
Abstract
Youth with mental disorders, especially those involved in the criminal justice system, experience violent victimization at greater rates when compared to the general population. Despite this, few studies examine mediating factors drawn from criminological theory to explain why this population experiences victimization at greater rates than the general population, nor identifies factors that explain differential risk for violent victimization based on disorder type. Using the Pathways to Desistance Study, a longitudinal study of 1,354 adjudicated adolescent offenders, direct and indirect effects of factors drawn from lifestyles/routine activities and control perspectives using path analyses are estimated to understand if they mediate the relationship between two different disorder types (mood and substance usage/dependence disorders) and violent victimization. For both disorder types, direct and indirect effects of proximity to motivated offenders significantly increased the odds of victimization and fully mediated the relationship between disorder type and victimization. Mechanisms linking mood and substance usage disorders to victimization suggest that this population are more likely to be victimized because of key elements connected to lifestyles/routine activities theory. Control perspectives, on the other hand, did not mediate the relationship between mental illness and violent victimization. Implications for interventions, theory, and future research are discussed.
Introduction
According to the 2022 National Victimization Crime Survey report, the rate of violent victimization events of persons aged 12 years or older rose from 16.5 victimizations per 1,000 persons in the previous year to 23.5 per 1,000 persons (Thompson & Tapp, 2023). Violent victimization, often a general term used to capture various forms of violent behavior that is perpetrated against someone, includes violent crimes like simple assault, aggravated assault, robbery, and sexual assault (Thompson & Tapp, 2023). These rates are especially problematic when accounting for mounting evidence demonstrating that certain subsets of the population—like people with mental illness—are more likely to experience violent victimization when compared to the general population (Desmarais et al., 2014; Silver et al., 2011). In fact, a recent meta-analysis demonstrated this populations’ violent victimization rate was four to six times greater when compared to the general population (see de Vries et al., 2019). Research has also established that youth with mental disorders experience greater rates of victimization (Turner et al., 2013)—with prevalence rates of victimization for justice-involved youth with mental illness ranging from 16% to 50% depending on measurement and type of charge (Aebi et al., 2015).
Unfortunately, there is also an understanding that experiencing violent victimization early in one’s life is often associated with severe, long-term physical and/or psychological problems. For example, researchers established several consequences associated with adolescent victimization including: worsening mental health symptomology; impacting one’s self-worth or health; and participating in deviant behaviors like offending or substance usage (Farrell & Zimmerman, 2017). For justice-involved youth experiencing mental health problems, some consequences are even more severe including: being psychiatrically hospitalized; engaging in non-suicidal self-injury; experiencing suicidal ideation; struggling with school and overall well-being; and engaging in deviant behaviors conducive to victimization experiences (Auerbach et al., 2017).
Considering that a disproportionate amount of victimization events are experienced by youth with mental disorders, it is critical to understand why this subpopulation is at a heightened risk for violent victimization. One notable gap in the existing research base on mental illness and violent victimization is the lack of identifying potential mediating factors from criminological theories, despite calls for research to do so (see Silver, 2006). This is an important line of inquiry, as interventions can be designed to target mechanisms that link mental illness to violent victimization. This could indirectly lead to reducing victimization events and negative outcomes for this population.
Although prior research has explored how traditional criminological theories—including general theory of crime, strain, social disorganization, or social learning theories (to name a few)—can be applied to victimization in the general population (Gottfredson, 2021; Schreck & Berg, 2021), there is limited research on how these theories may apply to victimization of youth with mental disorders. Doing so is important, as prior research has highlighted how this population has a unique set of risk and protective factors connected to victimization that are derived from having a mental disorder and are not shared with the general population (e.g., disorder classification, hospitalization, and conflicted relationships; Silver, 2002; Silver et al., 2011).
Two theoretical explanations that may be useful to understand why violent victimization risk is heightened for youth with mental disorders are: lifestyles/routine activities theory (L/RAT; Cohen & Felson, 1979; Hindelang et al., 1978) and control perspectives (Gottfredson, 2021; Gottfredson & Hirschi, 1990; Hirschi, 1969). Indeed, the L/RAT framework has been applied extensively to understand victimization experiences (see McNeeley, 2015 for review), and recent work has extended the applicability of self-control perspectives to victimization (Gottfredson, 2021)—showing that low self-control is a significant predictor of victimization (Pratt et al., 2014; Schreck, 1999). Other control perspectives, such as social control theory (Hirschi, 1969), have also been connected to victimization demonstrating that weak social ties increase the risk of victimization (Popp & Peguero, 2021). Because of empirical support for coupling lifestyles and control frameworks in explaining victimization for the general population (Turanovic et al., 2015), these perspectives provide ample opportunity to explore how they link to mental illness and violent victimization. For these reasons, the current study investigates potential mediating factors drawn from L/RAT and control perspectives to understand if/how these mechanisms contribute to violent victimization for especially at-risk youth—justice involved youth with mental disorders.
Lifestyles/Routine Activities Theory, Control Perspectives, and Victimization
Scholars have drawn on perspectives highlighting situational risk—like L/RAT or social control (Cohen & Felson, 1979; Hindelang et al., 1978; Hirschi, 1969)—and dispositional risk—like self-control (Gottfredson, 2021)—to understand contributing factors associated with victimization within the general population. Briefly, L/RAT highlights that there is a direct link between one’s lifestyle and exposure to victimization risk, with risk varying based on demographics and an emphasis on the convergence in time and space of three key factors including: motivated offenders, suitable target, and lack of capable guardians (Cohen & Felson, 1979; Hindelang et al., 1978). Thus, a core argument of L/RAT is that subgroups of the population have differential lifestyles, that vary because of demographic, trait, or environmental differences, which have varying effects on exposure to persons in high-risk times, places, and people (Pratt & Turanovic, 2016). Although early work using L/RAT focused on the differential risk of victimization based on demographic factors, there has been considerable push to consider dispositional factors, like self-control, among variables of interest when examining victimization (Daigle et al., 2008; Pratt et al., 2014; Schreck, 1999).
Alternatively, control perspectives are generally grounded in the assumption that it is human nature to pursue one’s self-interest. Because of this assumption, one type of control theory—general theory of crime (Gottfredson & Hirschi, 1990) and modern extensions—argues that people with lower levels of self-control are predisposed to engage in a host of criminogenic behaviors including victimization (Gottfredson, 2021). In other words, self-control may impact victimization in a number of ways including influencing one’s routines (Schreck, 1999), lifestyles (Schreck et al., 2006), and willingness to adjust behaviors following a victimization event (Turanovic & Pratt, 2013).
Relatedly, social control theory postulates that social ties to institutions and commitment to societal norms should decrease engagement in deviant behaviors (Hirschi, 1969), which may be conducive to victimization experiences. Specifically, Hirschi (1969) conceptualized social control theory based on the premise of four main elements: attachment to others (e.g., ties to others like adults and family), commitment to conventional lines of action (e.g., ties to activities like school, work), involvement in conventional activities (e.g., time devoted to activities), and belief in legitimate order (e.g., values/accepts conventional values; Hirschi, 1969). Thus, for youth with weaker ties to society, the potential to engage in risky behaviors conducive to victimization increases, thereby heightening the risk of experiencing victimization. Notably, in a recent review of social control theory, Costello and Laub (2020) found for youth with less ties to variables that promote social control, the likelihood of delinquency, risky behaviors, and involvement with delinquent peers significantly increased. Attachment to capable guardians like parents, schools, or pro-social peers, however, decreased. Consequently, the risk of victimization is heightened.
Despite prior research on the link between L/RAT and control perspectives with victimization in the general population, little is known on how these theories may connect to increased risk of victimization for youth experiencing mental health problems. This omission is surprising considering that research has shown that youth with mental disorders—especially those already involved in the justice system—are at a higher risk of engaging in risky behaviors and/or being influenced by deviant peers that are conducive to violent victimization (e.g., substance usage and offending; see Seitz et al., 2019 for review). Further, this subpopulation also exhibits lower levels of self-control when compared to the general population (Wolff et al., 2013) and often face disconnection from key institutions (Draine et al., 2002). In fact, over the past few decades, researchers have explored factors that increase the risk of experiencing violent victimization for people with mental illness. In general, risk factors identified typically fall into one of the following categories including: (1) clinical (e.g., disorder classification, hospitalization); (2) demographic (e.g., SES); (3) situational (e.g., substance usage, offending); (4) dispositional (e.g., psychopathy); and (5) theoretically-derived risk factors (e.g., conflicted relationships; Daigle et al., 2020; Harris et al., 2022; Johnson et al., 2016; Silver, 2002; Silver et al., 2011; Teasdale, 2009). Collectively, findings suggest that a large portion of risk factors associated to violent victimization are shared with the general population, with the acknowledgement that having a mental disorder is also associated with a unique set of risk factors specific to mental health (e.g., disorder classification, medication noncompliance, and hospitalization). Because of this, it is currently unknown if L/RAT or control theories used to examine violent victimization in the general population are also relevant for justice-involved youth with mental illness.
