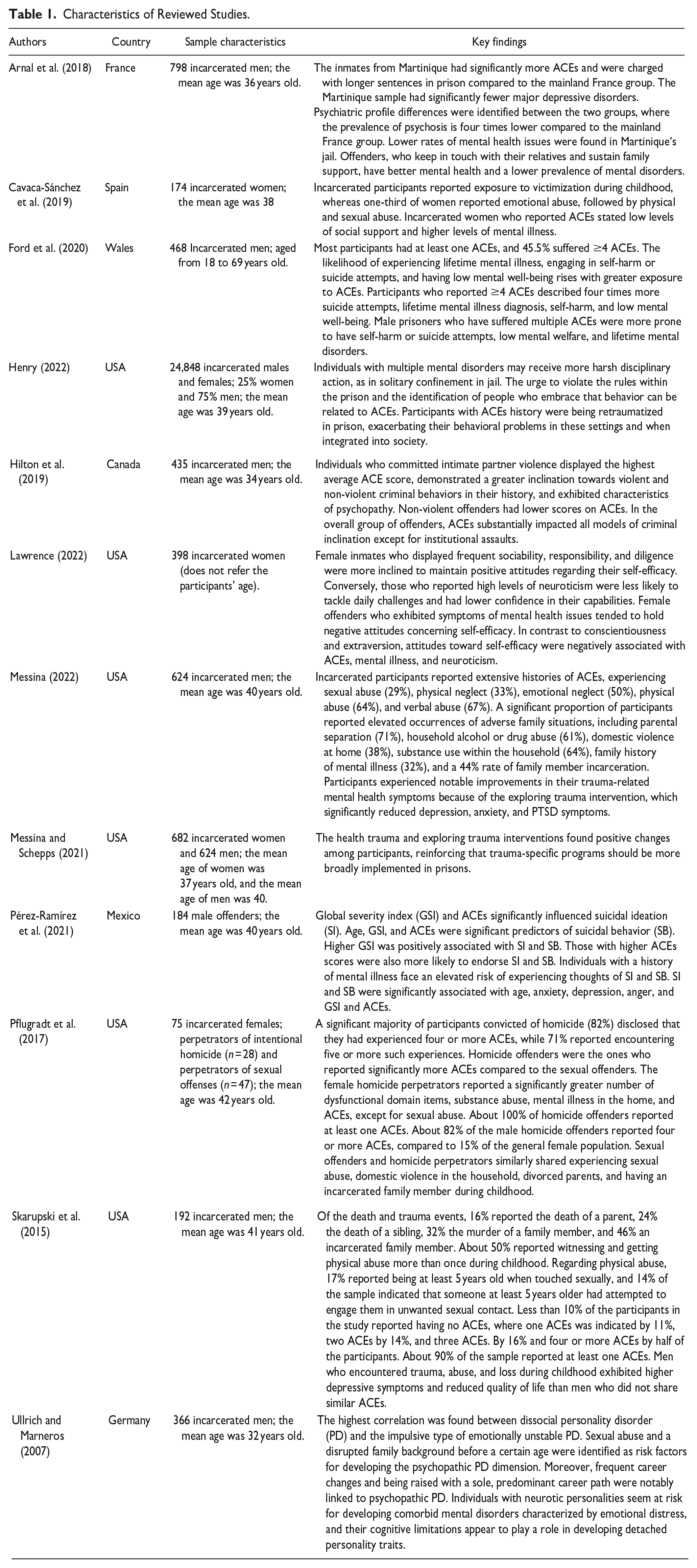
The studies comprised a total of 29,244 inmates. The characteristics of each sample, the country, and the key findings are described in Table 1. The samples differed in sex, age, and size. Participants were adults with ages greater or equal to 18 years old. Of the total studies, two comprised samples of female and male participants, three focused on female inmates, and seven focused on male inmates. The smallest sample size matched the number of 75 participants (Pflugradt et al., 2017), and the study with the largest sample size matched the number of 24,848 participants (Henry, 2022). Additionally, one of the studies focused on a sample with both sexual offense and intentional homicide perpetrators (Pflugradt et al., 2017), while the others integrated offenders with diverse types of aggression. Of the 12 studies, 6 were performed in the United States of America (e.g., Henry, 2022; Lawrence, 2022; Messina, 2022), 1 was conducted in France (Arnal et al., 2018), 1 in Spain (Caravaca-Sánchez et al., 2019), 1 in Mexico (Pérez-Ramírez et al., 2021), 1 in Canada (Hilton et al., 2019), 1 in Germany (Ullrich & Marneros, 2007), and 1 in Wales (Ford et al., 2020).
