
Abstract
In this study, we investigated the potential moderating role of instability in living arrangements in the association between 14 clinical factors of the Historical Clinical Future Revised (HKT-R) and 5-year violent recidivism. The sample included 316 male forensic psychiatric patients who were unconditionally released from Dutch forensic psychiatric institutions between 2004 and 2008. Results showed that instability in living arrangements did not moderate the association between the clinical factors and violent recidivism, however, it directly and positively predicted (OR = 3.28) violent recidivism. Likewise, hostility (OR = 4.36) and addiction (OR = 1.65) were directly and positively related to violent recidivism, while psychotic symptoms (OR = 0.25) were inversely related.
Keywords
It has been found that 19 to 23% of forensic psychiatric patients violently recidivate within 2 years after termination of a TBS measure (ter beschikkingstelling: involuntary admission by order of the state; De Ruiter & Trestman, 2007; Drieschner et al., 2018). Violent recidivism causes a lot of damage and can lead to higher costs of criminal prosecution (Nagtegaal et al., 2016). Homelessness is an important criminogenic factor associated with offending behavior (Mccarthy & Hagan, 1991). Among young people (16–19 years old), McCarthy and Hagan (1991) found a significant association between the number of crimes committed and being homeless. Crimes occurred more often in the group of participants with difficulties in living arrangements compared to participants with stable living arrangements, while there was no effect of age, gender, or earlier homeless experiences. Homelessness is a growing problem and can negatively affect physical-, emotional-, and social health ultimately leading to criminal behavior (Shaw, 2004; Victor, 1997). Compared to 2009, the number of homeless people has increased from approximately 17.8 thousand to 36 thousand homeless citizens in 2020. Eighty-four percent were male and 60% had a migration background (Centraal Bureau Statistiek, 2021).
The link between homelessness and crime can be substantiated by the Good Lives Model (GLM). The GLM is a positive psychological approach to offender treatment and rehabilitation (Barnao et al., 2016; Ward et al., 2007). According to this model, humans are goal-directed organisms seeking primary goods such as healthy living and functioning, knowledge, excellence in play and work, agency, happiness, and spirituality. People need secondary goods, like music or a car, to obtain these primary goods (Ward et al., 2007). Criminal behavior, as inappropriate behavior, arises from a discrepancy between the available pro-social resources and the resources needed to satisfy these goods (Ward & Stewart, 2003). Proper housing is such a secondary good (Barnao et al., 2016; Shaw, 2004); it is a place of consistency and control to build a social network and establish an identity of personal worth (Shaw, 2004). This corresponds to primary goods such as agency, friendship, and community. Homelessness prevents people from building successful careers and compromises their ability to participate in social, life, community, and friendship domains (Barnao et al., 2016; Gaetz, 2004). Social exclusion and vulnerability can lead people to use illegal strategies like theft and drug dealing and consequently come into contact with other criminals (Gaetz, 2004).
Homelessness in Relation to Recidivism
The positive association between homelessness and crime as well as reoffending has been well established in previous research (e.g., Jacobs & Gottlieb, 2020; Makarios et al., 2010). Jacobs and Gottlieb (2020) examined the relationship between living arrangements and recidivism in a longitudinal study with a sample of 2,453 participants on probation. The results showed that 56% of the participants experienced one or more residential changes within the observation period and 11% experienced more than two residential changes. About 40% of these residential changes resulted in homelessness and 25% of the participants were homeless for at least 6 months during observation. Homelessness increased the likelihood of recidivism by 50% and each residential change increased the recidivism odds by 12%. The effect was even stronger for participants who committed minor crimes (Jacobs & Gottlieb, 2020). In a study by Makarios et al. (2010) matching results were found. Multiple changes of residence increased recidivism odds by 70% in comparison to participants who had stability in their living arrangements.
Various studies investigated the effect of housing interventions on reducing recidivism in violent crime. They found indications of a positive effect on reducing recidivism in violent crime (Clark, 2016; Cohen, 2020; Listwan et al., 2018; Lutze et al., 2014). Direct transfers to private residential addresses after release from prison resulted in revocation rates of 25% compared to 45% of participants released in emergency shelters (Clark, 2016). Lutze et al. (2014) examined the effect of the Reentry Housing Pilot Program (RHPP) in Washington State. The RHPP was intended for high-need inmates who were released from prison without a place to live. Inmates who were willing to accept treatment and work on self-reliance were offered housing support for 12 months (Lutze et al., 2014). The RHPP was successful in reducing new convictions. Twenty-two percent of the participating inmates had a new conviction, while 36% of the control group were convicted of a new crime. The proportion of prison readmissions was significantly lower in the RHPP group compared to the control group (37 vs. 56%, respectively). Other studies also showed that stability in living arrangements reduced the probability of committing a crime, reduced the number of days in prison (Cohen, 2020), and resulted in fewer arrests (Listwan et al., 2018). Not all studies indicate a significant relationship between stability in living arrangements and reducing recidivism (Broner et al., 2009; Loong et al., 2021). For example, Broner et al. (2009) and Loong et al. (2021) found no significant relationship between homelessness and recidivism. Results further indicated that instability in living arrangements negatively affected the quality of life for both homeless and non-homeless individuals. It was claimed that not homelessness, but failure in treatment, the severity, the type, and the time of the offense predicted recidivism (Broner et al., 2009). Therefore, more research is needed to clarify whether and in what way homelessness can influence recidivism.