Mental Health, L/RAT, Self-Control, Social Control, and Victimization
Together, there are reasons to suspect mechanisms derived from L/RAT and control perspectives apply to victimization of justice-involved youth with mental illness. First, there is some empirical support for L/RAT contributing to victimization risk of youth with mental disorders. Specifically, Azimi and Daigle (2021) found some support for partial mediation on the relationship between violent victimization and mental illness once drug use and sexual activity were incorporated. Although Azimi and Daigle’s (2021) study has several strengths, there are some limitations worth mentioning. First, mental health variables were self-reported symptoms of depression, ADHD, and anxiety, limiting inferences on severity and functioning differences if diagnostic criterions are used. Second, one externalizing disorder was included limiting information on other types of externalizing disorders like substance abuse/dependence disorders (e.g., SUDs), which are often associated with participation in risky or antisocial behaviors that are conducive to violent victimization (Kim et al., 2019). Third, two components of RAT were used, limiting inferences on target suitability, which may be especially relevant for this subpopulation. These limitations are important to address, as doing so could highlight other mechanisms for change in prevention efforts that are specific to this population.
Second, it is possible that factors associated with mental disorders may impact factors proposed in L/RAT and control perspectives. For example, L/RAT highlights the idea of target suitability, with reconceptualization’s focusing on components of target suitability like vulnerability and antagonism (Finkelhor & Asdigian, 1996). Given that symptoms of mental disorders may impede cognitive processing and risk recognition, motivated offenders may perceive this population as suitable targets. If this is indeed the case, clinical risk factors, like heightened mental health symptomology, that signal possible functional impairment or the inability to recognize situations conducive to victimization, could also be proxies for target suitability as suggested in prior research (see Teasdale, 2009; Teasdale et al., 2021).
Researchers have also found that people with mental illness have lower levels of self-control when compared to the general population (Wolff et al., 2013), perhaps linked to disinhibitory characteristics that underly some mental disorders. Unfortunately, Baumeister et al. (1994) argue that people suffering from symptomology related to mental illness (e.g., depressive, anxious, and delusional states) are sometimes preoccupied with their internal world. This preoccupation with one’s internal world inhibits the cognitive resources needed for self-regulatory behaviors like self-control. In fact, research has noted the cognitive deficits associated with some mental disorders impedes executive functioning, thereby interfering with social, emotional, and daily functioning (Knight et al., 2020). As argued in the general theory of crime, people with lower self-control are predisposed to engage in criminogenic behaviors and increases the risk of violent victimization (Gottfredson, 2021; Gottfredson & Hirschi, 1990).
Furthermore, research has also shown that people with mental disorders are often disconnected from key elements found in social control perspectives. For example, Tracy and Biegel (2006) show in their systematic review that across studies, the social networks of people with mental disorders are often significantly smaller, weaker, and unstable when compared to the general population. Smaller networks, compounded with the likelihood that such social networks of this population are often conflicted in nature (Silver, 2002), significantly increases the risk of violent victimization. Consequently, these networks, in general, may be less capable to provide the degree and type of support that is sometimes needed for psychological well-being (Kawachi & Berkman, 2001; Tracy & Biegel, 2006). Similarly, adolescents with mental disorders are often less attached or involved in institutions like the school. Specifically, youth with mental disorders are more likely to have higher rates of missing school, being suspended, and dropping out of school, while exhibiting lower educational achievement (Dalsgaard et al., 2020). Thus, one’s ties to relationships and institutions are significantly impaired. As such, weaker ties to conventional society increases the likelihood of engaging in risky behaviors conducive to violent victimization risk.
Finally, L/RAT and control perspectives may have a differential impact on violent victimization depending on diagnostic type. For example, people with mood disorders (e.g., forms of depression and anxiety) may internalize psychological distress. This internalization can lead to an over-reliance on either social support networks or maladaptive coping strategies to cope with these negative emotions (Meyer, 2001). As Silver (2002) argues, when the social networks of people with mental illness are fraught with conflicts, the risk of experiencing violent victimization is significantly heightened. This can occur either through engaging in risky behaviors as a means to alleviate negative emotions or as a result of violent victimization within the network itself. Additionally, adolescents with mood disorders who engage in maladaptive coping mechanisms may experience reduced levels of self-control, affecting elements of social control, as previous research suggests (Turanovic & Pratt, 2013). In contrast, youth with SUDs, who often exhibit externalizing behaviors like offending, may already be considered vulnerable targets. This is particularly true when they associate with networks that have high rates of delinquency, increasing the likelihood of encountering motivated offenders (Schreck et al., 2004). Collectively, it is possible that there are differing mediating mechanisms associated with disaggregating disorder types and violent victimization.
Current Study
Despite the importance of understanding if elements in criminological theories like L/RAT or control perspectives mediate the relationship between mental disorder and violent victimization, limited research has explored this topic (for exception see Azimi & Daigle, 2021). Further, it is unclear how mechanisms drawn from these theories may differentially impact different types of disorders. This gap in the literature is important to identify, especially when accounting for recent heightened rates of violent victimization among youth (Turner et al., 2013), and justice-involved youth with mental disorders (Aebi et al., 2015). For these reasons, the connection between mental disorders and heightened rates of violent victimization are explored using an adjudicated, adolescent sample, with the hopes of identifying mediating mechanisms that can be targeted for change. Based on theoretical and empirical findings associated with mental health and violent victimization, the current study investigates three research questions: (1) Does having a mental disorder increase the risk of violent victimization for justice-involved youth?; (2) What factors drawn from L/RAT and control perspectives mediate the relationship between mental illness and violent victimization?; and (3) Do mediating factors vary based on diagnostic criteria and the occurrence of violent victimization?
Data and Sample
Data were drawn from the Pathways to Desistance Study (i.e., Pathways), a multi-site (Philadelphia, PA and Maricopa County, AZ), longitudinal study of 1,354 adjudicated youth (Mulvey, 2004). Eligibility for the study included youth between 14 and 17 years old at the time they committed their offense, and found guilty of a serious offense (predominately felonies). Recruitment of participants took place between 2000 and 2003, and adolescents were interviewed shortly after their adjudication hearing, and then were interviewed 10 times for follow-up interviews. The first six follow-up interviews were conducted every 6 months, totaling 3 years. Follow-up interviews were then conducted every 12 months, with data collection continuing through 2010. Data were collected at either participants’ homes, public places, or in facilities and computer-assisted interviews were used. Importantly, self-reported information was supplemented and validated through the use of official record information and interviews with collateral informants.
For the current study, measures of mental disorders, potential mediating factors, and demographic information were drawn from the baseline wave. Although it would be preferable to use the subsequent wave for the mediators, a large amount of missing data prevented doing so. 1 Given this limitation, the mediators were all bound by the previous 6 months, while measures of mental illness are lifetime, in an effort to establish temporal ordering. Waves 1 through 6 were collapsed together to examine violent victimization given that victimization is a rare event (see Daigle et al., 2016) and aligning with prior studies using these data to examine violent victimization (Daigle & Harris, 2018). 2
Lastly, it is important to highlight that the Pathways dataset is comprehensive and includes validated measures of mental illness, interpersonal violence, engagement in antisocial behaviors, individual characteristics, personal relationships, and demographic information. There are several reasons why this dataset is valuable for addressing the research questions of the current study. First, the dataset’s offender-based sample offers variation on factors like mental disorders, engagement in risky/deviant behaviors, impulsivity, and victimization, which allows understanding for how differing levels of these factors contribute to victimization risk. Second, the average age of the sample (e.g., 16 years) is a critical time period in which violent victimization is more likely to occur (Demaris & Kaukinen, 2005). Finally, because many criminological theories either originated from or were applied using high-risk subsamples that were involved in deviant behaviors or the criminal justice system at high-rates (e.g., Agnew, 1992), this dataset aligns with original testing of criminological theories.
Measures
Dependent Variable
Violent victimization includes six violent victimization events including: being chased, beaten up, attacked with a weapon; raped or sexually attacked; shot at, or shot and hit. If the participant had experienced a victimization event in waves 1 to 6, they were coded as 1 and coded as 0 if otherwise.
Key independent Variables
Measures of mental disorders are based on a modified version of the Composite International Diagnostic Interview (e.g., CIDI; Kessler et al., 2009), a fully structured interview in which trained lay interviewers generate clinical diagnostic estimates of DSM-IV disorders. Two measures were used at baseline from CIDI. Participants were asked a series of screening questions assessing symptoms of these eight selected mental disorders. If the participant selected positive responses to the screening items, detailed questions to assess if the endorsed symptom is part of a psychiatric symptom or due to something else (like medication and drugs) were then asked. Additional questions to establish onset and recency of the symptoms are subsequently asked if the questions endorsed occur in a pattern that suggests a diagnosis may be present. Two measures related to mental illness are included. First,mood disorders were grouped together, including major depression, dysthymia, post-traumatic stress disorder, and mania (coded as a 1 if participant met diagnostic criteria and coded as 0 otherwise). 3 Substance usage disorders (SUD) are captured if a participant met the diagnostic criteria for alcohol abuse, alcohol dependence, drug abuse, and drug dependence during their lifetime (coded as 1 if met criteria and coded as 0 if otherwise).