Characteristics of Reviewed Studies.
Study Design
Most studies were conducted quantitatively (n = 9), and one followed a mixed-method approach (3). The data were collected via individual interviews in prison facilities (n = 1), secondary data analysis (n = 3), self-administered questionnaires (n = 8), archival methods (n = 1), and group programs (n = 1).
Measures of Adverse Childhood Experiences and Mental Health
The assessment of ACEs in these studies was conducted using the Childhood Trauma Questionnaire (CTQ-28; Bernstein et al., 1994). Several instruments were used to assess mental health. Depression was measured using five different assessment tools: the Depression Anxiety Stress Scales (Lovibond & Lovibond, 1995), the PHQ Depression Subscale (Kroenke & Spitzer, 2002), the Patient Health Questionnaire (PHQ-9; Kroenke & Spitzer, 2002), the Centers for Epidemiologic Studies Depression Scale (CES-D; Irwin et al., 1999; Kohout et al., 1993), and the Columbia Suicide Severity Rating Scale (C-SSRS; Posner et al., 2011).
In eleven studies (e.g., Lawrence, 2022; Pérez-Ramírez et al., 2021; Ullrich & Marneros, 2007), mental health was assessed using additional instruments: the Consensus Clinical Global Impression (CGI; Kadouri et al., 2007), Short Warwick-Edinburgh Mental Wellbeing Scale (SWEMWBS; Stewart-Brown et al., 2009), General Self-Efficacy Scale (Sherer et al., 1982), Mini IPIP (Donnellan et al., 2006), modified versions of the Short Screening Scale for Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1994), PTSD (Breslau et al., 1999), Patient Health Questionnaire (PHQ-9; Kroenke & Spitzer, 2002), ICD-10 (IPDE; Loranger et al., 1997), and Schedules for Clinical Assessment in Neuropsychiatry (Aboraya et al., 1998), and the Psychological Distress Scale (K6; Kessler et al., 2002).
Four different instruments assessed anxiety in four studies (e.g., Caravaca-Sánchez et al., 2019; Messina, 2022). These instruments include the Depression Anxiety Stress Scales (Lovibond & Lovibond, 1995), PHQ Anxiety Subscale (Spitzer et al., 1999), Patient Health Questionnaire Anxiety Subscale (Spitzer et al., 1999), and Level 2 Anxiety—Adult (Schalet et al., 2016) of the PROMIS Anxiety Short Form.
Aggression was measured in two studies (Messina, 2022; Messina & Schepps, 2021) using the Buss–Warren Aggression Questionnaire (AQ), formerly known as the Buss-Perry AQ (Buss & Warren, 2000).
Group Differences in Adverse Childhood Experiences and Mental Health
Hilton et al. (2019) found that the scores of ACEs varied among different types of offenders. Intimate partner violence offenders had similar ACE scores to non-intimate partner violence offenders but scored higher than nonviolent offenders with no current or prior violent charges. Pflugradt et al. (2017) reported that 25% of the sexual offenders surveyed reported no ACEs. In contrast, 100% of the homicide offenders had experienced at least one ACEs, with 72% reporting five or more ACEs and 82% reporting four or more. Female perpetrators of homicide scored significantly higher on ACEs than the general female population, particularly in areas such as physical, emotional, and verbal abuse, substance use, emotional neglect, and having a family member with mental illness.
When comparing homicide and sexual offenders, Pflugradt et al. (2017) found that homicide offenders endorsed higher ACEs in various types of abuse and neglect, except for sexual abuse. Homicide offenders also reported significantly higher dysfunction related to having a family member with mental illness and substance use.
According to Henry (2022), certain types of adverse experiences were more likely to be reported by men, including neglect, verbal and physical abuse, and having a family member in incarceration. On the other hand, women tended to report higher rates of sexual abuse and mental illness within the household. Both men and women reported similar rates of domestic violence, parental separation or divorce, emotional abuse, and substance use in the home.
Higher ACE scores were associated with an increased likelihood of engaging in suicidal behaviors and experiencing suicidal ideations, as Pérez-Ramírez et al. (2021) found. These findings suggest that individuals who have experienced higher levels of trauma may be more susceptible to developing psychiatric problems, which can contribute to their involvement in the justice system.
