
Abstract
This study explores cannabis diversion and its associated factors through the lens of procedural justice theory and deterrence concepts. A quantitative research survey was conducted among 202 medical cannabis license holders in Israel to assess the prevalence, frequency, attitudes, trust in the healthcare system, and fear of punishment related to medical cannabis diversion. Our findings revealed that 60% of license holders engage in medical cannabis diversion, primarily driven by altruistic motives. Attitudes toward diversion were found to act as mediators between trust in the healthcare system, fear of punishment, and the act of diversion. The widespread occurrence of medical cannabis diversion underscores its significance and warrants focused attention. The disparity between criminal law and practical realities necessitates policy revisions concerning medical cannabis.
Keywords
Prescription drug diversion, a recognized issue within the medical and legal spheres, involves directing regulated medications into illegal markets (Inciardi et al., 2007). It occurs when patients distribute or trade their prescribed medications to others (Johnson & Richert, 2015). This is a widespread phenomenon, which poses significant health risks (Bardwell et al., 2021) and contributes to the availability of illicit substances (Garcia et al., 2022). Studies on drug diversion have primarily focused on sleeping pills, opiates, and psychiatric drugs (Bardwell et al., 2021; Garcia et al., 2022; McCabe et al., 2019). These studies reveal that the primary motivations behind diversion include altruistic intentions, such as aiding other patients in need, and financial incentives (Allen & Harocopos, 2016; Duffy & Baldwin, 2012; Johnson & Richert, 2015; Kaye et al., 2014).
Only a few studies have addressed attitudes toward cannabis diversion and actual medical cannabis diversion (Rozmann & Ne’eman-Haviv, 2023). Cannabis for recreational purposes is the most widely used illegal substance worldwide (Connor et al., 2021). However, while cannabis remains a prohibited substance in many countries, recent decades have witnessed a series of political, legislative, and judicial processes across different regions, leading to the establishment of various legal regulatory frameworks for its medical and therapeutic use. This trend appears to be solidifying in the United States, Latin America, the Caribbean, Canada, the Netherlands, UK, Italy, Switzerland, and beyond (Aguilar et al., 2018; Athey et al., 2017; Stevens, 2024). However, regulations pertaining to the nature of medical cannabis use, including aspects such as eligible amounts, permitted strains, authorization for cultivation versus solely purchasing dried cannabis, designated purchase locations, public smoking permissions, and more, exhibit significant variations from one country to another (Athey et al., 2017; Kinney, 2022).
According to the regulation changes, the phenomenon of medical cannabis diversion is increasing, although precise data regarding its extent remain unavailable. The existence of the phenomenon can be seen from various studies that allude to it, such as a study conducted in the USA, in which 40% of teenagers reported receiving marijuana from a person with a license for medical cannabis (Thurstone et al., 2011).
Israel has emerged as a frontrunner in the medical cannabis industry since the 1990s (Zarhin, 2020). In response to the growing demand and the necessity for a sustainable program, the Israel Ministry of Health established a dedicated governmental cannabis agency in 2011. The Israel Medical Cannabis Agency (IMCA) is tasked with overseeing the regulation of medical cannabis usage among patients, its authorization by physicians, and the comprehensive regulation and authorization of the entire supply chain (Isralowitz et al., 2021). Over time, the number of patients with medical cannabis prescriptions has steadily risen, reaching approximately 135,000 licensed patients by 2023 (Ministry of Health, 2023). As awareness grows regarding its efficacy across various medical conditions, the demand for medical cannabis treatment has surged. Upon the recommendation of the attending physician for medical cannabis treatment, the patient is issued a license to possess a controlled substance by the IMCA. This license provides explicit instructions regarding the permitted quantity of cannabis for the patient, along with specified percentages of THC and CBD. The medicinal cannabis is procured from a pharmacy, which is mandated to dispense the substance strictly in accordance with the license. The patient is prohibited from cultivating cannabis independently. License renewal occurs annually, and modifications to the license content are not permissible within the year. Additionally, the license for cannabis possession includes stipulations that the substance is for personal use only, must not be used in public spaces, and is strictly prohibited from being transferred to another individual, irrespective of whether the recipient possesses a medical cannabis license.
Consequently, a challenge arises in balancing providing cannabis for legitimate medical needs while curbing attempts by individuals to obtain it for nonmedical reasons (Naftali, 2016). The diversion of medical cannabis in Israel holds a distinct status, different from the diversion of other medicines, due to its criminal nature. In Israel, cannabis is classified as a dangerous substance, making its diversion a drug trafficking offense under the “Dangerous Drugs Ordinance,” carrying a potential punishment of up to 20 years in prison (Ne’eman-Haviv & Rozmann, 2023). However, despite its legal ramifications, the phenomenon of medical cannabis diversion remains widespread, suggesting a relatively low deterrence from engaging in this offense (Sznitman, 2020). Examining the phenomenon of medical cannabis diversion in Israel provides valuable insights into the limitations of the cannabis policy. This research offers a distinctive perspective that explores the repercussions of the current regulations on the diversion of medical cannabis, serving as a case study with implications for cannabis programs worldwide. This study aims to explore the factors relating to patients with medical cannabis licenses’ willingness to divert cannabis to others, despite being aware of its serious legal implications. This study suggests a model for evaluating several variables predicting medical cannabis diversion: attitudes toward the diversion of medical cannabis, patients’ trust levels in the healthcare system, and the fear of potential punishment.
Although no comprehensive research has been undertaken in Israel to assess the extent of medical cannabis diversion, existing data shed light on public attitudes toward this practice. Ne’eman-Haviv and Rozman’s (2023) study delved into the opinions of the Israeli public regarding cannabis diversion among patients. Contrary to the severity outlined in the law, the study revealed that the Israeli public perceives the diversion of medical cannabis as a moderately serious offense and, surprisingly, at times, even as a normative and morally acceptable act. Drawing from prior studies that establish a positive correlation between attitudes and behavior concerning psychoactive substances (Davis et al., 2022; Shechory Bitton & Noach, 2023), the first research hypothesis is:
H1: There is a positive association between attitudes toward medical cannabis diversion and the actual occurrence of cannabis diversion.