L/RAT Potential Mediators
Five mediators reflecting L/RAT were included. First, engagement in risky behaviors was assessed through the measure of crime perpetration, which included engagement in 21 illegal and antisocial activities (e.g., stealing a car, damaging/destroying property) during the previous 6 months (α = .85). If the participant indicated that they had engaged in one of these behaviors within the past 6 months, they were scored as a (1), and scored as a (0) if otherwise. Second, target suitability is evaluated through the use of a symptomology measure, in line with prior scholarship (Johnson et al., 2016; Teasdale, 2009). Specifically, the global severity index (GSI) drawn from the Brief Symptom Inventory scale (BSI) was used. Briefly, the GSI combines the number of symptoms as well as the intensity of perceived distress. Higher scores on the GSI indicate greater psychiatric distress. 4 Motivated offenders were examined through the measure delinquent peers, as prior research has found that having social ties to delinquent peers significantly increases the risk of a victimization event and is commonly used to proxy motivated offenders (Schreck et al., 2004). The peer delinquency scale includes 19 items, assessing the number of antisocial behaviors ones’ peers engaged in during the last 6 months (e.g., “during the last 6 months how many of your friends have sold drugs?”). Response options ranged from (0) none of them to (4) all of them. The peer delinquency scale was created by taking the mean of the 19 items, where higher scores indicate greater number of delinquent peers (α = .94). To examine lack of capable guardianship,unstructured activities and parental monitoring measures are used. Four questions examined the degree of absence of an authority figure (e.g., “how often did you get together with friends informally?”). Response options include (1) never to (5) almost every day. The mean of the four items was taken to create an unstructured activities measure, so long as there is valid data on three of the four items (α = .62). Higher scores indicate greater time spent in unstructured socializing. 5 Parental monitoring consists of four items (e.g., “how often do you have a set time to be home on the weekends?”). Response options include (1) never to (4) always. The mean of the four items was taken, so long as there was valid data on three of the four items. Higher scores indicate greater degrees of parental monitoring. 6
Control Perspectives Potential Mediators
Six mediators reflecting control perspectives were used. First, the impulse control subscale was used to assess self-control from the Weinberger Adjustment Inventory. The impulse control subscale includes eight items (e.g., “I will try anything once even if it is not safe”). Responses ranged from (0) false to (4) true. The measure,self-control, was created by taking the mean of the eight items, so long as six of the eight items had valid scores (α = .76). Higher scores reflect greater impulsivity (e.g., lower levels of self-control). To examine the social control perspective, four measures related to attachment and one measure associated with involvement were used.Domains of non-family support is included in which participants were asked about eight different domains (e.g., adults you admire and want to be like and adults you could talk to if you needed information or advice about something). The domains of non-family support measure is a count of the number of domains in which at least one non-family member was mentioned.Maternal attachment is measured through nine items (e.g., “how often does your mother let you know she really cares about you”). Response options range from (1) never to (4) always. The mean of the nine items was taken, so long as there was valid data for seven of the nine items. Higher scores indicate greater parental attachment provided by the participant’s mother (α = .92). 7 School attachment is measured through seven questions were asked to evaluate the participant’s educational experience (e.g., “schoolwork is very important to me”). Response options ranged from (1) strongly disagree to (5) strongly agree. The mean of these seven items was taken, where higher scores indicate greater attachment to school (α = .83). 8 Bonding to teachers is measured through three questions (e.g., “most teachers treat me fairly”). Response options range from (1) strongly disagree to (5) strongly agree. The mean of the three items was taken (α = .65), where higher scores indicate greater degree of bonding to one’s teachers.Involvement in extracurricular school activities was included as a count measure of total number of activities. Higher scores indicate greater participation in extracurricular school activities.
Control Variables
Several control variables are also included at baseline. Demographic control variables included age, race (White, Black [referent group], Hispanic, and Other), biological sex (male coded as 1), socioeconomic status (calculated based on the parent’s education and occupation level), and site (1 = Philadelphia). A measure of baseline victimization (1 = victimized at baseline) is also included encompassing the same six violent victimization events as the dependent variable.
Analysis
Analyses for this study involves several steps. First, multiple imputations—using the MI command suite in Stata 18—were used to account for missing data. 9 Specifically, using chained equations, 40 imputed datasets were pooled for analyses in which participant’s previous observed values are used to predict missing values (Schafer & Graham, 2002). Second, chi-square or t-tests were used to establish if there were significant group differences between youth with and without mental disorders on all of the included variables. Third, multivariate logistic regression models were used to investigate the independent impact of proposed mediating variables from each criminological theory on the key independent variables—mood disorders and substance usage disorders (SUDs)—and violent victimization. 10
To test for mediation, two stages were employed. In the first stage, path analyses in a structural equation modeling framework were used. Specifically, path models were examined in SPSS (v. 28) using the PROCESS macros package (Hayes, 2013; Preacher & Hayes, 2008). The PROCESS model allows to test direct and indirect effects simultaneously in one model, and was used to calculate the total, direct, and indirect effects. Because the PROCESS model only allows up to 10 mediators, a second stage was used to calculate the total, direct, and indirect effects of all potential mediators on the relationship between mental disorder and violent victimization. Thus, in the second stage, coefficients of the total, direct, and indirect effects of mental illness’ on violent victimization were calculated using the ldecomp command in Stata 18.Ldecomp allows for use of multiple mediators of any distribution and a binary outcome, using bootstrap standard errors to create estimates for the indirect and direct effects of the independent variable through mediators to the dependent variable (Buis, 2010). 11
Results
After multiple imputations, the total analytic sample includes 1,354 adolescents, in which 198 met the diagnostic criteria for mood disorders, 610 met the diagnostic criteria for substance usage disorders (e.g., SUDs), and 685 did not meet the diagnostic criteria for a mental disorder. As shown in Table 1, over half of youth with mood disorders or SUDs were violently victimized during waves 1 through 6. For reference, 36% of youth without mental illness experienced victimization, a statistically significant difference between youth with and without mental disorders. Further, statistically significant differences emerged between youth with and without mental disorders on all of the mediators, consistently showing higher averages of L/RAT and impulsivity. The average age was approximately 16 years, and the majority were male and non-White (Table 2).
Descriptive Statistics (N = 1,354) a .
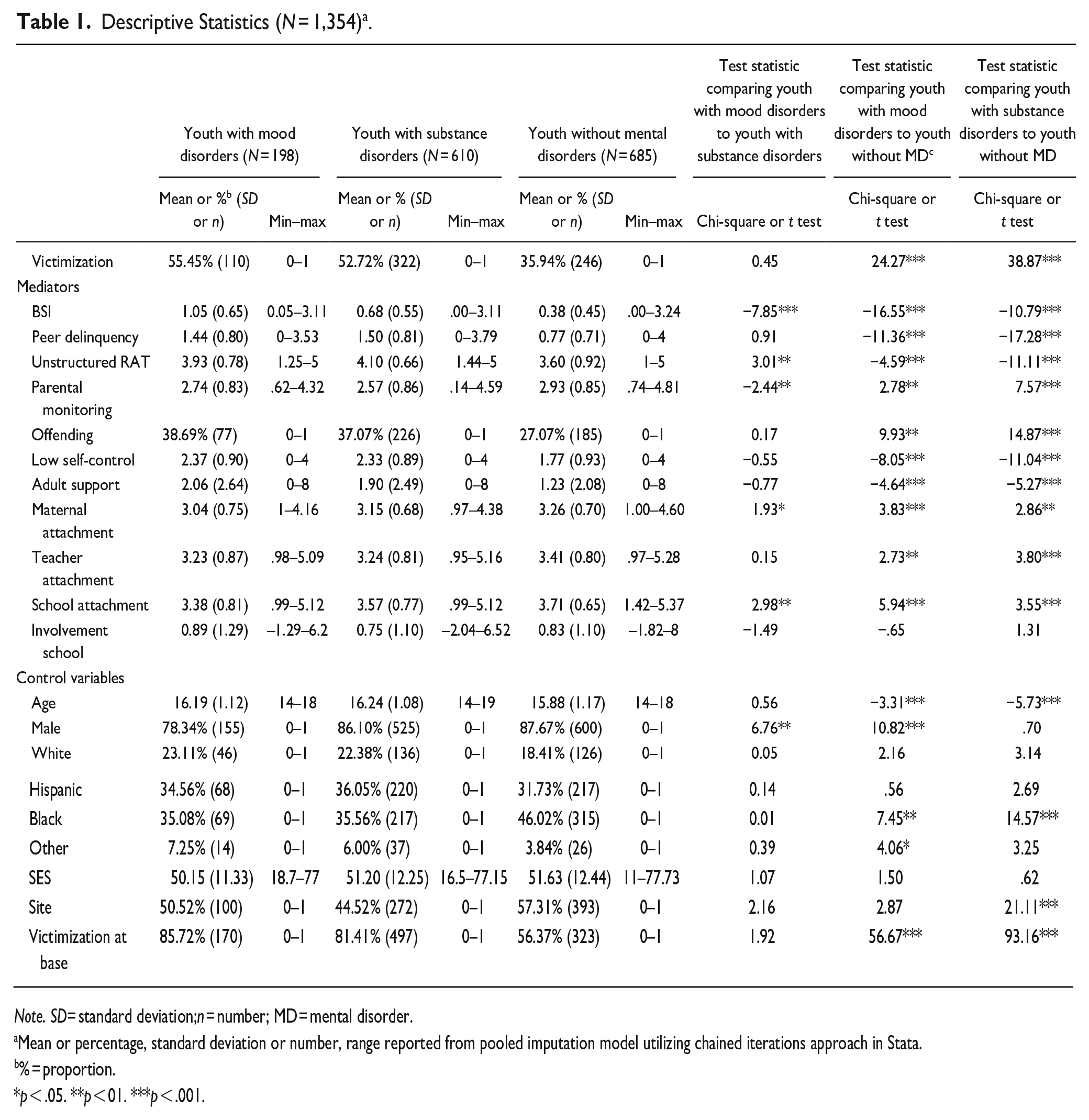
Note. SD= standard deviation;n = number; MD = mental disorder.
