
Abstract
Links between identified-victims, which occur if escape of one has led to rescue of others (as cluster of victims in single location or controlled-individuals across a network of locations), have implications for how the totality of victims of modern slavery is estimated. Information from identified-victims can help to identify densely or dangerously trafficked-routes. Vulnerability of victims is not ended by their liberation: evidence-based healthcare and other support protocols are needed to assist recovery and resilience. The evidence-base for national protocols would be enhanced if over half the identified-victims agreed to join a research-led cohort by which morbidity and mortality could be monitored; location notified if the participant was again in extremis; with DNA-sampling offered as means to re-unite trafficked family-members.
Principal Epidemiological Perspectives
The sort of labor (domestic, physical, sexual) enforced upon victims of modern slavery, for example those within the UK (Her Majesty’s Government et al., 2018), differs by the gender and age-group of the identified victim.
The toll of sex workers were murdered in the UK between 1 January 2000 and 25 May 2018 was 104, a 21st century rate of 5.6 such murders per year. 1 All were female, bar two, and 8/102 female sex workers died in Scotland where five convictions were achieved (Aberdeen 3/3; Falkirk 1/1; Glasgow 1/3; Renton 0/1). In the 1990s (Cunningham et al., 2018), eight female sex workers had been murdered in Scotland, with only two convictions achieved (Glasgow 1/7; Leith 1/1).
The 2018 UK Annual Report on Modern Slavery (Her Majesty’s Government et al., 2018) documented that 5,143 potential victims of modern slavery were referred to the National Referral Mechanism (NRM), the UK’s identification and support system for victims of modern slavery, of whom 2,121 (41%) were children. Another 1,694 potential adult victims were referred via the “duty to notify” provision of the Modern Slavery Act 2015 which applies to England and Wales, bringing the total number of potential victims identified to 6,837.
Of NRM’s 5,134 referrals, 2,454 (47%) were female. Having collected further evidence by which to make a decision on conclusive grounds, not all individuals referred to NRM as potential victims will ultimately be assessed “on conclusive grounds” as victims of modern slavery. Of the 5,143 potential victims referred to NRM in 2017, 151 (3%) were still awaiting their reasonable grounds decision; 977 (19%) had received a negative reasonable grounds decision or their application had been withdrawn; 4,015/4,992 (80%) had received a positive reasonable grounds decision. However, only 1,289/4,015 (32%) had received their decision on conclusive grounds, which was positive for only 883/1,289 (69%). If the decisions made before October 2018 were representative, then UK’s 6,837 potential victims in 2017 may translate into 3,767 victims of modern slavery on conclusive grounds. In 2017, Scotland accounted for 212 NRM-referrals.
It clearly matters whether estimates of modern slavery in UK are based on reasonable-grounds referrals or upon cross-counts of those with a positive “conclusive grounds decision.” Delays in classification may impede victims’ access to support; and hinder UK, and other nations, from estimating the totality of their “conclusive grounds” victims of modern slavery.
In 2017, type of exploitation was cited for 2,878 adult NRM-referrals, being labor exploitation for 1,326 (46%) versus sexual for 1,182 (41%). For 1,709 child NRM-referrals, labor exploitation was cited for 1,026 (60%) versus sexual for 564 (32%). Of all 5,143 NRM-referrals in 2017, country-of-origin was UK for 819 (16%, only 140 of whom were adults) followed by 776 from Albania (15%) and 738 for Vietnam (14%). As Table 1 illustrates, the top five countries-of-origin differ for adult and child victims. The percentage female for NRM-referrals also differs by country-of-origin.
Top Five Countries-of-Origin for Adult versus Child Referrals of Potential Victims of Modern Slavery in 2017 to UK’s National Referral Mechanism (NRM) and 95% Confidence Interval (CI) for Percent Female.