Trust in the Healthcare System
Trust in a specific institution or organization denotes an individual’s perception of that system possessing the competence to make decisions within its purview, being dependable, fulfilling its obligations, and consistently acting responsibly. This form of trust is rooted in a set of beliefs or expectations rather than merely an emotional reaction (Devos et al., 2002). As articulated by Jackson and Gau (2016), trust in a system bestows legitimacy upon the system within the public sphere, enabling the acceptance of its authority in shaping policies.
Research indicates that public trust in the public healthcare system, particularly in service providers, is crucial to securing patient cooperation and compliance with medical instructions. This trust fosters extensive cooperation, often leading to improved governance (Antinyan et al., 2021). Moreover, health policies play a pivotal role in shaping the population as a disciplined civil society and as creators of social norms (Gilson, 2006). Conversely, low levels of trust can lead to inefficiencies, undermine the healthcare system’s legitimacy, reduce solidarity (Maarse & Jeurissen, 2019), and ultimately impact the healthcare system’s overall success (Wilk & Platt, 2016).
Recent studies examined public trust in Israel’s healthcare system. According to the Committee for Strengthening the Public Health System’s report (Eitan, 2012), Israel’s trust index in the public healthcare system ranks relatively low compared to selected OECD countries. Only around 52% of the public expressed belief in receiving the best treatment for a serious illness, and merely 40% believed they could afford treatment for their illnesses (Bramley-Greenberg & Medina-Hartom, 2015). According to Schiff-Kern (2019), a significant number of patients in Israel perceive a lack of fairness or impartiality in the Ministry of Health’s decision-making processes regarding cannabis-related matters. This perception extends to the prescription issuance, the foundational aspects of cannabis reform, and the definition of cannabis’s legal status, contributing to a decrease in the ministry’s credibility in their eyes.
The procedural justice model, conceived by Tyler (1990), posits that the more authorities are perceived as legitimate, the less likely individuals engage in lawbreaking. This theory suggests that the fairness demonstrated by authorities correlates with public trust in them, perceptions of their legality, and consequently, individuals’ inclination to comply with the law (Bottoms & Tankebe, 2012; Hough et al., 2010; Jackson et al., 2012; Tyler, 2006; Tyler & Blader, 2003; Tyler & Huo, 2002). Conversely, when authorities are perceived as lacking procedural fairness, their legitimacy is undermined, potentially fostering disobedience and resistance (Fischer et al., 2008). Since its inception, the procedural justice model has emerged as a pivotal theoretical framework significantly shaping considerations within criminal law regarding citizens’ compliance behavior (Liu & Wu, 2023). According to the theory of procedural justice, the second research hypothesis is:
H2: Lower levels of trust in the healthcare system will be associated with more positive attitudes toward medical cannabis diversion, which in turn will be associated with a greater chance of actual diversion.
Obedience to the Law and Fear of Punishment
Attitude toward the law encompasses one’s positive or negative evaluation of the law and the decision to comply with or oppose it. Research suggests that attitudes toward the law serve as predictors for either compliance or noncompliance (Walters & Bolger, 2019). Therefore, understanding the factors influencing these attitudes is crucial. Studies have found that attitudes toward the law and actual compliance with the law are related, among other things, to fear of punishment. This aligns with deterrence theories in criminology, which argue that individuals, being rational, refrain from committing crimes due to the possibility of facing punishment (Rocker, 2021). It is of paramount importance to understand the law, comprehend the associated penalties, align the severity of punishment with the gravity of the offense, and ensure the certainty of punishment. All these elements are intended to deter against engaging in criminal activities (Tomlinson, 2016). However, many studies, including studies on drug diversion, show that despite their awareness of the legal violation and the severe penalties associated with it, holders of licenses/prescriptions for drugs continue to divert to others (Bardwell et al., 2021; Bonny-Noach & Ne’eman-Haviv, 2018).
In the context of cannabis use in Israel, both social and legal developments have contributed to diminishing deterrence concerning the use, trade, and diversion of cannabis. Socially, there has been a noticeable normalization of cannabis use over time, and it is perceived as a substance that is not dangerous or harmful, and therefore legitimate for use (Tandowski et al., 2019). Legally, Israel has undergone a process of regulating policies related to recreational cannabis consumption, moving away from criminalization (Chassid-Segin et al., 2023). Although this legal shift did not directly impact medical cannabis patients, the lack of strict enforcement regarding personal cannabis use likely contributes to a reduced sense of fear of punishment, even within the realm of medical cannabis. Accordingly, the third research hypothesis is:
H3: Lower levels of fear of punishment will be associated with more positive attitudes toward medical cannabis diversion, which in turn will be associated with a greater chance of actual diversion.
The Current Research
This study aims to explore the extent of the phenomenon of medical cannabis diversion and its associated variables. Drawing from the procedural justice theory and deterrence concepts, the study model seeks to understand factors contributing to medical cannabis diversion, as expressed in the fourth hypothesis:
H4: Lower levels of trust in the healthcare system, lower levels of fear of punishment, and more positive attitudes toward medical cannabis diversion will be associated with a higher frequency of actual diversion.
While the legal use of cannabis for medical purposes is permitted through a license to possess a dangerous drug, Reid (2022) observed prevalent stigmas associated with medical cannabis users, including being labeled as drug addicts, having low functional capabilities, or being seen as offenders. These stigmas detrimentally impact the interpersonal relationships of the patients, resulting in negative moral judgments that label any cannabis use as inherently problematic (Wheeldon & Heidt, 2022). These misconceptions contribute to the perception that cannabis patients deviate from societal norms, exploiting medical justification for recreational purposes. Despite acknowledging that medical cannabis users may experience pleasure during use (Athey et al., 2017), it is crucial to emphasize that this does not diminish their genuine medical needs or their adherence to normative perceptions of the law. Consequently, this study considers medical cannabis users as normative, law-abiding individuals, with “attitudes toward law adherence” serving as a control variable.