Men who reported experiencing multiple ACEs scored lower in quality of life and exhibited depressive symptoms than men who did not report similar experiences, as demonstrated by Skarupski et al. (2015). Additionally, prisoners had higher rates of mental illness diagnoses, self-harm, and suicide attempts than the general population, according to Ford et al. (2020). These findings highlight the significant impact of adverse experiences on mental health outcomes and the increased vulnerability of individuals within the prison system.
Relationship Between Adverse Childhood Experiences and Crime
All the studies reviewed have consistently indicated that an individual’s early life experiences significantly impact cognitive, emotional, social, and physiological functioning. More than half of the study participants reported experiencing at least one ACEs, highlighting the widespread prevalence of such events (Pflugradt et al., 2017; Skarupski et al., 2015).
Physical abuse, emotional abuse, the death or incarceration of a parent, and physical or sexual abuse emerged as the most reported childhood adversities across the studies (Henry, 2022). The accumulation of early trauma increased the likelihood of persistent engagement in criminal behavior, demonstrating a strong association between ACEs and criminal involvement (Ford et al., 2020). The pervasiveness of childhood trauma was high among incarcerated females and males, with more than half of the prison population reporting at least one ACEs (Pérez-Ramírez et al., 2021).
Relationship Between Mental Health and Crime
Ullrich and Marneros (2007) conducted a study highlighting the significance of personality disorders as a risk factor for developing criminal behavior. Their findings underscore the importance of considering personality disorders in understanding and addressing the complexities of criminal involvement and mental health issues among offenders. Hilton et al. (2019) found that mental illness is prevalent among offenders receiving psychiatric treatment in forensic hospitals and that the rates of mental illness do not significantly differ across different types of offenses. Similarly, Henry’s (2022) study reported that 39% of offenders exhibited various mental health disorders. Among the participants, 6% disclosed having a learning disability, 2% reported a bipolar or psychotic disorder, and 10% reported other mental health disorders, excluding personality disorders. It is important to note that 42% of the participants did not report having a diagnosed mental health disorder.
Caravaca-Sánchez et al. (2019) found that female offenders who had experienced sexual, emotional, and physical abuse during childhood reported higher levels of stress, depression, and anxiety than inmates who did not report ACEs. This suggests that the presence of ACEs, particularly abuse, significantly impacts female offenders’ emotional well-being. A study by Laurence (2022) found that female offenders who scored high on neuroticism tended to exhibit pessimistic attitudes toward self-worth. This suggests that individuals with a more negative outlook on their future were likelier to score higher on the neuroticism scale. The study also found significant correlations between stress, depression, and anxiety with social support variables such as affection, emotional interaction, and positive interaction.
Relationship Between Adverse Childhood Experiences, Mental Health, and Crime
A significant proportion of the offender population had experienced a wide range of ACEs before incarceration. These ACEs included domestic violence, substance abuse, neglect, and physical, emotional, verbal, and sexual abuse. Additionally, a prevalent factor in their history was the presence of mental illness within their household. More than half of the individuals in the sample had received a mental health diagnosis at some point (Messina, 2022). These findings highlight the high prevalence of traumatic experiences and mental health challenges among offenders, emphasizing the need for comprehensive interventions and support systems to address their complex needs.
Individuals exposed to multiple ACEs are more likely to engage in self-harming behavior and experience mental illness while incarcerated. Unfortunately, prisons often lack sustainable support systems to address the mental health needs of this vulnerable population, exacerbating their difficulties (Ford et al., 2020). Additionally, Pérez-Ramírez et al. (2021) found a significant association between trauma exposure, ACEs, depression, anger, anxiety, and suicidal ideation and behavior among prisoners. Younger male inmates were more likely to endorse suicidal behaviors than older individuals, and higher ACEs were associated with a greater likelihood of engaging in such behaviors. Skarupski et al. (2015) also found a correlation between repeated physical harm by an adult or parent and depression among participants. These findings highlight the profound impact of early life adverse experiences on mental health, affecting coping mechanisms, attachment, stress responses, emotional regulation, and overall functioning, which can contribute to deviant behaviors (Ford et al., 2020).
This analysis underscores the correlation between the number of ACEs and the increased likelihood of developing a mental health disorder. It further reveals that most offenders have encountered adverse childhood events and received a mental health diagnosis.