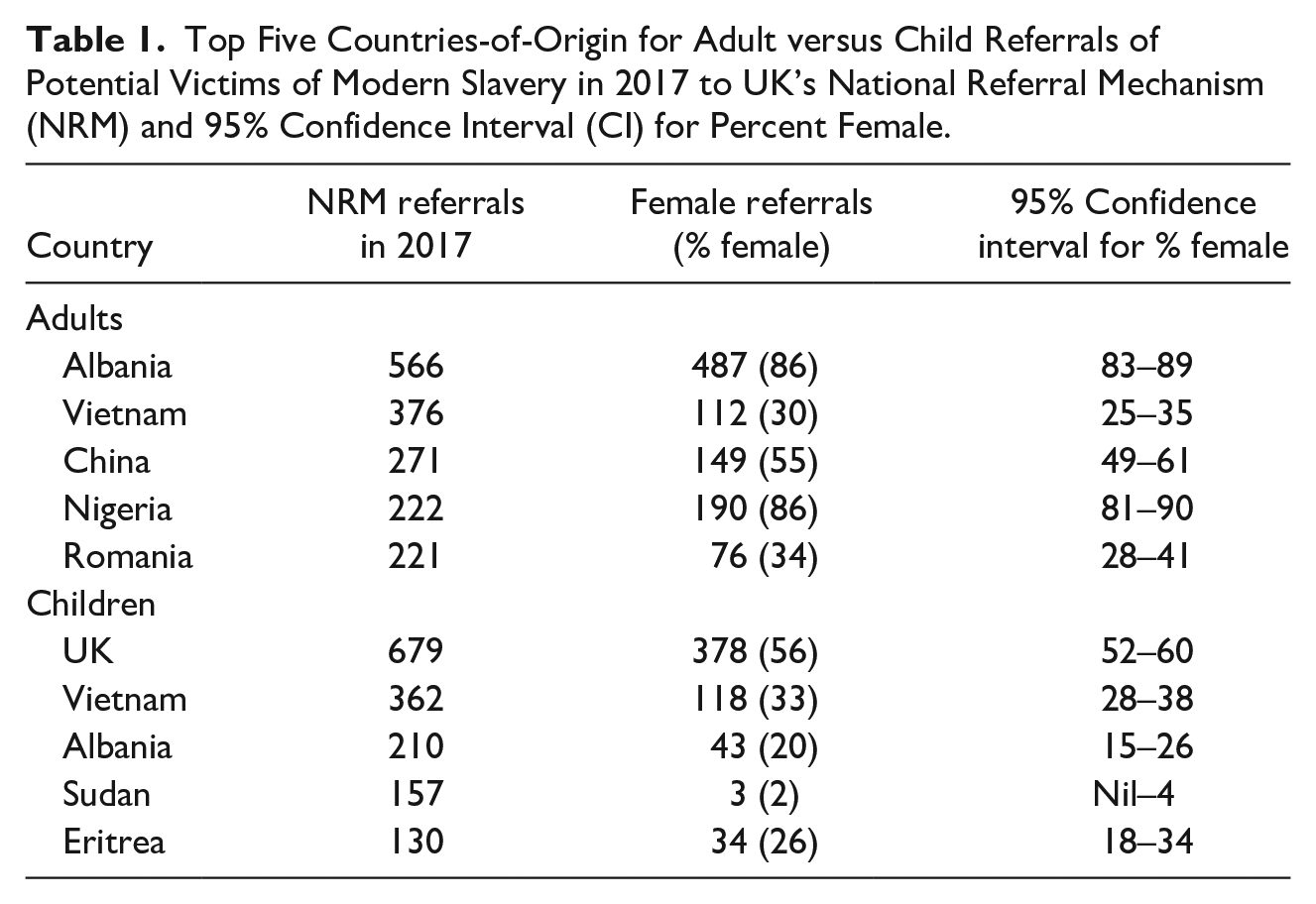
Of course, the top five countries-of-origin for NRM-referrals, or identified-victims, may not be a true reflection of the top five countries-of-origin when hidden victims are taken into account.
Type of victimization may determine whether an escaped victim was held in a cluster of fellow-victims, whose rescue can be attempted if at least one identified-victim has made their escape successfully; or as a solitary victim. Even if an identified-victim was held in isolation, his or her trafficker or controller, if apprehended, may nonetheless disclose the locations of a series of other victims, each held in separate locations.
A key method for estimating the number of victims of modern slavery, such as those held in UK (Bales et al., 2015; Silverman, 2020), is multiple systems estimation (MSE), see Bird and King (2018). Practitioners have acknowledged a range of technical challenges including: covariates which determine propensity-to-be-listed, minimal overlap between lists (national crime agency, healthcare, non-governmental voluntary support-organizations, such as for adult females versus males), dominance by a particular list (national crime agency, say), scooping (when referral to one list typically entails onward-referral to another), or perturbation when a large cluster of victims is rescued (Jones et al., 2014; King et al., 2005; Sharifi Far et al., 2020).