Homelessness, Clinical Risk and Protective Factors, and Recidivism
In addition to a direct link between instability in living arrangements and recidivism (Jacobs & Gottlieb, 2020; Makarios et al., 2010), there are some indications that homelessness may influence the association between clinical risk and protective factors for reoffending and recidivism into a new crime (Broner et al., 2009). Clinical risk and protective factors are changeable characteristics of individuals and their environments that are expected to increase (risk factors) or decrease (protective factors) the likelihood of reoffending (Andrews & Bonta, 2010; Bonta et al., 2007). Within the Risk-Need-Responsivity (RNR) model, Andrews and Bonta (2010) identified eight central risk factors for predicting recidivism that can also be considered important treatment goals in offender rehabilitation. They are antisocial personality patterns, pro-criminal attitudes, history of crime, social support for crime, substance abuse, family relationships, school/work, and prosocial activities. A frequently used instrument in the Netherlands for the assessment of these clinical risk factors in forensic psychiatric patients is the Historical Clinical Future-Revised (HKT-R) (Spreen et al., 2014). This study will focus on the 14 clinical HKT-R factors, which can be broadly categorized into seven risk and seven protective factors (Bogaerts et al., 2020; Table 1).
Historical Clinical Future–Revised (HKT-R) Clinical Domain: Risk and Protective Factors.
Research has been done on the relationship between specific clinical factors and recidivism which are specific to the homeless population. The available evidence suggests that homelessness can result in the withdrawal of people from their family and their community (Gaetz, 2004) and involvement in an antisocial network (Toohey et al., 2004) and antisocial behavior (Heerde et al., 2022). Subsequently, this social exclusion can prevent them from finding work and provide them with proper living arrangements. Due to the inability to secure themselves with necessities, they may take the risk and turn to theft and robbery (Gaetz, 2004). Poor relationships with family and friends, lack of employment (Lee et al., 2010), and an antisocial social network (Lee et al., 2010; Shaw, 2004) have all been identified as predictors of recidivism among released offenders and especially among the homeless.
Social exclusion and lack of support for homeless people can result in substance abuse as a coping mechanism (Watson et al., 2016). Substance abuse is an established factor for recidivism among juvenile and adult offenders (Guebert & Olver, 2014; Thompson et al., 2013). Kesten et al., (2012) found that comorbidity of mental illness and substance abuse are important characteristics of rearrest and reincarceration. Substance abuse can perpetuate homelessness and social exclusion (Toohey et al., 2004) and alcohol abuse was associated with higher chances of recidivism and multiple episodes of homelessness (Jones et al., 2021; Tsai & Rosenheck, 2012). In addition, substance abuse is also one of the major risk factors for developing psychotic disorders, along with a lack of health care and loss of contact with parents (Lamberti, 2007; Odell & Commander, 2000). Taken together, instability in living arrangements may influence the link between certain clinical risk and protective factors for recidivism. However, to our knowledge, no previous studies have investigated this.
The Present Study
The goal of this study was to investigate whether instability in living arrangements influences the association between 14 clinical factors of the HKT-R (Table 1) and violent recidivism within 5 years after discharge from a forensic psychiatric center. These 14 clinical factors are all separately investigated in relation to the recidivism of individuals who have been homeless in the past. To investigate the moderating effect of instability in living arrangements, the housing situation was categorized into three levels: 1) no or very rare problems with living arrangements, 2) occasional problems with living arrangements and homelessness, and 3) chronic difficulties in living arrangements and homelessness.
In general, difficulties in living arrangements were expected to strengthen the positive link between risk factors and violent recidivism, and weaken the negative link between protective factors and violent recidivism. In other words, the effect would be strongest for the third group, less strong for the second group and least strong for the first group. Specifically, based on previous research, we hypothesized that difficulty in living arrangements would significantly moderate the positive associations of addiction, antisocial behavior, psychotic symptoms, and high-risk network members with violent recidivism in a way that the effect would be strongest in the group with the most severe problems in living arrangements. Due to the lack of evidence, we did not formulate specific hypotheses about the remaining four risk factors investigated (hostility, impulsivity, and violation of terms and agreements). Additionally, we hypothesized that the difficulty in living arrangements would significantly moderate the negative associations of labor skills with violent recidivism, so that the effect would again be strongest in the group with the most severe problems in living arrangements. Due to the lack of evidence, no specific hypotheses were formulated about the remaining six risk factors (self-reliance, coping skills, cooperation with treatment, social skills, problem insight, and responsibility for the offense), however, they would also be investigated.
The results of this study could have important implications for the treatment of the specific clinical factors and for housing programs for forensic patients after release from a forensic clinic to decrease the chances of recidivism in violent crime.
Methods
Participants and Procedure
The original sample consisted of 347 Dutch forensic psychiatric patients with a TBS measure (De Ruiter & Trestman, 2007) who were unconditionally released from 12 Dutch Forensic Psychiatric Centers (FPC) between 2004 and 2008. This means that the court order is terminated without further conditions. The person is no longer under the supervision of the institution and there are no mandatory treatments. This can happen when treatment has been successful and the person is no longer a danger to society (Janković et al., 2021). A TBS order can be imposed if 1) the defendant is declared partially or completely unaccountable due to the presence of a mental disorder, 2) the prison sentence is at least 4 years and 3) the person poses a threat to public safety (De Ruiter & Trestman, 2007). Within the sample 91.3% were male and 8.7% were female. However, the females were excluded from the sample because the HKT-R was not validated for female offenders (Spreen et al., 2014) and the female population was very small for the intended statistical analysis. Data on demographic characteristics and psychiatric disorders based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev. [DSM-IV-TR]; American Psychiatric Association [APA], 2000) were retrospectively derived from patient electronic files. Furthermore, 20 trained coders scored the HKT-R at the time of unconditional release using information from patients’ files that contained details about their background, criminal history, psychiatric evaluation reports, treatment history, appeals for resignation and prolongation advice. The interrater reliability of the Historical (.66–.89) and Clinical domains (.67–.94) was rated as good to very good. The interrater reliability of the Future domain (.09–.67) was considered low to reasonable, but this domain was not included in our study (Bogaerts et al., 2018). Before running analyses, all data were anonymized. The study was approved by the Scientific Research Committee of the FPC Kijvelanden, the Dutch Ministry of Security and Justice, the 12 directors of the forensic institutions included in this study, and the Ethical Review Board of Tilburg University.
