
Abstract
The current study examines rates of victimization by sexual orientation disaggregated by sex (female = 7,972; male = 6,985) using the National Longitudinal Study of Adolescent to Adult Health data (wave IV). Results from design-adjusted logistic regression analyses indicate bisexual people, regardless of sex, are most at risk for forced sexual assault. While women, especially bisexual women, had higher rates of sexual victimization, differences in risk were larger for bisexual men versus straight men than for bisexual women versus straight women. Bisexual respondents were likely to engage in alcohol-related risky behaviors, lifestyle factors did not fully account for differences in victimization risk among bisexuals. Results highlight the need for awareness, prevention, and intervention policies, particularly with regard to bisexual identities.
Introduction
Sexual violence can have a devastating impact on victims, including psychological, physical, social, and academic problems (Baker et al., 2016; Banyard et al., 2017; Dworkin et al., 2017). Although varying across states, definitions of sexual victimization generally include a range of unwanted sexual contacts from sexual assault to rape, by force, threat, incapacitation, or coercion (National District Attorneys Association [NDAA], 2016). Historically, official measures and responses to this crime have applied a heterosexual and women-exclusive lens. For example, the FBI Uniform Crime Reports definition of rape did not allow for male victims until 2012 and the National Crime Victimization Survey (NCVS) did not inquire about sexual orientation until 2016.
This sexist and heteronormative approach fails to capture a great deal of sexual victimization and neglects important risk groups. Specifically, studies reveal higher rates of victimization among LGBTQ people, including men (Coulter et al., 2017; Ford & Soto-Marquez, 2016; Semprevivo, 2021). For example, results from the Youth Risk Behavior Surveillance System (YRBSS) found lesbian, gay, bisexual, and questioning students had more than twice the victimization rate of their heterosexual counterparts (Kann et al., 2018). Only a few studies have had sufficiently large samples to differentiate among sexual minority subgroups. Those that have, including the American, Canadian, and British national victimization surveys find rates are especially high among bisexuals (Bender & Lauritsen, 2021; Cotter, 2021; Mahoney et al., 2014), but few investigate possible moderators of this association.
To that end, the current study situates sexual victimization at the intersection of sexual orientation and sex. We identify how sexual victimization rates vary across bisexual men and women compared to their straight peers. Consistent with lifestyle/routine activities (Cohen & Felson, 1979; Hindelang et al., 1978) and target congruence (Finkelhor & Asdigian, 1996) theories, we explore possible explanations for these relationships by including risk factors commonly found in the victimization literature (e.g., substance use, multiple sex partners, feeling unloved; Bradley & Teasdale, 2022; Hayes et al., 2020; Ray et al., 2021; Turchik, 2012; Turchik & Hassija, 2014). Our approach explores the extent to which the impact of bisexuality on sexual victimization may vary by sex and if and how the bisexual experience varies by sex in relationship to risky lifestyles and the target vulnerability that may come with an emotionally harsh or abusive (e.g., feeling unloved) childhood.
Literature Review
Studies find lesbian, gay, bisexual, transgender, and queer or questioning (LGBTQ) individuals have higher rates of victimization than their counterparts (Bender & Lauritsen, 2021; Canan et al., 2019; Kann et al., 2018; Ray et al., 2021). For instance, rates of rape and sexual assault victimization were significantly higher among sexual minorities than heterosexuals according NCVS data (Bender & Lauritsen, 2021). Specifically, rates were substantially higher among lesbian and bisexual women compared to heterosexual women (3.8, 40.9, and 3.2, respectively) and rates among gay and bisexual men were significantly higher than those of heterosexual men (6.3, 7.5, and .3, respectively; Bender & Lauritsen, 2021, Table 2), with bisexuals having the highest rates among both men and women. College student samples also find higher rates of sexual victimization among sexual minorities than their non-sexual minority counterparts (Ford & Soto-Marquez, 2016; Semprevivo, 2021). For example, using data from the Online College Social Life Survey (N = 21,000) gay (24.3%) and bisexual (17.7%) men had rates of victimization similar to heterosexual women (24.7%), but bisexual women had the highest rate of victimization (37.8%; Ford & Soto-Marquez, 2016). Similar results were obtained using YRBSS data, where LGBQ females had the highest risk of victimization (odds 4.6), followed by LGBQ males and heterosexual females, who had the same risk (odds 2.6; Semprevivo, 2021).
Theoretical Frameworks
Criminologists have used lifestyle/routine activity theory (LRAT; Cohen & Felson, 1979; Hindelang et al., 1978) and target congruence theory (TC; Finkelhor & Asdigian, 1996) to examine lifestyle and target factors that help to explain the higher rates of victimization experienced by LGBTQ individuals (Elvey & McNeeley, 2019; Waldner et al., 2008; Zavala & Guadalupe-Diaz, 2019). LRAT (Cohen & Felson, 1979; Hindelang et al., 1978) posits criminal victimizations are more likely to occur when one’s lifestyle facilitates the convergence of three key elements: A motivated offender, a suitable target, and a lack of guardianship. Research generally shows LRAT is well suited to explain criminal victimizations (Davis et al., 2021; Elvey et al., 2018; Hayes et al., 2020; Outlaw, 2015), as factors that make a target more “suitable” including being intoxicated or having risky sex are associated with higher victimization rates (Turchik, 2012; Turchik & Hassija, 2014). However, others have argued this framework is limited when it comes to explaining interpersonal victimization where victims and perpetrators frequently know one another, affecting offender motivation (Finkelhor & Asdigian, 1996; Schwartz & Pitts, 1995). Finkelhor and Asdigian’s (1996) target congruency theory specifically incorporates the real or perceived characteristics that make a target “suitable” from the offenders’ perspective to include their vulnerability (i.e., easier to victimize), gratifiability (i.e., desired), and antagonism (i.e., hostility). Regarding sexual violence, offenders may consider LGBTQ people to be more “vulnerable” because they are marginalized and stigmatized by society (Goffman, 1963; Link & Phelan, 2001). Bisexuality has been referred to as an “invisible” minority, due to a lack of public awareness or support for bisexuals (Burleson, 2005). Offenders may also view LGBTQ people as more “gratifiable” targets because of stereotypes of promiscuity. Bisexuals, especially women, are perceived as more sexualized and promiscuous (Hequembourg & Brallier, 2009; Zivony & Lobel, 2014; Zivony & Saguy, 2018). Because of these stereotypes, offenders may erroneously assume that victims wanted to have sex, “led them on,” and were responsible for the outcome (Dyar et al., 2021). Alternatively, offenders may view LGBTQ individuals as more “antagonistic,” because they are sexual minorities and although public opinions have improved over the years, many people still disagree with, or disapprove of their sexual orientation (Adamczyk & Liao, 2019). Bisexuals may be especially at risk as research finds US adults have negative attitudes regarding bisexual men and women (Dodge et al., 2016) and that bi- and other non-monosexuals experience stigma from both heterosexual and gay/lesbian communities (Davis et al., 2021; Friedman et al., 2014). Anderson et al. (2016) use the term “bisexual burden” to describe ways individuals identifying as bisexual experience discrimination. Scholars argue that heteronormative emphasis on binary conceptualizations of sexuality foster discrimination and oppression against bisexual people (Duffin, 2016; Klesse, 2011). Thus, target congruence perspective would predict LGBTQ individuals would have higher rates of victimization than their straight counterparts.