Discussion
The present systematic review aimed to analyze and synthesize the literature, exploring the relationship between adverse childhood experiences and mental health in adult offenders. The analysis of 12 scientific articles included in this study showed findings consistently and followed one another, where ACEs affect the offenders’ mental health and criminal behavior.
Results demonstrate that physical abuse, emotional abuse, the death or incarceration of a parent, and physical or sexual abuse are the most frequent ACEs identified by criminal offenders, and ACEs are expected within the offender population (Henry, 2022). Compared to general populations, more ACE experiences and a higher total number of maltreatments are evidenced in individuals who have committed a crime (Skarupski et al., 2015). Studies have revealed that the presence of ACEs differs according to gender and the type of offense (Pflugradt et al., 2017). Neglect, verbal and physical abuse, and a family member in incarceration were significantly more likely to be reported by men. In contrast, women often reported more sexual abuse and mental illness in the household (Henry, 2022).
On the other hand, similar rates of domestic violence, parental separation or divorce, emotional abuse, and substance use in the home were exposed by both genders. Furthermore, concerning gender, the female perpetrators who committed homicide population endorsed higher ACE scores among all items (Pflugradt et al., 2017). Nevertheless, regardless of gender, this population shows a marked presence of ACEs and mental health issues (Ford et al., 2020; Pérez-Ramírez et al., 2021), considered risk factors for future criminal behavior in an individual.
According to Pflugradt et al. (2017), homicide offenders, regardless of gender, have experienced a significantly higher ACEs than other criminal offenders. The most commonly reported ACEs among participants in various studies include physical abuse, emotional abuse, sexual abuse, and the death or incarceration of a parent (Ford et al., 2020; Henry, 2022). These ACEs can profoundly affect a child’s mental health, personal skills, and relationships, potentially influencing dysfunctional or criminal behavior in adulthood. Individuals with higher ACEs also exhibited higher negative emotional states (Ford et al., 2020). Mental health issues were prevalent among all samples of offenders and did not differ significantly based on the type of offense committed. Furthermore, higher ACE scores were associated with increased negative emotional states (Pflugradt et al., 2017; Skarupski et al., 2015).
The study conducted by Pflugradt et al. (2017) found that 25% of the population of sexual offenders did not report any ACEs. However, for those sexual offenders who did experience childhood abuse, it was suggested that their abusive experiences directly affected their engagement in sexual offenses. These individuals may perceive their childhood victimization as normal sexual conduct, leading to distorted views of sex and inappropriate behaviors toward others, as Steely (2023) supports.
On the other hand, a recent study by Almeida and Costa (2023) found no significant differences in childhood sexual victimization scores or benevolent childhood experiences between sex offenders and the general population. This suggests conflicting findings in the literature regarding whether experiencing childhood sexual abuse leads to sexual assault behavior in adulthood.
The relationship between ACEs and mental health problems in offenders has been well-established in the literature, as demonstrated by studies such as Almeida et al. (2024). Individuals who have experienced four or more ACEs are at increased risk for lifetime mental illness diagnosis and suicide attempts. They are 15 times more likely to engage in self-harming behavior and 8 times more likely to attempt suicide in prison (Ford et al., 2020). Even individuals who have experienced two or more ACEs are more likely to engage in these harmful behaviors (Ford et al., 2020). This highlights that offenders who have experienced ACEs throughout their lifetime are more vulnerable to experiencing poor mental health and engaging in self-harm.
Nevertheless, the relationship between ACEs and mental health is intricate and influenced by various factors. Several moderating and mediating variables intervene in ACEs’ impact on mental health throughout individuals’ development and adulthood (Crandall et al., 2019). Benevolent childhood experiences have been identified as moderators in the ACEs and mental health relationship. These positive experiences, such as supportive relationships and stable environments, can mitigate the adverse effects of ACEs (Almeida et al., 2023). Resilience, the ability to bounce back from adversity, can also be a significant moderator. Individuals with higher levels of resilience possess better-coping mechanisms and may be more adept at handling the impact of ACEs on mental health. Resilience is often characterized by strong coping skills, a positive self-image, and a robust social support network (Almeida et al., 2021).
Emotional intelligence emerges as a critical factor in the relationship between ACEs and mental health. The capacity to understand and manage emotions can act as a mediator, potentially lessening the adverse impact of ACEs on mental health (Morales, 2022). Emotional intelligence enhances coping strategies and fosters healthier interpersonal relationships. A sense of purpose or meaning in life is also essential (Subhi et al., 2012). Individuals who find meaning in their experiences are more likely to show psychological resilience, helping them overcome the adverse effects of ACEs on mental health (Tranter et al., 2021). Additionally, social support from friends, peers, and community networks can alleviate psychological distress associated with ACEs, promoting overall mental well-being (Morales, 2022).
It is important to note that mental illness can negatively impact individuals’ emotions and behavior, potentially leading to criminal conduct (Ford et al., 2020). This emphasizes the interplay between ACEs, mental health, and criminal behavior. Understanding and addressing these complex relationships is crucial for providing adequate support and interventions to offenders who have experienced ACEs and are at risk of experiencing mental health issues and engaging in self-harm behavior.
Strengths and Limitations
The primary objective of this research was to contribute to the existing literature by investigating the association between mental illness and ACEs. This study utilized an outcome measure that had not been previously used in this specific context, highlighting the significance of this research. Moreover, the present study substantially contributed to our understanding of the relationship between mental health and ACEs in offenders, as it involved a large sample with diverse data available for analysis. Certain studies have acknowledged the limitation of small sample sizes, which can restrict the statistical power of their analyses (Pérez-Ramírez et al., 2021; Pflugradt et al., 2017). Additionally, the temporal sequence between exposure to ACEs and the development of mental illness has not been explored in depth. By not examining the timing of self-harm, mental illness diagnosis, and suicidal ideation and behaviors, it becomes challenging to ascertain how the timing of these experiences may influence criminal behavior (Ford et al., 2020; Hilton et al., 2019). Despite these limitations, this study provides valuable insights into the history of ACEs and mental health among adult inmates and their connection to adult outcomes in criminality.
Conclusion
The current research proposes valuable future implications. Firstly, it emphasizes the need to adjust prison conditions for offenders to help them adopt non-deviant behavior inside and outside when released into society, reducing recidivism rates. To do so, some strategies are suggested. Research has shown that exploring trauma through mental health treatment programs helped incarcerated men and women with an ACEs complex history who were responsive to trauma-specific treatment (Messina, 2022; Messina & Schepps, 2021). As such, this approach could be implemented in these establishments to reduce criminality. Sending inmates to solitary confinement has been criticized for accentuating their bad conduct behavior and retraumatizing them (Henry, 2022). The current aim of prisons is to reeducate and to help these people not replicate deviant behaviors and follow the social norms when living in society instead of solely punishing them and not showing how they can follow a different path once out of jail. Further research should consider the time an individual’s mental health issues or mental illness, as well as ACEs, has unfolded in their lifetime to establish a more in-depth relationship between these two variables.
Policy Implications
The necessity for treatment with offenders in prison establishments is overly documented as mental health symptomology is a risk factor for the aggravation of deviant behavior (Pérez-Ramírez et al., 2021). However, it has continuously been scarcer over history within prison settings (Messina & Schepps, 2021). Although these researchers agree with their findings, further refinement is needed on how ACEs influence criminal behavior and how mental illness may influence the individual to crime. Exploring the time of the ACEs’ and mental health occurrence could help explain its relationship to crime.
Implementing programs focused on preventing these adverse experiences may help avert the increase in mental health problems and criminality. Moreover, as prisons focus on rehabilitation and reducing recidivism, mental health should be considered a primary treatment focus. It is indeed required for mental health treatment programs and post-release outcome measures (Messina, 2022; Pérez-Ramírez et al., 2021). It is enhanced how trauma influences an individual’s behavior. Therefore, trauma-focused programs can be implemented to prevent the reoccurrence of violence and aggression in offenders (Papalia et al., 2019). Addressing those traumatic experiences within a psychological setting and treatment can help an individual’s mental health, emotion management, and behavior strategies schemes (Messina, 2022).
These approaches would help them adopt a more socially acceptable behavior inside and outside of prison, reducing the likelihood of reoffending. Preventive measures should also be integrated into prison policies, focusing on averting the escalation of mental health problems and criminality. Implementing programs geared towards preventing ACEs and prioritizing mental health treatment within prisons can serve as crucial steps to reduce violence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CiiEM has provided support through Project 10.54499/UIDB/04585/2020, funded by FCT.