
Abstract
People make sense of healing and growth through their cultural lenses. This study discusses the posttraumatic growth of Somali refugee women in the aftermath of traumatic events. Specifically, the study incorporates the Somali term ka bogso (being healed toward psychological wholesomeness) that emerges in cultural and spiritual response to life’s adversities into the 5Rs posttraumatic growth model for Somali refugee women. Grounded in humanizing research and decolonial psychological science perspectives, the study employed collaborative autoethnography to develop the model. Its key concepts are Running, Resettlement, Residual Stagnation, Reconciliation, and Resolution. Descriptions of the model were originally constructed orally and are presented in both written language and visual arts to make community knowledge accessible. Based on the model, the study discusses implications for community-oriented practice and the importance of decolonial knowledge coconstruction in supporting Somali refugee women who seek healing and growth. Suggestions for training, advocacy, and future research are discussed.
Somali refugee women seek to have their stories and perspectives incorporated into psychological theories and healing approaches. Therefore, we propose a five-phase posttraumatic growth model that explains the Running, Resettlement, Residual Stagnation, Reconciliation, and Resolution phases, which are developed from a Somali woman’s perspective. The model reflects the Somali cultural concept of ka bogso (being healed). We provide both narrative and visual arts as tools for utilizing this model when working with Somali refugee women.Significance of the Scholarship to the Public
Posttraumatic growth, or positive transformation as a result of highly stressful events, is ancient and universal (Calhoun & Tedeschi, 2006). However, its processes and cultural nuances are lesser known for refugee women of color from the Global South. Recognizing their displacement, humanitarian crisis, culture and spirituality, and experiences with racial, ethnic, and gender oppression is essential to understanding and facilitating their posttraumatic growth (Gómez et al., 2021; Grier-Reed et al., 2023; Lincoln et al., 2021; Sadaghiyani et al., 2023).
In particular, Somali refugee mental health is underexplored in the field of counseling psychology while Somali refugees and their families continue to encounter significant systemic, cultural, and linguistic barriers to access mental health services (Jorgenson & Nilsson, 2021). A lack of theories reflecting Somali refugee women’s perspectives perpetuate the friction between their cultural beliefs (e.g., collectivist and Islamic worldviews with the community as the expert) and those of Western and Global-North-centered approaches (e.g., individualistic and Judeo-Christian worldviews with the psychotherapist positioned as the expert; Ali-Faisal, 2020; Delaney, H. D., & DiClemente, 2005; Jacoby et al., 2015). Such frictions elicit feeling unheard, judged, alienated, and ashamed in Somali refugee women (Pavlish et al., 2010; Weatherhead & Daiches, 2010).
The present study thus attempts to address these barriers by exploring Somali refugee women’s posttraumatic growth with the utmost value of making psychological knowledge accessible and grounded in their lived experiences. Specifically, this research aims to theorize and amplify the Somali concept of ka bogso—a process of being healed toward psychological wholesomeness—which is grounded in Somali women’s epistemology. The study sought to answer the following inquiry: What does ka bogso look like for Somali refugee women in the aftermath of traumatic events? This attempt is consistent with the steadfast voice of Somali refugee women, community leaders, cultural brokers, practitioners, and scholars. That is, Somali refugee women’s perspectives on mental health should be centered and these women’s participation in psychological knowledge production should be encouraged (e.g., Jacquez et al., 2021).
In seeking deeper understanding, the study incorporates two key methodological frameworks of knowledge-coproduction: humanizing research (Paris & Winn, 2013) and a framework for decolonizing psychological science (Neville et al., 2024); in terms of data generation, the study employs a collaborative autoethnographic method (Karalis Noel et al., 2023). Somali people value oral stories, and refugees often benefit from tangible experiences (e.g., active viewing and sensory experiences, such as touch) when dealing with emotional challenges they face. The oral stories become more powerful and accessible when the stories are informed by experiential knowledge of people from similar cultural backgrounds (Makwarimba et al., 2013); the visual stories are also accessible, as they are translingual, supporting Somali refugee women’s reflections and storytelling, inclusive of those who have varied literacy skills. The following sections are organized into (a) multilayered traumas among Somalis; (b) Somali refugee women’s perspectives; (c) etic and emic perspectives on posttraumatic growth; (d) authors’ reflexivity, axiology, and methodology; (e) ka bogso: the 5Rs posttraumatic growth model; and (f) implications for theory, practice, advocacy, education, training, and research.
Multilayered Traumas Among Somalis
Somalia is in northeast Africa, bordering Kenya, Ethiopia, and Djibouti, in the area known as the Horn of Africa. The word Somali means “go and milk” (soo maal), reflecting pastoralism as the root of Somali culture and way of life (Fellin, 2013). Most Somalis have nomadic or semi-nomadic lifestyles and a rich tradition of orality and values of family/kindship/neighborhood cohesiveness, mutual support, commitment, and spirituality (Koshen, 2007). This section recognizes how their traditions, values, and communities have been disrupted by numerous traumatic events.
Historical and Collective Trauma
Although the refugee crisis is a widely known global humanitarian issue, it is important to recognize how Somalis have endured the legacy of European (e.g., Italian, British, and French) colonialism (1897-1960; Fellin, 2013). Despite Somali anti-colonial resistance, colonial rule disrupted Somali self-determination, ecological balance, autonomous labor, and the food supply system (e.g., colonial investment of agricultural land and livestock exports) while threatening Somali unity (Hough, 2011). Such colonial expansion led to prolonged droughts, floods, famine, and long-standing internal conflicts within Somali communities (Fellin, 2013), ultimately resulting in the refugee crisis which began in 1991 with the outbreak of civil war following the collapse of authoritarian military rule (Hough, 2011). This refugee crisis is called “the age of qaxootin,” a desperate exodus for Somalis who experienced the worst horrors and disbelief watching as “[their] former neighbors and friends turned on each other” (Hough, 2011, p. 7). Globally, it is estimated that over 3.8 million Somalis have been forcibly displaced (United Nations Refugee Agency, n. d). Most Somalis have fled to neighboring countries and later moved across the world, including countries of the Global North (United Nations High Commissioner for Refugees, 2023). In the United States, the number of Somali refugees increased from 2,500 in 1990 to 150,000 in 2015 (Connor & Krogstad, 2016).
Premigration Trauma
Somalis continue to cope with unresolved premigration trauma. Various premigration traumatic events include experiencing torture, witnessing the injury or death of humans and animals, family separation, conflicts between clans, shortage of food and water, disease, and illness (Carroll, 2004; Jorgenson & Nilsson, 2021). Somali women in particular experience gendered traumatic events, including gudnin (female genital mutilation) and faro-xumeyn (violence against women) in Somalia (Gardner & El Bushra, 2004; Jacoby et al., 2015; Torrance et al., 2024). They continue to be at risk of experiencing gendered violence within refugee camps. For instance, women in the Dadaab refugee camps in Kenya (94% Somali women) have reported violence rates of 93%, 91% and 16% for physical, emotional, and sexual violence, respectively (Hossain et al., 2021). Somalis have lived in refugee camps for about 30 years, leading to intergenerational impacts of the displacement, with many Somali children born in refugee camps (United Nation High Commission for Refugees, 2023).