The sample characteristics are presented in Table 2. Of the final sample of 316 males, 95.3% (n = 301) had a Dutch nationality, 2.8% (n = 9) had another nationality, and 1.9% (n = 6) had an additional nationality. The mean age at admission to the clinic was 32 years old (range 17–66) and patients stayed in the FPCs for 7.77 years on average (SD = 3.15, range 2–20). Within the sample 49.7% (n = 157) had some problems with living arrangements but were not homeless, 24.4% (n = 77) had occasional periods of relocation and homelessness, and 25.9% (n = 82) of the sample had a very problematic history of homelessness. Regarding to clinical diagnosis according to the DSM-IV-TR (APA, 2000; Table A1 in Supplemental Appendix) substance-related disorders (n = 112, 35.4%) and schizophrenia and other psychotic disorders (n = 70, 21.3%) were the most common. The most frequently diagnosed personality disorders were personality disorder not otherwise specified (n = 165, 52.2%) and cluster B personality disorders (n = 84, 26.6%). Concerning previously committed offenses, the participants were convicted of traffic and civil violations (n = 131, 41.5%), drug-related offenses (n = 24, 7.6%), destruction of property (n = 107, 33.9%), fiscal capital and profit offenses (n = 203, 64.2%), moderate violence and possession of arms (n = 192, 60.8%), power by force (n = 124, 39.2%), severe violence (n = 85, 26.9%), sexual offenses to adults (n = 56, 17.7%), and children (n = 23, 7.3%), manslaughter (n = 120, 38%), arson (n = 44, 13.9%), and murder (n = 52, 16.5%). Of the patients, 16.5% (n = 52) recidivated within 5 years after unconditional release from the FPC. The descriptive statistics of the clinical factors are presented in Table 3.
Sample Characteristics.
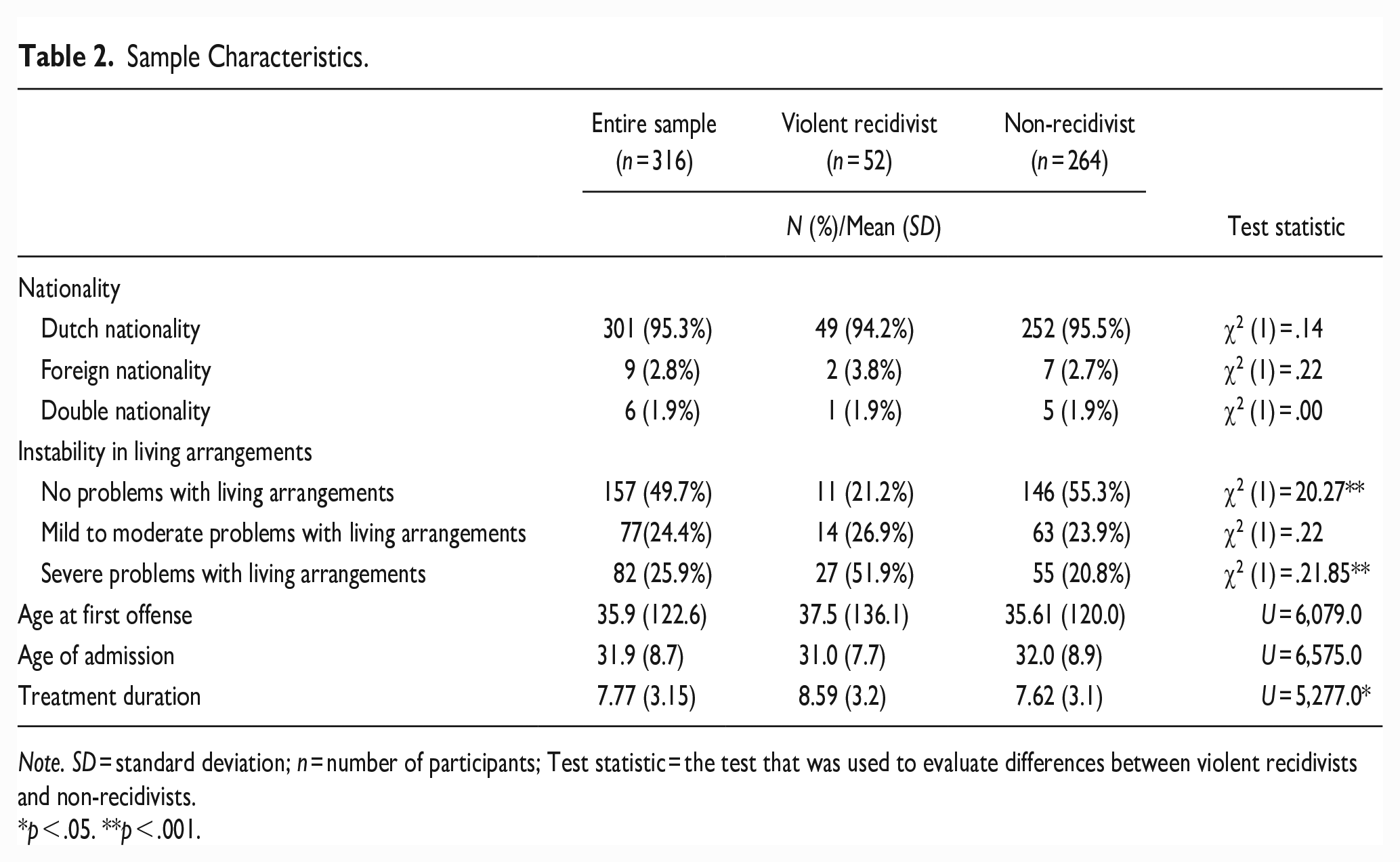
Note. SD = standard deviation; n = number of participants; Test statistic = the test that was used to evaluate differences between violent recidivists and non-recidivists.
p < .05. **p < .001.