LRAT (Cohen & Felson, 1979; Hindelang et al., 1978) suggests some behavioral routines put people in more frequent contact with potential offenders and if sufficient guardianship is not available, may differentially expose them to victimization. In the context of sexual violence, substance use can increase victimization risk by reducing self-guardianship. Likely due to the stress conferred by discrimination, research finds sexual minorities report higher rates of problematic alcohol use and dependency (Drabble et al., 2005; Qeadan et al., 2022), and that bisexual women in particular are more likely to use and misuse substances than their straight counterparts (Kerr et al., 2015). Similarly, risky sexual behavior can place an individual at greater risk of victimization through increased contact with potential offenders. Studies find youth who identify as LGBTQ report more risky sexual behavior (e.g., unprotected sex, multiple sex partners, drunk sex; Kann et al., 2016) and bisexual women report more lifetime sexual partners than their straight counterparts (Scheer et al., 2002).
Finally, experiencing emotional harshness, verbal/emotional abuse, or generally feeling unloved is another vulnerability included under the LRAT/TC framework. Research finds emotional abuse is one of the most prevalent forms of childhood victimization (Finkelhor et al., 2015) and LGBT youth experience higher rates than their straight counterparts (Baams, 2018; Gorczynski & Fasoli, 2022). Indeed, previous research finds that gender nonconformity is associated with greater parental abuse among both women and men (Friedman et al., 2006; Lehavot et al., 2012; Plöderl & Fartacek, 2009) with one study reporting that although lesbians and bisexual women did not differ in their rates of parental abuse, bisexual women had higher rates of adult sexual assault (Lehavot et al., 2012). There is a strong relationship between childhood adversities and several negative outcomes including risky sexual behavior, substance use, and sexual victimization (Norman et al., 2012; Ports et al., 2016). These outcomes may make individuals more vulnerable targets as offenders may find them easier to victimize. Thus, LRAT/TC not only suggest LGBTQ individuals may have higher rates of victimization, but also that lifestyle and vulnerabilities factors may help to explain the heightened risk of sexual violence victimization experienced by sexual minorities, especially bisexual women.
While not all previous literature is guided by these perspectives, research on sexual violence victimization is generally consistent with these frameworks. That is, sexual minorities have higher rates of victimization, and lifestyle and vulnerability factors, some of which may stem from their experience of stigmatization and trauma (Davis et al., 2021; Ports et al., 2016; Qeadan, 2022), including number of sex partners, drunk sex, substance use, and feeling unloved increased the risk of victimization (Bradley & Teasdale, 2022; Ford & Soto-Marques, 2016; Hayes et al., 2020; Lehavot et al., 2012; Ray et al., 2021) as illustrated below.
Correlates of Victimization
In additon to sexual minority status, substance use is associated with higher risk of sexual violence victimization among female and male college students regardless of whether it is operationalized as alcohol use problem, heavy drinking, or drug use (Turchik, 2012; Turchik & Hassija, 2014). Fewer studies have examined the influence of substances on victimization risk among LGBTQ individuals, but the association appears similar. For instance, Ray et al. (2021) examined forced, incapacitated, and coerced sexual victimization among 1,413 college students and found sexual minority females had the highest victimization rate, for both forced and incapacitated sexual victimization, while heterosexual males had significantly lower rates. Logistic regression revealed heavy drinking increased victimization risk for both heterosexuals and sexual minorities.
Studies with heterosexual women and men generally find risky sex (e.g., multiple sex partners or hook ups) is associated with increased risk of sexual victimization (Turchik, 2012; Turchik & Hassija, 2014). However, the limited research on the influence of risky sex among LGBTQ individuals (Ford & Soto-Marques, 2016; Ray et al., 2021) has produced mixed results. For instance, Ford and Soto-Marques (2016), found number of prior hookups with both strangers and acquaintances was associated with increased victmization risk among lesbian and bisexual women, and gay men, while number of sex partners was significantly associated with victimization for all four groups; lesbian and bisexual women and gay and bisexual men. In contrast, Ray et al. (2021) found risky sex was only significantly associated with victimization risk among heterosexuals, not sexual minorities. The lack of consensus among the limited research points to the need for additonal investigation into this relationship.
Conceptualized as a form of emotional harshness (Mendle et al., 2019) or childhood emotional abuse (Richards et al., 2017), feeling unloved or rejected by loved ones is associated with increased victimization risk (Cotter, 2021; Lehavot et al., 2012; Richards et al., 2017). A prospective study of college women found lack of attachment and loneliness predicted sexual victimization even after controlling for prior victimization (Fite, 2006). A study on bullying found a “vicious cycle” between being victimized, feeling unlovable, and subsequent victimization (Choi & Park, 2021). Feeling unloved was also a significant risk factor in a study examining recurring physical assault victimization. Bradley and Teasdale (2022) found that the indirect effects of feeling unloved provided some explanation for the greater rates of victimization experienced by same-sex attracted individuals. Combined these results suggest it is productive to examine the relationship between feeling unloved and sexual victimization to explore its possible role in the elevated risk of victimization found among sexual minorities.
Current Study
LRAT/TC frameworks provide some explanation for the disproportionate rates of sexual victimization experienced by sexual minorities. Specifically, the societal stigma, negative stereotypes, and discrimination experienced by sexual minorities, especially bisexuals (Davis et al., 2021; Dodge et al., 2016; Duffin, 2016; Kerr et al., 2015) may alter their routine behaviors and may make them more “vulnerable,” “gratifiable,” and “antagonistic” targets for offenders. Although not a specific test of LRAT/TC theories, these explanations provide some insight into the relationships we may expect between sex, sexual orientation, and victimization. Guided by these frameworks, we formulate the following research objectives. First, we investigate whether bisexual respondents had higher rates of victimization than their heterosexual counterparts. Second, we determine whether these results hold when controlling for other theoretically relevant correlates of victimization (e.g., substance abuse, multiple sex partners, drunk sex, and feeling unloved). Third, we explore whether the risk of victimization among bisexual individuals varies by sex.