Postmigration Trauma
Even though not all postmigration stressors (e.g., limited social support, finding employment, learning new languages; Jorgenson & Nilsson, 2021) are traumatic, such stressors impede Somali people’s ability to adjust to a new environment and live safely, fully, and joyfully. Especially, as they encounter postmigration trauma and resettlement challenges exacerbated by anti-Black, anti-Muslim, and anti-refugee biases and rhetoric in the United States (Magan, 2020). Jorgenson and Nilsson (2021) reported that 70% of Somali refugees experience shortages of food, water, or clothing because of poverty or discrimination. Somali refugee families often face additional barriers when navigating education, healthcare, and criminal justice systems due to their race, religion, language, and nation of origin. In education settings, Somali mothers often deal with dismissive and unfair treatment of their children in schools (Abdi, 2022, p. 757). In healthcare settings, Somali women often experience not only language barriers but also mistrust toward Western health beliefs, and providers may dismiss their lived experiences of physical and emotional pain (Pavlish et al., 2010). In criminal justice systems, Somali refugees and their offspring are disproportionately stopped, frisked, arrested, and incarcerated (Crosby & Brazelton, 2017; Ellis et al., 2020). Experiencing ongoing and persistent discrimination is traumatic, and the accumulated experiences with pre- and postmigration trauma can increase mental health risks. Indeed, in a clinical setting, 58% of Somali refugee women show comorbidity of depression and posttraumatic stress disorder, a prevalence rate significantly higher than the 3.4% observed in non-Somali women (Kroll et al., 2011).
Somali Refugee Women’s Perspectives
Somali women’s self-knowledge and voices play key roles in their healing and growth. Ali-Faisal’s (2020) framework of Islamic anti-patriarchal liberation psychology explains how patriarchy, racialization, and colonialism erode the identities of Muslim women. It focuses on anti-patriarchal resistance and decolonial processes; these foci aid psychologists in challenging zulm (oppression), pursuing dignity, and recovering the ethics of ummah (community care). The framework also challenges the imposition of patriarchy on Muslims, including gender-specific rules that limit full and equal participation in society. Gardner and El Bushra (2004) used similar perspectives in describing Somali refugee women’s identities, empowerment, and full participation in society. These Somali refugee women shared how they navigated both patrilineal norms and the impact of war and displacement; they also identified their strengths as caretakers, peacebuilders, and agents of change within their Somali communities.
Researchers have also recognized Somali refugee women’s emotional pain by using cultural idioms of distress, which symbolize their distress in language (Im et al., 2017). These idioms are valuable knowledge for psychologists as they serve as indicators of exposure to trauma, psychosocial and emotional functioning, and tools for the meaning-making process after trauma (Hinton and Lewis-Fernández, 2010). They also promote clients’ help-seeking and inform them of the support they need. Murug is the most common term that Somali refugees use to describe their sorrow, mourning, and grief stemming from the aftermath of traumatic events (Carroll, 2004; Im et al., 2017). Murug also has prolonged grief that overlaps with sadness, financial pressure, and anhedonia (Carroll, 2004). Additionally, qaracan is mental shock characterized as fatigue, fear, anxiety, worries, uneasiness, agitation, and suspicion of others. Both murug and qaracan are responses to the devastation of war and the loss of loved ones (Carroll, 2004; Im et al., 2017).
Somali refugee women have voiced their concerns about the U.S. healthcare systems. In a study by Pavlish et al. (2010), a Somali nurse reported that Somali refugee women experienced significant trauma before resettling in the United States, yet their trauma went untreated. Somali refugee women tend to endure their psychological struggles in silence, influenced by the stigma surrounding the outward expression of distress. Such expression can result in being gossiped about as a person with walli—a term of stigmatization in the Somali language in which an individual is considered “crazy”—and can also result in social disapproval from the Somali community (Im et al., 2017; Pavlish et al., 2010). Moreover, Somali refugee women refrain from disclosing their sorrow to their healthcare providers. This reluctance is due to the lack of vocabulary to express their struggle, discordant beliefs about health, and perceptions of healthcare providers’ judgment and disinterest in listening to their concerns (Pavlish et al., 2010).
Several studies have attempted to address traumas among Somali refugee women. For example, the Health Realization Community Coping Intervention is a community-delivered and strengths-based intervention, which emphasizes people’s resilience: “the human core of health remains accessible as resilience regardless of past experiences” (Robertson et al., 2019, p. 1079). The intervention focuses on instilling hope for health and building skills (e.g., strategies for grounding, recognizing moods) and does not encourage retelling past traumatic experiences. The intervention effectively increased Somali refugee women’s resilience and alternative cognitive strategies, such as noticing one’s thinking habits. Although not exclusively focused on women’s perspectives, Syed et al.'s (2022) analysis of digital narratives among Somalis showed that there is a mixture of progressive, stable, and regressive stories; yet, their stories may lack narratives of strength and positivity gained through suffering. These findings suggest the need to explore ways in which Somali refugee women can heal and grow after traumas, given their values and strengths, as well as the challenges accumulated from premigration and resettlement.
Etic and Emic Perspectives on Posttraumatic Growth
Etic Perspectives
From time immemorial, cultures have faced questions about the meaning and manifestation of growth in the aftermath of traumatic events. In psychology, Tedeschi and Calhoun (1996) conceptualized such growth as posttraumatic growth, which applies to events of death, serious injury and illnesses, and catastrophes. O’Leary and Ickovics (1995) suggest different terminologies, as there are three statuses after experiencing a highly stressful event: survival (changing and sustaining lower levels of functioning), recovery (returning to baseline functioning), and thriving (transforming oneself to a higher level of functioning). Posttraumatic growth is viewed as a higher level of functioning; the effective mobilization of individual and social resources enables individuals to achieve and retain such growth. Furthermore, Tedeschi and Calhoun (1996) identified five common changes of posttraumatic growth: (a) increased appreciation of life and realignment of life priorities; (b) an increased sense of relational warmth and meaningfulness in relationships; (c) a greater sense of personal strength; (d) new vision and possibilities for life; and (e) strengthened connection to spiritual and existential aspects of life.
Scholars explain two perspectives about how posttraumatic growth occurs. One perspective posits that posttraumatic growth is an outcome of the struggle with a traumatic event (Calhoun & Tedeschi, 2006). This view identifies personal variables (e.g., disposition) and environmental predictors (e.g., social support, living conditions) of posttraumatic growth, which are linked by feedback loops. In the same vein, the way individuals change their beliefs, goals, behaviors, and life narratives is influenced by distal factors (e.g., past experiences) and proximal factors (e.g., current or enduring stress; Tedeschi & Calhoun, 1996).