Means and Standard Deviations of Clinical Risk and Protective Factors.
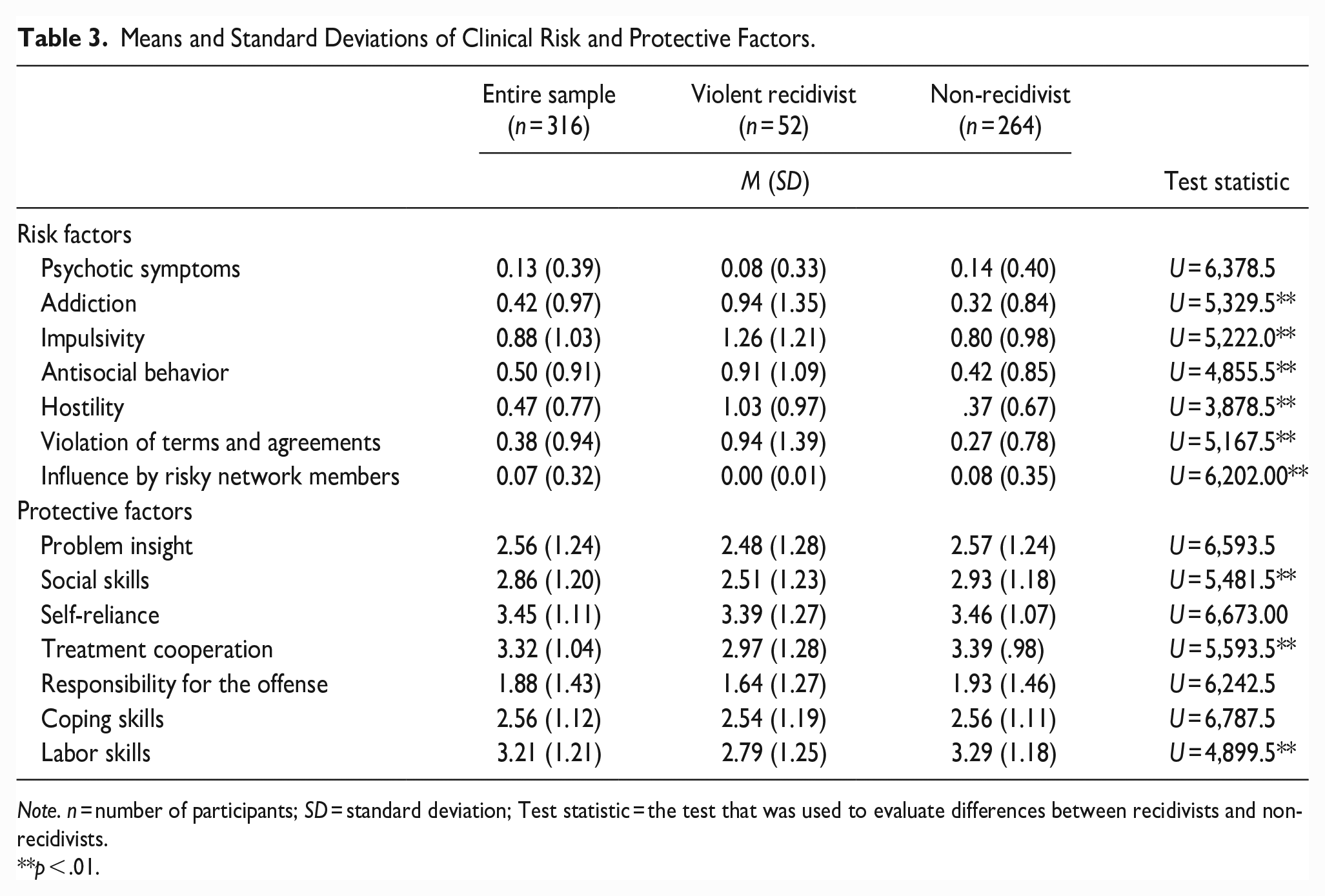
Note. n = number of participants; SD = standard deviation; Test statistic = the test that was used to evaluate differences between recidivists and non-recidivists.
p < .01.
Additionally, differences between violent recidivists and non-recidivist were computed regarding the sample characteristics (Table 2), axis I and axis II psychiatric disorders (Table A1 in Supplemental Appendix), clinical risk and protective factors (Table 3), and criminal history (Table A2 in Supplemental Appendix). Results showed that recidivists had significantly more severe problems regarding living arrangements in comparison to non-recidivist and were more frequently diagnosed with intellectual disability. Moreover, recidivists scored significantly higher on the clinical risk factors addiction, impulsivity, antisocial behavior, hostility, and violation of terms and agreements, while non-recidivists scored significantly higher on influence by risky network members. Regarding protective risk factors, recidivists scored significantly lower on social skills, treatment cooperation, and labor skills in comparison to non-recidivists. Lastly, there were no other significant differences between violent recidivists and non-recidivists. For a complete overview, see Tables 2 and 3 and Tables A1 and A2 in Supplemental Appendix.
Measures
Historical Clinical Future–Revised (HKT-R)
The HKT-R (Spreen et al., 2014) was used to assess the instability in living arrangements as well as clinical risk and protective factors. It is a well-validated instrument for assessing the risk of violent and general recidivism among forensic psychiatric patients. It measures 12 historical factors, which refer to the patient history before the TBS-index offense. It also measures 14 clinical factors referring to the patients’ dynamic behavior within the 12 months before the assessment. In previous research, the predictive validity of the Clinical domain was marginal (area under curve = 0.69) 5 years after discharge (Bogaerts et al., 2018). Lastly, it assesses seven future indicators for violent reoffending, which estimate the necessary skills of the patient to avoid prospective risky situations (Spreen et al., 2014). In this study, we only included the historical indicator instability in living arrangements as well as 14 clinical indicators.
Instability in living arrangements can be defined as the severity and chronicity of social and psychiatric problems, that result in homelessness (Spreen et al., 2014). The indicator living arrangements was originally rated on a 5-point Likert-type scale ranging from 0 = no problems regarding living arrangements to 4 = reflected homelessness and incapability to live incidental. To facilitate the interpretation and maintain statistical power, the number of categories was reduced to three. The first category included patients who had no problems with living arrangements and the group who had difficulties with living arrangements only for a period but were not homeless (0). The second category (1) included a group of patients with occasional periods of relocation and homelessness. The third category (2) were patients with repeated periods of homelessness, problematic history in living arrangements and who were incapable of living independently.
Furthermore, the 14 clinical indicators of the HKT-R were equally divided into seven risk factors and seven protective factors (Table 1). All factors were independently rated on a 5-point Likert-type scale, ranging from 0 = none or very low risk to 4 = high level of risk.
Original protective factors were recoded such that 0 = no protection and 4 = high protection.
In the present study, the internal consistency of the Clinical domain was very good with Cronbach’s alpha of .85.
Violent recidivism
Violent recidivism was defined as violence or the threat of violence against another person (e.g., Garritsen et al., 2022). This includes crimes of mild to moderate violence, power by force, severe violence, moral offenses to adults, violent sexual assault, robbery with violence, manslaughter, and premeditated murder. Information about violent recidivism was assembled by the Dutch Ministry of Security and Justice, after discharge up until July 11, 2011. The reconviction data was collected up until 5 years after unconditional release. It was coded such that 0 = non-recidivist and 1 = violent recidivist.
Statistical Analysis
All analyses were conducted using IBS SPSS statistics version 28 and the Process extension (Hayes, 2017). Firstly, we excluded 30 female participants and one participant with more than 10% missing values (Bennett, 2001), which resulted in a final sample of 316 participants. Subsequently, it was also checked if missing data were at random by using Little’s missing completely at random (MCAR) test. The test was significant, χ2 (1313) = 1491.95, p = 0.000, which means that we cannot assume that the data are MCAR. Because the HKT-R was assessed by trained researchers, missingness was most likely caused by deficiency within the patient files, and not by specific patterns in the missing data. Thus, in the case of missing data, the multiple imputation method was used. Multiple imputation runs simulations on missing data relative to data that is available and replaces missing values with imputed values. In the next step, the descriptive statistics of the final sample were computed. To evaluate whether sample characteristics differentiated between violent recidivists and non-recidivists, we utilized Mann-Whitney U tests for ordinal and or not normally continuous variables and Chi-square for categorical variables. Furthermore, to analyze the associations between the clinical risk and protective factors, living arrangements, and violent recidivism correlations were conducted. Because recidivism is a binary outcome, we conducted a point biserial correlation between 14 clinical HKT-R factors and recidivism, and a Pearson’s correlation between pairs of clinical factors.
To investigate whether instability in living arrangements moderates the link between the 14 clinical factors and violent recidivism up to 5 years following unconditional release, 14 separate moderation analyses were performed using PROCESS macro (model 1) with a three-level categorical moderator. Within each analysis, we used the 13 remaining variables as covariates. In the case of a binary outcome, PROCESS macro (model 1) uses binary logistic regression to determine which independent variables are of influence on the dependent variable and evaluate the probability of the outcome (Petrie & Sabin, 2005). Finally, in case of significant interactions, we would investigate the influence of each category of living arrangements on the effect between the seven risk and seven protective factors on violent recidivism using a simple slope analysis. In the absence of significant interactions, we would remove the interaction effects from the model when interpreting the direct effects by means of a binary logistic regression.
Before performing a binary logistic regression, we checked whether all necessary assumptions were met. They included the dependent variable to be measured on a dichotomous scale, to have at least one independent variable that is measured on a continuous or nominal scale, independence of observations, a linear relationship between the logit transformation of the dependent variable and the independent variables (Box-Tidwell, 1962), and to have a minimum of 10 cases per independent variable to get reliable estimates (Peduzzi et al., 1996). Clinical risk and protective factors were originally measured on an ordinal scale; however, they can be treated as continuous variables in binary logistic regression (Winship & Mare, 1984). All the assumptions were met, except for the assumption of linearity in the logit of coping skills. Therefore, to meet this assumption, natural logarithm transformation was used (Schreiber-Gregory et al., 2018).
Results
Correlations are presented in Table 4. Considering risk factors, addiction, impulsivity, antisocial behavior, hostility, and violation of terms and agreements were significantly positively associated with violent recidivism. For the protective factors, social skills, treatment cooperation, and labor skills were significantly negatively associated with violent recidivism. Other risk and protective factors were not significantly associated with violent recidivism. Regarding living arrangements, it was significantly positively associated with violent recidivism as well as with psychotic symptoms, addiction and violation of terms and agreements, and significantly negatively associated with antisocial behavior and treatment cooperation.
Correlations Between the Main Variables.
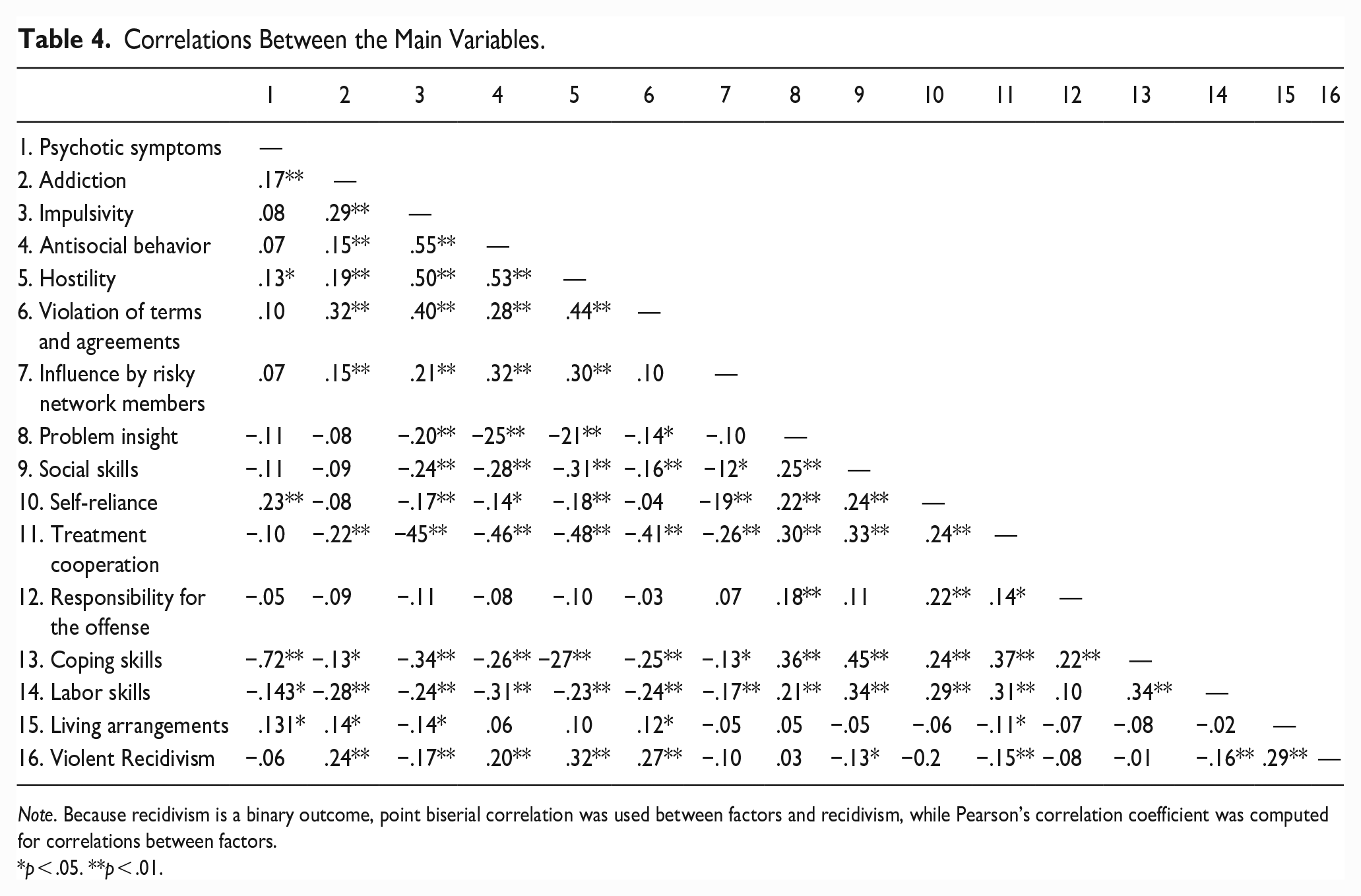
Note. Because recidivism is a binary outcome, point biserial correlation was used between factors and recidivism, while Pearson’s correlation coefficient was computed for correlations between factors.
p < .05. **p < .01.
Next, the moderating effect of living arrangements was tested on the association between the 14 clinical risk and protective factors and violent recidivism. Instability in living arrangements was not a significant moderator in the association of the seven clinical and protective factors with violent recidivism (see Tables A4 and A5 in Supplemental Appendix).
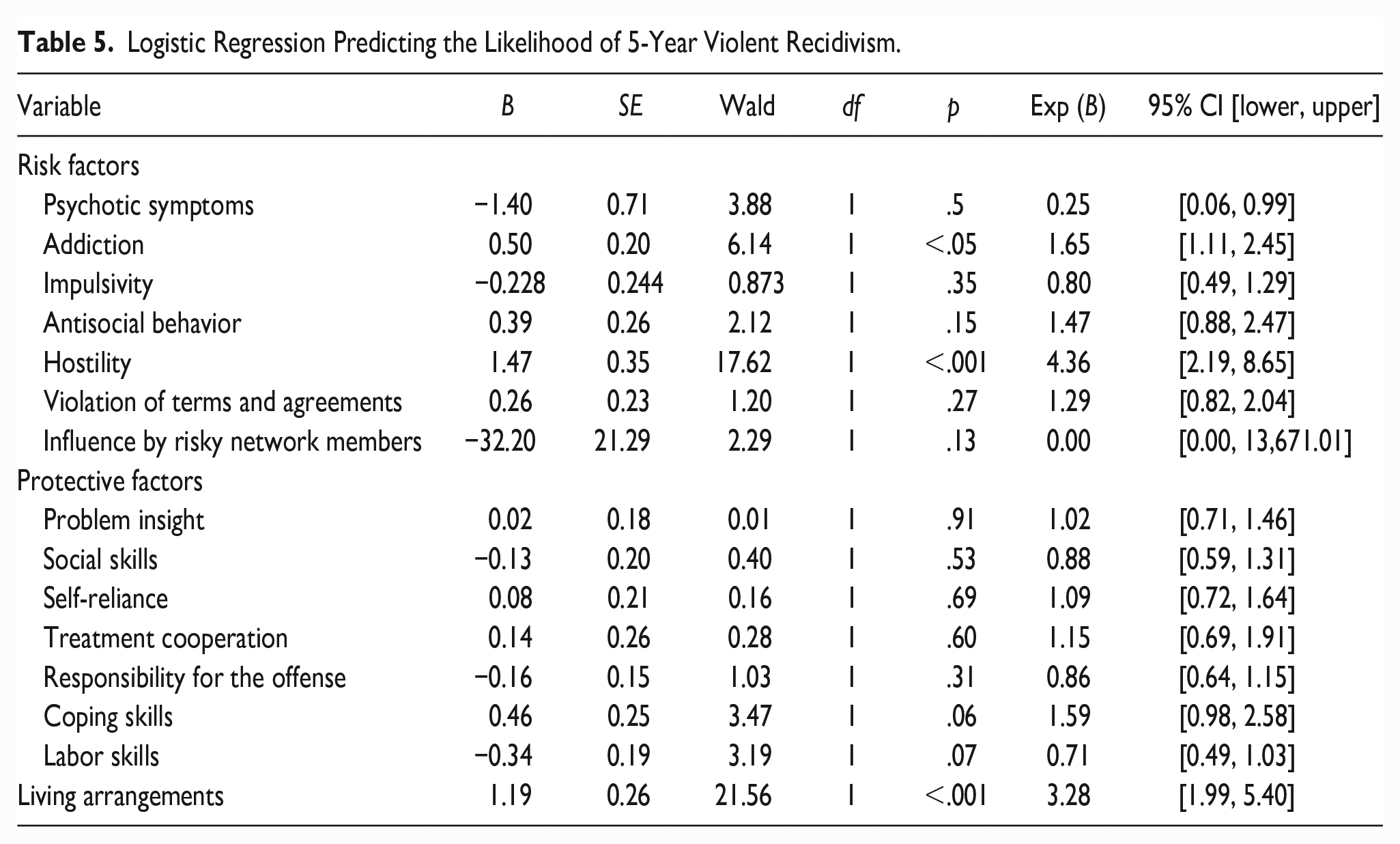
In the absence of a moderation effect, a binary logistic regression was performed to analyze the direct effects of the clinical HKT-R factors and living arrangements on the risk of violent recidivism. The model containing all factors could differentiate between recidivist and non-recidivist χ2 (15) = 106.50, p < .001 and the data fitted the model well based on the Hosmer and Lemeshow test, χ2 (8) = 14.60, p = .07. According to the Nagelkerke’s R2 the model explained 48.4% of the variance in violent recidivism and correctly classified 90.2% of the cases. The results (Table 5) revealed that hostility (OR 4.35), addiction (OR 1.65), and instability in living arrangements (OR 3.28) were significantly positively associated with violent recidivism implying that the likelihood of violent recidivism increases with each unit increase of these factors. In contrast, psychotic symptoms (OR 0.25) had a significant and negative association with violent recidivism indicating that the likelihood of violent recidivism decreases with each unit increase of this factor. Within the model, there were no other significant predictors of violent recidivism.
Logistic Regression Predicting the Likelihood of 5-Year Violent Recidivism.
Discussion
This study investigated the influence of instability in living arrangements on the association between the seven risk and seven protective factors of the HKT-R and violent recidivism in a sample of 316 male forensic psychiatric patients. Patients were followed for up to 5 years after unconditional release from any of the 12 Dutch FPCs. Contrary to our expectations, there was no moderating effect of instability in living arrangements on the 14 HKT-R factors in predicting violent recidivism. Instability in living arrangements and some risk factors significantly and directly predicted violent recidivism.
Our results provide no evidence that living arrangements enhance the negative link between risk factors and violent recidivism and weaken the positive link between protective factors and violent recidivism. A possible explanation for the lack of significant moderation effect may be that the data were obtained at the end of the treatment program. At unconditional release, 94.9% (n = 285) of the participants had contact only with protective network members, who provided treatment support. Only 4.7% (n = 30) focused on both their prosocial network and antisocial network and only one participant (0.3%) was influenced by an antisocial network. Furthermore, our hypothesis that instability in living arrangements would moderate the association between psychotic symptoms and violent recidivism can also be rejected. It is possible that this result was influenced by the high skewness and kurtosis of psychotic symptoms (Table A3 in Supplemental Appendix; Cain et al., 2017), which may lead to non-significance. Likewise, no moderation effect was found for the association between addiction and violent recidivism. This result can be partially explained by the GLM which states that stability in living arrangements does not mean that a person necessarily has the prosocial resources to fulfill all other primary goods. In the absence of prosocial resources, maladaptive behavior can cause crime (Ward & Stewart, 2003). Thus, regardless of the stability in living arrangements, a person may still have an addiction that needs to be satisfied. A similar statement also applies to labor skills. If someone does not have a prosocial way to obtain an income, he or she may turn to crime to satisfy this primary good.
Because of the absence of significant moderation effects, we examined the direct effects of the 14 clinical HKT-R factors and living arrangements on violent recidivism. The results showed that more unstable living arrangements and higher levels of addiction and hostility, but lower levels of psychotic symptoms, significantly increased the likelihood of violent recidivism up to 5 years after unconditional release from an FPC. Our finding revealed that the higher the instability in living arrangements, the greater the chances of violent recidivism, which is consistent with previous studies (Jacobs & Gottlieb, 2020; Markarios et al., 2010). This finding is also in line with the GLM model, in which criminality can be seen as maladaptive behavior, resulting from a discrepancy between available prosocial results and the resources necessary to satisfy primary goods (Barnao et al., 2016). Homelessness prevents people from participating socially (Barnao et al., 2016; Gaetz, 2004) and professionally (Gaetz, 2004), which may lead to adopting illegal strategies to obtain income.
Moreover, consistent with previous research (e.g., Guebert & Olver, 2014) we found that patients who had more problems with addiction had a higher chance of recidivating into violent crime after release. This finding also supports the RNR model that identifies addiction as one of the central eight risk factors for violent recidivism (Andrews & Bonta, 2010; Bonta & Andrews, 2007). It could be that higher levels of addiction contribute to more violent behavior because drug use can negatively affect impulse control and risk perception (Jung, 2010), which can subsequently lead to getting into conflict situations more easily. Alternatively, addiction may initiate a criminal carrier because of the need to finance drug habits (Nordstrom & Dackis, 2011).
In line with prior studies on recidivism among sexual offenders (Firestone et al., 2005), hostility was also found to be a direct predictor of violent recidivism. High scorers on hostility suspect others of negative intentions and attribute hostile motives to systems, others, or institutions (Spreen et al., 2014). It is possible that individuals who have experienced aggression develop more hostile attribution bias, which makes them more likely to interpret ambiguous information as threatening or hostile (Klein-Tuente et al., 2019).
Furthermore, unlike previous research documenting a significant positive association between psychotic symptoms and violent recidivism (Draine & Solomon, 1994; Jones et al., 2021; Lamberti, 2007), our study found an inverse association. A possible explanation for this finding could be attributed to the fact that the maximum score of this variable was two. That indicates there were one or more psychotic episodes that led to undirected transgressive behavior (Spreen et al., 2014). Patients with psychotic symptoms may have stopped taking medication after release, making them more likely to be hospitalized and less likely to recidivate. Alternatively, it may also be that the diverged skewness and kurtosis (Table A3 in Supplemental Appendix) lead to an artificial significant effect (Cain et al., 2017). This can be further supported by the fact that no bivariate association was found between psychotic symptoms and violent recidivism.
Finally, no other factors were directly related to violent recidivism. Although violent recidivism correlated significantly and positively with impulsivity, antisocial behavior, and violation of terms and agreements, these associations became insignificant in the presence of other clinical HKT-R factors.
This study is not without limitations. First, only male forensic psychiatric patients were included, making generalizability only possible for male forensic patients. Second, because the data collection was based on patients’ criminal files, some factors could not be coded due to a lack of information. In addition, the HKT-R was retrospectively coded, which may lead to biased estimates Therefore, to obtain more accurate estimates, it would be better to base the assessment on direct observations. Third, of the 316 participants, only 52 recidivated violently within 5 years after unconditional release. Since it is a small percentage of the total sample, this could have impacted the statistical power of the current study. Future studies may be able to use longer follow-ups. A fourth limitation regards the historical item instability in living arrangements. This item tells us about living arrangements before the index offense, however, results would be more accurate if living arrangements after unconditional release were taken into account.
Despite these limitations, the study offers important insights into the associations between instability in living arrangements, clinical risk and protective factors, and violent recidivism. This is highly relevant because of the potential damage of violent recidivism to both victims and society (Nagtegaal et al., 2016). To the best of our knowledge, this is the first study to investigate whether instability in living arrangements influences the links between seven risk and seven protective factors of the HKT-R and violent recidivism in forensic psychiatric patients. Although instability in living arrangements did not moderate these links, it directly contributed to violent recidivism. This means that housing interventions can be seen as an essential part of offender rehabilitation in preventing violent recidivism. Besides that, in the current study, addiction and hostility were found to directly influence violent recidivism and therefore, they can also represent important treatment targets. Since hostility is significantly associated with antisocial behavior and impulsivity (Bogaerts et al., 2020), these factors may indirectly reduce as well, while reducing addiction is already included as an important treatment goal within the RNR model (Bonta & Andrews, 2007).
In addition, we also discuss key policy implications of these findings and promising paths for policy-relevant research. People with mental illnesses who are homeless or have previously been institutionalized are particularly susceptible to being imprisoned again (Hatcher, 2010). Perhaps the lack of appropriate resources to care for the mentally ill contributes to their incarceration. Alternative services for those with mental illnesses should be introduced as part of a policy change to ensure that they receive the appropriate care needed to function adequately in society. Possibly programs such as Housing First can help offenders after their release from an FPC. As a first step in treating homelessness, the Housing First strategy seeks to help clients obtain permanent housing. Housing is provided regardless of adherence to medical treatment or abstinence from drugs or alcohol. Housing First includes ongoing support via programs like Assertive Community Treatment or Intensive Case Management. Numerous Housing First initiatives have already been launched in North America and Scandinavia, and governments in other countries, such as France and the United Kingdom, have expressed interest in adopting the idea (Baxter et al., 2019). Housing First approaches appear to be quite effective at reducing homelessness among disadvantaged participants, according to a systematic review (Baxter et al., 2019). Particularly, compared to control groups, intervention groups had lower rates of emergency room visits, fewer hospitalizations, and less time spent in the hospital. In each study, intervention participants spent more days in housing. However, there was no clear difference in substance use. Research on the long-term health effects is necessary. It would also be relevant to investigate whether recidivism rates can be reduced after these housing interventions in the forensic population.
Overall, the present study helps to understand what factors may influence the recidivism of mentally ill individuals. This study also supports both the GLM and the RNR model and highlights the importance of reducing the needs of individuals that lead to crimes. This could be highly relevant to the development of criminal justice decision-making and the implementation of well-designed programs in correctional institutions. The current study showed that addiction and hostility should be considered important targets for treatment, along with housing interventions that could be a valuable component of care for forensic psychiatric patients.
Supplemental Material
sj-docx-1-cad-10.1177_00111287231180125 – Supplemental material for The Influence of Homelessness on the Relationship Between Clinical Risk and Protective Factors With Violent Recidivism
Supplemental material, sj-docx-1-cad-10.1177_00111287231180125 for The Influence of Homelessness on the Relationship Between Clinical Risk and Protective Factors With Violent Recidivism by Iris Francke, Stefan Bogaerts and Marija Janković in Crime & Delinquency
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.