Generally, MSE assumes that, having conditioned on demographic and other determinants of individuals’ propensity to feature on particular lists (Bird & King, 2018; Jones et al., 2014; King et al., 2005), there is independence of the thus-listed individuals. This independence assumption is breached when listing can occur either as singletons or as a rescued-cluster or liberated-network.
For example, see Table 2, the escape and listing of singleton-A may lead to a subsequent police raid to rescue cluster-A (in a location identified by singleton-A) or to the rescue of network-A (comprising individuals e, f, and g, who are unknown to singleton-A because held separately) because the network was trafficked or controlled by the same person [controller-A] as controlled singleton-A and whose arrest was achieved thanks to information provided by singleton-A. Members of cluster-A or network-A will generally have been rescued by a national crime agency but the other organizations on whose lists these rescued-members also appear may differ because the rescued-victims have different healthcare or other needs, see Table 2.
Identified-Victims (Children in Red).
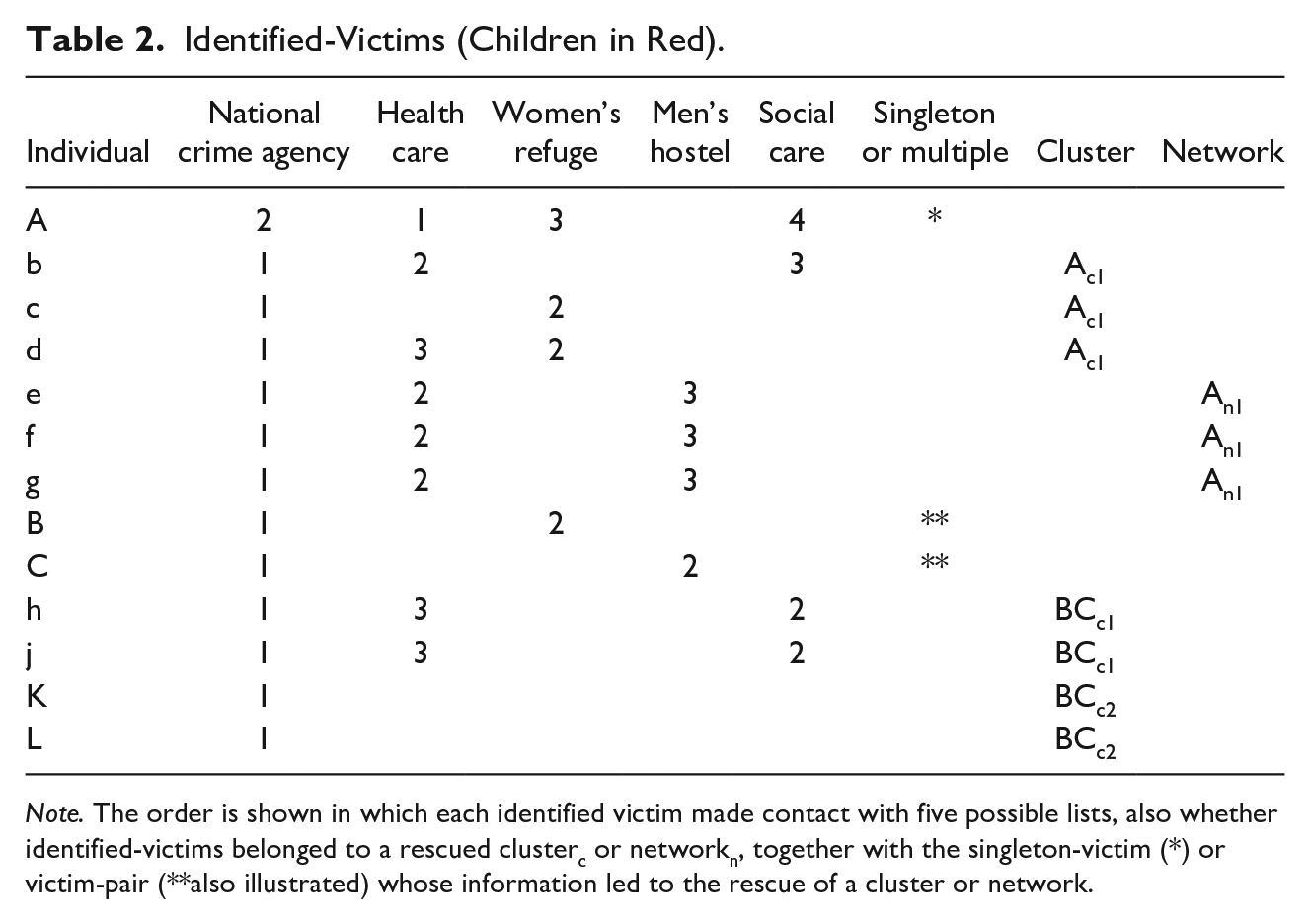
Note. The order is shown in which each identified victim made contact with five possible lists, also whether identified-victims belonged to a rescued clusterc or networkn, together with the singleton-victim (*) or victim-pair (**also illustrated) whose information led to the rescue of a cluster or network.
Entries in Table 2 identify, for each individual victim, the lists on which they feature and the date-order (1 = first, 2 = second, etc.) by which the individual was recruited to, or referred to, the different lists. The final three columns describe victims’ status as singleton, cluster or network-member: females b, c and d belong to cluster-A and were rescued on account of information that singleton-A was able to provide to the National Crime Agency, whereas males e, f, and g were held separately but belonged to network-A which was controlled by the same trafficker as had controlled the female cluster-A. Worse, controller-A may be responsible for additional clusters (Ac2, Ac3) or networks (An2). See BCc2 in Table 2 about which the informant-pair (BC) was unaware but which controller-BC disclosed when arrested.
Typically, details about individuals’ date-order of listing and the intelligence-source(s) which led to the rescue of clusters or networks of other victims are neither in the public domain nor available to analysts. However, geographical and other visualizations of the type of information on singletons, clusters and networks, such as those illustrated in Table 2, could be insightful. For example, how often do clusters entail the rescue of at least one child-victim? By contrast, informants are less unlikely to know the gender and age-group of victims who are held separately from them but controlled by the same trafficker.
Identified victims are likely to need healthcare, practical, and psychological support to aid their gradual recovery from the ordeals that they have undergone; and to build resilience, including to reduce the risk of being re-victimized. Support-protocols should be evidence-based in content and appropriately tailored to key characteristics of the victim and the type of victimization endured.
Consented (or pseudonymized) record-linkage and research-led follow-up of identified-victims, both within the UK and after re-patriation (as appropriate), should be available to this community of vulnerable victims so that “recovery-outcomes” and “hazards” are rigorously documented and subsequently ameliorated. Support-protocols could then updated on the basis of this type of research. Identified victims should have the opportunity, if willing and consented, to take part in randomized controlled trials of support-components about which the current evidence-base is weak.
Importantly, identified victims are also a major source of vital intelligence for policing and public health: not only about their cluster of fellow-victims (to be rescued) or about their trafficker/controller (to be apprehended) who may have distributed fellow-victims to diverse locations (as in Table 2) but also about their trafficked-route and the survivorship of fellow-travellers.
Trafficked-route might be from country of origin, C0, to UK via intermediate countries C1, C2 and Clast. Identified victims may recall the typical number of their “fellow-victim-travellers” en-route to UK, together with the route-section (Clast to UK, say) where the number of “fellow-victim-travellers” was maximal. Other key information could be the number of fatalities (if any) en route; and, for each fatality, the route-section (if known) wherein the fatality occurred and cause of death (given as a verbal autopsy by the informant). In principle, fatality-rates en-route to UK for “fellow-victim-travellers” can thereby be estimated; and an attempt made to put in place harm-reduction measures for the implicated route-sections.
Alternative practice is that a subset of victims of modern slavery in the UK may have made their own, or controller-subsidized, way to the UK in the false belief that an attractive, well-remunerated job awaits them. For a substantial proportion of identified child-victims, depressingly, their country of origin is UK itself. Confidential record-linkage investigation and other follow-up for at least these UK-born child-victims should be an essential public health duty. See Zarocostas (2019) who urges that health providers should receive training to enable them to give more help in recognizing and eradicating modern slavery.