Another perspective views posttraumatic growth as cognitive coping (Davis et al., 1998; Filipp, 1999). According to an information-processing view of coping, individuals initially engage in attentive and comparative processes—comparing themselves to their past self or others—to perceive their reality and then reach an interpretive reality, seeking a subjective explanation of what happened and why it happened (Filipp, 1999). Similarly, from a meaning-making point of view, individuals synthesize both causal attributions (e.g., “Why did it happen?”) and benefit attributions (“What was it for?”; Davis et al., 1998).
These etic perspectives may capture some aspects of Somali refugee women’s experiences with posttraumatic growth. However, they often assume trauma is a past, individual, and isolated event and that posttraumatic growth follows a linear, universal process. Such assumptions fail to account for the complexities of Somali refugee women’s unique and collective experiences, which include historical and premigration trauma compounded by ongoing postmigration stressors and traumatic events.
Emic Perspectives
Şimşir Gökalp and Haktanir’s (2022) identified four psychological gains across 12 qualitative studies on refugees’ posttraumatic growth: (a) improved psychological functioning (e.g., distress tolerance); (b) enhanced interpersonal relationships (e.g., compassion); (c) reconstructed meaning of life (e.g., appreciation of life); and (d) positive future directions (e.g., hope for the future). Scholars have also observed that individuals’ experiences with posttraumatic growth vary depending on their geographic and cultural context. For instance, Ferriss and Forrest-Bank (2018) articulated the conceptual dissonance between Somali refugees’ perspectives and Western and Global-North-centered perspectives. The major dissonance arises due to the lack of Islamic worldviews and the use of individualistic concepts and language, such as “Personal Strengths.” They underscored that Somali refugees believe in collective strengths that lie in family, neighbors, and communities. These findings suggest the importance of including cultural, collectivist, and spiritual influences in posttraumatic growth among Somali refugee women.
Two levels of cultural influence play a role in ways of conceptualizing and responding to traumatic events: (a) proximate influences and (b) distal influences. Proximate influences refer to people with whom the individual directly interacts, including primary reference groups (e.g., family, friends, neighbors); social norms influence what are acceptable behaviors facing highly stressful events, including the desirability of emotional disclosure (Calhoun et al., 2010). Early interactions in Somalia with their kinship influence Somali refugee women’s worldviews (Gardner & El Bushra, 2004). After resettlement, they face a loss of connection to their original primary groups (Ferriss & Forrest-Bank, 2018). While attempting to cope with loss and change, they also try to form new reference groups in the United States, such as religious groups, close friends, neighbors, community leaders, or newcomers from Somalia or other countries (Makwarimba et al., 2013; McMichael & Manderson, 2004).
Distal influences refer to societal narratives and prevailing views within a cultural context relevant to persons facing highly stressful events (Calhoun et al., 2010). These narratives and views are embedded in the spiritual and religious dimensions of society, literature, media, and folklore. For instance, people in North America may tell a story with the underlying theme of “everything happens for a reason.” In Somali culture, Islamic worldviews may shape the commonly shared narratives about how Somalis, especially women, handle hardship and transform it into positive change (Clarkson Freeman et al., 2013; Ferriss & Forrest-Bank, 2018).
Both proximal and distal influences interact with people’s cognition (Calhoun et al., 2010). Although rumination can be intrusive and depressogenic, positive rumination (e.g., reflective, deliberate, seeking meaning-making) can also occur as a result of the aftermath of traumatic events (Calhoun et al., 2010). The content of rumination in Somalis may focus on how their response to a highly stressful event might affect others due to their collectivistic worldview. In addition, societal views on linear perceptions of events prevail in North America, whereas Somali traditional culture may emphasize holistic health beliefs and nonlinear explanations of the events (Clarkson Freeman et al., 2013; Pavlish et al., 2010; Wolf et al., 2016).
Self-disclosure is another area shaped by proximal and distal cultural influences (Calhoun et al., 2010). Social messages and responses from the reference groups influence the individual’s understanding of the desirability of disclosing personal information, which may also be differently shaped depending on the individual’s gender role and social status in the community (Calhoun et al., 2010). Self-disclosure can also be inhibited by the absence of Somali role models who promote it. Research shows that Somali women may avoid self-disclosure because it may be perceived as disruptive to the harmony of the group. Avoiding self-disclosure, however, can result in silent worries (Pavlish et al., 2010). Distal cultural influence that promotes emotional processing may play a positive role in Somali refugee women’s self-disclosure of their emotions related to traumas. For instance, when there are community traumas, emotions about the event may be publicly expressed through rituals, memorials, or mass media. Individual traumas can also be publicly shared via media, stories, expressive arts, or songs (Kashyap & Hussain, 2018).
Authors’ Reflexivity, Axiology, and Methodology
Although both theoretical and cultural perspectives are helpful in understanding Somali refugee women’s posttraumatic growth, a Somali-centered coherent healing narrative has not been established. Therefore, the present study takes a novel and integrative approach to answer its research questions. The authors of the study share their knowledge cocreating process by discussing their (a) reflexivity as coresearchers (people and relationships), (b) axiology (beliefs, values, and frameworks that guide processes), and (c) methodology (procedures to gather and make sense of data).
Reflexivity
The first author, Musse, is a Somali Muslim woman in Lewiston, Maine, USA, and a mother of five children. She is in her early forties, and she was displaced from Somalia in 1988 and lived in Ethiopia until 1995. She has lived in the United States about 30 years. She had the privilege of living a life without disability until 2022. She is now a person with a disability who uses a wheelchair. A shooting spree during her 2022 visit to her family in Ethiopia resulted in the loss of one of her legs and the death of her younger sister. Close to the 1-year anniversary of the tragedy, Lewiston faced its own mass tragic shooting, where both authors reside. These losses and tragedies compelled her to support collective healing within the local community, including her Somali brothers and sisters, and within the broader communities where healing stories remain untold.
As a highly regarded community leader, Mussee supports refugees and immigrants’ resettlement and community integration. She also promotes community-orientation and advocates for healthy living for all. Over the past two decades, she has worked as a cultural broker, interpreter, community organizer, and advocate for refugees and immigrants. As a cultural moderator, she has prior experience facilitating interviews on posttraumatic growth among Somali refugee women. For the present study, she embraced her Somali cultural tradition and bilingual strengths; therefore, she used oral English mixing Somali language, incorporating translations to repeatedly share her perspectives of healing and growth after trauma. These perspectives are integrative and draw from her own experiences going to psychotherapy for years and the stories of the Somali women she has worked with.
Musse invited the second author, Garrison, to cowrite the 5Rs posttraumatic growth model. Garrison is a Korean woman and a non-Black, non-Muslim immigrant of color in Lewiston, Maine, USA. She is in her early forties and she has lived in the United States over a decade. She was trained as a counseling psychologist and she works as a junior psychology professor teaching courses at a small liberal arts college, including community-based research methods. She has developed a relationship with Maine Community Integration over the past 4 years. She participated in several extant Somali-led programs, such as the parent leadership program, the youth program, and collective grief space that primarily serve Somali refugee women and their children.