Mean or percentage, standard deviation or number, range reported from pooled imputation model utilizing chained iterations approach in Stata.
% = proportion.
p < .05. **p < 01. ***p < .001.
Correlation Matrix of Key Variables.
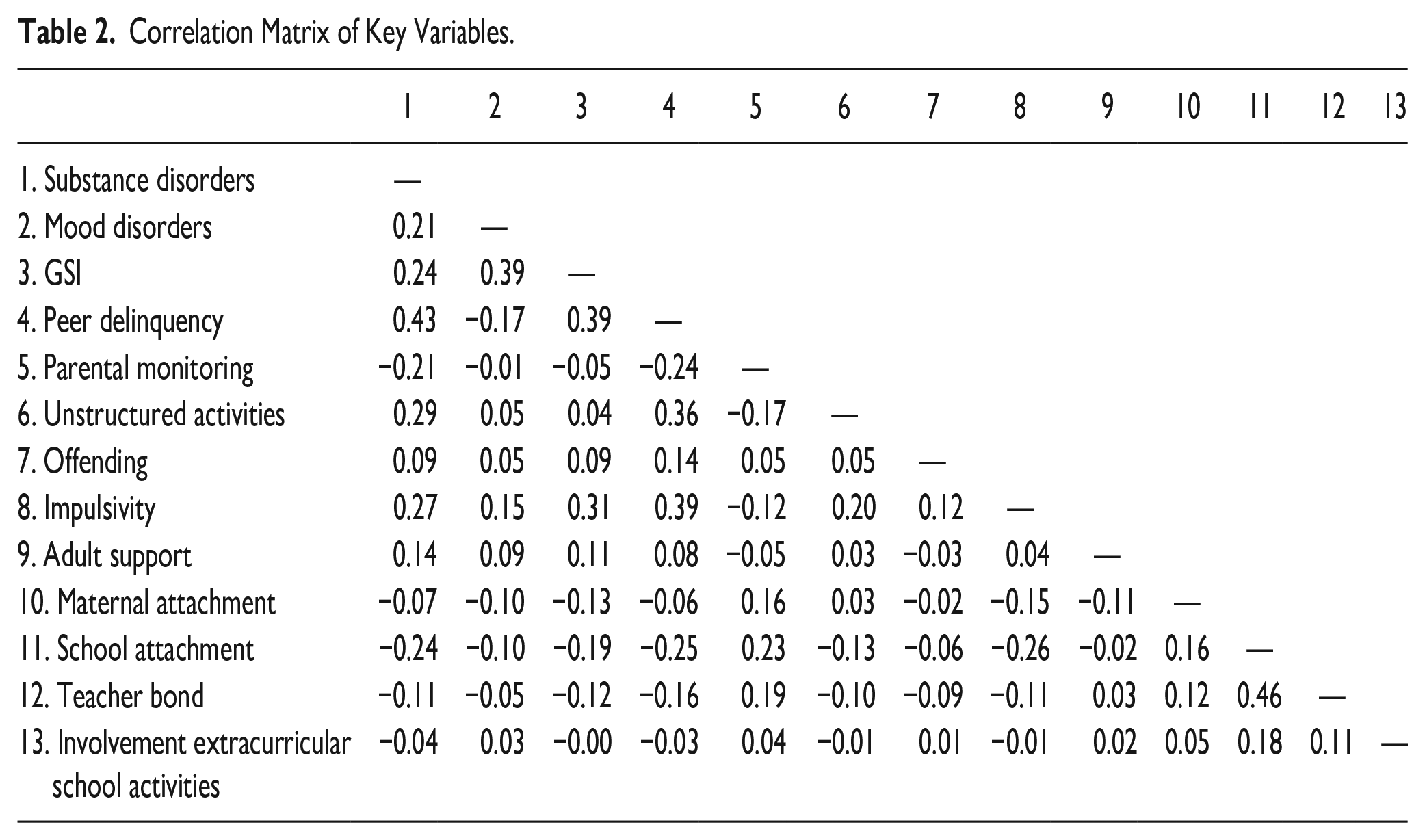
Table 3 displays the results of the independent impact of proposed mediators drawn on the relationship between mood disorders and SUDs on victimization. As shown in model 1 of Table 3, mood disorders (OR = 1.52,p < .01) and SUDs (OR = 1.61,p < .001) were both significantly associated with violent victimization. Each set of mediators were then incorporated into Table 3. As shown in model 2 of Table 3, only one mediator from L/RAT, peer delinquency (OR = 1.67/1.63,p < .001), emerged as significant for both models split based on diagnostic types. Model 3 of Table 3 shows that low self-control significantly increased the odds of victimization (OR = 1.28/1.25,p < .001). None of the social control measures were significant predictors of victimization (model 4, Table 3). Model 5 of Table 3 incorporates all mediators into the models. One mediator, peer delinquency (OR = 1.60,p < .001), was significant.
Multivariate Logistic Regressions Predicting Violent Victimization (N = 1,354).
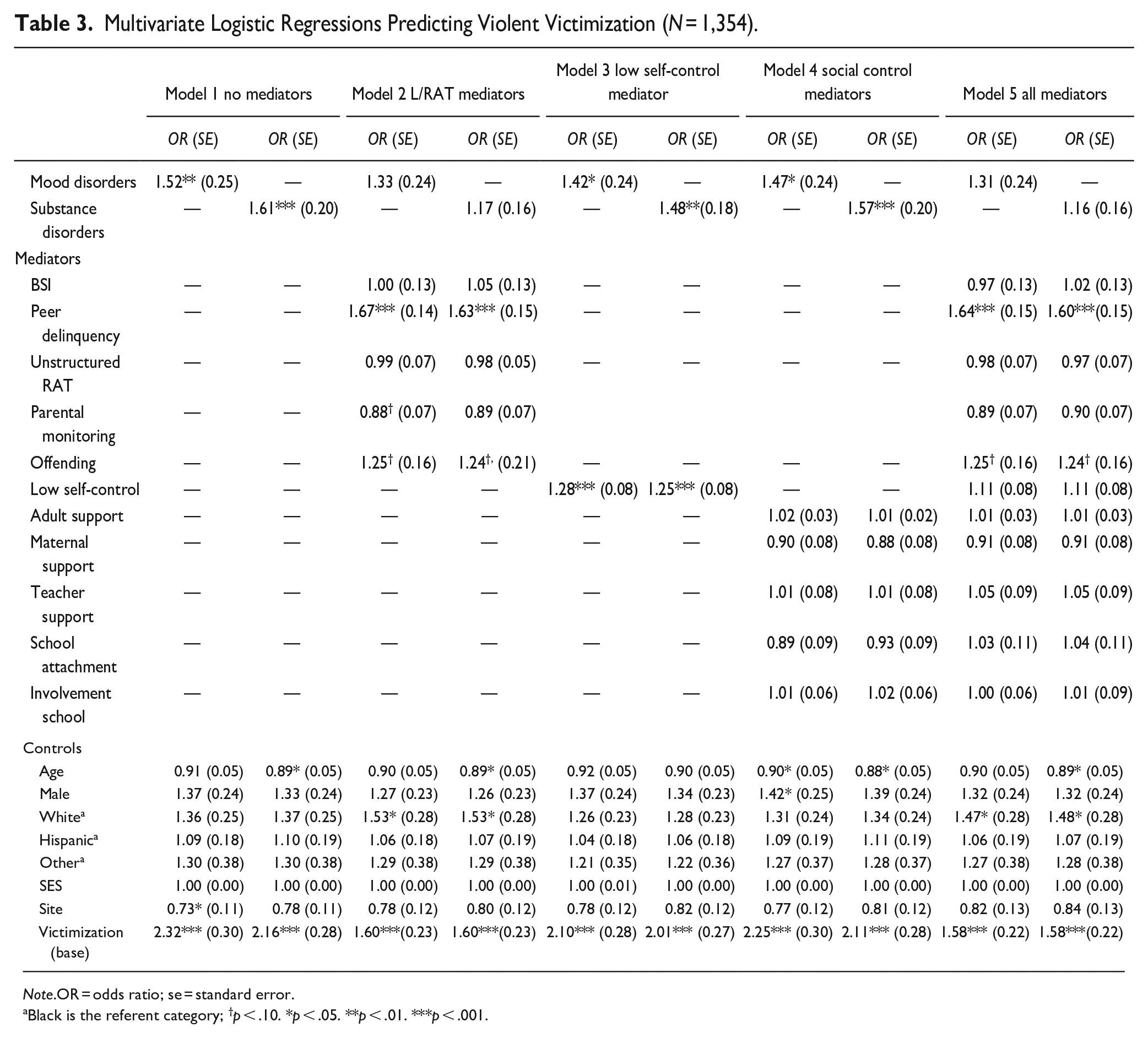
Note.OR = odds ratio; se = standard error.