This study extends prior literature by examining the risk of sexual victimization among bisexuals using wave IV of the National Longitudinal Study of Adolescent to Adult Health data. We explicitly model a cross-product interaction effect between sexual orientation and sex (male vs. female) to examine differences in the association between bisexuality and sexual assault by biological sex. That is, does being bisexual increase the risk for sexual assault equally for men and women?
Methodology
Data
This study uses data from The National Longitudinal Study of Adolescent to Adult Health (Add Health), which is a nationally representative sample of students who were in grades 7 to 12 in 1994 (Chen & Chantala, 2014). The respondents were reinterviewed 5 times after the initial interview. Wave IV interviews were completed in 2008 when the sample was between 24 and 34 years old. The sampling frame for Add Health has been described extensively (Bearman et al., 1997). In brief, schools that met inclusion criteria were stratified by region and then sampled proportional to size. Within each middle-high school pair, students were stratified by grade level and sex and students were randomly sampled within strata until a quota was reached. The data also include oversamples for special populations. Overall, 15,640 respondents provided valid responses to the sexual assault item (our dependent variable). Item level missingness on the independent variables reduced our sample to 14,867. Since this represents less than a 10% loss of data due to item level missingness, we used a listwise deletion to handle missing data. Because of the low level of missingness, it is unlikely that results are biased by missing data. The clustered and stratified nature of the sampling plan is accounted for in our analysis, described below. Our final sample includes 7,916 women and 6,951 men.
Variables
Dependent Variable
We used the physical sexual assault item provided by Add Health to assess sexual victimization, consistent with prior research (Bones, 2020; Lee et al., 2020). This item asks, “Have you ever been physically forced to have any type of sexual activity against your will?” Respondents were instructed to exclude experiences with a parent or caregiver, as this was covered in a section on childhood sexual abuse. Responses were coded 1 for yes (0 = no).
Sexual Orientation
We used one indicator of sexual orientation as in prior studies (Yun et al., 2022). Survey respondents were asked “Please choose the description that best fits how you think about yourself.” Response options ranged from “100% Heterosexual” through bisexual to “100% Homosexual.” We collapsed the middle categories into bisexual indicating that the respondent did not choose 100% heterosexual (coded straight) or 100% homosexual (coded gay).
Lifestyle
Consistent with the importance of risky lifestyles noted in the research reviewed above (Hayes et al., 2020; Ray et al., 2021), we include four variables reflecting risky lifestyles. With regard to sexual situations two dichotomous variables were used. Involvement in multiple simultaneous sexual relationships was determined based on a single item asking respondents “In the past 12 months, did you have sex with more than one partner around the same time?” Response options were coded 1 for yes and 0 for no. In addition, intoxicated sexual behavior was assessed based on responses to the question “The most recent time you had sex, had you been drinking/drunk?” Responses were dichotomous, with 1 = yes. Add Health measures several problematic behaviors by asking respondents “how many times has each of the following things ever happened?” Referring specifically to alcohol use, the survey question asks, “How often have you been under the influence of alcohol when you could have gotten yourself or others hurt, or put yourself or others at risk, including unprotected sex?” Respondents rarely reported this activity, therefore we recoded this item into a dichotomy, with never = 0 and any reported activity (once or more) = 1. Similarly, respondents’ drug use was rare and so was based on any reported use of cocaine, crystal meth, heroin, or another illegal drug during their lifetime. This variable was coded 1 indicating any reported drug use (0 = none).
Target Vulnerability
Consistent with previous research that finds emotionally harsh or verbally abusive parenting, and consequently feeling unloved is associated with victimization (Bradley & Teasdale, 2022; Fite, 2006; Lehavot et al., 2012; Richards et al., 2017), we used the single item indicator feeling unloved, which asked “Before your 18th birthday, how often did a parent or other adult caregiver say things that really hurt your feelings or made you feel like you were not wanted or loved?” Response options ranged from “this has never happened” (0) to “more than 10 times” (5).
Control Variables
We included controls for age and race/ethnicity as well. We measure age in years. Race/ethnicity is measured as a series of dummy variables, including Black or African American, Latino/a, or other versus White (the excluded reference category).
Statistical Analyses
First, to investigate whether bisexuals are at an increased risk of sexual victimization, crosstabulations on sexual victimization status, by sexual orientation, layered by sex were computed and chi-squared tests were completed. Next, to determine whether greater risk of victimization can be explained by “risky lifestyle” and “target vulnerability” variables we used one-way analysis of variance with follow-up post hoc Tukey’s HSD test to compare means across the three sexual orientations. Finally, to examine whether the effect of sexual minority status on victimization was moderated by sex (male/female), we estimate a design adjusted logistic regression model in Stata with a cross-product term (sexual minority status by sex). The latter analysis accounts for the complex nature of the Add Health sampling plan, using the svyset commands in Stata. These analyses estimate sandwich standard error estimators to take into account the clustering of the individuals within study schools (based on the original sampling design), the stratification of schools by region and also the weights for oversampling.