Accepting an invitation to coauthor a psychological theory while witnessing the aftermath of a shooting that resulted in Musse's loss of a leg and her sister, brought back memories of her late older brother, a person with intellectual disability and Down syndrome. He had once invited her to write about his story following his passing. These reflections serve as a moral and humanistic foundation for her to deeply explore the meaning of cowriting and sharing untold stories. Therefore, as a witness, listener, and cowriter, she approached this research with a commitment to honoring the legacies of both the Musse’s sister and her own older brother—striving to help create a society that is more inclusive and compassionate toward marginalized individuals and communities. She engaged in iterative deep reflection using the following prompts: “What does it mean to be an intimate cowriter?” “What do I hear from Somali refugee women’s voices?” “What do I see in their faces?” “What historical memories emerge in their stories?” “What could collective healing look like for them?” “What do I feel in my body as their stories moved through our shared time and space?” She kept reflexivity notes and photo journals throughout the project and shared her reflections with Musse and diverse community audiences.
Axiology
The authors’ beliefs, reflections, and decision-making were underpinned by pragmatic, social constructivist, and critical paradigms. For the pragmatic aspect, the authors asked, “What does our Somali refugee community already know, and how will this knowledge benefit the community?” This paradigm supported the authors in producing both an academic paper and visual artwork, as visual work is a translingual and accessible form of knowledge to communities, particularly Somali refugee women. For the social constructive aspect, the authors engaged in lengthy dialogues to describe posttraumatic growth, using storytelling in different spaces with different audiences, reflecting, and checking on shared understanding in an iterative manner. For the critical paradigm aspect, the authors discussed whose knowledge is represented in the psychology and societal discourse and made efforts to center Somali epistemology.
The authors of the study conceptualized coresearching and cowriting as a process involving a series of mutual decisions grounded in shared values. Therefore, the authors’ overall approaches and specific decision-making were guided by decolonizing psychological science. According to decolonizing psychological science (Neville et al., 2024), psychological science is relational science with five foundational domains. The first domain facilitates human and community relationships; therefore, the authors developed a relationship through authentic dialogue, deep listening, and mutual learning, each influencing the other’s academic or community contexts. The second domain promotes critical ethical consciousness, which informed the priority of the community’s epistemology and shared authorship. The third domain pertains to generating reciprocal knowledge while making knowledge accessible to the communities. The fourth domain adopts engaged pedagogies involving the Global Majority (people of African, Asian, Latin, and Arab desent who together make up the vast majority of the world, challenging the idea that whiteness is the global norm; Lee et al., 2023). For instance, Musse's (the first author’s) in-person storytelling was incorporated into Garrison's (the second author’s) college psychology classroom over several years. Lastly, the fifth domain increases structural equity, which enabled the authors to name the epistemic exclusion of the Global Majority and ultimately centered Somali refugee women’s perspectives.
Methodology
Collaborative autoethnography integrates collaboration, autobiography, and ethnography. This method is participatory and relational as research processes involve empathic listening, working together, compassionately bearing witness to their own, and others’ experiences (Ellis & Rawicki, 2013). Both authors of the study are researcher-participants and the study was approved by the second author’s academic institution. This methodology was chosen because it aligns with their reflexivity and axiology. Specifically, the methodology is relational, reflective, and collaborative which is consistent with Paris and Winn’s (2013) emphasis on processes that seek to humanize research to all parties toward becoming more fully human. It emphasizes the authors’ role and transformation of becoming “a friend who understands fully” (Paris & Winn, 2013, p. xiii). As such, the chosen methodology created room for stories, feedback, reflexivity, creativity, and emotions.
From Ideas to Oral Story
As a community leader empowering refugee and immigrant women, the first author (Musse) wanted to design concepts to support Somali refugee women and girls, and offer healing narratives that understand and empower them. She has designed numerous community programs rooted in the philosophy of isku-filan (strong girl) to educate and empower refugee and immigrant women and girls to be confident in themselves, work together, and make positive changes in their communities. As an active community educator and leader, she attended numerous trainings, including Psychological First Aid training, a 10-month-long cultural brokering program to support therapists in providing culturally and logistically appropriate services, and trauma-informed care training. She also spent 6 years working directly with Somali clients in therapy settings across private practice, hospitals, and nonprofit organizations. Drawing from her lived experiences and observations of other Somali women, she spent eight years formulating concepts related to 5Rs, a process that unfolded in a nonlinear manner. Several community trainings, including an emergency and triage system using 5Rs (rescue, recovery, reentry, reconstruction, and rehabilitation) inspired her; she decided to use the 5Rs system to organize her ideas, which yielded: running, resettlement, residual stagnation, reconciliation, and resolution.
Musse developed the first theoretical component, Running, by observing the feet of refugees and contemplated where those feet have been. Her extensive experiences in organizing resources, such as basic needs and healthcare interpretation services, gave her insight on the second stage of Resettlement. She conceptualized the third component, Residual Stagnation, after being inspired by community lead control education, especially the term “residue” of lead paint. Her deep reflection on the term helped her connect how some psychological experiences are like “residue.” She coined the term “Residual Stagnation.” The fourth concept of Reconciliation was inspired by training in recognizing the ongoing nature of trauma and collective healing among Indigenous people. Her own self-reflection also helped her conceptualize the process of reintegrating old and new aspects of the self. The concept of Resolution was inspired by training on women’s empowerment, identity, autonomy, and humanistic psychology concept of self-actualization. As a community leader empowering refugee women and girls, she envisioned these concepts specifically to impact Somali refugee women and girls who may not have been exposed to healing narratives that include their community experiences.
From Oral Story to Written Story
The first author (Musse) shared her stories orally between October 2020 and October 2024 across various naturalistic spaces in the presence of the second author (Garrison). The first storytelling was a one-on-one dialogue with Garrison in Musse's community work space in October 2020. During that time, Musse also invited Garrison to visit various community spaces, such as a Somali grocery store, garment store, and Farmer’s Market, where they interacted with local Somali residents. Since October 2020, Garrison has attended various community gatherings organized by Musse. Musse shared her elaborated stories about the 5Rs in multiple spaces, including a community gathering setting, college classrooms, additional one-on-one dialogues with Garrison, and even her recovery from a critical injury following amputation. Musse's storytelling was uninterrupted, which lasted 20–30 minutes each time. Based on mutual consent, Garrison audio-recorded her stories, transcribed and repeatedly listened to them, discussed what her stories conveyed and evoked, explored emotional, cognitive, and behavioral aspects of each phase, and wrote a written description of her stories. The process of developing the model was also explored and audio-recorded. Musse validated the written pieces.