Black is the referent category; †p < .10. *p < .05. **p < .01. ***p < .001.
Mediation (Path) Analyses
Path analyses were used to disentangle the total influence on mental disorder and violent victimization through proposed mediators into direct and indirect pathways (Hayes, 2013). Figures 1 through 5 displays the results. As shown in Figure 1, which shows the total effect of mental disorder on violent victimization, those with mood disorders (b = 0.42,p < .01) or SUDs (b = 0.59,p < .001) were significantly more likely to be violently victimized.

Direct effects of mental illness on violent victimization.
The second figure (Figure 2) presents the results of the direct and indirect effects of mental illness on violent victimization through L/RAT mediators. Adding L/RAT factors to the model reduced the mood disorder path coefficient from .42 to .23, and SUDs path coefficient from .59 to .20, and both paths to violent victimization were no longer significant. Despite strong path associations from mood and SUD’s to the proposed mediators, only one mediating factor, in turn, significantly predicted violent victimization. Specifically, mood disorders were strongly associated with peer delinquency (b = 0.22,p < .001), and peer delinquency, in turn, was significantly related to violent victimization (b = 0.49,p < .001). Similarly, SUDs were strongly associated with peer delinquency (b = 0.59,p < .001), and peer delinquency was then strongly associated with violent victimization (b = 0.47,p < .001). Thus, approximately 55% (.23/.42) and 34% (.20/.59) of the relationship between mood disorders, SUDs, and violent victimization was direct, and 45% and 66% operated through peer delinquency.
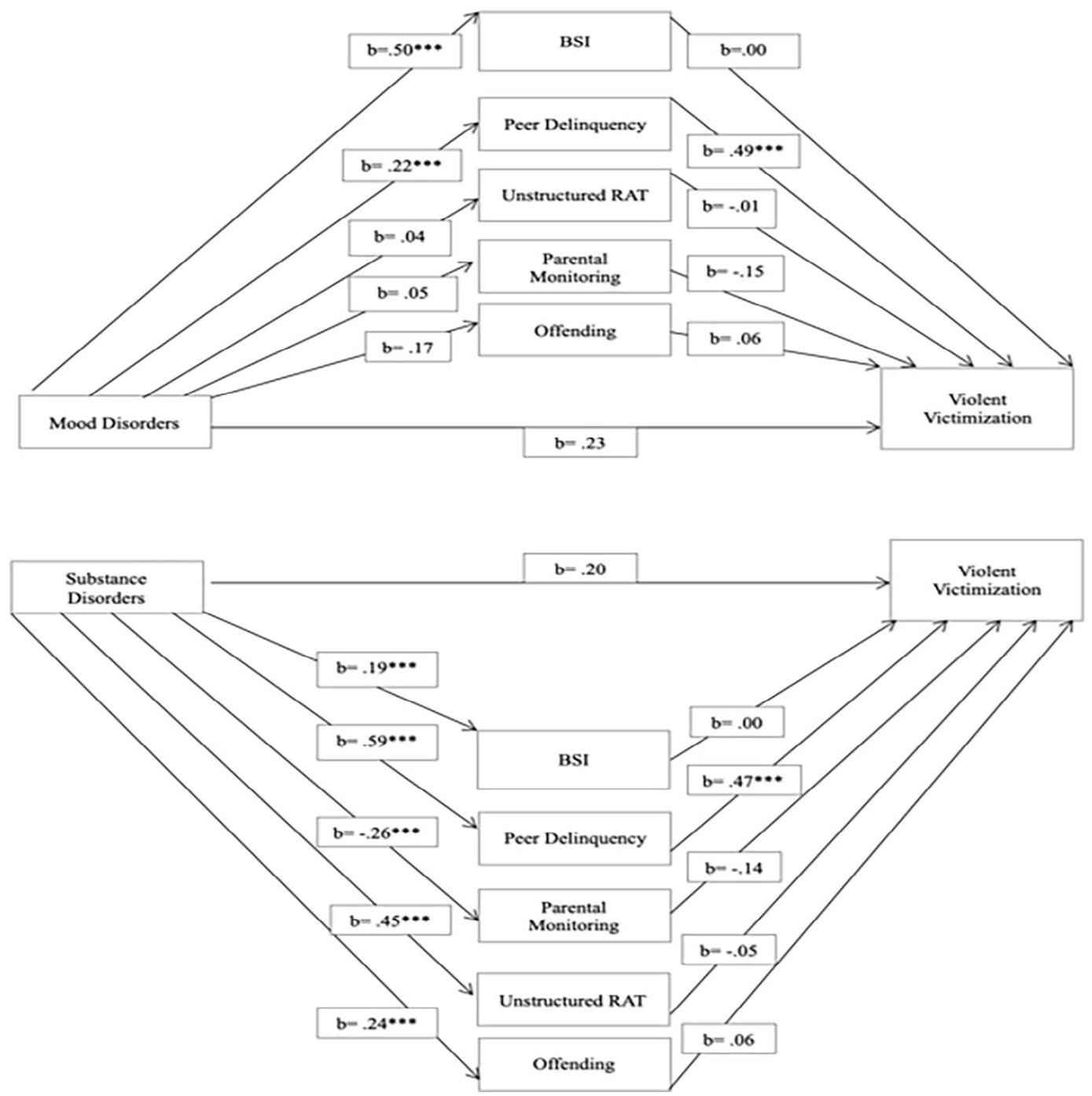
Direct and indirect effects of mental illness on violent victimization, through lifestyles/routine activities mediators.
Figure 3 displays the results of the direct and indirect effects of mental illness on violent victimization through the self-control mediator. Unlike the model with the L/RAT mediators, both the mood disorders (b = 0.35,p < .05) and SUDs (b = 0.39,p < .01) path coefficients to violent victimization remained significant, but were slightly reduced from Figure 1. Importantly, both mood disorders (b = 0.30,p < .001) and SUDs (b = 0.42,p < .01) were significantly associated with self-control, which self-control, in turn, was significantly associated with violent victimization in both the mood disorder (b = 0.25,p < .001) and SUDs paths (b = 0.23,p < .001). Thus, approximately 83% (.35/.42) and 71% (.42/.59) of the relationship between mood disorders and SUDs and violent victimization was direct, and 17% and 29% operated through self-control.
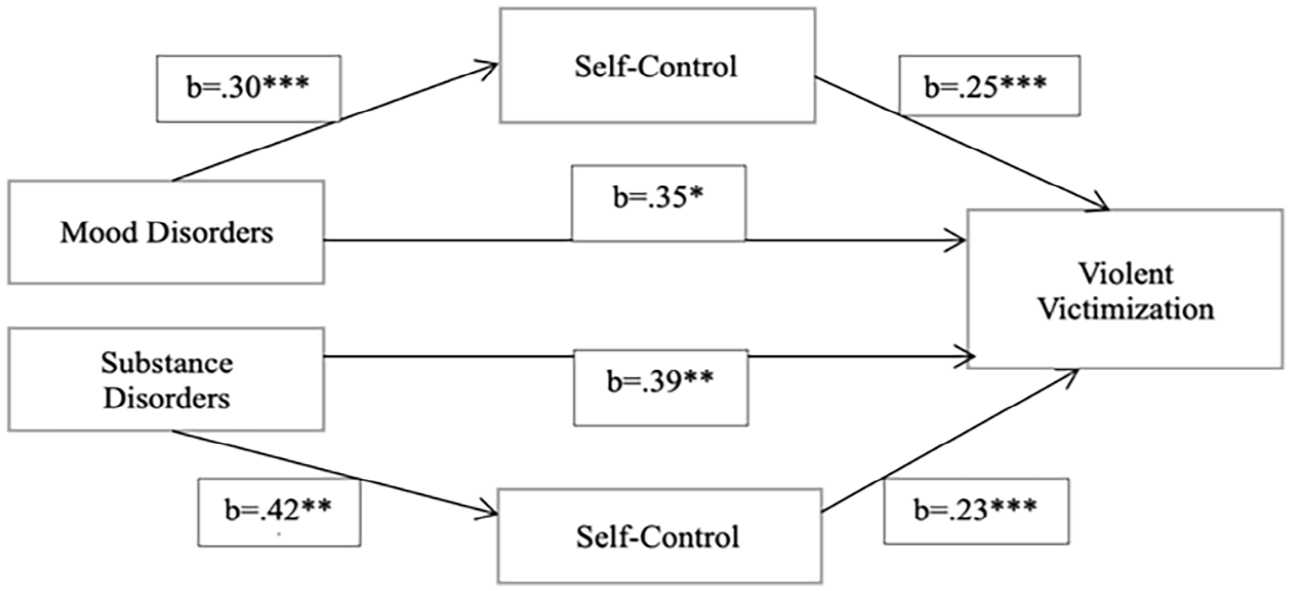
Direct and indirect effects of mental illness on violent victimization, through self-control mediator.