Understanding the diversion of medical cannabis is significantly important both in research and practical applications. While there is abundant literature on prescription drug diversion, there has been limited focus on medical cannabis diversion and its related variables. The present study seeks to fill this gap. Exploring these factors can provide valuable insights for policy making regarding medical cannabis, potentially minimizing instances of illicit trade.
Method
Participants
Participants were 202 Israeli adult citizens, all licensed for medical cannabis. Close to 60% of them were males, ranging in age between 19 and 81 years (M = 39.03 years, SD = 13.32). Most were secular (close to 80%), and had 10 to 20 years of education (M = 13.41 years, SD = 2.11).
Tools
The following tools were used in the study:
Attitudes Toward the Law Questionnaire: Control Variable
The questionnaire was compiled by Daniel and Kanfo (2011). Attitudes toward law enforcement were measured by the participants’ agreement with five statements, rated on a 5-point Likert scale. Example item: “I prefer to behave according to the law even if there is no chance of getting caught.” A score was calculated for each participant by averaging the five items, with a higher score indicating more positive attitudes toward law enforcement. In the present study, good internal consistency was found, Cronbach’s alpha was α = .78.
Trust in the Healthcare System Questionnaire
The questionnaire was taken from a follow-up survey by the (Ministry of Health, 2018). The questionnaire includes 10 items, rated on a 5-level Likert scale. Example item: “How sure are you that if, God forbid, you get a serious illness, you will receive the best and most beneficial treatment?” A score was calculated for each participant by averaging the 10 items. A higher score indicates a higher level of trust in the healthcare system. Cronbach’s alpha reliability was α = .81.
Attitudes Toward the Diversion of Medical Cannabis Questionnaire (Supplemental Appendix 1)
Since this issue has not been examined before, the questionnaire was specifically compiled for this study. The questionnaire’s content validity was based on an extensive literature review in the field, as well as on two relevant questionnaires that were used in previous studies: the study by (Johnson & Richert, 2015), which examines attitudes toward the transfer of prescription drugs, and the study by Ne’eman-Haviv and Rozman (2023), which examined attitudes toward cannabis diversion through participants’ responses to different scenarios of medical cannabis diversion. To establish the reliability of the questionnaire, a preliminary study was conducted, in which an internal reliability of .84 was found. A CFA calculated in the current study showed a good fit for the one-factor model: Cmin/df = 1.29, NFI = 0.971, TLI = 0.983, CFI = 0.993, RMSEA = 0.038, with item loadings ranging between 0.46 and 0.85 (p < .001).
The questionnaire includes eight statements, where the participant indicates the extent of agreement with each of the statements on a Likert scale ranging from 1 (not at all) to 5 (very much). Example item: “In my opinion, a person must not, under any circumstances, transfer his/her legal medical cannabis to another person.” A score was calculated for each participant by calculating the average of the answers, where a higher score indicates more positive attitudes toward medical cannabis diversion. In the present study, good internal consistency was found: α = .87.
Fear of Punishment Questionnaire
The questionnaire includes three questions that examine the degree to which the participant thinks there is a chance that someone with a cannabis license will be caught, prosecuted, and convicted, if that person transfers some of the licensed cannabis to someone else. The participant is asked to mark the answers on a Likert scale ranging from 1 (not at all) to 5 (very much). The questionnaire is based on the fear of punishment questionnaire by (Wikström et al., 2011), adapting it to the issue of medical cannabis. A score was calculated for each participant by calculating the average of the subjects’ answers, where a higher score indicates a higher fear of punishment. In the current study, a medium but acceptable internal consistency was found: α = .65.
Medical Cannabis Diversion Questionnaire (Supplemental Appendix 2)
The questionnaire examines whether the cannabis license holder has transferred some of the substance in his/her possession to another person. The questionnaire was specifically compiled for the current study and contains 12 questions concerning the possession and transfer of cannabis. Two variables were constructed from this questionnaire: one is dichotomous - transferred/did not transfer part of the material to another person, and the second is graded regarding the frequency of diversion among those who transfer material to another: a few times/several times a year/every month.
Demographic Questionnaire
This includes personal-details questions such as gender, age, marital status, religion, level of religiosity, number of years of education, and income level.
Procedure
The study was approved by the university’s ethics committee. The research population is unique, as it included only licensed medical cannabis patients. Patient identification was based on a purpose-oriented convenience sample in this population. The approach was made through social networks, in groups dedicated to cannabis patients, and face-to-face meetings in meeting places for cannabis patients, such as shops and smoking centers. In these sessions, the experimenter gave the participants a QR code containing a link to the questionnaire. The participants filled out the questionnaire in their free time, and not in the presence of the experimenter. All questionnaires were sent via an internet link. The subjects signed an informed consent form, which informed them that their answers are anonymous, that they can stop answering the questionnaire at any time, that there are no right answers, and that they are asked to express their opinion. The subjects then answered the research questionnaires. All study participants answered all questions in the questionnaire. Answering the questionnaire took about 10 minutes. Data collection was done using Qualtrics software. No compensation was given for answering the questionnaires.
Data Analysis
Data were analyzed with SPSS version 29. Descriptive statistics were calculated for the demographic variables and those concerning the use and diversion of medical cannabis. A CFA was calculated for the new questionnaire of attitudes toward the diversion of medical cannabis, using AMOS version 29. Fit measures were Cmin/df, NFI, TLI, CFI, and RMSEA. Cronbach α was used for internal consistency. The study variables were described with means, standard deviations, and Pearson correlations. Demographic associations with the mediating and dependent variables were examined, using simple logistic regressions and independent t-tests. Mediation was examined with the PROCESS procedure model 4 (Hayes, 2013) for a binary dependent variable, using 5,000 bootstrap samples, and 95% confidence interval. Variables were standardized. A multiple logistic regression was calculated for participants who reported the frequency of cannabis diversion, assessing the odds for a frequent diversion of medical cannabis as a function of the study variables.