Results
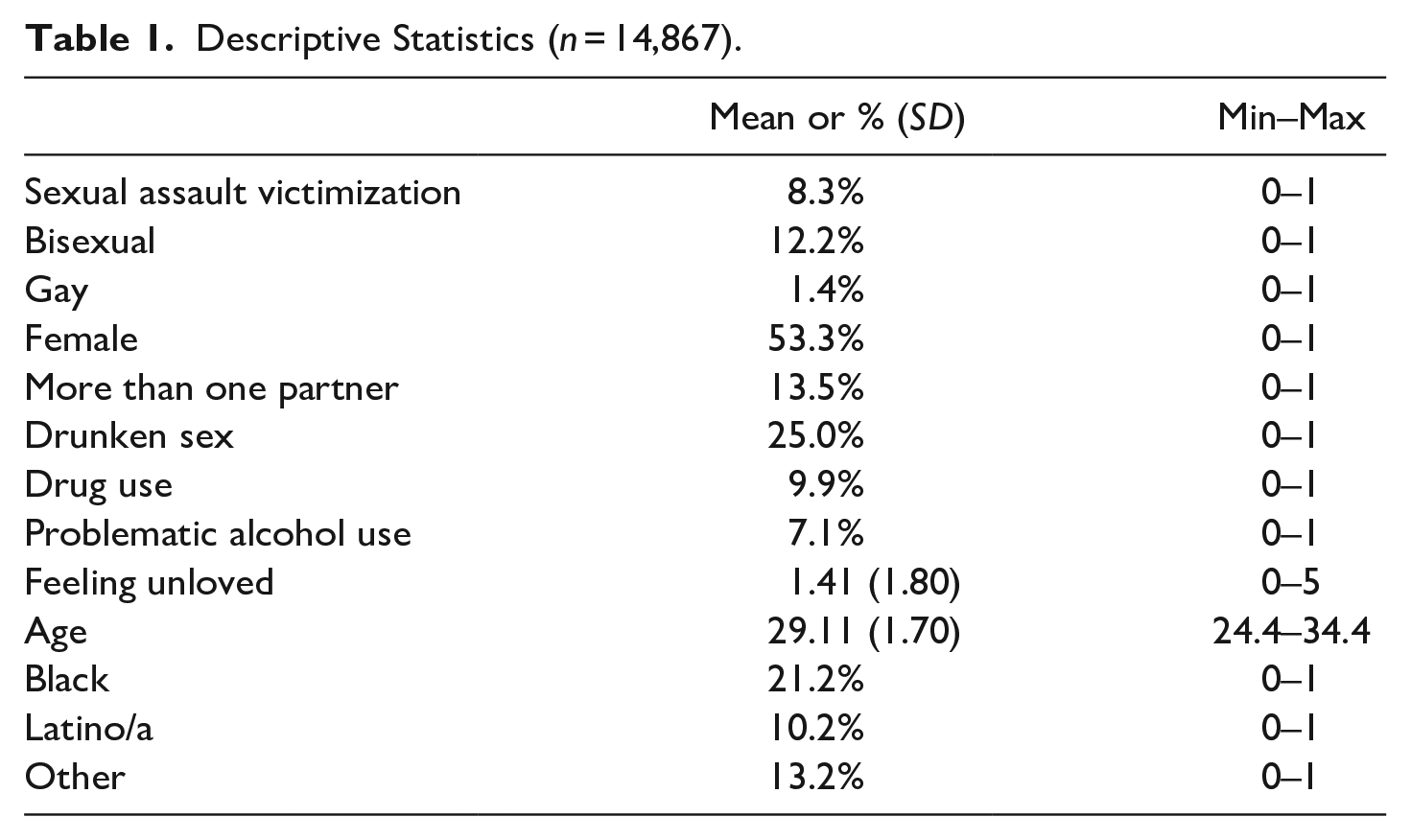
As shown in Table 1, 12.2% of respondents reported being bisexual and 1.4% reported being gay, with the remaining 86.4% identified as straight. Regarding sexual victimization, 8.3% of the sample indicated they had been physically forced to engage in sexual activity. Thus, our sample includes 1,228 victims reporting physical sexual assault. Approximately 13.5% of respondents indicated they had multiple sexual partners at about the same time. Twenty-five percent of respondents had engaged in sexual activities while drunk and about 7% of respondents reported problematic use of alcohol.
Descriptive Statistics (n = 14,867).
A cross-tabulation of sexual assault victimization by sex and sexual orientation is presented in Table 2. Not surprisingly, the distribution of sexual assault is uneven. Approximately 14% of women reported physical sexual victimization, compared with just under 2% of men. Larger prevalence of sexual victimization is found among women across all categories of sexual orientation. Bisexual women reported the highest rates of sexual victimization (23%), followed by lesbians (17.3%) and straight women (11.7%). Bisexual women have almost double the risk of straight women of being sexually assaulted. Similarly, although sexual victimization rates among men generally appears low (less than 2%), that risk appears particularly borne by bisexual men. Paralleling the results for women, bisexual men (8.1%) are at an increased risk for sexual assault compared to both gay men (3.2%) and straight men (1.6%). Compared with straight men, bisexual men have 5 times the risk of being sexually assaulted.
Crosstabulation of Sexual Assault Victimization by Sexual Orientation Layered by Sex. a .
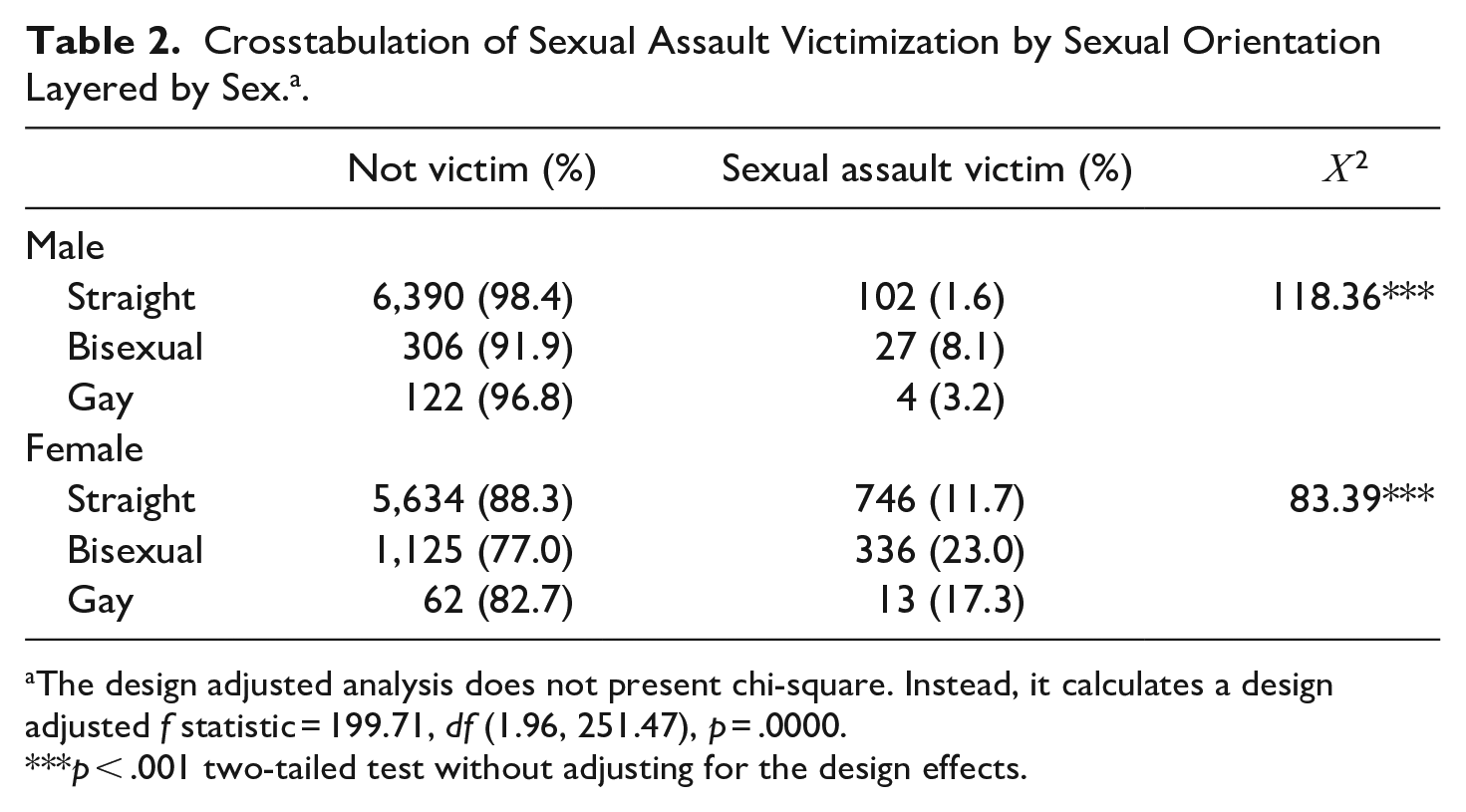
The design adjusted analysis does not present chi-square. Instead, it calculates a design adjusted f statistic = 199.71, df (1.96, 251.47), p = .0000.