From Written Story to Visual Story
After completing the writing, the authors invited a public artist to visualize the concepts, making the written concepts on the paper more accessible to Somali refugee women. Visual arts can capture their attention, evoke emotions, and communicate without the need for language. The artist is a woman of color who teaches at a local public elementary school. Four meetings were held to transform written words to visual images. During the first meeting, the authors discussed the mission for the research, vision for visualization, meaning of color, and use of fabric. For instance, they decided to include the image of Baati (i.e., Somali long dress) and use fabric for parts of the art pieces. The fabrics came from Garrison's personal collection of ethnic belongings, passed down from her grandmother—who also endured colonial and war trauma—to represent a collaborative relationship between the author and the resilience of women across generations and continents. During the second meeting, Garrison reviewed the initial sketch and shared the progress with Musse. During the third meeting, all of them reviewed the finished art pieces, shared emotional reactions, and narrated written stories juxtaposed with each artwork. During the final meeting, a revision was made to one of the art pieces to add more fabric for consistency across the art pieces. The artist was compensated for her work through a commission.
Ka Bogso: The 5Rs Posttraumatic Growth Model
This section describes the synthesis of Musse's (the first author’s) oral narratives and Garrison's (the second author’s) 4-year-long reflections and dialogues with her, articulating the 5Rs posttraumatic growth model. The model is grounded in the Somali concept of ka bogso, or being healed from adverse life experiences toward feeling wholesome psychologically. The model is intended to support a child, adolescent, or adult of Somali descent in the United States who seeks to make sense of their experiences in parts of the African continent as well as ongoing encounters with oppressive structures in the United States. The model was also developed to guide psychologists and allied health professionals to effectively work with Somali refugee girls and women to address the accumulated long-term effects of traumatic experiences, including childhood trauma, gendered violence, forced displacement, discrimination, and losses on their psychological, spiritual, and social well-being. The 5Rs posttraumatic growth model comprises five phases: (a) Running, (b) Resettlement, (c) Residual Stagnation, (d) Reconciliation, and (e) Resolution. Each phase is presented with a written description and visual art representing each phase. Larger versions of the visuals are included in the Supplemental Material.
Phase I: Running
The Running phase is represented by “fleeing feet” as a Somali girl runs from violence and war, for survival during chaos. The girl can be literal but also symbolic, representing a Somali woman’s memory of their younger self, highlighting the long-standing impact of the trauma over time. This phase also signifies a child with bare feet whose sense of being is threatened. In the Running phase, a Somali girl may not comprehend the necessity of fleeing when they face catastrophic events such as wars, which occur in sudden, abrupt, and unexplained ways. She may be uprooted forcefully from a community and flee the country. Running also encompasses psychological experiences of confronting gendered and domestic violence (e.g., gudnin, faro-xumeyn), including the desire to escape from unwanted or traumatic encounters.
Emotionally, a Somali girl may feel anxious about threats, chaos and instability, fear and terror, and a heightened need for survival during this phase. Her attention may shift away from her internal feelings. Cognitively, this phase is marked by a limited comprehension of catastrophes, accompanied by confusion, uncertainty, worries, and intense focus on signs of threat and danger. Behaviorally, this phase involves escaping, rapid movement, freezing, hiding, maintaining silence, and constant problem-solving.
The image entitled “Phase I: Running” (Figure 1) represents the Running phase, emphasizing fleeing with bare feet and motion. The visual art shows how the running implies the constant real and perceived experiences of danger and chaos. The girl wearing a humble Somali Baati is running, seeking refuge and safety, symbolized by small squares that visually represent pieces of hope. The trees represent a strong sense of self and a heightened will to live against all odds. The visual depiction of 5Rs posttraumatic growth: Phase I: Running
Phase II: Resettlement
The Resettlement phase represents “living in a tent” in a country other than Somalia. This phase symbolizes temporary shelter, displacement from home and communities, limited resources, and the instability of life. Resettlement includes memories of staying in refugee camps in neighboring countries, such as Kenya, Ethiopia, and Djibouti, where Somali girls and women often experience additional losses, sexual violence, mistreatment, and malnourishment. The feeling of living in a tent may also be present in the memories of attempting to settle in a third country, such as the United States, where they receive temporary assistance with housing, food, language learning, and services for basic needs. During this phase, the individual comes to the realization that their status has dramatically shifted from an ordinary person living in Somalia to a “refugee.”
A Somali woman’s emotions during this phase include a sense of temporary relief, nervousness, uneasiness, isolation and worry, which are simultaneously accompanied by a realization of consequential disruptions as well as loss of community, family, and life. Both murug (i.e., profound sadness, grief) and qaracan (i.e., mental shock, agitation) arise in her consciousness. Cognitive experiences are marked by intrusive thoughts, flashbacks, rumination, memory control or impairment, mental fog, thought suppression, difficulties concentrating, and negative beliefs about oneself, such as self-blame and guilt. Behaviors associated with the phase include avoidance, daydreaming, constrained responses to people and the environment, hypervigilance about potential threats, social withdrawal, and suspicion of others.
The image entitled “Phase II: Resettlement” (Figure 2) shows multiple tents which depict temporary shelter and symbolizes a transient life situation with limited resources. The humble clothing signifies few to no necessities. The barren and thin trees symbolize a diminished and weakened sense of self during this phase. Pieces of hope symbolized as little squares may not be visible to them, yet they exist and grow. A Somali woman feels hope beneath her feet and painted across the sky; these depictions reflect her appreciation of being alive and her interconnectedness to nature and spirituality. The visual depiction of 5Rs posttraumatic growth: Phase II: Resettlement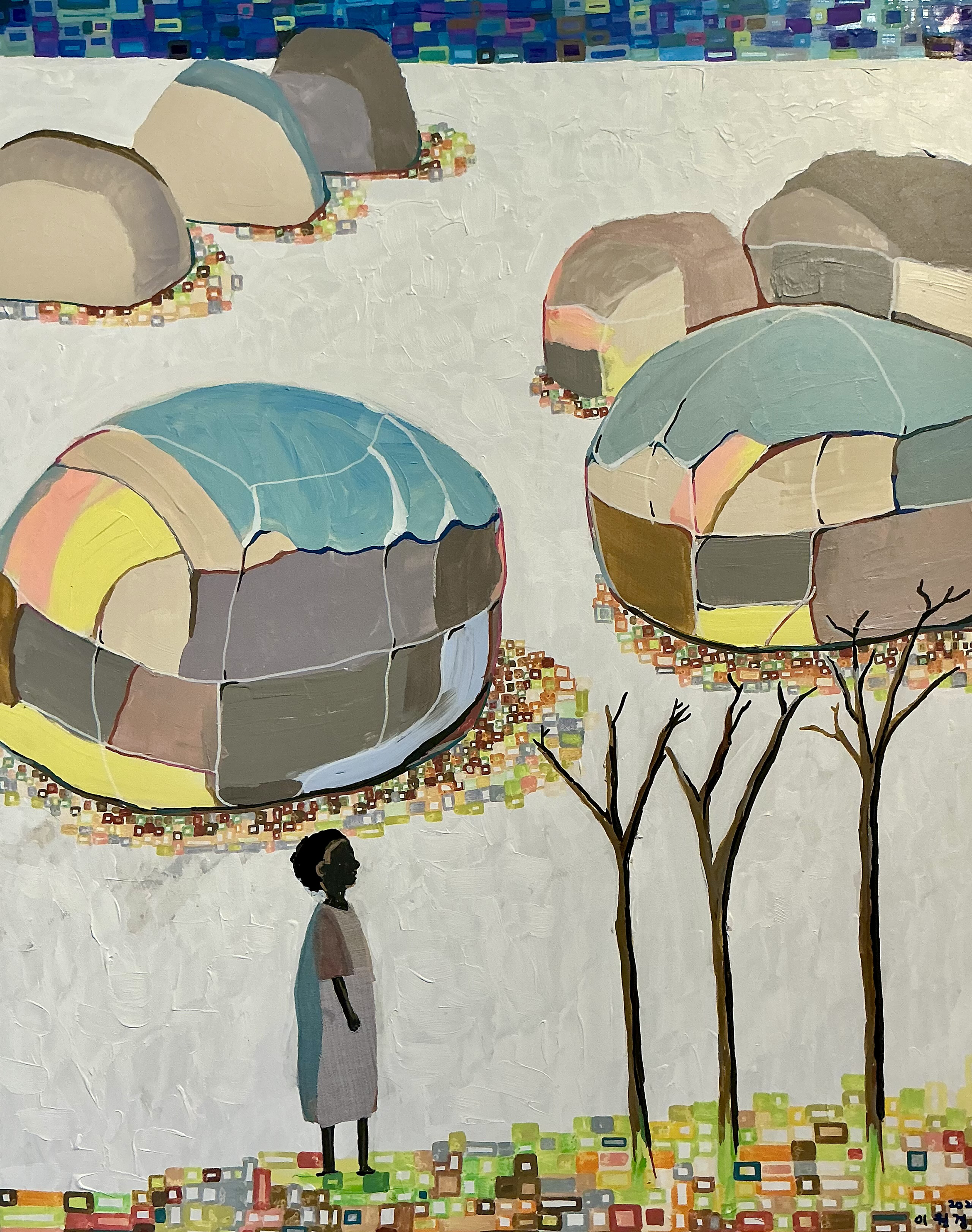
Phase III: Residual Stagnation
The Residual Stagnation phase entails prolonged psychological pain despite the fulfillment of basic physiological and safety needs. A Somali woman may say to herself or others that having a roof over her head and a place to lie down should be enough compared to what she went through during migration and resettlement. She also compares herself to others. For instance, other Somali women may say, “Every Somali woman went through trauma, but no one talks about it.” The stigma around mental health among Somali communities makes them mask their struggle, such as smiling or acting as if they are okay. Such messages hinder the collective well-being and perpetuate judgment and lack of empathy. Over time, murug grows inside of a Somali woman and she feels a shattered sense of self. In her public and social sphere, she appears unaffected by murug; however, in her internal world, she feels extreme emotional pain. External pressure from both U.S. society and the Somali community is present. Messages like “You should get over it” are hard to hear at her worst, and darkest times. The message about pushing oneself to achieve self-actualization at her darkest time exacerbates emotional pain. The contradiction between being told to feel whole and feeling broken inside is hard to explain to others. One may say, “I don’t know how you feel whole when you feel broken.”
Emotionally, a Somali woman may experience prolonged sadness, helplessness, melancholy, anger, and fluctuation in their mood. Feelings of brokenness, alienation, disconnection from oneself and others, suffocation, and despair may also arise. The cognitive aspects of this phase include viewing the self as fragmented, unstable, and defective. A pessimistic and cynical future outlook emerges; such an outlook may evoke dissonance from her spiritual beliefs about how one should handle hardship. Behaviorally, she may exhibit hyperactivity, restlessness, lethargy, and impulsivity, such as going on shopping sprees, emotional eating, angry outbursts, self-destructive actions, or engaging in risky behaviors like substance abuse. It is possible to show none of these behaviors while suppressing emotions and avoiding interpersonal closeness. Nevertheless, she may continuously take care of her family, serve the community, and pray.
The image entitled “Phase III: Residual Stagnation” (Figure 3) is the image of shattered pieces in a crouched body portrayed in dark shades of color. The shattered self is precariously supported by a frail tree. Although hopes are indiscernible, a Somali woman continues living while having faith in life. The squares of hope spread even in darkness, surrounding the tree and beneath and above the self. The visual depiction of 5Rs posttraumatic growth: Phase II: Residual Stagnation
Phase IV: Reconciliation
The Reconciliation phase represents the reintegration of life experiences and perspectives, yielding a holistic understanding of Somali refugee women as seekers of healing and growth. Somali women grieve the parts of their lives, constantly dealing with the adverse impact of chronic exposure to war, violence, and mistreatment by others. They reclaim ways to live, including community orientation and gratitude; empowering other women and fostering a strong sense of sisterhood; a positive attitude toward the self, others, and the world; and forgiveness and patience. This phase entails relearning how to walk on the ground gently and humbly, in contrast to the frantic running with fleeing feet described in Phase I. They recognize how they have been living in survival mode since childhood and reconnect their feet to the ground with an increased sense of ecological and spiritual connection. For instance, messages such as “God doesn’t burden any soul with more than it can bear” give them resilience and hope. They also reconcile their wounded and renewed parts as well as old and new worldviews in their social contexts that have drastically changed. The reconciliation is facilitated by spiritual self-reflection. With acceptance, support, and empathy from others, they feel permission to express and share their murug.
Emotions in this phase are characterized by feelings of compassion, connectedness, care, acceptance, trust, and commitment to living fully. There is also a growing sense of joy, wonder, and hope. Cognitively, they reorient, reclaim, or renew their values with a flexible and positive cognitive reappraisal of significant life events and everyday experiences. Behavioral aspects of the phase involve purposeful behaviors that contribute to the well-being of their family, neighbors, and communities, while aimless and impulsive behaviors decrease. They engage in behaviors such as practicing gratitude, walking in nature, nurturing people, animals, and nature, learning new skills, enhancing life skills and leadership, and participating in community activities.
The image entitled “Phase IV: Reconciliation” (Figure 4) visualizes the Reconciliation phase, integrating women’s memories, experiences, and identities into their sense of wholeness. The girl who carries painful life memories is wearing humble clothes, and she is used to running all the time. She is embraced by an adult woman in vivid Baati who offers the girl compassion, protection, and love. The young girl also reaches the adult woman, symbolizing no longer trying to disconnect from herself and suppress her emotions. They look at the same tree that represents wholeness and growth. Their sight is filled with colorful squares and circles, each representing a piece of hope. The visual depiction of 5Rs posttraumatic growth: Phase IV: Reconciliation
Phase V: Resolution
The Resolution phase is marked by honoring the legacy of loved ones, family, neighbors, and friends who died due to traumatic events and setting meaningful goals to improve the lives of others and communities. The phase is not a final destination on a linear path; instead, resolution involves being a seeker of lifelong healing, which enables women’s experiences to be a process. Room for feeling, sharing, and releasing murug allows them to better remember their loved ones’ courage, wisdom, and love, honoring their memory and the impact they left behind. Examples include building and operating a shelter for unhoused youth and training other Somali women and families to address anti-Black racism, gender-based violence, gun violence, mental health stigmas, and substance use issues. Community cohesion, a core Somali cultural value, is put into action, such as supporting other refugees and immigrants in connecting with each other and institutions in local society, such as schools, hospitals, employment services, and banks. The resolution phase is also marked by increased civic engagement and participation in local and large-scale advocacy for creating a safe and healthy environment for their neighbors. During this phase, Somali refugee women recognize and appreciate humanity, saying that “We all struggle,” including people in influential positions, such as parents or leaders.
Emotionally, this phase is characterized by feeling wholesome: feelings of love, joy, courage, compassion for the self and others, gratitude, resilience, empowerment, motivation, and fulfillment. Difficult emotions, such as murug, are no longer avoided, suppressed, or hidden. Somali women open up their vulnerable emotions within safe relationships, such as with close friends, trusted neighbors, community leaders, or mental health professionals. Cognitively, this phase is characterized by a restored or enhanced mental focus on creating positive changes and engaging in problem-solving. The Somali women can return to their values and goals even if distractibility or mental fog continues. Behavioral aspects of this phase are characterized as conscious actions in partaking in meaningful self-reflective, contemplative, and spiritual activities. Meaningful social behaviors increase, such as listening to others, caring for others who may struggle, addressing community issues collectively, and sharing stories, food, and time with others.
The image “Phase V: Resolution” (Figure 5) is the final visual depiction of the 5Rs posttraumatic growth model through the journey of ka bogso—being healed and feeling wholesome. The Somali refugee woman’s hands are together, and her baati is collaged with emerald green fabric, expressing the sentiment of resolution; it also symbolizes her deceased family member who used to hold her hands in life and wear the emerald green baati. The red background was chosen as red symbolizes healing in Somali culture. With its colorful and varied shapes of hope, the tree depicted in the previous four phases becomes whole and lush in the final phase, symbolizing posttraumatic growth. The visual depiction of 5Rs posttraumatic growth: Phase V: Resolution
Discussion
This research conceptualizes and visualizes the 5Rs posttraumatic growth model applicable to Somali refugee women. The model shows a journey of ka bogso, meaning being healed and feeling wholesome, outlined by five Rs, representing Running, Resettlement, Residual Stagnation, Reconciliation, and Resolution.
The Running phase of our model may be connected to the traditional trauma concept of flight or fight mode (Barkil-Oteo et al., 2018); it involves either the actual activation of the sympathetic nervous system or the recollection of an intense state of fear and terror. The language of running literally and figuratively better represents the Somali refugee women’s premigration trauma in that organized violence was not something they imagined fighting against. Ferriss and Forrest-Bank (2018) reported Somali refugee women’s experience, stating, “[E]ven after resettlement, they still feel like they may need to run” (p. 637). The feeling of being on the run was likely an actual experience among Somali refugee women, which may make it easier for them to relate to and communicate with each other. Additionally, running represented a form of agency for Somali refugee women, contrasted with the violence, loss, death, and chaos that was beyond their control, which is connected to the development of murug. From a trauma-informed perspective, using an accessible and nontriggering symbol like running and fleeing feet may be more effective than recounting the details of traumatic events (Robertson et al., 2019).
The characteristics of the second phase, Resettlement, are aligned with the existing literature on Somalis’ experiences in refugee camps with extremely poor quality of life and their mental state (Horst, 2006; Im et al., 2017). Horst (2006) articulated the concept of buufis, a Somali concept of longing for resettlement in need of peace and security. Im and colleagues (2017) found that from Somalis’ perspectives, buufis is directly related to a lack of livelihood, education, and opportunity, as well as poverty, a direct result of forced displacement and resettlement in a new country. Our model captures the sentiment of longing for a better quality of life, which continued from the refugee camps throughout their time in the United States.
The third phase, Residual Stagnation, may be the missing puzzle piece in the literature on Somali refugee women’s posttraumatic growth. A qualitative study on refugees’ posttraumatic growth (Hirad et al., 2023) shared that most refugee participants perceived resettlement as relatively less challenging than the immediate threat to life in their home country they had already overcome. Although this type of comparative attention may be a common cognitive coping strategy related to posttraumatic growth (Filipp, 1999), such a comparison may not resolve the immense and deep emotional pain and isolation among Somali refugee women who still have difficulties with moving forward. This difficult time is important to acknowledge as Somali refugee women face numerous gendered and racialized challenges in the United States. Some Somali refugee women feel frustration about not being able to carry out social and community responsibilities due to oppression and struggles with housing, employment, and parenting issues (McMichael & Manderson, 2004). Indeed, studies show evidence suggesting the high comorbidity of depression and posttraumatic growth (Kroll et al., 2011), ongoing struggles with murug (Carroll, 2004; Im et al., 2017), and stories that include narratives of not only moving forward but also stagnating among Somali refugees (Syed et al., 2022). Posttraumatic growth researchers (e.g., Calhoun & Tedeschi, 2006) also recognize that pretrauma characteristics (distal factors) and enduring stress within the person and environment (proximal factors) play a role in moving forward.
Our model makes such nuance explicit and normalized: the residual stagnation concept demonstrates a nonlinear healing process. Residual may capture murug, the prolonged and persistent emotional pain, and stagnation captures the frustration stemming from both proximal and distal cultural influence, which may shape unrealistic expectations about the pace of healing. Although posttraumatic growth research tends to minimally discuss the darkest times, our model embraces and validates stagnation as an essential part of the posttraumatic growth process.
The fourth phase, Reconciliation, is congruent with Ferriss and Forrest-Bank’s (2018) findings that Somali refugees experience improved self-awareness, compassion, warmth, and acceptance and reconstructed meaning of life associated with appreciation and gratitude. The phase is also aligned with the overall refugees’ posttraumatic growth process (Hirad et al., 2023). Both old and new worldviews shaped by religious, cultural, political, and geographic contexts are integrated, and contradictions within them and internal and relational conflicts are reconciled. Consistent with the importance of social support and positive religious coping for Somalis’ posttraumatic growth (Kroo & Nagy, 2011), our model underscores how support, empathy, and deep listening play a role in Somali refugee women’s reconciliation. It is plausible that Somali women read the Quran throughout all phases of posttraumatic growth as the holy text for living their daily lives and medicine dealing with health concerns (Clarkson Freeman et al., 2013). During the reconciliation phase in particular, Somali women may feel its curative role.