Figure 4 presents the direct and indirect effects of mental illness on violent victimization through the social-control mediators. The direct effect of mood disorders (b = 0.39,p < .05) and SUDs (b = 0.56,p < .001) on violent victimization remained significant. Despite some significant pathways from mood disorders and SUD’s to the social control mediators, none of the social control mediator paths were significantly associated with violent victimization.
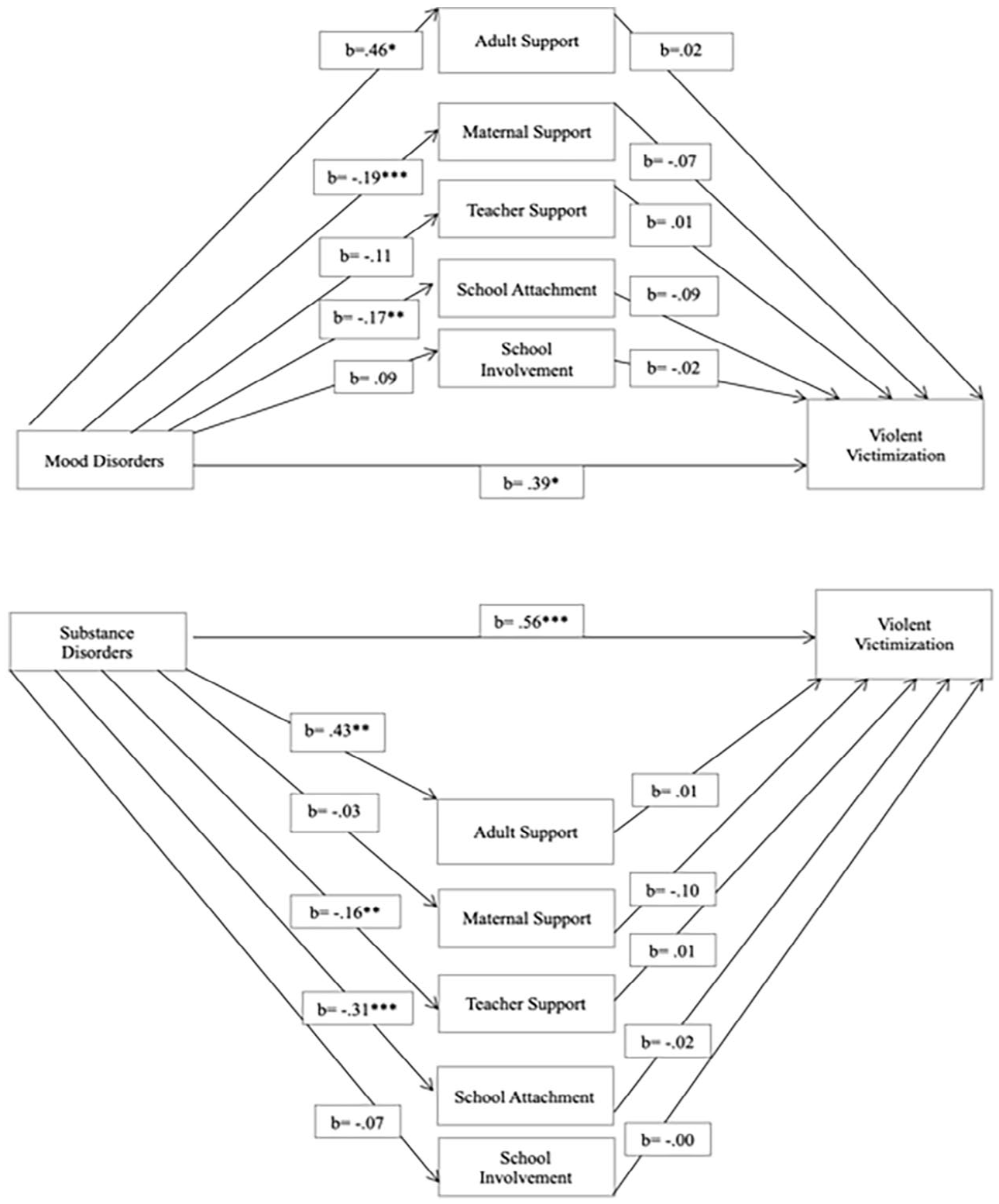
Direct and indirect effects of mental illness on violent victimization, through social control mediators.
Figure 5 displays the direct and indirect effects of mental illness on violent victimization through the L/RAT and self-control mediators. 12 The direct path of mood disorders (b = 0.22) and SUDs (b = 0.18) on violent victimization were both reduced to non-significance. Mood disorders were significantly associated with the BSI (b = 0.50,p < .001) and peer delinquency (b = 0.22,p < .001), but only the peer delinquency path, in turn, was significantly associated with violent victimization (b = 0.46,p < .001). SUD’s was significantly associated with all the L/RAT and self-control mediators, but only peer delinquency (b = 0.44,p < .001), in turn, predicted violent victimization. Thus, approximately 52% (0.22/0.42) and 30% (0.18/0.59) of the relationship between mood disorders and SUDs and violent victimization was direct, and 48% and 70% operated through peer delinquency.
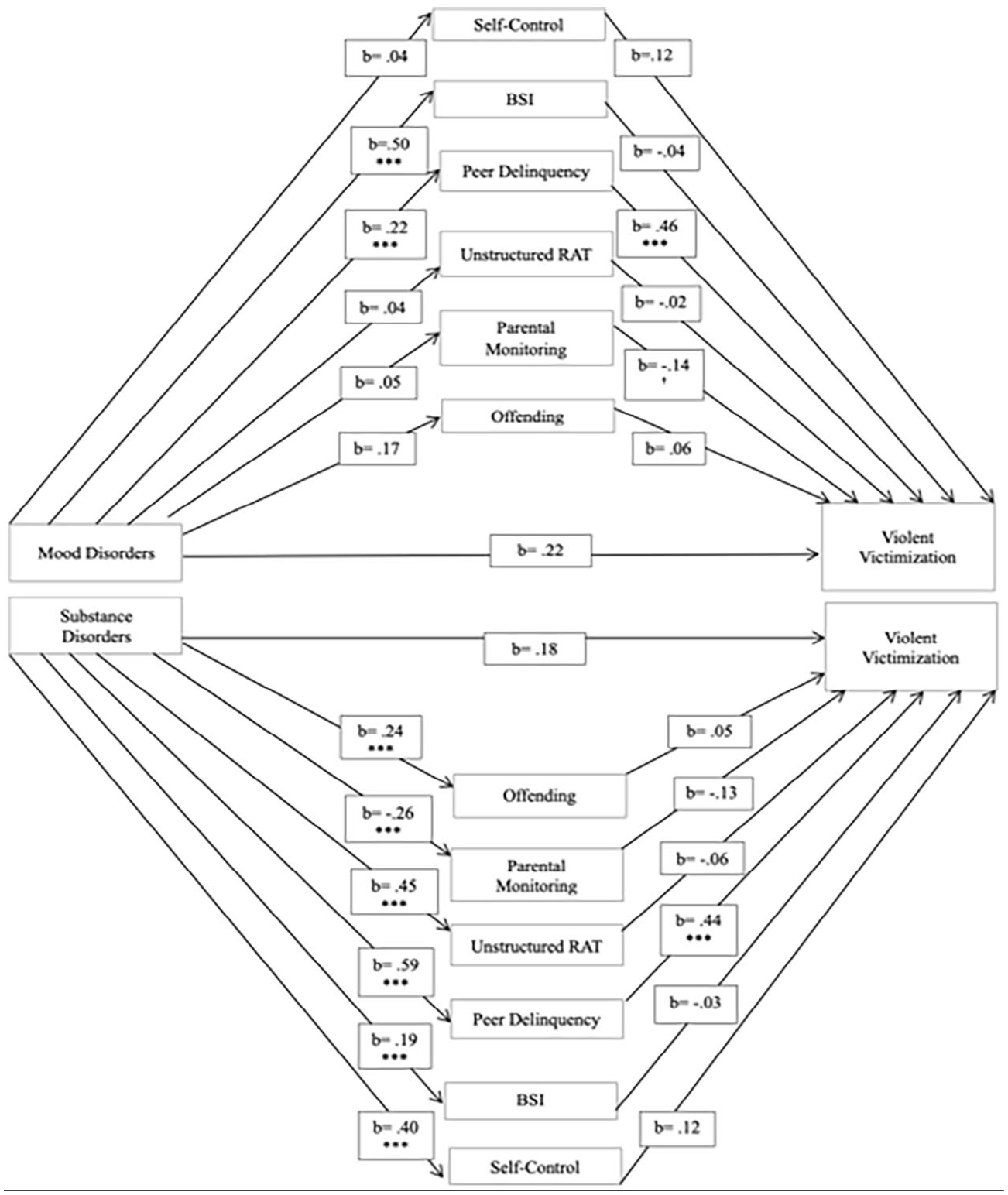
Direct and indirect effects of mental illness on violent victimization, through lifestyles/routine activities and self-control mediators.
Lastly, the total, direct, and indirect effects of all hypothesized mediators on the relationship between mental disorder and violent victimization were estimated using Stata’s command, ldecomp. As shown in Table 4, the indirect effects of all the mediators accounts for approximately 52% of the relationship between mood disorders and violent victimization, and 82% of the relationship between SUDs and violent victimization.
Total, Direct, and Indirect Effects of All Mediators on the Association Between Mental Illness and Violent Victimization (N = 1,354).
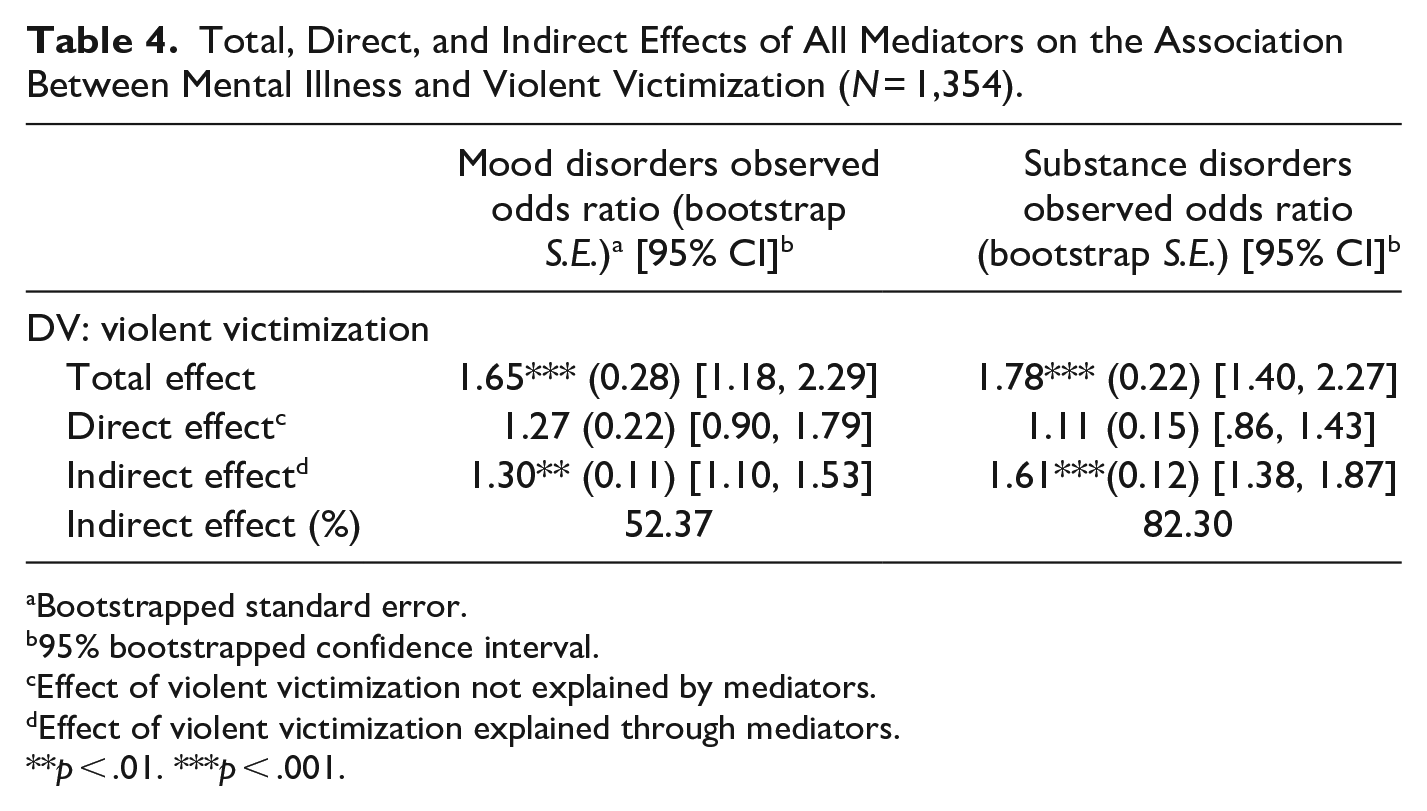
Bootstrapped standard error.
95% bootstrapped confidence interval.
Effect of violent victimization not explained by mediators.
Effect of violent victimization explained through mediators.
**p < .01. ***p < .001.
Discussion
Research has established that youth with mental disorders are at a greater risk to experience violent victimization when compared to the general population (Turner et al., 2013), which can increase the risk of experiencing adverse events later in one’s life course. Because of this, understanding why this population’s risk to experience violent victimization is important. Previous research has emphasized the distinctive risk and protective factors associated with violent victimization among youth with mental illness (Harris & Daigle, 2023; Teasdale, 2009). Considering the distinctive factors associated with violent victimization among those exhibiting signs of mental illness, it is reasonable to suspect that applications of criminological theories could yield differing results from the general population. For these reasons, the current study explored the impact of mediating factors drawn from L/RAT and control theories on the relationship between mental illness and violent victimization, contributing several main findings.
First, the risk of violent victimization for justice-involved youth with mental disorders was significantly higher when compared to youth without mental disorders. Specifically, over half of the sample of youth with mental disorders were violently victimized during the follow-up waves compared to approximately a third of youth without mental disorders experiencing victimization during the same time period, a statistically significant difference. At the multivariate level, having a mental illness significantly increased the odds of victimization by 52% for youth with mood disorders and 61% for youth with SUDs during the follow-up waves, holding constant demographic factors and baseline victimization. Differences in the predicted odds of victimization associated with the type of mental illness makes sense, especially when considering how expression and behaviors connected to psychological distress are accounted for.
For example, adolescents with SUDs may face increased vulnerability to victimization due to externalizing behaviors like drug usage and lack of capable guardianship. This assertion is supported by the statistically significant differences observed at the bivariate level, indicating that youth with SUDs generally exhibit lower levels of parental monitoring and higher averages of unstructured routines. Alternatively, youth with mood disorders may resort to maladaptive coping strategies as a means of managing intense internal stress or exhibit disinhibitory traits that significantly affect their executive functioning and self-regulation abilities (Baumeister et al., 1994; Meyer, 2001). As a result, their preoccupation with internal states may impede the cognitive resources required for engaging in self-regulatory behaviors and daily activities (Knight et al., 2020). Considering that the average symptomology measure for youth with mood disorders was significantly higher compared to those without, it is plausible that this subgroup may have a reduced likelihood of recognizing risks or implementing preventive strategies to protect against victimization (Turanovic & Pratt, 2013). Together, these findings emphasize the heightened risk of violent victimization among this subgroup, underscoring the need to identify mediating mechanisms that contribute to this elevated risk. By focusing on mediating factors linking mental illness and violent victimization during adolescence, interventions can be tailored to effectively reduce overall rates of violent victimization and mitigate negative long-term consequences for this population.
Second, only a few hypothesized mediators drawn from L/RAT and control perspectives had significant direct and indirect effects on the relationship between mental illness and violent victimization. Surprisingly, only one mediating variable drawn from L/RAT — proximity to motivated offenders (proxied through peer delinquency; Schreck et al., 2004) — was a contributing mechanism impacting the relationship between mood disorders, SUDs, and violent victimization. Specifically, as shown in the path analyses, 52% of the relationship between mood disorders and violent victimization was direct, and 48% of that relationship operated through proximity to motivated offenders, as proxied by peer delinquency. These effects were even greater for youth with SUDs. Specifically, 30% of the relationship between SUDs and violent victimization was direct, with an indirect effect 70% when accounting for peer delinquency.
There are a few reasons why youth with mental disorders (especially those who are involved in the justice system), whom have a network of delinquent peers, are especially at risk to experience violent victimization. First, these findings could be viewed through the lens of L/RAT, which argues that victimization is most likely to occur when three factors converge in time and space including being around motivated offenders, lacking capable guardianship, and being a suitable target (Cohen & Felson, 1979; Hindelang et al., 1978). As a reminder, the sample used for the current study involves youth whom are adjudicated for serious crimes. Research has shown that offenders tend to distrust others around them, including those they choose to co-offend with (McCarthy et al., 1998; Schreck et al., 2004). In the lens of social learning perspectives (Akers, 1998), which emphasize that individuals with similar mindsets and behaviors often gravitate toward one another, ties to delinquent peer groups not only increase the likelihood of co-offending and heightened engagement in delinquent behaviors but often signal a greater exposure to motivated offenders.
Although it could be argued that some peer groups may function instead as capable guardianship, it is noteworthy that the opposite may be true for delinquent peer groups. According to Schreck et al. (2004), the effectiveness of guardianship from a peer group relies on the willingness of those around the potential victim to actively engage in efforts and take the risk to potentially prevent a victimization experience. Research has shown, however, that delinquent peer groups are typically unwilling to accept the risk and potential sacrifice often required to prevent victimization (Gottfredson & Hirschi, 1990; Schreck et al., 2004).