p < .001 two-tailed test without adjusting for the design effects.
Our analyses next explore potential risk factors for victimization. Table 3 presents the mean level of these variables for each group of respondents based on sexual orientation. As shown in Table 3, bisexual (21%) and gay (28%) individuals are significantly more likely than straight respondents (12%) to report having multiple partners. Drug use was also more common among bisexual and gay respondents (19% and 18% respectively vs. 9% for straight respondents), as was feeling unloved with both groups reporting higher mean levels (means = 1.74 and 1.81, respectively) when compared to straight peers (mean = 1.29). Interestingly, bisexual individuals are the most likely to report having sex while drunk (35%), compared to 24% for gay respondents and 24% for straight respondents. Thus, bisexuals are disproportionately more likely than both heterosexual and gay/lesbian respondents to engage in alcohol-related behaviors that place them at risk for sexual victimization.
Mean Comparison of Lifestyles/Target Vulnerability Variables Across Sexual Orientation.
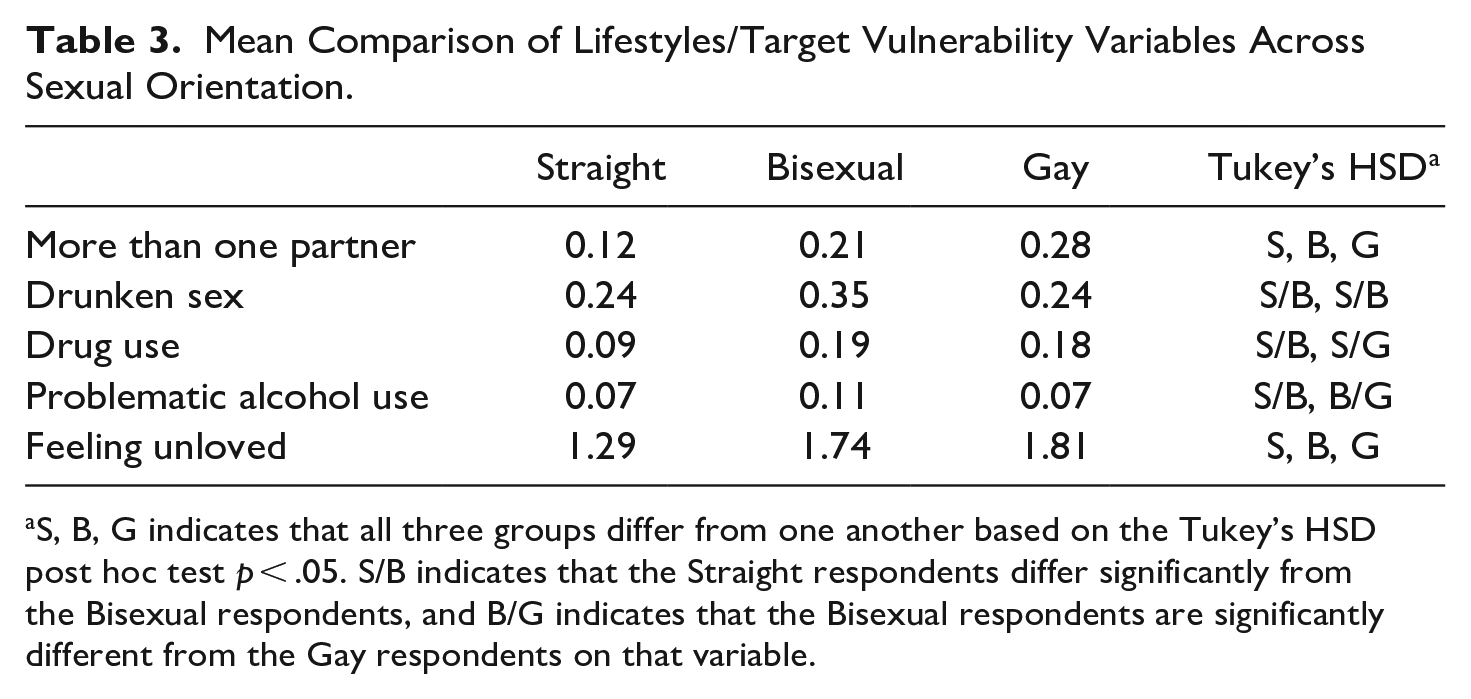
S, B, G indicates that all three groups differ from one another based on the Tukey’s HSD post hoc test p < .05. S/B indicates that the Straight respondents differ significantly from the Bisexual respondents, and B/G indicates that the Bisexual respondents are significantly different from the Gay respondents on that variable.
To examine whether the effect of sexual minority status on victimization varied by sex (male/female), we estimate a design adjusted logistic regression model. First, to determine whether the addition of the interactive terms significantly improved model fit we computed the main effects model (not shown) and compared it to the interactive model. Results from deviance test (i.e., difference in the −2logliklihoods between the two models) was significant (deviance = 17.44, df = 2, p = .0001) indicating the interactive model provides a significantly better fit and is therefore presented in Table 4. Based on this analysis, we find that having more than one partner, engaging in sex while drunk, and drug use all significantly increase the odds of sexual assault victimization. Results also suggest that feeling unloved multiplies the odds of a sexual assault victimization by nearly 1.3 times. As shown in Table 4, the risk for sexual assault is greatest for bisexual individuals compared with those who identify as straight. This risk is substantial, almost 4 times the odds of being sexually assaulted for bisexual individuals, holding all else constant. Women are also at a substantially and significantly higher risk of sexual assault than are men, experiencing 9 times the odds of sexual assault than men, net of other variables. Finally, the risk of sexual assault amongst bisexual individuals varies by sex. We find a significant interaction between identifying as bisexual and sex. The negative interaction term indicates that although bisexual individuals of both sexes are more at risk (the main effect of bisexuality) and women are more at risk than men (the main effect of sex), the increase in risk associated with being bisexual is smaller for women than for men. That is, whereas there is a doubling of the risk of being victimized for bisexual women compared to straight women, there is a near quintupling of the risk for being a bisexual man compared to a straight man.