Identified victims can also be asked about hospitalizations (by cause) and pregnancy (by outcome) for themselves and for fellow-victims (by gender, age-group, and type of victimization) within the UK; and to report on the death (if any; and by cause, gender, age-group, and type of victimization) of fellow-victims within the UK. This vital public health and safety information that identified victims may be able to provide can then be triangulated with other National Health Service (NHS) or police sources to arrive at improved estimates for the morbidity and mortality of UK-based victims of modern slavery.
In addition, the information gleaned could be used to improve diagnostic alerts by which the plight of other possible victims is inquired into by healthcare workers: for example, by ensuring that a patient’s accompanying person is excluded from the consultation-room for some conversations and that patient and doctor have the services of an independent interpreter. Tradesmen too—window-cleaners, plumbers, electricians—who attend domestic or work premises can also ring important alarm-bells by reporting visible or other concerns to the police.
Proper awareness of the major sources of morbidity and mortality for UK-identified victims of modern slavery in different post-identification epochs of follow-up (1st semester; 2nd semester; 2nd year; 3–5 years post-identification) would be well served if UK-identified victims of modern slavery were willing to be enrolled in a clinical research cohort, as suggested above. The inequity of what has happened to victims of modern slavery merits our best effort, properly informed by rigorous research, in learning how to redress the late sequelae of their victimization.
Research-partners in repatriation countries could have shared responsibility for ensuring that scheduled annual check-ups and unscheduled requests for support are delivered upon. Realistically, the level of follow-up to be achieved may depend on the country to which an UK-identified victim is repatriated. However, all nations to which UK-identified victims are repatriated should, ideally, be capable of tracking the survival-status of those repatriated—even if the tracking of hospitalization-events is problematic.
Mobile technology could be designed which assists cohort-participants in having their physical, psychological or psychiatric status assessed with suitable support extended, for example by UK-based research-teams even after repatriation of a participant UK-identified victim. If the cohort-participant is re-victimized, any such mobile-assist device may, unfortunately, be removed by force from her/him. Consideration might be given to minimally-invasive technological solutions, which are specifically designed to inhibit removal or provide a locator-alarm (such as the Emergency Position Indicating Radio Beacon (EPIRB) used by mountaineers) that the participant could activate in extremis to signal his/her physical location.
Victimized family-members, such as siblings, may be trafficked to different countries or to different parts (England, Wales, Scotland, Northern Ireland) of the same-destination-country (UK). Consultation with UK-identified victims would be necessary to discover the extent of their willingness (or not) to provide a DNA-sample for a novel identified-victim-DNA database: to be used to re-unite trafficked-family-members; and hence give potential justification for their not being repatriated to country-of-origin but co-located more safely in UK or a third country. Re-uniting of trafficked family-members would be more likely if, periodically, any such identified-victim-DNA-databases could be pooled internationally.
Public Health Perspective on Mortality
A priori estimates for the death-rate within UK of victims of modern slavery who have been trafficked to UK may depend upon whether the victim has become drug-dependent—for example, to cope with prostitution; or has endured other forms of serial or severe physical (and/or psychological) abuse. Whereas the death-rate of young adult males in the UK is around 1 per 1,000 person-years (pys), and deprivation may account for (say) 3-fold-increase to 3 per 1,000 pys, opioid-dependence increases the death-rate dramatically to between 10 and 20 per 1,000 pys.
Based on the relative population-sizes for England and Scotland, Scotland may have 1,500 victims of modern slavery in any 1 year, only 500 of whom (i.e., one-third) have been identified to Police Scotland, medical or voluntary services. Assuming that at most 70% of identified victims (i.e., 350 per annum) would be willing to give consent to join a research-cohort with planned follow-up for at least 5 years but with 10% loss to follow-up per annum likely, then initial research-funding for 6 years (say) would be needed for Scotland to achieve the person-years of follow-up in Table 3.
Person-Years’ Follow-Up From Recruiting 350 Identified Victims Annually to Research-Cohort.
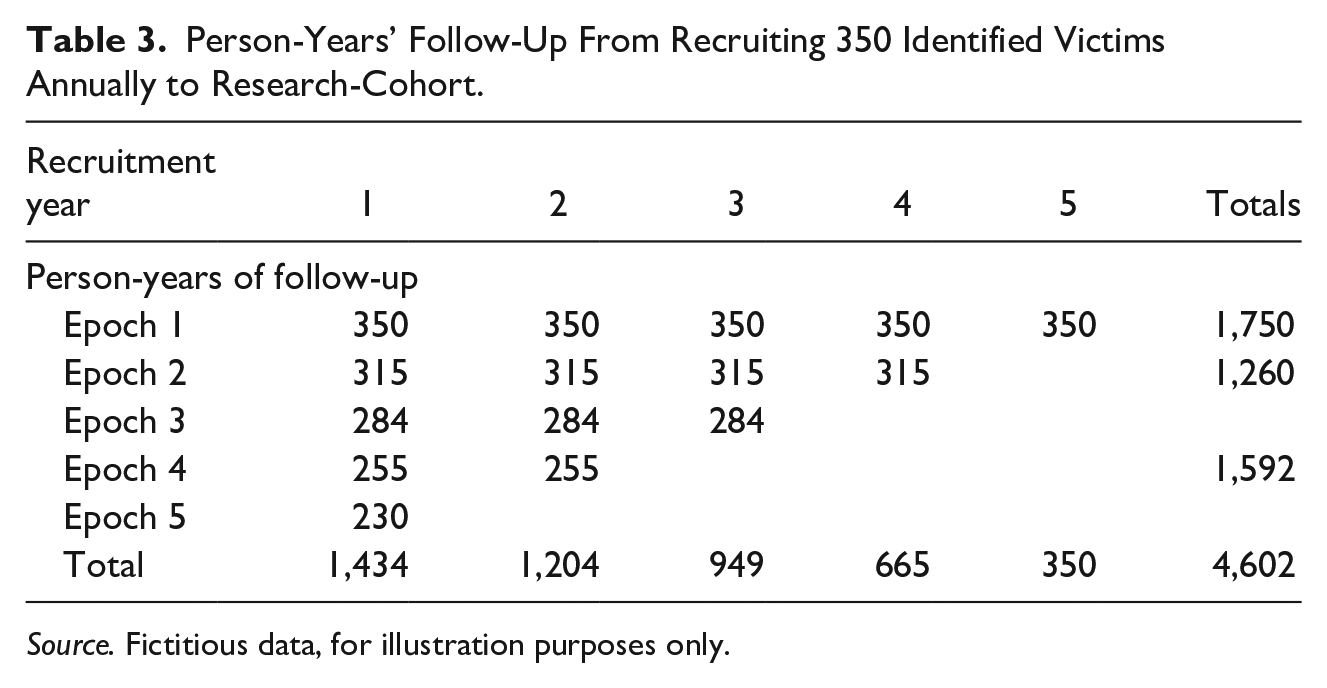
Source. Fictitious data, for illustration purposes only.
If the same death-rate pertained in the first two epochs of follow-up and a different rate in epochs 3 + 4 + 5, then the expected width of 95% confidence intervals (CIs) for indicative death-rates in Epochs 1+2 versus Epochs 3 + 4 + 5 are shown in Table 4.
Expected Width of 95% Confidence Intervals for Death-Rates Ranging from 3 to 20 per 1,000 Person-Years of Follow-Up (0.3%–2%), According to Epoch of Follow-Up.
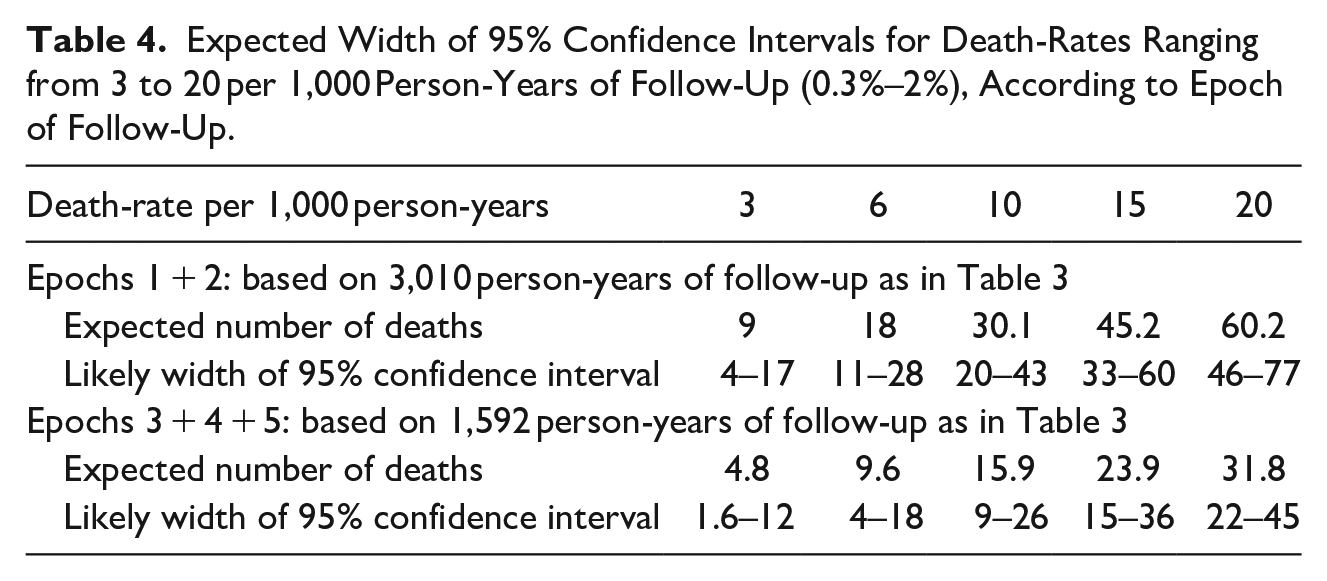
The proposed research-cohort would be sufficiently large both to identify 3-fold differences in Epoch 1 + 2 death-rates per 1,000 person-years (such as
Expected Number of Deaths Based on Person-Years of Follow-Up Shown in Table 3 and Presumed 50% Reduction in Death-Rate from Epochs 1 + 2 to Epochs 3 + 4 + 5 (Recovery).
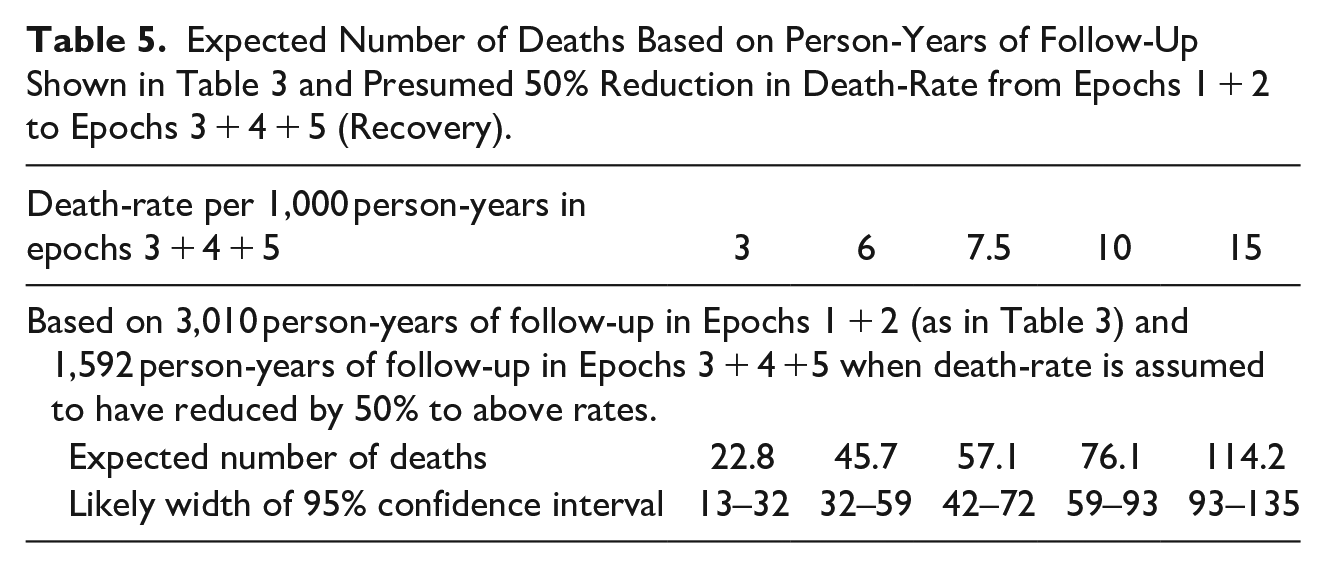
The expected number of deaths across 5-years of follow-up of the proposed enlisted cohort could range from 23 in 4,600 person-years (pys), which would be reassuringly low, to between 76 and 114 per 4,600 pys (equivalently, 1.6%–2.5% per annum) which would be as concerning as for Scotland’s methadone-clients in 2009 to 2013 (Gao et al., 2016).
National Protocol Needed for the Healthcare and Other Support of Uk-Identified Victims of Modern Slavery
Victims’ range of healthcare issues can include: malnutrition; sexually transmitted or other infectious diseases; vaccinations; fractures; grief or bereavement; psychological trauma, including post-traumatic stress disorder; psychiatric morbidity; opioid dependence or other addiction; lack of schooling. Care for victims can be complicated by lack of a shared language and by fear of policing or deportation.
Although all elements of the national healthcare and support protocol should be addressed, the order and timing for doing so must be at a pace that is comfortable for, and acceptable to, the victim, that is: patient. Both healthcare and national crime agency have a duty of care for this victim; but the window of opportunity for police to rescue other victims may close quickly if officers are unable, sensitively—as a matter of training and empathy, to question the identified-victim to elicit from them information with the potential to aid the rescue of others.
Links between identified victims (singleton, cluster, network) matter for how MSE estimation proceeds and can be investigated by simulation studies, (Sharifi Far et al., 2020); and for the extra intelligence (about type of victimization or age-group of victims) that cluster-membership entails. In policing terms, the success of rescue-raids can also be documented by the size-distribution for the rescued-clusters; or rescued-networks.
Other information which each UK-identified victim can provide about the number of those with whom s/he was trafficked to UK and about the survival of trafficked-fellow-travellers can await the victim’s willingness to relive and retell those experiences. Potentially more urgent, if murder or manslaughter were involved, is elicitation of information about the suspected death of any victim of modern slavery in the UK whom the identified victim has knowledge of.
The question of providing a DNA-sample for retention on any novel DNA-database for UK-identified victims of modern slavery, together with discussion of the potential uses of such a database, needs to be addressed very sensitively indeed as there may be initial, or ultimate, unwillingness—not only on the part of victims but also on ethical grounds by healthcare teams or if the non-governmental voluntary organizations which offer support to identified-victims are themselves sceptical about the intended uses.
Finally, each UK-identified victim can be encouraged, and helped, to answer some limited questions about her/his trafficked-route and the fate of fellow-travellers so that UK authorities and their international counterparts can appraise the relative risk-to-life of different routes and consider practical approaches to mitigate these disclosed risks for the benefit of others.
Where (whether in UK or country-of-origin) an UK-identified victim of modern slavery is relocated to after the initial phases of any national healthcare and support protocol have been worked through has potential implications for the future well-being of the victim as well as for their legal-status and entitlement to UK benefits.
Finally, if victims were willing to participate as members of a research-led follow-up cohort, UK could at least begin to amass robust information which, in time, would constitute an important evidence-base for future decision-making not only about its national protocol but also on the legal status and repatriation-risks for victims. Alternatively, the cohort’s epidemiological findings might be hypothesis-generating with randomized controlled trials instituted as the best means of determining What Works?
Discussion
We do not under-estimate the often-considerable difficulties in offering assistance: some victims of modern slavery do not wish to identify themselves as such; others claim to be working to send money home to provide for their children—even if they have no sign of having ever given birth; yet others, who need medical help, may be denied access to it or, if they attend an accident and emergency department, will have an ever-present-minder so that private conversation with the attending healthcare staff is inhibited.
Nor do we under-estimate the difficulties of follow-up of identified victims—even within UK—unless they can be registered with a general practitioner and given a Community Health Index-number (in Scotland) or NHS-number; let alone if re-atriated to their county-of-origin when date-of-emigration-from-UK and subsequent death-date may be all that can be relied upon. However, we must try and, by trying, improve our methods and support mechanisms—for victims’ sake.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.