Alternatively, it is also possible that involvement with delinquent peer groups can indicate their vulnerability as potential targets for victimization, which may be especially evident for youth with mood disorders. Research has already established that the social networks of individuals with mental illness, in comparison to the general population, tend to be smaller, unstable, and conflicted in nature (Silver, 2002; Tracy & Biegel, 2006). Conflicted social networks, in turn, increase the risk of violent victimization for people with mental disorders (Silver, 2002). Silver’s (2002) findings could be interpreted similar to the argument above. These relationships are increasing the presence of motivated offenders.
It could also be argued, however, that these networks, particularly those involving high rates of delinquent behaviors, may have limited capability to provide the necessary level of support for psychological well-being that may be especially important for youth with mental disorders (Kawachi & Berkman, 2001). Expanding on this idea, youth with mental disorders may require capable guardianship due to their increased vulnerability for victimization. This vulnerability stems from two main factors: (1) cognitive deficits that hinder the ability to recognize risky situations, and (2) behaviors linked to antagonism, which may unknowingly provoke attempts at social control when their symptoms are heightened (Felson, 1992; Silver, 2002; Teasdale et al., 2021). Additionally, youth with mental disorders may face additional cognitive deficits, further hindering their executive functioning (Knight et al., 2020). Consequently, perceptions of target suitability may be heightened from motivated offenders, thereby increasing the risk of victimization. Although the paths from mood disorders and SUDs to the proxy for target suitability (e.g., BSI) were highly significant, the global severity index measured through the BSI, did not, in turn, influence violent victimization. It is plausible, however, that the global severity index, which measures the degree of psychological distress, does not account for the potential antagonizing behaviors hypothesized to influence social control attempts that sometimes accompany higher degrees of psychological distress. Thus, future research would benefit by exploring other proxies of target suitability for this population, particularly focusing on antagonizing behaviors that may directly illicit social control attempts theorized to result in victimization (e.g., Felson, 1992).
Surprisingly, no other mediators drawn from criminological theories significantly impacted the association between mental illness and violent victimization, despite support when examining the general population. For example, a substantial body of research shows significant covariation between victims and offenders (Jennings et al., 2012). Because the victim-offender link has been replicated across samples, types of populations (including adults with mental disorders; Silver et al., 2011), and has been established as a mediating variable when understanding victimization in the general population (Chen, 2009), it is striking that offending did not emerge as a significant contributing mechanism in understanding why youth with mental disorders are violently victimized at higher rates.
Similarly, findings connected to general theory of crime also differed for youth with mental disorders when compared to the general population. When considered independently from the other criminological theories (e.g., Table 2 model 3 and Figure 3), the current study’s findings seem to confirm these hypotheses, specifically showing that self-control did exhibit both, significant direct and indirect influence on the relationship between mental disorders and violent victimization. Once L/RAT factors were incorporated into analyses, however, self-control no longer showed significant direct or indirect associations to the relationship between mental disorders and violent victimization. This is quite surprising, differing from other work showing a direct (see Pratt et al., 2014 for meta-analysis) and indirect (Weisner & Shukla, 2018) link between self-control and violent victimization in the general population. This signifies that youth with mental disorders are unique, warranting additional exploration into why this subpopulation is at heightened risk for violent victimization.
Additionally, none of the factors drawn from social control theory (Hirschi, 1969) directly or indirectly influenced victimization for youth with mood or substance usage disorders. Given that social control theory has been found to impact victimization (Popp & Peguero, 2021) in the general population, it is striking that social control did not have an influence on violent victimization among youth with mental disorders. It is notable, though, that prior research has found that youths’ involvement in the justice system (Murray & Murray, 2010) and experience of a victimization event can hinder the formation of strong social ties (Cunningham, 2007). Because over 80% of youth with mood disorders or SUDs indicated that they had experienced victimization during the baseline wave, and the acknowledgement that elements of having a mental illness can negatively impact social relationships (e.g., Silver, 2002), it is likely that social ties to non-familial adults, parents, teachers, and school have been impacted. Nevertheless, for youth with mental disorders, connection to relationships or institutions did not influence violent victimization within this subsample, further highlighting how criminological theories may be limited in scope in explaining victimization depending on the type of subpopulation.
Third, mediating factors connected to the mental disorder-violent victimization relationship did not vary based on diagnostic type. What did differ based on disorder type, however, was the degree to which the indirect effects accounted for the relationship between disorder type and victimization. Specifically, mechanisms drawn from L/RAT and control perspectives indirectly accounted for over three quarters of the relationship between substance usage disorders and violent victimization, compared to half for mood disorders. Considering that the overall indirect influence of these mechanisms differed based on diagnostic type, future research should continue to investigate this topic through disaggregated measures of mental illness. Further, future research should examine a variety of mood disorders independently to understand if and how different diagnostic type relates to violent victimization. Given data constraints, the current study had to collapse together four mood disorders that, while share some commonalities, are distinct from one another and should be examined independently. This is especially evident when considering that the proposed mediators only accounted for about half of the relationship between mood disorders and violent victimization. It is highly probable that there are differing mechanisms between mediating factors, diagnostic type, and victimization. Doing so allows interventions to be designed to target mediating mechanisms associated with victimization that is specific to one’s disorder type. As a result, effective interventions are likely to occur, aligning with the responsivity principle (Andrews et al., 1990).
Collectively, findings from the current study have theoretical and policy implications. As argued by Decker (2015), a critical role of theory is to provide suggestions on future directions for interventions aimed at changing behaviors and outcomes of interest that are linked to people, groups, or institutions. To do so, however, empirical research is needed to determine the applicability of the theory to the subgroup and outcome of interest. As stated above, results suggest that factors drawn from L/RAT and control perspectives may be limited in understanding the mental illness-violent victimization link. Because of this, work understanding mechanisms that link violent victimization to mental illness are important to conduct, as it is likely that youth with mental disorders have unique mediating mechanisms that may be connected to mental illness. It is also possible that traditional criminological theories could be limited in scope based on the type of population of interest. Stated differently, it is possible that the unique, and often strained (Silver & Teasdale, 2005), life circumstances experienced by special populations may not be accounted for in criminological theories. It is important to keep in mind, however, that it was not possible to test all components associated with each perspective in this study. Nevertheless, this study represents a first step in understanding how factors drawn from L/RAT and control perspectives extend to youth with mental disorders, and highlights that there are likely other mechanisms contributing to increased risk of violent victimization for this population that are not captured by these perspectives. Given this, it is crucial to explore how factors derived from other theoretical perspectives, which have previously been used to understand violent victimization among people with mental disorders, may be relevant in this context. Exploration into stressful life events (Felson, 1992) or learning theories (Akers, 1998), for example, may be one of many potential avenues future research could explore in understanding the link between mental disorder and violent victimization, a line of research the current study was unable to explore.
Finally, it cannot be stressed enough that identifying how these mechanisms intersect with mental health and violent victimization are important topics of research, as they can be malleable targets for change rather than (sometimes) stable factors associated with mental disorders. In this way, interventions can be designed to target situational factors like attachment to pro-social people, thereby potentially reducing engagement with delinquent peers whom may place this population among motivated offenders. One promising avenue practitioners could explore are attachment-based interventions, which have showed beneficial outcomes for adolescents with mental disorders (see Moretti et al., 2015). Collectively, these findings suggest that, while having a mental illness can heighten the risk of violent victimization, this risk can be attributed to, in part, how mental disorder indirectly intersects with variables drawn from theory.
Limitations and Future Research
Despite these novel findings, there are some limitations that should be addressed. First, the Pathways sample includes data on justice-involved, adjudicated youth with and without mental disorders and thereby may not generalize to other samples. Further, the sample primarily consists of non-White, males, further limiting generalizability. Future research should examine the potential differential effects based on biological sex on the relationship between mental illness, L/RAT, control perspectives, and victimization. Additionally, there was a low rate of endorsement on mood disorders, limiting the ability to parse out effects for specific mood disorder types. Future research should also examine differential effects based on diagnostic type and comorbidity relate to these topics. Further, although it would be preferable to measure mediators at a subsequent wave from the measures of mental illness, a large amount of missing data prevented from doing so. In an effort to establish temporal ordering, mediators were all bounded by the previous 6 months, while measures of mental health are lifetime measures. It is notable that Kessler et al. (2007) show that most lifetime estimates of mental disorders start by early/mid-teens, which would likely occur before the mediators. Nevertheless, caution should be taken in interpreting these findings. Finally, the measure of violent victimization encompasses differing degrees of severity of violence across waves 1 through 6, aligning with prior scholarship (Daigle & Harris, 2018). Given that victimization is a rare event, the victimization measures could not be disaggregated. Future research should explore how mental illness, L/RAT, and control perspectives relate to differing types of violent victimization.
Conclusion
Despite these limitations, this study examined how factors drawn from L/RAT, self-control, and social control perspectives impact the relationship between mental disorders and violent victimization. Results demonstrate that adolescents with mental disorders, like the general population, would benefit from targeting risk factors specific to proximity of motivated offenders. Findings also highlight the need for continued research in understanding why youth with mental disorders experience violent victimization at greater rates, as traditional criminological theories may be limited in scope to certain populations in understanding violent victimization.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.