Logistic Regression Predicting Sexual Assault Victimization (n = 14,867).
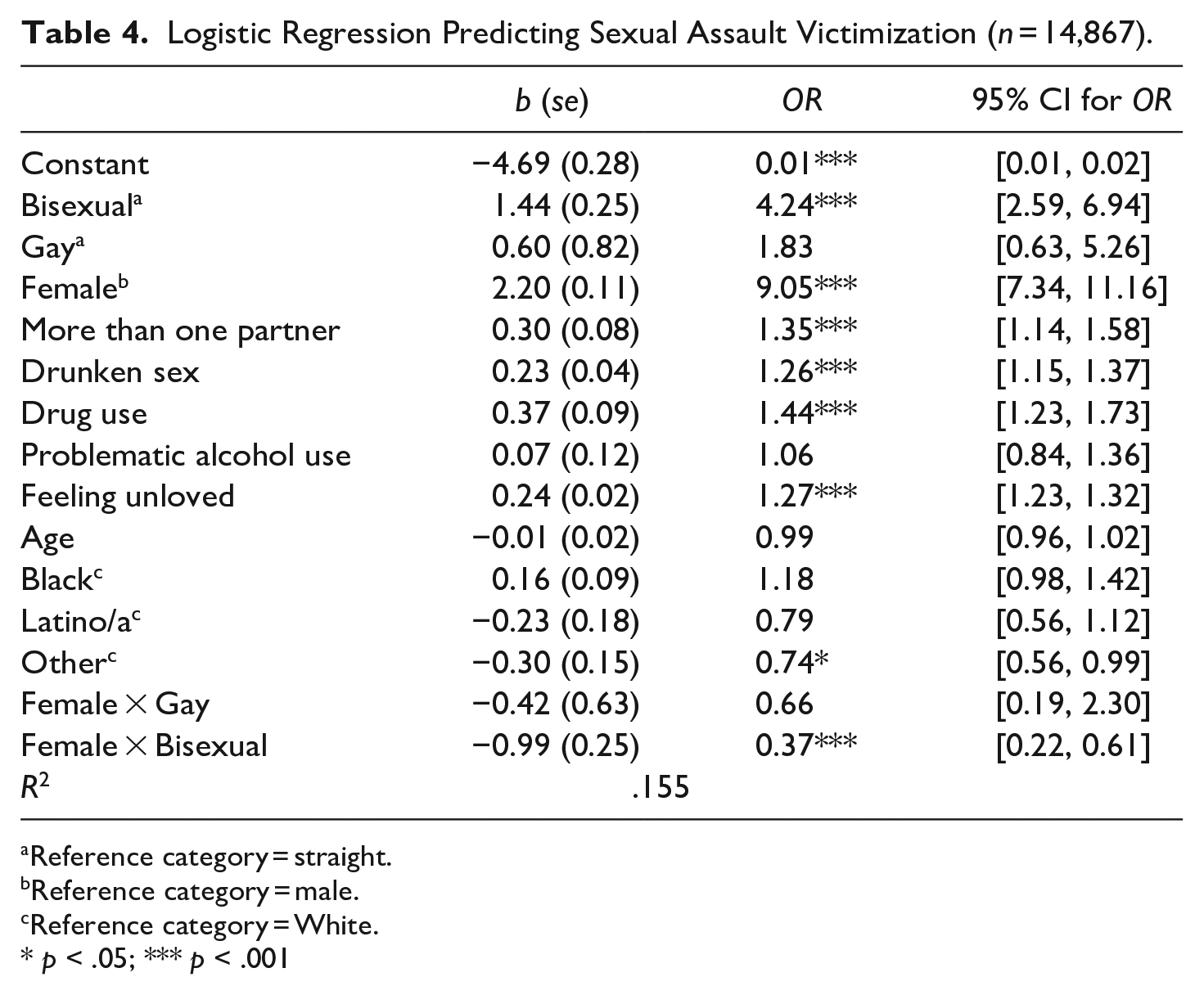
Reference category = straight.
Reference category = male.
Reference category = White.
p < .05; *** p < .001
Figure 1 helps to visualize the interaction between sex and sexual orientation, showing the percent who experienced sexual assault by sexual orientation across sex. As shown in Figure 1, women experience more sexual assault victimization across all sexual orientation categories. Moreover, bisexual individuals experience more sexual assault victimizations than any other sexual orientation regardless of sex. These indicate the main effects. If we compare the relative height of the bars within a sexual orientation category, we can see that the bars show substantial differences between male and female respondents in both the gay and the heterosexual groups, but the bars appear to be closer together in the bisexual group. This indicates the interaction effect between sex and bisexuality.