The final phase, Resolution, is consistent with the literature on overall posttraumatic growth, highlighting hopes, new visions, and possibilities for their life (Calhoun & Tedeschi, 2006; Umer & Elliot, 2021). Distinctively unique from other research, our model acknowledges and incorporates the interconnectedness between the self and others, including memories of lost loved ones. Consistent with the research on Somali women’s self-identity and full participation in society (Gardner & El Bushra, 2004), Resolution includes fulfilling social responsibilities and taking actions to contribute to communities. Resolution is presented as the final phase, yet it is noteworthy that posttraumatic growth is an ongoing process of healing that promotes accepting and compassionate healing narratives. This process may create a positive feedback loop between Somali refugee women and their proximal and distal cultural influence. The contributing roles in family, community, and society are crucial in the Somali concept of living a good life, consistent with Islamic perspectives (Saritoprak & Abu-Raiya, 2023).
Limitation
Our model is based on a single perspective informed by the first author’s firsthand experiences and her extensive experiences working with Somali refugee women. Therefore, we acknowledge that there may be multiple and alternative explanations for the posttraumatic growth among Somali refugee women. Somali refugees have various premigration experiences differently shaped by their social status, wealth, lifestyle (e.g., pastoralist), education and literacy, and region. Ethnopolitical tensions among people from Somalia are complicated; therefore, the interpretation of our model requires cultural sensitivity with minority ethnic groups, such as Somali Bantu refugees. Although we strive to describe the model in a symbolic yet concrete way, the model may not apply to all Somali refugee women. In addition, the interpretation of the visual arts is open, and evidence regarding the perception of and impact of the visual arts on Somali refugee women is not included in the research.
Implications for Theory, Practice, Advocacy, Education and Training, and Research
Theory
The 5Rs model is the first posttraumatic model developed by and for Somali perspectives. The model highlights the complexity of dealing with accumulated traumas, including displacement, violence, loss, societal oppression, and a sense of stagnation—a process often overlooked in existing posttraumatic growth research. Our model may complement existing conceptual tools developed for refugees, such as the psychological stages of the refugee process (i.e., early arrival, destabilization, exploration and restabilization, return to normal life, and decompensation; Gonsalves, 1992). While Gonsalves’s model emphasizes crisis response and skill acquisitions for survival and adaptation, our model can offer a holistic framework of healing and growth while emphasizing collective space for grief, reflection, support, and empowerment.
Practice
Our model can be more resonant with Somalis’ health beliefs than diagnostic or medicalized language about trauma symptoms and posttraumatic growth. Somali refugee women view health holistically and within the context of their daily lives (Pavlish et al., 2010; Wolf et al., 2016). Community leaders and faith leaders, such as Imam, can use our model to ask how Somali women engage in productive activities, relate to themselves, family, and faith, and how their communities watch their children and avoid violence. Community organizations working with Somali refugees can also normalize the nonlinear experiences with posttraumatic growth, especially residual stagnation, during which time some women may feel weary of self-disclosure. Community practice can prioritize sharing time and food together as a valued part of Somali women’s way of being. Community organizations can hold social events, gatherings, or allabari (collective prayer meetings) to honor their own journey of ka bogso and discuss their reflection on the 5Rs posttraumatic growth model. Such gatherings may play an important role in Somali women’s lives by providing space for interactions, the continuance of Somali culture, community life, hospitality, and spirituality (Koshen, 2007; McMichael & Manderson, 2004).
Clinicians in traditional health service settings can use the descriptions of our model and visual arts. For instance, clinicians may tell a short story about the 5Rs posttraumatic growth model and its experiential source of knowledge based on Somali refugee women’s experiences. The story may become a refreshing and relatable view of the client’s distal cultural influence, such as the story of someone from their culture related to posttraumatic growth (Calhoun et al., 2010; Makwarimba et al., 2013). Open exploration, such as inviting the client to identify one of the five images that resonate with their internal state or external circumstances, may also serve as a meaningful prompt for the client to share their experiences. Clinicians may encourage the client to share their cultural narratives of healing, how they make sense of symbols and images, and identify strengths within their communities. Our model can be complementary to various therapeutic interventions. For instance, clinicians can use the inner child metaphor to explore the reconciliation phase, and value-driven actions may also help support the client’s experiences with resolution.
Education and Training
Training for students and continuing education for psychologists may include didactic and reflective activities to discuss the strengths and values of Somali refugee women. Reflection questions may help them recognize deficit-oriented narratives and the roots of anti-Black, anti-Muslim, and anti-refugee biases. Moreover, training can be offered in collaboration with historians, interdisciplinary researchers, and documentarians to present various dimensions of the Somali refugee experiences locally, nationally, and globally. As psychologists increasingly suggest the importance of collaborating with community members in knowledge production and dissemination (e.g., Neville et al., 2024), academic institutions, pedagogy professionals, and instructors can create learning environments for students. Such a learning environment may encourage students to gain theoretical and experiential knowledge about building community partnerships and engaging in participatory knowledge-making with their local refugee-serving community organizations. Psychologists and Somali community leaders may offer collaborative training in community settings. For instance, the role of an Imam is predominantly held by men in the Somali community. Therefore, it is important to train Imams on Somali women’s healing and growth, with an understanding of the lifelong impacts of sexual and domestic violence and female genital mutation in addition to shared refugee trauma.
Advocacy
We outline two ideas that aim to advocate for the health of Somali refugee women, specifically promoting posttraumatic growth. First, psychologists and allied professionals, such as psychiatrists, social workers, and mental health counselors, can copresent with Somali refugee community leaders to discuss psychological issues and approaches to reduce the gap between clinical knowledge and communities’ priorities. These copresentations may occur in professional and academic conferences, undergraduate and graduate classes, and various academic and clinical institutions’ speaking series. Second, resources, training, and funding should be allocated to encourage and honor Somali oral traditions. For instance, Somali refugee women’s digital stories and oral histories can serve as tools for sharing knowledge about life and growth, increasing public awareness, and creating a sense of community.
Suggestions for Future Research
Our model could be explored further by conducting interviews with Somali refugee women on their perception of the model. Future research may include organizing a community gallery exhibit and discussion sessions about the model. Researchers could create digital oral stories to add an auditory experience in understanding the model. Similarly, disseminating brochures to Somali-serving organizations and social and health services and exploring the perceived effectiveness of using the model can be another future research direction. Although people may not have identical traumatic events, the model could be applicable to broader populations, such as nonrefugee trauma survivors or Somali refugee men. Validating the model by exploring people’s diverse experiences and identities may improve the utility of the model. The model is open to revision and iteration, and we encourage Somali refugee women’s full participation in theory development. Therefore, interviews may aid researchers in describing the subjective experiences among Somali refugee women.
Supplemental Material
Supplemental Material - Ka Bogso: The 5Rs Posttraumatic Growth Model for Somali Refugee Women
Supplemental Material for Ka Bogso: The 5Rs Posttraumatic Growth Model for Somali Refugee Women by Fowsia Musse, Yunkyoung L. Garrison in The Counseling Psychologist
Footnotes
Acknowledgments
The project was partially supported by the Bates College Faculty Development Fund and the Harward Center. We appreciate our collaboration with artist Won Kyoung Lee. We appreciate the meaningful and encouraging feedback provided by the reviewers and guest editors to improve the manuscript.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.