Sample size: the minimum acceptable sample size for complex models that involve mediation is often regarded as 200 participants. In addition, the criterion of using 10 to 20 participants per model parameter is common (N:q) (Kline, 2023). According to Hayes (2013), a total sample size for complex models cannot be directly calculated, as each part of the model (direct effect, mediated effect, etc.) requires a different sample size, according to its effect size and the desired power level. Thus, we used the minimum acceptable general criterion of 200 participants. This allows using up to 20 parameters in the model.
Results
Descriptive Results
As shown in Table 1, 56.9% of the participants were males, with an average age of 39 years (SD = 13.32 years). About 43% of them were single, and roughly 40% were married, with most (78.7%) being secular. Average years of education were 13.4 years (SD = 2.11 years). The participants’ income level varied, between below average (24.2%), average (42.6%), and above average (34.2%).
Demographic and Cannabis Related Characteristics of the Participants (N = 202).
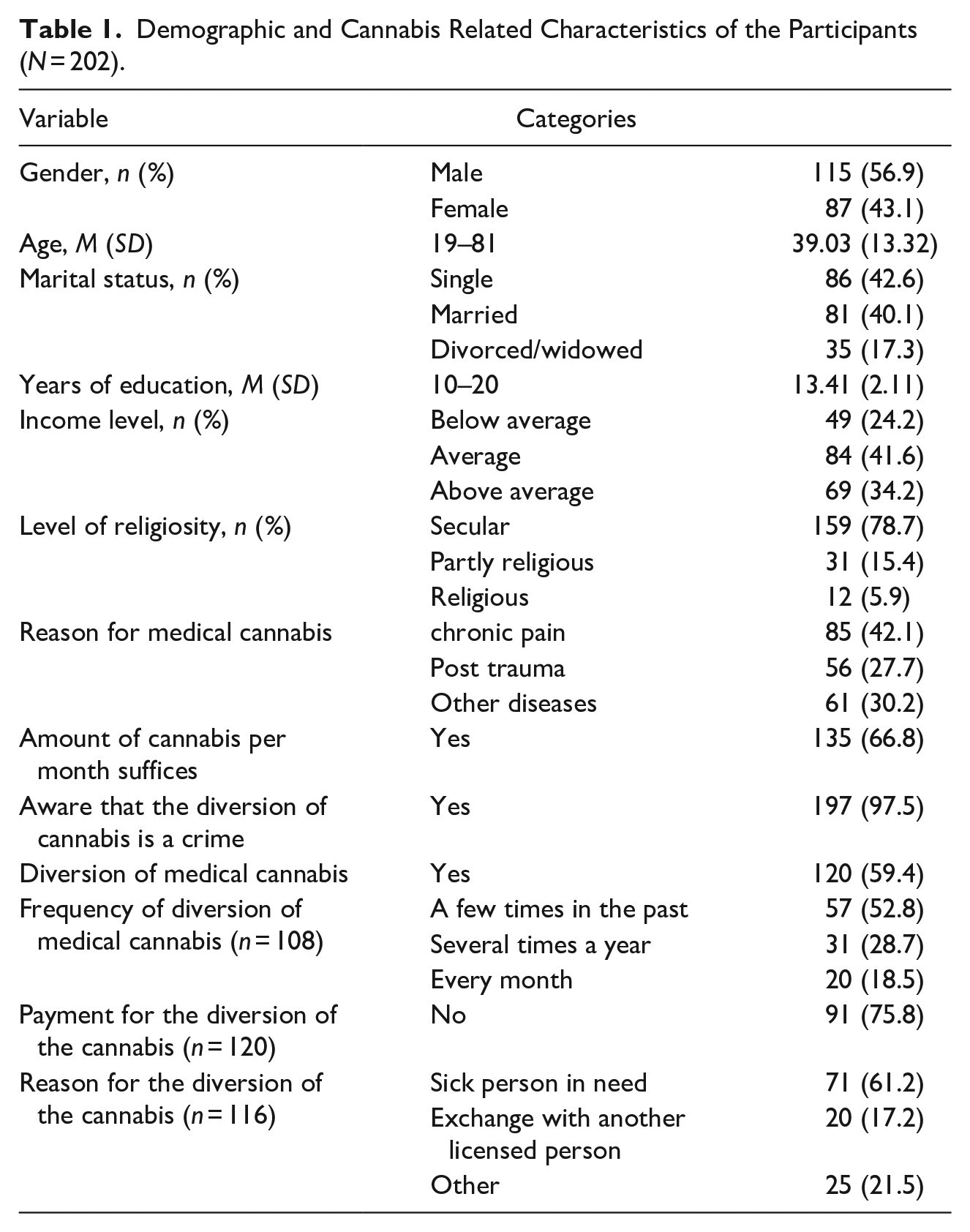
Chronic pain (about 42%) and post-trauma (about 28%) were the most common reasons for receiving cannabis. About two-thirds of the participants reported receiving sufficient amounts of cannabis (about 67%), and almost all knew that that cannabis diversion was a crime. However, about 60% of the participants reported on diverting cannabis, at least a few times in the past. Most did not divert the cannabis for payment (about 76%), and gave it to a person in need (about 61%).
Significant correlations were found among the study variables. Trust in the healthcare system and fear of punishment were positively associated, and both were negatively associated with attitudes toward the diversion of medical cannabis and its actual diversion (except for the association between trust in the healthcare system and the diversion of medical cannabis). As expected, as in the first hypothesis, the attitudes toward the diversion of medical cannabis were positively associated with its diversion. Attitudes toward the law, the covariate variable, were positively associated with trust in the healthcare system and fear of punishment, and negatively associated with the attitudes toward the diversion of medical cannabis, and with its actual diversion. Table 2 presents these correlations.