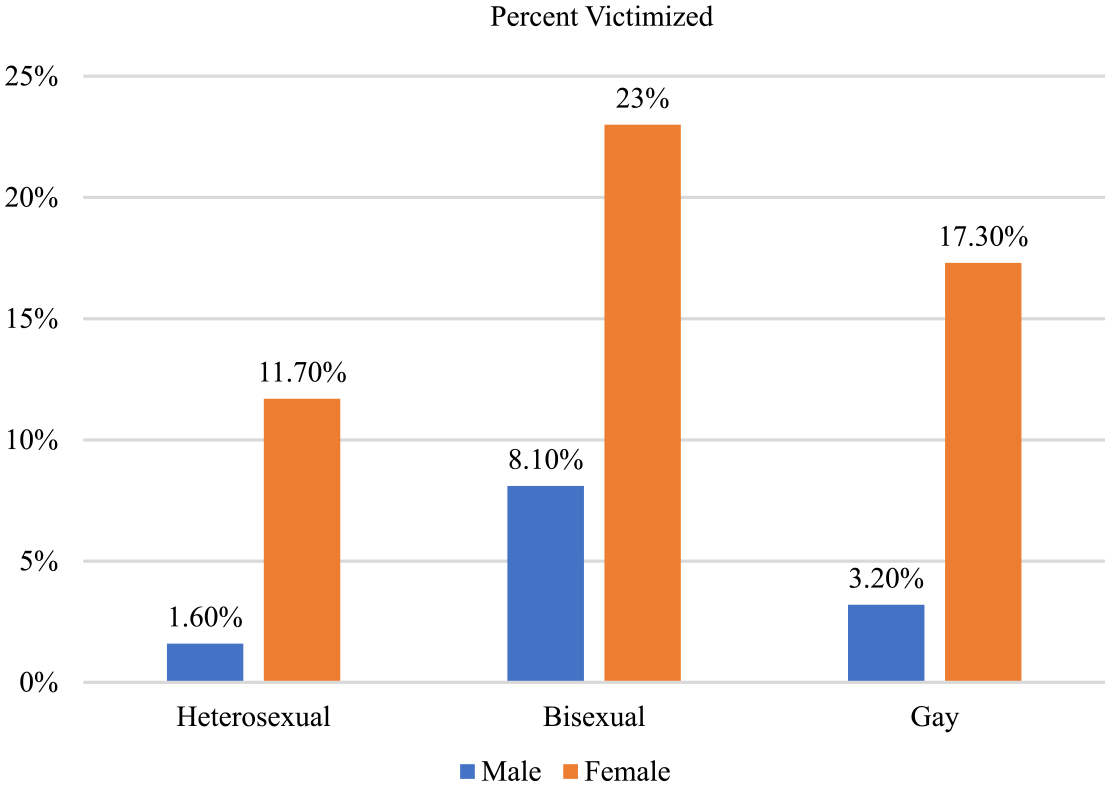
Probability of sexual assault victimization by sex and sexuality.
Discussion
This study reveals the relationship between sexual orientation and sexual assault victimization varies by sex. We demonstrate some of the many ways in which the identity of being a man/woman and gay/straight/bisexual represents both shared and distinct experiences. While there are clear differences in sexual victimization risk across sex, the degree of these differences depended substantially on one’s sexual orientation. Conversely, the impact of sexual orientation on victimization risk depended substantially on one’s sex. Thus, our results are consistent with prior findings that sex conditioned the risk of sexual violence, with women who identified as sexual minorities having the highest odds of sexual violence victimization, followed by sexual minority men and heterosexual women (Bender & Lauritsen, 2021; Ford & Soto-Marquez, 2016; Semprevivo, 2021). These findings suggest both sexism and sexual orientation discrimination play a role in sexual victimization risk, and bisexual women’s dual identities may make them especially vulnerable. Sexual objectification of women (Vasquez et al., 2018) and stigma, discrimination, and a lack of public support for bisexuals (Burleson, 2005; Dodge et al., 2016), combined with the heightened sexualization of brought about by stereotypes of promiscuity (Zivony & Saguy, 2018) may make bisexual women more attractive targets to motivated offenders when compared to their sexual minority counterparts.
Differences in sexual victimization across subgroups persisted, even with several theoretically relevant correlates of victimization taken into account. To be clear, women are most certainly at the highest risk across all sexual orientations. We note that bisexual women are the most highly victimized group in our sample. But our results uncover important differences in relative risks. That is, being bisexual indicates greater risks for men than it does for women, relative to their respective straight counterparts. These patterns hold despite controls for risk taking behaviors and the feelings of being unloved that stem from emotionally abusive or harsh parenting.
One explanation for this might lie in sex differences in exposure to sexual situations with potential perpetrators. Straight men, who are typically involved in sexual situations involving women, have very low rates of victimization. Whereas by definition, bisexual men are likely to have more sexual contact with men, than straight men. Given statistics indicate 96.6% of sex offenders are men (Federal Bureau of Investigation [FBI], 2021, Table 42), this difference in exposure to men, regardless of sexual orientation, may provide some explanation for higher relative odds of victimization among bisexual men.
Our study suggests the circumstances associated with sexual victimization may differ substantially across situated identities. Prevalence of specific risk behaviors varied across sexual orientation, with distinct differences between bisexual and gay/lesbian respondents. Rate of alcohol-related behaviors varied substantially across groups and appear particularly problematic among the bisexual population. Notably, victimization risk remained considerably high among bisexuals, even after taking this and other risk behaviors into account. Research finds rates of substance use are high among young adults who identify as gender or sexual minority (Allen & Mowbray, 2016), especially bisexual women (Kerr et al., 2015), and that discrimination increases the risk of substance use (Qeadan et al., 2022).
Our findings suggest that particular theoretical approaches and concepts may be more or less salient for explaining each subgroups sexual violence experiences. Further, although not directly tested, LRAT/TC may help explain why sexual minorities are at increased risk of sexual victimization relative to their heterosexual counterparts. Research finds higher rates of multiple forms of victimization among LGBTQ individuals (Bender & Lauritsen, 2021), which may be a form of homophobia/hate crime (Herek, 2009). Sexual minorities may be targeted specifically because of their minority status either as a result of the offender’s prejudice against minority individuals and/or belief that they will be “easier,” more vulnerable targets. Relatedly, sexual assault among sexual minorities may involve instances of “corrective rape” (Doan-Minh, 2019). Although this term was originally defined as straight men’s sexual assault of lesbians, it has been more broadly applied to suggests some straight male perpetrators sexually victimize sexual minorities in order to “cure” their homosexuality or bisexuality and/or as punishment for violating traditional gender presentation.
This is also consistent with research findings that masculinity is often narrowly defined, such that men having sexual contact with other men is viewed as “feminine” (Duffin, 2016). Increased exposure to male sexual partners may represent instances of gender identity threat to male perpetrators wrestling with the stigma of non-heterosexuality. Studies find that men who have sex with other men will often feel compelled to defend their identity as straight and degrade and demean “femininity” among men and frame “gay” behavior as anti-masculine (Duffin, 2016). This is consistent with the larger cultural devaluation of femininity (Connell, 1995; Pascoe, 2007). Whether these ideas and theoretical framework apply uniformly across gay, lesbian, bisexual, and other sexual orientation subgroups remains unknown. Future research should explore the extent to which these and other explanations may apply differentially across sexual minority subgroups and a theoretical framework focused specifically on LGBTQ stigma (e.g., Worthen, 2020) may be especially well suited for this task.