Means, Standard Deviations, and Correlations for the Study Variables (N = 202).
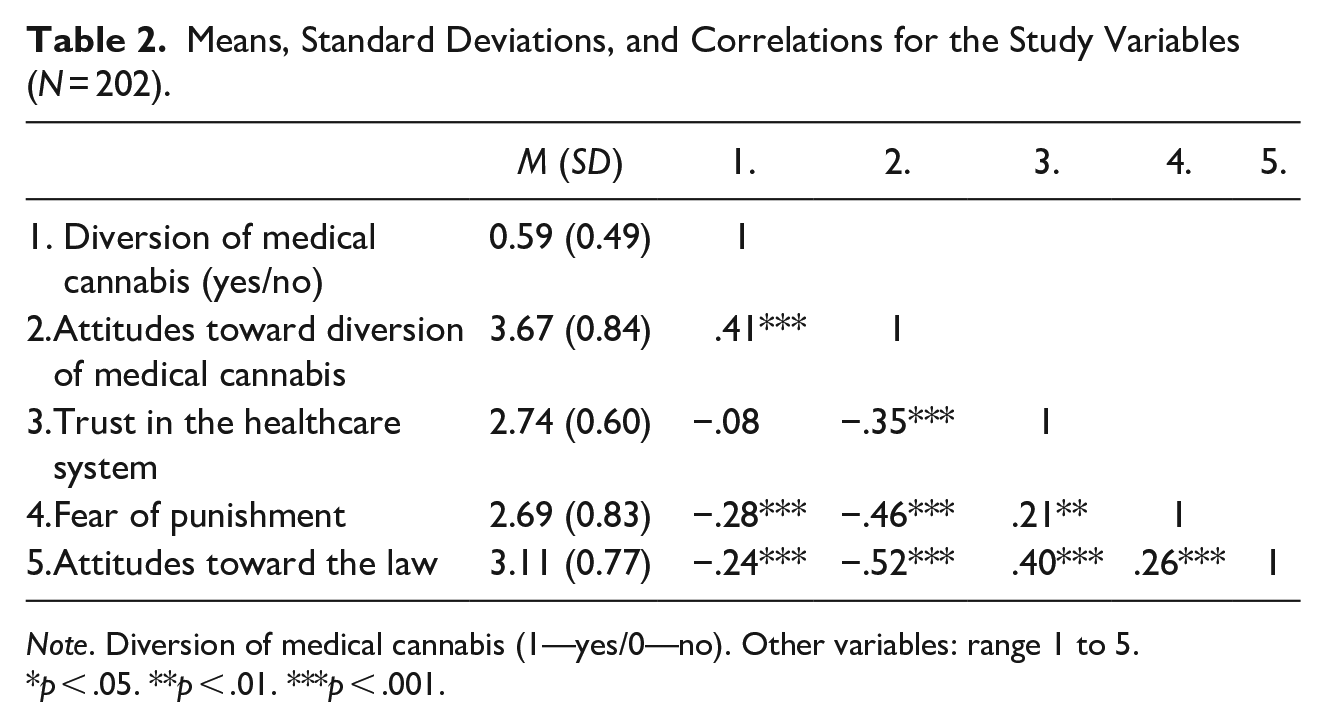
Note. Diversion of medical cannabis (1—yes/0—no). Other variables: range 1 to 5.
p < .05. **p < .01. ***p < .001.
Demographic associations were examined for the mediating and dependent variables, to identify additional covariates that needed to be controlled for. The diversion of medical cannabis was higher among secular participants (n = 102, 64.2%) than among religious and partly religious participants (n = 18, 41.9%) (OR = 2.48, p = .009, 95% CI [1.25, 4.94]). The diversion of medical cannabis odds were further higher for younger participants (OR = 0.98, p = .047, 95% CI [0.96, 1.00]), and for participants with fewer years of education (OR = 0.84, p = .012, 95% CI [0.73, 0.96]). In addition, the attitudes toward medical cannabis diversion were more positive among secular participants (M = 3.75, SD = 3.39) than among religious and partly religious participants (M = 3.39, SD = 0.88) (t(200) = 2.58, p = .010, d = 0.44). Other demographic associations were not significant, and thus the study hypotheses were examined while controlling for age, years of education, level of religiosity (0—religious and partly religious, 1—secular), and attitudes toward the law.
The study model was examined with the PROCESS procedure model 4 (Hayes, 2013) for a binary dependent variable. Age, years of education, level of religiosity, and attitudes toward the law were controlled for. Trust in the healthcare system and fear of punishment were the independent variables, attitudes toward medical cannabis diversion were the mediator, and medical cannabis diversion (1—yes, 0—no) was the dependent variable. The indirect effect was found significant for both trust in the healthcare system (effect = −0.15, SE = 0.09, 95% CI [−0.35, −0.02]), and fear of punishment (effect = −0.26, SE = 0.10, 95% CI [−0.51, −0.11]). The direct effects are shown in Figure 1, and reveal that higher trust in the healthcare system and higher fear of punishment were associated with less positive attitudes toward the diversion of medical cannabis, which in turn was associated with lower odds for reporting the diversion of medical cannabis.
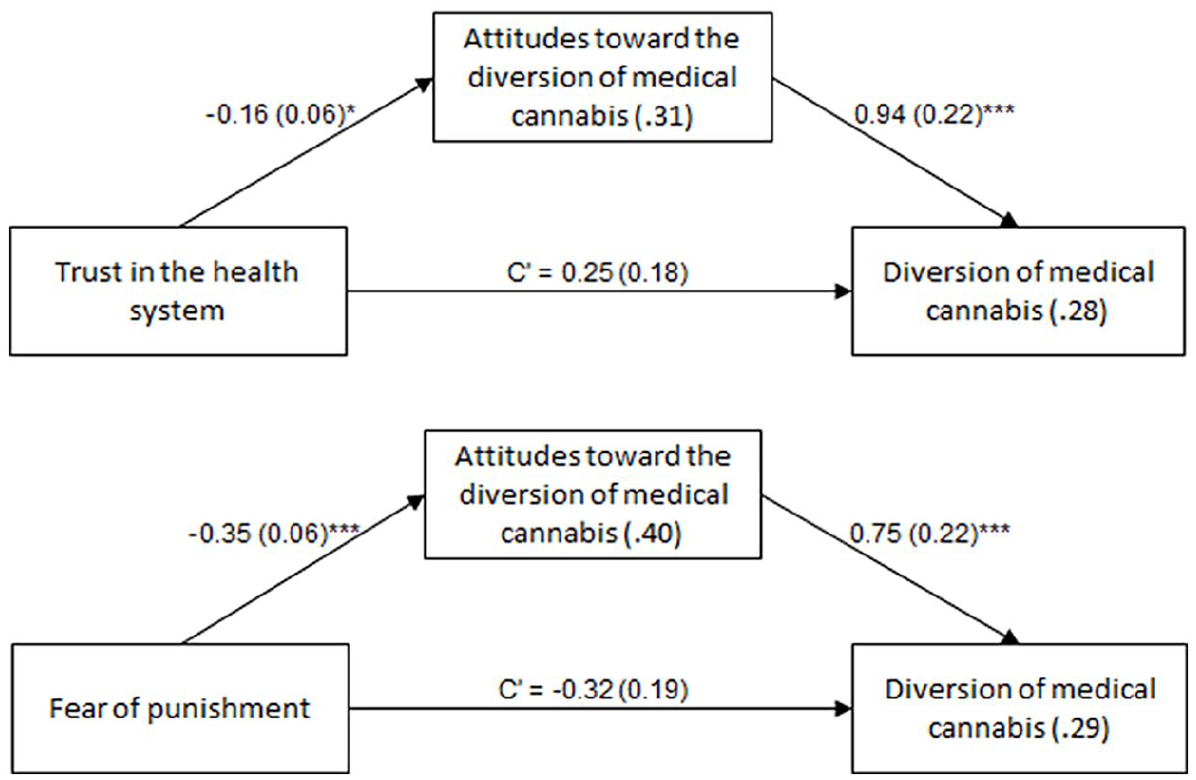
The mediating role of attitudes toward the diversion of medical cannabis in the association between trust in the healthcare system and fear of punishment, and the diversion of medical cannabis
A comparative examination of the association between trust in the healthcare system and attitudes toward the diversion of medical cannabis (B = −0.16, SE = 0.06, p = .012) versus the association between fear of punishment and attitudes toward the diversion of cannabis (B = −0.35, SE = 0.06, p < .001) (calculated in a regression model), showed that the difference was significant (Z = 2.43, p = .015). That is, fear of punishment was more meaningful than trust in the healthcare system concerning the report of the diversion of medical cannabis.
Finally, and as mentioned earlier (in Table 1), 108 participants reported the frequency of medical cannabis diversion (out of n = 120, 90%). About a half of them claimed they did so a few times in the past (n = 57, 52.8%), and the others admitted to doing so at least several times a year or even every month (n = 51, 47.2%). A logistic regression was calculated to assess the extent to which the odds for a frequent diversion of medical cannabis were a function of the study variables (Table 3). The regression model was found significant, explaining about 31% of the variance. The odds for a frequent diversion of medical cannabis were higher with lower fear of punishment and with more positive attitudes toward the diversion of medical cannabis.
Multiple Logistic Regression for the Frequency of Medical Cannabis Diversion (N= 108).
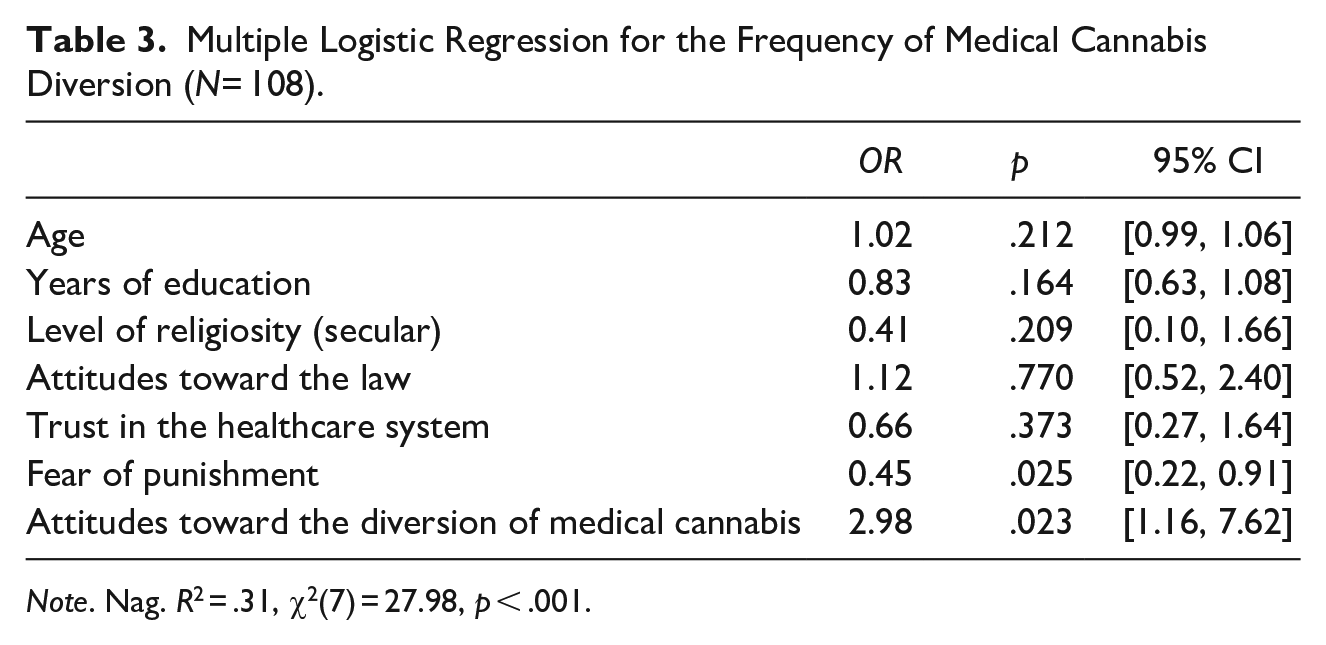
Note. Nag. R2 = .31, χ2(7) = 27.98, p < .001.
Discussion
The medical uses of cannabis have been known for thousands of years, yet its institutionalized regulation as a medicinal substance emerged only in recent decades (Zarhin, 2020). Like other prescription drugs, drug diversion also occurs in medical cannabis. However, while extensive research exists on the diversion of various medications like neuropathic, sleep, and psychiatric drugs (Inciardi et al., 2007; Kurtz et al., 2019; Milani et al., 2020; Wood, 2015), studies on medical cannabis diversion are notably scarce globally and specifically in Israel. This scarcity is noteworthy considering the significant legal implications of cannabis diversion. Unlike other diverted drugs, cannabis diversion constitutes a drug-trafficking offense (Ne’eman-Haviv & Rozmann, 2023). This study aims to address this gap in the literature by delving into the phenomenon of medical cannabis diversion and exploring the associated variables, thereby contributing to a deeper understanding of this issue.
Furthermore, the significance of this research is in shaping policy and regulation surrounding medical cannabis. The study’s findings underscore the applicability of Wheeldon and Heidt’s (2022) perspective, asserting that cannabis regulatory environments can give rise to new forms of crime, which extends to the realm of medical cannabis.
Aligning with Kinney’s (2022, 2023a, 2023b) research, which characterizes regulations related to cannabis use as “sumptuary laws,” aimed at governing conduct deemed immoral, such as prostitution, gambling, or drug abuse, our study supports the notion that improper cannabis regulation may contribute to the emergence of a gray market for cannabis sales. While the current study did not investigate the existence of a commercial gray market for medical cannabis, our findings indicate the presence of exchange, both with and without compensation, among cannabis patients.
The initial contribution of this study lies in shedding light on the extent of medical cannabis diversion among patients, a largely unexplored phenomenon lacking available data. The research findings reveal a widespread occurrence of this behavior. Approximately 60% of licensees admitted transferring a portion of their cannabis supply to another person, with nearly half of them engaging in this behavior regularly. Notably, in 76% of cases, the transfer occurred without any financial exchange, while in the remaining instances, some form of payment for the material was involved. Only 6% of patients reported transferring the substance solely for financial gain.
These findings essentially refute assertions that medical cannabis diversion is driven by drug trafficking for financial gain and that the individuals involved are engaging in criminal behavior. This gains further strength considering that the primary motivation for diverting cannabis is to assist those in need and to exchange strains with other licensed individuals. For instance, roughly a third of the participants disclosed that the quantity of cannabis allocated in their prescription is not sufficient until the subsequent prescription renewal the following month. This deficit creates a necessity to procure additional cannabis beyond the license limits, clarifying the patients’ inclination to help others and divert the drug. These findings align with previous studies on various medications, demonstrating that the primary motive behind diverting medications is altruistic (Allen & Harocopos, 2016; Duffy & Baldwin, 2012; Johnson & Richert, 2015). This finding is important, especially considering that past studies have highlighted the moral imperative of patients as a de facto driving force behind policy changes in the broader context of cannabis in general, and specifically, medical cannabis (Kinney, 2023b; Stevens, 2024).
The research outcomes highlight a significant aspect: nearly all research participants were aware that their cannabis license was strictly personal and non-transferable, and that diverting cannabis constituted a criminal offense. This finding intensifies the central inquiry of the study: Why would law-abiding individuals, aware of the legal ramifications, engage in diverting cannabis? To probe this question, the study incorporated the variable “attitudes toward law” as a control variable, aiming to understand the nuances surrounding this behavior despite its legal implications.
The attitudes of medical cannabis patients toward the seriousness of cannabis diversion reveal that they consider cannabis diversion as only moderately severe. This contrasts with legal definitions that categorize cannabis diversion as a drug trafficking offense. Similar findings were echoed in the research by Ne’eman-Haviv and Rozmann (2023), who explored the general public’s attitudes in Israel toward cannabis diversion. Their findings also reflect a perception of moderate seriousness regarding guilt and punishment, occasionally even considering it a moral and normative act. To elucidate this phenomenon, the researchers drew upon Kohlberg’s theory of moral development (Kohlberg & Hersh, 1977). According to this theory, individuals might reject legal norms when they perceive a conflict between the morality of the law and their internal moral principles. This explanation gains support from the fact that most patients who admitted to diverting cannabis did so for altruistic motives, reinforcing the idea that moral considerations might influence their actions in this context.
In accordance with the second research hypothesis, a significant correlation was found between trust in the healthcare system and attitudes toward the diversion of medical cannabis. The difficulties faced by cannabis patients, from obtaining the license to obtaining the substance (Schiff-Kern, 2019), depending on the quantity and strain needed, are reflected in the current study as a low level of trust in the healthcare system. Hence, the research findings strengthen the foundations of the procedural justice theory (Tyler & Fagan, 2008), and point to the importance of trust in government institutions to uphold the law.
Another variable, which was found to be related to attitudes toward the diversion of medical cannabis, is fear of punishment. The participants showed low fear of punishment levels, despite their awareness of the law’s severity. This reduced fear might stem from recent legal developments in Israel surrounding cannabis usage beyond medical purposes. These alterations signify a growing leniency trend within the public sphere, reflected in legal policies toward cannabis use. The assumption is that medical cannabis patients believe that law enforcement authorities’ lenient attitude on cannabis use will also be expressed if they are caught diverting cannabis, especially when it comes to diversion between licensed patients.
The study’s findings provide partial confirmation for the second and third hypotheses, indicating that there is not a direct link between the level of trust in the healthcare system or the fear of punishment and the actual diversion of cannabis. Instead, these factors are associated solely with attitudes toward cannabis diversion. However, the research model proposed in the fourth hypothesis revealed a relationship: the level of trust in the healthcare system and the fear of punishment are connected to actual cannabis diversion, mediated by attitudes toward cannabis diversion. These findings highlight a psychological process among patients. It suggests that these individuals, typically law-abiding, find it challenging to commit an offense. Engaging in diversion represents a perceptual shift for them, requiring a change in attitudes before actual diversion occurs. Only after cultivating justifications or lenient positions toward cannabis diversion do individuals proceed with the act of diversion itself. This emphasizes the importance of internal attitudes and moral considerations in influencing behavior, especially among those unaccustomed to criminal conduct.
The prediction model also explored the influence of demographic variables on medical cannabis diversion, revealing significant roles for religiosity, age, and education level. Secularism, younger age, and lower education were associated with a higher likelihood of diverting medical cannabis. Among these demographic factors, religiosity emerged as the most impactful. Secular individuals exhibited more favorable attitudes toward cannabis diversion compared to traditional or religious counterparts and showed a higher likelihood of actual diversion. This distinction might be attributed to the conservative views held by religious individuals regarding psychoactive substances, including cannabis. Studies suggest that traditional or religious individuals perceive these substances as more dangerous (Ne’eman-Haviv & Wilchek-Aviad, 2017), leading to infrequent usage compared to secular populations, even when prescribed medically (Siddiqui et al., 2022). Despite acknowledging cannabis’s medical value through prescriptions, the heightened perception of its dangers among religious individuals potentially dissuades them from diverting it to others. The correlation between stronger support for medical cannabis diversion and younger age in study participants is not unexpected and can be attributed to several factors. Numerous studies have highlighted that younger individual are generally more supportive of cannabis use, both for medical and recreational purposes (Tanco et al., 2019). Additionally, this demographic tends to perceive cannabis use as normative and less dangerous (Siddiqui et al., 2022), leading to reduced apprehension about passing it on to others.
Limitations and Future Research
The present study has several limitations. Although the number of cannabis license holders has increased in recent years, there was difficulty in recruiting participants to participate in the study, which limiting the size of the sample and its implications. Moreover, a significant portion of cannabis patients avoid sharing information in the field, both for criminal reasons and for personal modesty regarding their reasons that make them entitled to a prescription in the first place. This fact may impair the ability to generalize the research findings to the entire patient population. The issues that the participants were asked about include admitting to committing crimes and therefore, there was a difficulty in recruiting participants. Some of them expressed concern about the level of anonymity and the credibility of the research’s origin and goals. Therefore, biasing of the answers should be taken into account for those who fear changes in the field and cancellation of their license. Further research is warranted in which examination of additional variables related to diversion, such as moral aspects, which lead to the justification of the phenomenon of diversion should be studied.
Conclusions
The current study offers substantial contributions both theoretically and practically. From a theoretical standpoint, it illuminates the relatively unexplored area of medical cannabis diversion. This study, to the best of our knowledge, represents the first investigation into the extent and associated variables of this phenomenon among medical cannabis patients. By shedding light on these aspects, it significantly augments our understanding of medication diversion, a critical global issue in the medical and legal realms.
Furthermore, this research strengthens the concept of procedural justice, demonstrating its relevance in domains previously unexamined, such as medication diversion. The findings underscore how low fairness perception in governing bodies diminishes cooperation and fosters disobedience, aligning with existing research (Murray et al., 2021; Tyler & Fagan, 2008). Given the recent surge in diversion incidents, this study serves as an initial database concerning the perception of fairness among medical cannabis patients in Israel, offering insights into their relationship quality with authorities.
In practical terms, this study bridges the gap between legal frameworks and their perception among patients, providing critical insights into real-world practices. The ongoing shift toward medicalizing cannabis necessitates aligning its use with standard medical practices. As the research findings show, the medical cannabis policy in Israel creates legal distortions and a significant gap between what actually happens and the law. Athey et al. (2017) raised the question: “Does the pursuit of cannabis users stem from the desire to demarcate those who choose a lifestyle unlike our own?” Accordingly, the current study raises the question of whether the existing regulation in Israel is intended to ensure social rectitude regarding the use of cannabis, which is also commonly used for recreational purposes, but paradoxically harms patients who need cannabis for medical reasons. According to Reid (2022), beyond the legal consequences, the strict regulations toward patients may mainly lead to their stigmatization as non-normative people.
The model introduced in this study holds promise for policymakers within health ministries and law enforcement. It illuminates the disparities between legal perceptions and public viewpoints and identifies associated variables. These findings offer valuable insights that can inform adjustments aimed at enhancing patient services and refining regulations to better align with the evolving landscape of medical cannabis usage. They serve as a foundation for establishing policies and regulations specific to medical cannabis in Israel and provide broader implications for similar considerations worldwide.
Supplemental Material
sj-docx-1-cad-10.1177_00111287241237980 – Supplemental material for Explaining Medical Cannabis Diversion Among Medical Cannabis License Holders: A Moderation Model
Supplemental material, sj-docx-1-cad-10.1177_00111287241237980 for Explaining Medical Cannabis Diversion Among Medical Cannabis License Holders: A Moderation Model by Vered Ne’eman-Haviv and Ron Paz in Crime & Delinquency
Supplemental Material
sj-docx-2-cad-10.1177_00111287241237980 – Supplemental material for Explaining Medical Cannabis Diversion Among Medical Cannabis License Holders: A Moderation Model
Supplemental material, sj-docx-2-cad-10.1177_00111287241237980 for Explaining Medical Cannabis Diversion Among Medical Cannabis License Holders: A Moderation Model by Vered Ne’eman-Haviv and Ron Paz in Crime & Delinquency
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.