Policy Implications
Results conform to prior research and theory that being a sexual minority may incur many negative effects, including greater risk of sexual victimization. These findings underscore the need for educational and awareness programing to reduce the stigma experienced by LGBTQ individuals, especially those who identify as bisexual. Interventions including education, contact with LGBTQ communities, and inducing tolerant social norms were found to reduce sexual prejudice in one meta-analysis (Bartoş et al., 2014). Internalized homophobia also needs to be addressed and one online intervention designed to reduce internalized binegativity has shown some promise (Israel et al., 2019). Together, these studies point to the need to expand the use of evidence-based interventions to reduce bias. The reduction of bias among society more generally would likely also impact those who sexually offend as research finds many rapists are living in the community undetected (Foubert et al., 2020; Lisak & Miller, 2002). Further, although bisexual women had the highest rate of victimization, bisexual men’s relative odds of victimization were higher than their straight counterparts, suggesting they should not be forgotten in prevention, outreach, and treatment efforts. Research finds people are less sympathetic to male victims (Allen et al., 2015), are less likely to help men, especially those perceived to be gay (Katz et al., 2015), and that even rape crisis centers are less equipped to provide services to men (Donnelly & Kenyon, 1996).
There is also a need to overcome barriers to help seeking found among LGBTQ individuals, who may feel less supported by friends and family (D’Augelli et al., 2005; Thoma et al., 2021), underserved by police (Kuehnle & Sullivan, 2001), and consequently are less likely to report or disclose their victimization to anyone (Duke & Davidson, 2009; Felix et al., 2021). In particular, research finds bisexual individuals are less attached to LGBTQ communities than their lesbian and gay counterparts (Frost & Meyer, 2012) and may be stigmatized by both the heterosexual and the gay/lesbian communities (Davis et al., 2021; Friedman et al., 2014). Among bisexuals, stigma, “invisibility,” and lack of belonging to the straight and LGBTQ communities poses serious consequences for both their risk and responses to victimization. Thereby demonstrating the need for strong outreach for those who identify as bisexual, including online resources that may be more accessible than their immediate social networks. The development of LGBTQ resource centers that provide individuals with a safe environment, where they have legitimacy and advocacy can be critical, particularly if they are sensitive to the unique needs of bisexuals (Pitcher et al., 2018; Self & Hudson, 2015).
Treatment also needs to be inclusive and affirming for LGBTQ people. Currently, treatment programs often fail to take LGBTQ identity into consideration. One review of intimate partner violence programs found none catered to LGBTQ populations (Subirana-Malaret et al., 2019). Research finds mental health professionals also lack knowledge regarding the social obstacles and stigma bisexuals face (Barker, 2007). The high prevalence of problematic alcohol-related behaviors among bisexuals is worrisome and highlights the need for the development and expansion of programs to address their unique needs (Schulz et al., 2021). Clinicians should be trained to provide bisexual-affirmative care and to teach bisexual clients healthy, empirically supported ways to cope with stigma to reduce substance misuse (Feinstein et al., 2019). In sum, we echo Love et al.’s (2017) recommendations that sexual assault help agencies need to produce more inclusive advertising and to provide more LGBTQ-led services with more welcoming environments. Finally, additional resources need to be allocated toward treatment, especially given the prevalence and financial burden of sexual violence exceeds that of other public health problems (e.g., cancer, cardiac disease), yet receives far less funding (Waechter & Ma, 2015).
Limitations
As in most research, there are limitations that present opportunities for future investigations. Although the study was theoretically-informed and the results are not inconsistent with prior research (Ray et al., 2021; Semprevivo, 2021), we are nonetheless analyzing cross-sectional data and thus limited in our ability to draw direct causal inferences. A benefit of the large, nationally-representative secondary dataset is its sufficient subsample sizes enabled lesbian, gay, and bisexual statistical comparisons. But the use of secondary data hinders our ability to identify and measure all aspects of identity (i.e., sexual and gender), victimization, and potential moderators. Perhaps the study’s most important limitation is our single-item measurement approach, and consequently our inability to capture other forms of sexual victimization in addition to physically coerced sexual behavior. Indeed, there are many ways in which a person can be sexually victimized that do not included actual physical force (such as through threat of force, verbal, emotional, or financial abuse or manipulation). Our outcome also misses attempted sexual assaults and did not include sexual abuse by caregivers. Similarly, the use of a single item to measure sexual orientation may not be ideal, but concerns about this construct apply mostly to the first, rather than the fourth wave of Add Health data (Savin-Williams & Joyner, 2014), which was used here. That is, we capture identity, not attraction or behavior. While the three concepts may be correlated, they are not synonymous and should not be construed as such. Individuals who identify as bisexual may have sexual relationships with only men, only women, or both. The identity is not indicative of behavior. We leave it to future research to unpack the role of partners’ sex and gender identities in the experience of sexual assault victimization. The use of one item “feeling unloved,” to represent target vulnerability may be restrictive as this construct has been measured in a variety of ways (e.g., poor mental health, physical disability; Elvey et al., 2018; Reyns & Scherer, 2018). However, prior research shows that even this narrow conception of vulnerability can be informative (Bradley & Teasdale, 2022; Choi & Park, 2021; Cotter, 2021). Still, more information about the context of the victimization, most notably the offender’s actual motivations would have been helpful. The updated motivation-facilitation model of sex offending, which was influenced by target congruency theory, may be helpful in capturing offenders’ motivations, and informing future research, assessment, and intervention (Seto, 2019).
A three-way interaction of sex-race/ethnicity-sexual orientation would have no doubt been even more informative, but early investigations quickly revealed the current data lacked adequate subsamples in this regard. Future research should also include the interacting effects of race/ethnicity with other marginalized identities on sexual assault victimization risk, as studies find having multiple marginalized identities increases risk for sexual assault victimization (Coulter et al., 2017). Yet, research finds African American women, for example, are least likely to disclose or seek help following their assault (Tillman et al., 2010) and face substantial barriers to service utilization (Ullman & Lorenz, 2020). Research on discrimination against LGBTQ people and bisexuals in Black communities and the “Down Low” culture (Duffin, 2016) begs questions regarding how anti-LGBTQ attitudes may relate to intimate partner and sexual violence against and among African American men. Thus, studies should oversample for individuals who identify as race or ethnic minorities as they may face unique forms of oppression and be especially in need of resources.
Nevertheless, our study provides compelling evidence that there is a clear need for data collection efforts and research exploring violence among and against bisexuals. Identifying the extent to which factors such as lack of support from family, friends, and other community members (D’Augelli et al., 2005; Duke & Davidson, 2009; Felix et al., 2021; Thoma et al., 2021), may place these individuals at risk is essential for developing effective prevention and intervention strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Add Health is directed by Robert A. Hummer and funded by the National Institute on Aging cooperative agreements U01 AG071448 (Hummer) and U01AG071450 (Aiello and Hummer) at the University of North Carolina at Chapel Hill. Waves I-V data are from the Add Health Program Project, grant P01 HD31921 (Harris) from Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), with cooperative funding from 23 other federal agencies and foundations. Add Health was designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill.