
Abstract
Suicide deaths are rising in the United States, with some evidence that they are rising most rapidly among men of color. However, men of color in emerging adulthood face unique barriers to accessing life-saving services, such as the 988 Suicide and Crisis Lifeline. In the present study, we examined factors that influence help-seeking for suicidal thoughts among undergraduate men of color with a reported history of suicidality. In this consensual qualitative research study, 20 undergraduate men of color responded to an anonymous open-ended questionnaire administered through an institutional research system. Our analysis yielded four domains (a) Intrapersonal Factors, (b) Systemic Factors, (c) Expectations of Using a Crisis Line, and (d) Expected Experience of Disclosure, that explained participants’ perceived barriers to, facilitators of, and potential experiences with crisis line utilization. Findings highlight the unique impacts of participants’ cultural beliefs, as well as the influence of traditional masculinity on help-seeking intentions.
Undergraduate men of color with histories of suicidal thoughts identified several facilitators to using a crisis line for suicidal thoughts, including having hope, experiencing relief, and receiving help. They also described barriers to crisis line use, such as self-reliance, sociocultural norms, uncertainty about crisis lines, and concerns about sharing their suicidal thoughts. These findings illustrate the need for mental health professionals to develop and promote culturally responsive crisis line services, as well as engage in efforts to destigmatize seeking help among undergraduate men of color.Significance of the Scholarship to the Public
Suicide rates have increased significantly among people of color (Centers for Disease Control and Prevention [CDC], 2022), who often receive inadequate care within U.S. healthcare systems (Kaiser Family, 2022). Compared to White people, who saw a 3.9% decline in age-adjusted 2021 suicide rates, American Indian or Alaska Natives had a 26% increase, Black or African Americans had a 19.2% increase, Hispanics had a 6.8% increase, and Asians had a 1.5% increase (Stone et al., 2023). Additionally, there are age and gender disparities in suicide deaths, with men dying by suicide at a roughly four times greater rate than women and suicide being the second-leading cause of death for college-aged individuals (CDC, 2024). These disparities are particularly pronounced among marginalized racial and ethnic groups (e.g., Garnett & Curtin, 2023; Stone et al., 2023). Therefore, there remains a need to address gaps in professional help-seeking among men of color (Villatoro et al., 2018), particularly given the limited literature that explores help-seeking intentions at the intersection of race and gender (Wong et al., 2014). Compounding this challenge, people of color are underrepresented broadly in psychological literature. For example, only 26.3% (n = 757) of articles published in four key counseling psychology journals from 2000 to 2019 focus on racial or ethnic minority groups (Hawkins et al., 2022). Therefore, additional inquiry is needed to understand help-seeking behavior among people of color who are at greater risk of suicide and to in turn better inform psychological practice about these individuals.
Given the disparities described above, one such gap in the psychological literature is help-seeking for suicide among college-aged men of color, for whom suicide is a leading cause of death (CDC, 2020). Historically, reports indicated that undergraduate students of color exhibited lower suicide risk relative than their White peers (e.g., Shadick et al., 2015), leading suicide research and subsequent prevention and intervention efforts to focus on White (e.g., Smith-Millman et al., 2022), female (e.g., Wolitzky-Taylor et al., 2020) or students from other marginalized groups (e.g., sexual minority students; Goodwill & Zhou, 2020; Shadick et al., 2015). This presents a barrier to counseling psychologists and other helping professionals working with college students, particularly given that psychologists are called to provide culturally responsive suicide prevention and intervention approaches, notably when serving communities of color (Wong et al., 2014). Another barrier to suicide prevention among college-aged men of color involves both mental health stigma and limited access to care, given that men of color are less likely to seek help than other groups (e.g., Huerta et al., 2021). Men of color who do seek help, including undergraduate students, may also experience harmful interactions with law enforcement (Harrell & Davis, 2020; Rengifo & Pater, 2017) and inappropriate pathologizing by clinicians (National Public Radio [NPR], 2023) when accessing suicide intervention. Therefore, one resource available to psychologists working to prevent suicide among college-aged men of color is crisis lines.
Crisis Line Services
To advance access to crisis services for all people, the American Psychological Association (APA) advocated for the development of the 988 Suicide and Crisis Lifeline as an upgrade from the former 10-digit National Suicide Prevention Lifeline (Weir, 2022), underscoring the relevance of crisis line services to psychological practice. Crisis line chat and text interventions have demonstrated efficacy in reducing distress and suicidality (Gould et al., 2021, 2022). Although help-seeking barriers persist for people of color, crisis lines such as the 988 Lifeline incorporate culturally responsive practices in their training and offer services tailored to various cultural groups, including specific racial and ethnic groups (988 Lifeline, n.d). Furthermore, given the history of harmful interactions between marginalized communities and law enforcement (Harrell & Davis, 2020; Rengifo & Pater, 2017), crisis lines can serve as a safer alternative or entry point for supporting men of color during mental health and suicidal crises. For example, although crisis lines may employ emergency services, less than 2% of calls to the 988 Lifeline have involved these services as of 2025, with counselors emphasizing alternative options, such as collaborating with callers on a safety plan (988 Lifeline, n.d).
Despite the potential benefits of crisis lines in supporting undergraduate men of color at risk of suicide, a recent poll found that public awareness of the 988 Lifeline is generally low (Kaiser Family, 2022), and there is evidence that this trend is true specifically among undergraduate students (Shaikh et al., 2024). Shaikh et al. (2024) found that undergraduate students generally expressed low intentions of using any type of crisis phone line when experiencing suicidal thoughts. Due to the low help-seeking via hotlines among undergraduates overall, and the higher suicide rates among undergraduate men of color, understanding how and when undergraduate men of color might access crisis support for suicidal thoughts is essential to informing psychological practice and intervention efforts for this population. This study therefore examined factors that might influence help-seeking intentions and behavior regarding crisis line use among undergraduate men of color.
Help-Seeking and Psychological Intervention for Suicide
Despite elevated suicide risk, people of color have historically received inadequate healthcare in the United States, resulting in underdiagnoses and misdocumentation of mental health issues and suicidal behavior (Ali et al., 2022). Among college students who reported thoughts of suicide, Downs and Eisenberg (2012) found that Black, Asian, and Latino students had lower rates of mental health service use as compared to their White peers. Evidence suggests that these structural barriers contribute to attitudinal resistance toward help-seeking among men of color. For example, among African American men, everyday racism, masculinity norms, and threats to one’s sense of control negatively influenced help-seeking for mental health (Powell et al., 2016). Among college men specifically, masculinity-related distress indirectly influenced psychological distress by reinforcing barriers to help-seeking, and this effect was stronger for men of color compared to White men (Berke et al., 2022). Race-related stress also negatively influenced help-seeking among college men of color (Berke et al., 2022). Further, Horwitz et al. (2020) found that, among college students at elevated risk of suicide, cisgender men endorsed privacy and stigma concerns (e.g., concerns about parental notification, fear of documentation in medical or academic records) as greater barriers to mental health services compared to cisgender women, who were less likely to view these concerns as significant barriers. Students of color identified cultural barriers to service use, such as cultural norms, stigma, and experiences with racism (Horwitz et al., 2020). Taken together, these findings illustrate that undergraduate men of color are less likely to engage with suicide prevention and intervention services, despite facing elevated risk compared to their peers.
Although scholars have documented reported barriers to mental health service use among students of color (e.g., Miranda et al., 2015), including those at elevated risk of suicide (e.g., Busby et al., 2021; Horwitz et al., 2020), research remains limited on the specific barriers that disproportionately affect students of color in accessing crisis services, such as the 988 Lifeline. Even further, limited research captures the cultural nuances that may influence the help-seeking pathway among undergraduate men of color, such as cultural values and beliefs related to suicidality, despite increasing rates of suicide deaths among this population (Stone et al., 2023). As the college student population becomes increasingly diverse (Kim et al., 2024), it is therefore essential for psychologists to consider these challenges and tailor suicide intervention and prevention efforts to meet the needs of students of color to ensure equitable access to life-saving support. Counseling psychologists in particular have been called upon to adopt culturally relevant suicide preventive interventions for communities of color, especially at the intersection of race and gender (Wong et al., 2014). To meet this need, we, therefore, sought to understand the factors that influence help-seeking from a crisis line for suicidal thoughts among undergraduate men of color with reported histories of suicidal concerns.
Method
We utilized consensual qualitative research (CQR; Hill et al., 2005), an inductive, exploratory approach designed to elicit participants’ internal experiences and perspectives (Hill, 2015) for analysis. CQR emphasizes multiple accuracy checks and consensus among trained research team members, making it a particularly rigorous qualitative approach (Hill et al., 2005). CQR involves the development of superordinate themes, or domains, and associated categories and subcategories (Hill et al., 2005).
Participants
Participant Demographics
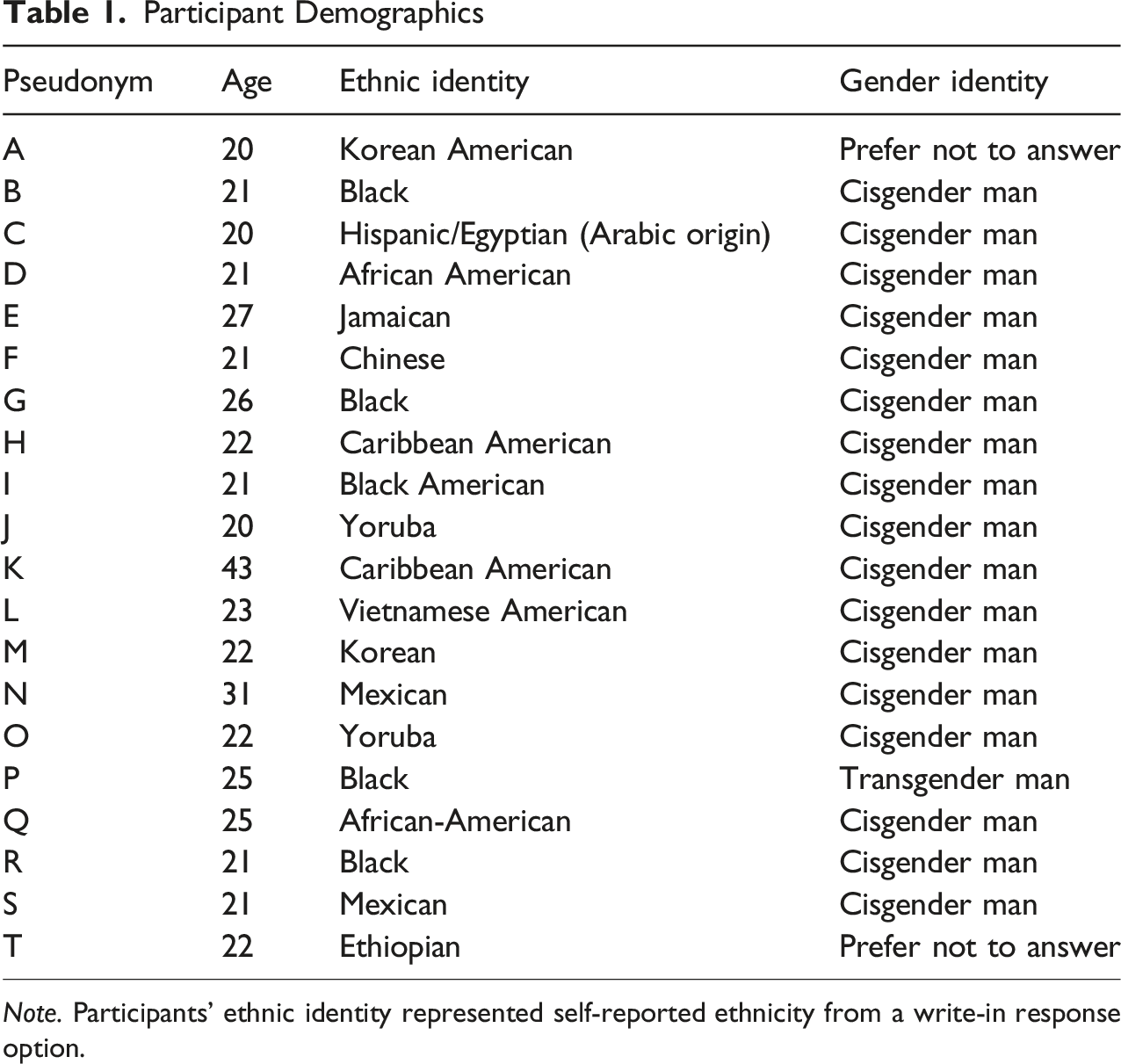
Note. Participants’ ethnic identity represented self-reported ethnicity from a write-in response option.
Procedure
Following institutional review board approval, we recruited undergraduate students from a Southeastern urban university using the institutional research system. Participants were compensated with class credit for completing the questionnaire and were provided with contact information for crisis services. Data were collected between September and October 2023 using an asynchronous Qualtrics open-ended questionnaire to preserve anonymity given the sensitive nature of the information (e.g., Bouchard, 2016; Braun et al., 2021). Additional benefits to our selected approach included: a broad scope to investigate relatively understudied phenomena (Braun et al., 2021); better inclusion of marginalized groups (Braun et al., 2021); enhanced participant comfort due to the anonymity it offers (Bouchard, 2016; Braun et al., 2021); and evidence suggesting it enhances accurate reporting of mental health symptomology (Fear et al., 2012). The method’s inclusivity may extend beyond men of color to benefit other marginalized groups, such as neurodivergent individuals who may have better access to participation in this format. To access the SONA Systems and participate in the study, participants had to be enrolled students at the university. Alongside providing inclusion criteria in the informed consent document, we included screening questions to ensure that respondents belonged to the population identified. Additionally, we did not exclude participants who had not experienced thoughts of suicide from completing the questionnaire, therefore improving accuracy of self-reporting by ensuring that respondents did not have to endorce suicide ideation to be eligible to participate and thus receive class credit. Respondents who did not endorse current or historical suicide ideation were not included in the present analysis.
Measure Development
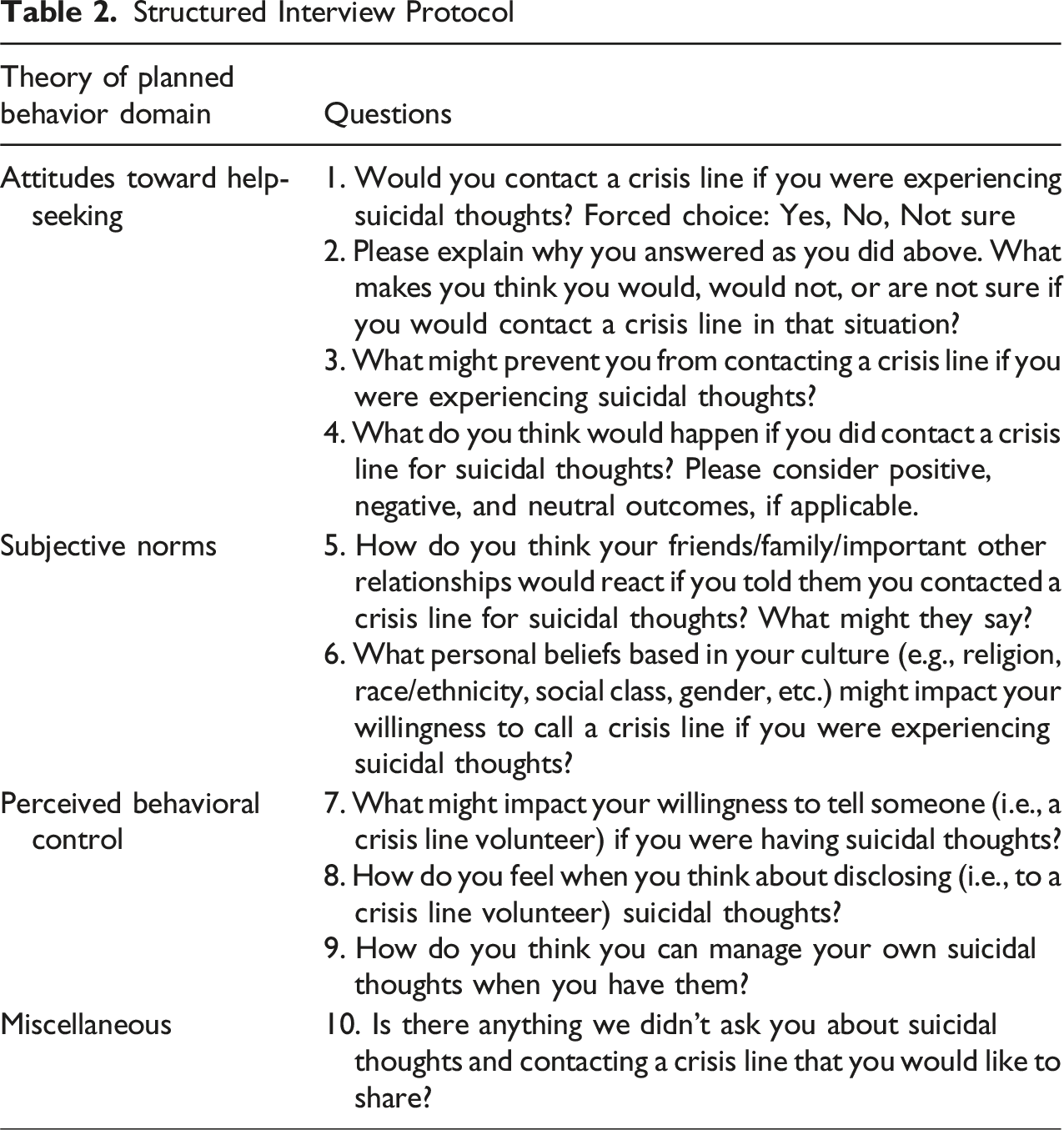
Participants provided demographic information by responding to a series of multiple-choice (e.g., selecting gender identity categories) and open-ended questions. The primary coding team and internal auditor collaboratively developed the structured qualitative online questionnaire using Ajzen’s (1991) theory of planned behavior (TPB), a psychological theory used to understand behavior that has historically been applied to help-seeking behaviors (e.g., Smith et al., 2008; Zorrilla et al., 2019), as a framework to conceptualize help-seeking from a crisis line among undergraduate men of color with current or past thoughts of suicide. Ajzen (1991; 2020) proposes that behavioral intentions are shaped by attitudes toward a specific behavior, an individual’s subjective norms related to that behavior, and their perceived behavioral control.
Ajzen (2020) defined attitudes toward behavior as an individual’s beliefs about performing a behavior and its outcomes, including attitudes toward help-seeking, crisis lines, and disclosure and managing suicidal thoughts in this study. Subjective norms consist of two types of normative beliefs: inductive and descriptive (Ajzen, 2020). Inductive beliefs reflect what a person expects from others, such as the approval or disapproval of behaviors like help-seeking, use of a crisis line, and disclosure and management of suicidal thoughts by friends and family. In contrast, descriptive beliefs focus on whether significant others engage in behaviors like help-seeking, using a crisis line, and disclosing and managing suicidal thoughts themselves. Finally, perceived behavioral control includes beliefs concerned with enabling or impeding factors (e.g., time, money, resources) for the execution of behaviors (Azjen, 2020), like help-seeking, use of a crisis line, and disclosing and managing suicidal thoughts. Moreover, Azjen (2020) noted that perceived behavioral control moderates the influence of attitude and subjective norms on behavioral intention, while actual behavioral control moderates the effect of intention on behavior. Therefore, according to the TPB, a person may be motivated to use a crisis line for suicide ideation when they have a favorable attitude and supportive subjective norms on help-seeking for suicide ideation (e.g., an important family member seeks help using a crisis line for their suicidal thoughts). However, only when perceived control over behavior (i.e., help-seeking for suicidal thoughts) is sufficiently strong will a concrete intention form.
Structured Interview Protocol
Data Analysis
We analyzed data using CQR, a team approach consisting of developing initial domains, creating core ideas within these domains to abstract the data, and constructing categories from the data using a cross-analysis (Hill, 2015; Hill et al., 2005). The research team consisted of a primary coding team (the first, second, and fourth authors), an internal auditor (the third author) who supported the development of the project, and an external auditor (the last author) who was not involved until the external audit to provide quality checks. Prior to conducting data analysis, the primary coding team and internal auditor met to discuss their biases and expectations of the data (Hill, 2015; Hill et al., 2005).
The primary coding team developed initial domains using the interview protocol as a starting list (Miles & Huberman, 1994), leading to three initial domains that corresponded to the TPB (i.e., Attitudes Toward Help-Seeking, Subjective Norms, and Perceived Behavioral Control; Ajzen, 1991). Participants’ verbatim responses to questions within each domain were data in the initial three domains. Next, the primary coding team members independently reviewed the data in each domain prior to consensus meetings, where we constructed core ideas within each domain collaboratively. All core ideas achieved full consensus and all coding occurred during consensus meetings. We used this coding method over independent coding because deeper discussion of the data can enhance the consensus process and improve the validity of data (Hill et al., 2005).
Domains, Categories, and Associated Definitions
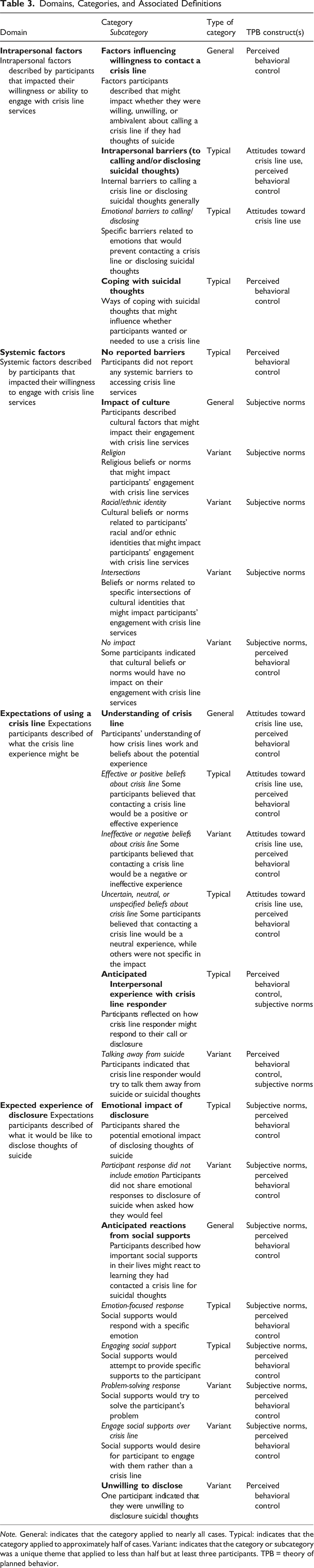
Note. General: indicates that the category applied to nearly all cases. Typical: indicates that the category applied to approximately half of cases. Variant: indicates that the category or subcategory was a unique theme that applied to less than half but at least three participants. TPB = theory of planned behavior.
Research Team Reflexivity
The research team consisted of two faculty members in counselor education and three doctoral candidates in counselor education at the time of data collection and analysis. Notably, one faculty member was a student at the same time as the doctoral candidates, and the other faculty member who served as an external auditor no longer held a supervisory role over any team members. His role as an external auditor was selected to reduce potential power influences over the coding and analysis experience. Two members of the research team identified as Black cisgender men, one as a Latino cisgender man, one as a biracial White and Asian cisgender woman, and one as a White cisgender woman. The primary coding team and internal auditor met to discuss biases and expectations prior to starting data analysis. Some of the resulting expectations of the data included that participants would encounter systemic barriers related to racism and patriarchy, potential past negative experiences accessing services, and that internal barriers such as self-reliance and mental health stigma might emerge. All team members noted that being mental health providers themselves might create blind spots related to participants’ experiences of mental health stigma. Additionally, all team members observed that they would not use a crisis line themselves, noting concerns about stigma associated with mental health providers needing access to support services.
The team also discussed our salient social and cultural identities and how these might influence our interpretation of the data. For example, we acknowledged that one’s own experience as a man of color might lead to projection onto participant experiences. Conversely, being a privileged member of an outsider group, such as a White woman, might inhibit full understanding of the nuanced experiences of racist bias described by participants trying to access services. We also raised concerns about potential misunderstandings of culture-specific language, particularly in the absence of opportunities for member checking. We additionally discussed strategies for addressing blind spots or misunderstandings among team members, including how to have direct conversations about the data, and revisited previous discussions in future team meetings to ensure that all team members could share concerns about data interpretation if needed.
Trustworthiness and Credibility
Alongside engaging in a priori discussions about our biases and expectations (Hill et al., 2005), we engaged additional strategies to enhance the trustworthiness, credibility, dependability, transformability, and confirmability of our findings (Ahmed, 2024; Lincoln & Guba, 1985). The primary coding team maintained individual reflexivity journals, and, at each stage of data analysis, we concluded with group reflexive discussions to identify our reactions to the data and how that might influence our analyses (Barry et al., 1999). For example, as data analysis progressed, religion and spirituality emerged as a salient factor. A group reflexivity discussion revealed that none of the primary coding team members were especially religious, and the discussion helped bracket assumptions about religion and suicide among team members. At each coding meeting, as well as each audit meeting, we explicitly explored our interpretation of the data, biases, and ways that our findings did or did not align with our initial expectations to better understand how our experiences shaped our results. For example, we expected to see gender emerge in the data as a more salient identity; however we observed that gender appeared to be more covertly related to masculinity or masculine expectations. Similarly, primary coders and the internal auditor expected to see more reluctance to engage a crisis line, and we found that our meeting discussions were biased at times toward the negative expectations expressed by some participants. During these discussions, we then worked to return to core ideas associated with willingness to engage a crisis line.
The internal and external auditor received notes about these discussions and access to individual reflexivity journals as part of the audit trail. The audit trail also included the organization and structure of the data at each step of the analysis, alongside written feedback from the audit, to ensure that auditors could track the progression of data analysis. The internal auditor provided written feedback about core ideas, domains, and categories, and attended two consensus meetings. As a result of the internal auditor’s feedback, the primary coding team recognized an over-emphasis on emotional language in our original coding of core ideas (e.g., coding a neutral response with an emotion label) and revised accordingly to better capture instances in which an emotion was not presented. The internal auditor’s feedback led to a significant revision of categories and subcategories. The external auditor’s feedback confirmed these changes and led to minimal revision of language during a consensus meeting.
Results
Our analysis yielded four domains: (a) Intrapersonal Factors, (b) Systemic Factors, (c) Expectations of Using a Crisis Line, and (d) Expected Experience of Disclosure. These domains and their associated categories and subcategories are summarized in Table 3, where they were also categorized as general, typical, or variant (see footnote; for more information, see Hill et al., 2005). Additionally, respondents indicated in the first question whether they would contact a crisis line for thoughts of suicide. The minority (i.e., 20%; n = 4) said that they would, whereas most respondents indicated that they would not (40%; n = 8) or were unsure (40%; n = 8) if they would contact a crisis line. Therefore, much of what we found emphasized barriers to engagement.
Domain 1: Intrapersonal Factors
The Intrapersonal Factors domain represented intrapersonal factors described by participants that impacted their willingness or ability to engage with crisis line services.
In the Factors Influencing Willingness to Contact a Crisis Line general category, participants highlighted specific factors or characteristics that might impact whether they were willing, unwilling, or ambivalent about calling a crisis line if they had thoughts of suicide. Factors that enhanced willingness included trust that crisis lines are helpful resources, a desire not to die by suicide, and hope that the situation may be resolved. The ability to connect anonymously with service providers also contributed: Participant G shared, “I would want somebody to talk to outside of my family. I wouldn’t want them to know my thoughts.” For others, talking to someone outside their existing support network made them unwilling to contact a crisis line. Participant K noted that, “I already have my spiritual leader who I go to.” Self-sufficiency led participants to be unwilling to contact a crisis line: Participant M stated, “I don’t want outside help.” Several participants felt that crisis lines were ineffective or would not “really change anything” (Participant O). Finally, some participants were unwilling to contact a crisis line because they did not believe they would follow through on their suicidal thoughts.
Alternatively, some participants were ambivalent about contacting a crisis line. Factors that contributed to this ambivalence included uncertainty about receiving help, having strong support systems, and preferences to deal with problems alone. Similarly, Participant C shared: “It depends a lot on my circumstances at the time and many other factors not easily explained. What would my headspace be? How would I go about it?”
Alongside these factors, participants also explored specific intrapersonal barriers to contacting crisis lines. Several participants shared personal beliefs that might block them from contacting a crisis line, including viewing crisis lines as “a last line of defense” (Participant C) and concerns that “someone may not show up or if they do they wouldn’t help me” (Participant B). Specific emotional experiences also emerged as intrapersonal barriers in the typical subcategory of Emotional Barriers to Calling a Crisis Line or Disclosing Suicidal Thoughts. The primary emotional barrier that emerged was fear of unpleasant outcomes, such as “judgment” (Participant T), “rejection” (Participant C), and of “being treated differently” (Participant K). “Pride” (Participant A and I) and feeling “shy” (Participant A) were also salient.
Many participants also referenced Coping with Suicidal Thoughts, a category within the Intrapersonal Factors domain, on their own. Participants named specific coping skills, such as “exercise” (Participant D and F), “talking to a friend” (Participant E), “being around loved ones” (Participant G), “distract myself through my academics” (Participant H), and “do something I enjoy” (Participant L), among others. Multiple participants highlighted engaging social supports, such as parents, members of their faith community, and friends, although typically not by disclosing their thoughts of suicide. Participant A, however, stated that he would “definitely talk with another about my thoughts. There is probably no way I will be able to handle suicide thoughts alone.” Participants appeared to feel that these coping strategies were effective and could prevent the need to engage with crisis line services.
Domain 2: Systemic Factors
The Systemic Factors domain included factors described by participants that impacted their willingness to engage with crisis line services. In the No Reported Barriers typical category, multiple participants suggested that there were no systemic barriers that would prevent them from contacting a crisis line when experiencing suicidal thoughts. Participant K specified, “I have no thoughts against contacting the crisis center if absolutely necessary.”
In the Impact of Culture general category, however, several participants highlighted cultural factors that might impact their use of crisis line services, such as the “pressure to be successful” (Participant P). Specific cultural experiences emerged in the Religion, Racial/Ethnic Identity, and Intersections variant subcategories. Religious factors that might impact their use of services included preferring faith-based services or a crisis responder with shared religious beliefs, alongside the belief that “suicide is a sin” (Participant S). Participants also highlighted racial/ethnic cultural norms, such as those around help-seeking. For example, Participant Q shared, “The social norms/stigmas that the Black community has with mental health could definitely sway my decision because of how I would be seen for reaching out to a crisis line or a therapist in general.”
Participants also explored the impact of intersecting cultural identities, such as social class and race, that might impact their engagement with crisis services in the Intersections variant subcategory. Multiple participants highlighted the impact of race/ethnicity and gender on help-seeking. Participant B shared that “Black men don’t go to therapy we just toughen it out,” whereas Participant C noted that “Hispanic culture is very big on making sure that men work and provide and are the household leaders so they shouldn’t be the ones to go get help and wallow in their feelings.” On the other hand, in the No Impact variant subcategory, several participants indicated that there were no personal or cultural beliefs that would impact their use of crisis services.
Domain 3: Expectations of Using a Crisis Line
In the Expectations of Using a Crisis Line domain, participants described their expectations of the crisis line experience. In the Understanding of Crisis Line general category, participants expressed their understanding of how crisis lines work and their beliefs about the potential experience when using a crisis line. Some participants shared the belief that contacting a crisis line would be a positive or effective experience in the Effective or Positive Beliefs about Crisis Line typical subcategory. Participants described potential benefits, including experiencing “short-term relief” (Participant A) and being “direct[ed] to positive help” (Participant I). Participant Q shared that the interaction would “encourage me to reach out to others and sway me away from any rash decisions.” Other participants, however, believed that contacting a crisis line would be a negative or ineffective experience in the Ineffective or Negative Beliefs About Crisis Line variant subcategory. For example, concerns included “the cost of sharing what is going on in my life to someone else” (Participant L) and “feeling worse/helpless” after the interaction (Participant Q). Another participant expressed logistic concerns, noting that contacting a crisis line would “take a while” (Participant B). Alternatively, several participants believed that contacting a crisis line would be a neutral experience, while others were not specific in the impact, as described in the Uncertain, Neutral, or Unspecified Beliefs About Crisis Line typical subcategory. Some participants shared that they were unsure what to expect from using a crisis line, with Participant P specifying that they “haven’t thought about it until now.” Participants also highlighted potentially feeling “neutral” (Participant O) or “indifferent about life” (Participant Q) and getting “nothing out of the conversation” with the crisis responder (Participant C).
Alongside the overall experience, participants reflected on how they believed crisis line responder might respond during the interaction in the Anticipated Interpersonal Experience With Crisis Line Responder typical category. Participants discussed concerns that the crisis line responder would “not be empathetic” (Participant H) or would “generalize” their experience (Participant B). Other participants expressed that the crisis responder’s reaction or affect would impact their willingness to share suicidal thoughts. More specifically, Participant R shared that “feeling like someone is pitying me” would inhibit their willingness to share. Participant D noted, “I wouldn’t want to tell them if it sounded like I was bothering them.” In the Talking Away From Suicide variant subcategory, participants specified that crisis line responders would try to talk them away from suicide or suicidal thoughts. Participant H shared “I’m not sure what to expect but I can assume they’ll talk you out of a suicidal situation.”
Domain 4: Expected Experience of Disclosure
Lastly, in the Expected Experience of Disclosure domain, we derived three categories in which participants described expectations of what it would be like to disclose thoughts of suicide. Participants shared the anticipated emotional impact of disclosing thoughts of suicide in the Emotional Impact of Disclosure typical category. Many participants described potentially negative emotional responses, including “vulnerable” (Participant D), “fear” (Participant G), “awkward” (Participant A), “weak” (Participant O), and “intimidated, insecure” (Participant R). However, some shared they anticipated they might feel positive emotions, such as “somewhat relieved” (Participant Q), “mildly hopeful” (Participant R), and “a sense of comfort” (Participant T). A variant subcategory Participant Response did not Include Emotion emerged from respondents who shared they felt “nothing” (Participant I and M) when they thought about what it might be like to disclose thoughts of suicide or who did not disclose an emotional reaction when asked what it might be like to disclose (e.g., “Sometimes it helps but doesn’t always go away,” Participant B). This also illustrated that some respondents, like Participant B, may have shared thoughts of suicide historically and base their responses on that experience.
Participants described how important social supports in their lives might react to learning they had contacted a crisis line for suicidal thoughts in the general Anticipated Reactions From Social Supports general category. Some were unsure (Participant E) how their social supports would respond. However, among participants who provided an answer, four distinct responses emerged. Many participants reflected on Emotion-Focused Response, in which social supports would respond with a specific emotion (e.g., “be worried” [Participant C], “be stunned to realize that I’ve been feeling this way” [Participant H], “be shocked, but not surprised” [Participant O]). Others focused on Engaging Social Support in which social supports would attempt to provide specific supports to the participant. These kinds of responses included “a long conversation” about “my emotions” (Participant D), “ask what was going on” (Participant B), and “offer emotional support” (Participant H).
A variant, Problem-Solving Response highlighted ways that social supports would try to solve the participant’s problem, such as “direct me to a therapist” (Participant I) or “crowd me and never let me leave the house” (Participant G). Finally, in the Engage Social Supports Over Crisis Line variant subcategory, some respondents shared that their social supports would desire for the participant to engage with them rather than a crisis line. For example, Participant T noted, “I think they would be very disappointed that I went to the crisis line for help rather than coming to them and I also think they would be very worried about me and my mental state.” One respondent shared in the variant category Unwilling to Disclose that they simply would not disclose suicidal thoughts.
Discussion
We sought to better understand help-seeking among undergraduate men of color with lived experiences related to suicide, given elevated suicide risk among this population (Stone et al., 2023), unique barriers to help-seeking (Berke et al., 2022), and limited research exploring mental health service use in this population (Lipson et al., 2022). The results of this study provided insight into attitudes toward crisis line use, as well as factors that might impact utilization, among our sample. The domains and categories we developed from the data did not align directly with categories within TPB (Ajzen, 1991) in that components of Attitudes Toward Help-Seeking, Subjective Norms, and Perceived Behavioral Control appeared in a category or subcategory within every domain (see Table 3). However, our findings reveal important nuances in how attitudes toward behavior, subjective norms, and perceived behavioral control may interact with one another to facilitate help-seeking among our sample. Attitudes toward help-seeking were best demonstrated in expectations of using a crisis line and of disclosing thoughts of suicide (domains 3 and 4), whereas aspects of subjective norms and perceived behavioral control appeared in the unique intrapersonal and systemic factors (domains 1 and 2) endorsed by the participants. Indeed, aspects of behavioral control (e.g., coping with suicidal thoughts, anticipated reactions from social supports) appeared related to participants’ attitudes toward crisis line use. Similarly, participants’ existing subjective norms, internalized from their cultural backgrounds, influenced respondents’ attitudes toward crisis line use. Furthermore, these findings primarily emphasize barriers rather than facilitators of crisis line use, as most respondents indicated they would not contact a crisis line or were ambiguous about use.
Intrapersonal and systemic factors that acted as a barrier to crisis line use among our participants align with those that inhibit psychological service use broadly. In our sample, cultural norms related to respondents’ religious beliefs, racial and ethnic identities, and intersections with other relevant social and cultural identities were most influential. Indeed, it was evident that the specific composition of being a man of color alongside other salient identities (e.g., religious beliefs, specific racial identities) shaped how our participants understood help-seeking for suicide, aligning with Grzanka and Miles (2016) conceptualization of intersectionality as an experience of structural dimensions of social inequality that require attending to the unique social position of an individual based on their composition of social identities. Cultural norms for men of color frequently emerge as an intrinsic barrier to help-seeking (e.g., Powell et al., 2016), although fewer studies related to help-seeking for suicide exist. Our findings suggest that, despite the potential benefits of anonymized contact available through a crisis line (Boness et al., 2021), traditional ideas of masculinity and mental health stigma prevent some undergraduate men of color from accessing crisis line services for thoughts of suicide. This is particularly alarming, given that men of color are also less likely to access professional psychological help (Yu et al., 2022) despite facing rising suicide rates (Stone et al., 2023).
The barriers described by our respondents were situated in the context of their unique social positions as men of color, particularly in systemic factors (domain 2) and associated cultural expectations. Although they did not explicitly discuss racism, one way to interpret some of the systemic factors and cultural experiences they named is through the lens of systemic racism and its effects on racially and ethnically minoritized communities. It should be noted that this is a tentative interpretation, and more data from future studies is necessary to substantiate the impacts of racism on crisis line use. Racism contributes to negative mental health outcomes among people of color (e.g., Carter, 2007; Keum & Li, 2023), including associations with suicide and suicide-related outcomes (Boyd et al., 2024; Wong et al., 2014). Simultaneously, racial stigma has a positive relationship with help-seeking barriers, including those described by our sample, which can be exacerbated by internalized self-stigma (Yu et al., 2022). This may explain why participants in our sample were more likely to describe alternate routes of help-seeking, such as seeking services from mental health supports aligned with their religious beliefs, which may be more culturally acceptable and reduce the risk of exposure to greater racist stigma (e.g., Lynch et al., 2018; Moreno & Cardemil, 2013).
Indeed, in our sample, many respondents who indicated that they were unlikely to access crisis line services indicated that they would instead turn to religious figures or members of their faith communities for support. Religion was a source of support for participants as they noted that they would seek help through a faith leader or that they would not act upon suicidal thoughts due to their faith. Religion, more specifically faith-based suicide stigma, could also be a barrier to utilizing crisis lines. Indeed, Lehmann et al. (2021) have argued that more effort is needed to better prepare healthcare professionals to work with religious individuals while also equipping religious leaders with suicide prevention techniques to reduce stigma toward suicidal thoughts.
Relatedly, the intersection of gender appeared particularly salient for most respondents in the sample, particularly those who were unlikely to access crisis line services. However, this was most salient in participants’ reflections on intersecting components of their gender identity and racial or ethnic identity rather than gender as an isolated social identity, further aligning with the importance of intersectionality in our findings. Although respondents did not call out gender as salient, it is impossible to separate their experiences as men of color from their experience with help-seeking (e.g., Grzanka & Miles, 2016). The salience of gendered messaging for men of color specifically aligns with previous research focused on help-seeking among men of color, for whom masculine norms are often influenced by cultural expressions of gender (e.g., Griffith et al., 2012; Powell et al., 2016). Factors such as hyper-independence, needing to be a provider, and unacceptability of vulnerability emerged in our sample as barriers to crisis service line use, which are associated with traditional masculinity (Joyce et al., 2024). This may suggest that, while participants did not call out gender as a salient identifier, their understanding of cultural influences was impacted by masculine expectations and socialization.
If so, this may in part explain the greater reticence among our sample to utilize a crisis line. Joyce et al. (2024) found in a thematic synthesis that adhering to traditional masculine norms, such as those endorsed by respondents in this study, inhibited help-seeking across 25 studies including men at risk of suicide. Indeed, men of color who endorse traditional norms of masculinity experience negative impacts on both their physical and mental health (Griffith et al., 2012), suggesting that these individuals may have greater need for mental health supports yet be less willing to seek them out. Our findings suggest that the intersection of traditional masculine ideas with one’s racial or ethnic identity influenced the kinds of messages participants had internalized, which in turn inhibited intrapersonal help-seeking. When these norms are internalized, factors that contradict them (e.g., vulnerability associated with help-seeking) may be seen as less desirable. For example, Cabrera et al. (2016) suggested that undergraduate men of color may view asking for help as vulnerable and therefore avoid help-seeking.
Alongside systemic and internalized norms, participants’ expectations of the crisis line experience influenced whether they would seek help for suicide. Because most participants had never interacted with a crisis line, they relied on assumptions about what the experience might be like. Our findings suggest that our participants were particularly concerned about practical elements of crisis response (i.e., how the responder would intervene), as well as the emotional impact on themselves. This aligns with previous research: Blanchard and Farber (2020) found that people opted to conceal suicide ideation from a mental health service provider due to unwanted practical impacts as well as to avoid certain emotional experiences. This effect may be larger for men of color, who are more likely to experience fatal police violence (Edwards et al., 2019; Martin & Higginbotham; 2024) including during mental health crises (Shadravan et al., 2021). Additionally, given what is known about the barriers introduced by racism and discrimination in accessing mental healthcare (Yu et al., 2022), our respondents may have believed that they might encounter similar barriers trying to access crisis services. Indeed, several participants indicated that they believed the racial identity of the crisis responder would greatly impact their experience accessing services, illustrating the potential fear of encountering racism or being culturally misunderstood in a time of crisis. Men of color, particularly in higher education settings, have been found to employ numerous strategies to conceal their emotions (Schwab & Dupuis, 2021). For example, scholars have discussed the “cool pose” (Majors & Billson, 1992) among Black men, wherein they may attempt to appear stoic or emotionally unphased to avoid feeling vulnerable or weak (Cofield, 2023; Jackson, 2018). In doing so, men of color have been influenced by the intersection of gender socialization and racial socialization to minimize their feelings and revert to self-coping as opposed to seeking help (Ellis et al., 2015). These findings emphasize the need for crisis counselors who are also men of color in order to combat potential barriers to emotional disclosure (Cabral & Smith, 2011). Because we are unaware of any other studies examining how men of color use crisis line services, there is a need for inquiry to understand how crisis lines can better reach undergraduate men of color, as well as how these individuals experience service use.
A final consideration to contextualize our findings is how the composition of our sample might have influenced what we found. Specifically, participants overall were older than the average traditional undergraduate student, and the wide range of ages and large standard deviation suggests that older students were well-represented in our sample. Some research suggests that mental health and help-seeking stigma is decreasing in the United States, with much of this positive shift being attributed to younger generations (e.g., Min, 2019; Pescosolido et al., 2021). This suggests that the greater prevalence of negative attitudes toward help-seeking in our sample may be in part because our sample was older than the average undergraduate student and therefore may retain more mental health stigma. However, there is also evidence that stigma is greater among younger people relative to older groups (e.g., Bradbury, 2020; Mackenzie et al., 2019). This appears to be truer for men than for women for both anxiety (Bradbury, 2020) and suicide (Mackenzie et al., 2019). Similarly, older men of color endorsed greater mental health treatment stigma versus older White men (Min, 2019), suggesting that gender and racial differences may contribute to greater stigma among older people in our sample.
Limitations and Future Research
Although we employed methods to enhance trustworthiness and transferability, there remain limitations within this study. Like all qualitative work, we as the researchers served as the instrument for interpretation. Despite efforts to bracket our biases and expectations, we may have shared biases as a group that influenced our interpretation of the data. As the interview was anonymous, we could not clarify vague or hard-to-interpret responses. Asynchronous data collection also introduces limitations regarding participant authenticity, information elicited through developing rapport with the interviewer, and observation of nonverbal behaviors or tone of voice that might influence data interpretation (Bouchard, 2016). Moreover, the research team could not invite participants to engage in member checking to preserve anonymity, limiting our ability to determine ways they might have revised our interpretations and findings. Additionally, by relying on TPB to structure the questionnaire, we were limited in our ability to explore salient population-specific questions related to culture, racial and ethnic identity, and structural barriers to crisis line utilization unique to individual participants’ cultures. Furthermore, we could not follow up on this information as respondents explored them at the outset. Although this “wide-range” (p. 643) lens on a phenomenon can be useful, it also limits depth and nuance in interpretation (Braun et al., 2021). There were additional limitations related to the structure of our questionnaire and selected questions. For example, by not explicitly inviting motivating factors, we may have missed opportunities to learn more about what would motivate use of crisis lines. We also did not ask participants about their history of crisis line use or previous suicide attempts. This inhibited our ability to differentiate individuals who may have previously engaged in help-seeking behavior or who may be at higher risk of future suicide behavior, as well as our ability to understand how previous suicide attempts and potential intervention efforts might impact future engagement with crisis lines.
Future research might include follow-up individual or focus group interviews to further explore the four identified domains. Additionally, the sample was more representative of Black and African American, heterosexual, cisgender voices relative to other social identities. Future studies may aim to replicate this study with larger, more diverse sample sizes, including those with varied mental health experiences and levels of suicidality. Future inquiry should explore these constructs among specific ethnic samples to examine how the unique experiences of race, ethnicity, gender, and help-seeking can further inform the impact of social-cultural identities on crisis line use. Additionally, given differences in observed trends related to mental health and help-seeking stigma, future research may explore the impacts of age alongside racial/ethnic identity and gender to better understand unique trends at these intersections.
Implications for Practice, Advocacy, Training, and Research
Our findings also have implications for the delivery of crisis line services. Similar to previous studies (e.g., Moore et al., 2023; Swift et al., 2018), participants emphasized greater trust in working with crisis line responders with similar social and cultural identities to themselves, highlighting the need for systematic efforts to recruit and retain crisis line responders who identify as men and/or persons of color. These efforts may allow men of color the opportunity to navigate the negative emotions associated with emotional disclosure with someone who occupies a similar social position. Additionally, participants mentioned having support networks (e.g., family, friends, faith communities) that they would rely on during mental health crises; however, similar to previous findings (e.g., Blanchard & Farber, 2020), several participants were unwilling to disclose suicide ideation to their social support networks due to stigma, potential consequences, and emotional impacts. Counseling psychologists assess both a person’s support network and their willingness to engage with it, particularly in crisis situations such as suicide ideation. Psychologists may also consider exploring clients’ expectations of crisis line use, particularly for clients at greater risk of suicide, when recommending such a service during safety planning.
Crisis lines represent a powerful public health initiative to reach individuals who may not otherwise access psychological care for suicidal thoughts, yet respondents in our sample were largely unlikely to use or ambivalent about using crisis line services. Furthermore, many of the same barriers present in psychological help-seeking generally appear to influence whether respondents in this study would access a crisis line. Therefore, efforts to destigmatize help-seeking for either, formal psychological services or crisis lines, are needed to facilitate positive mental health outcomes among undergraduate men of color. Efforts to instill hope may also enhance help-seeking among communities of color (McDermott et al., 2017), including undergraduate men of color. In addition, psychologists can advocate for increased state funding to support crisis services, such as the 988 Lifeline, in order to improve culturally responsive training and expand staffing, particularly through the inclusion of counselors of color (Weir, 2022).
Better integration of culturally responsive suicide frameworks (e.g., Wong et al., 2014) and psychological intervention models broadly (e.g., the psychological framework of radical healing in communities of color; (French et al., 2019) within counseling psychology as a discipline may address both concerns and facilitate better access to mental health services. Moreover, faith played a role in creating a support system for some individuals while for others, it was a barrier towards help-seeking due to suicide stigma. As suggested by Lehmann et al. (2021), more efforts need to be made to train psychologists to incorporate sociocultural identities, such as religious beliefs, into suicide prevention efforts. Opportunities also exist for psychologists to train faith-based leaders in suicide prevention to reduce stigma and remove barriers for men of color. Lastly, practicing psychologists can work to stay informed about evidence-based and culturally responsive suicide assessment tools and resources that are appropriate to use within communities of color (Weir, 2022).
The results of this study also present an opportunity for research to explore what specific cultural norms prevent men of color from help-seeking for suicidal thoughts. Moreover, some participants were especially concerned about the identities of the crisis line responders and the consequences they would face for being vulnerable when contacting a crisis line. Researchers could investigate how men of color negotiate consequences like being vulnerable and seeking help with those of their same racial identity versus others. Lastly, many participants shared having strong support systems that they could use if they needed help. However, they also disclosed that they would not use this same support system for suicidal thoughts. Researchers could explore this contradiction and how men of color could either engage their support systems or explore an alternative support system for complex topics like suicide. As faith was an important identity for these men of color, researchers could investigate how faith-based support or faith-based suicide stigma play a role in suicide prevention.
Conclusion
Despite limitations, our findings provide insight into help-seeking intentions and behaviors among undergraduate men of color, who are increasingly at risk of suicide. Although crisis lines, such as the 988 Suicide and Crisis Lifeline, offer promise in addressing this public health crisis and increasing access to crisis services, our findings suggest that perceived experiences with mental health systems inhibit help-seeking among this population. Cultural stigma, traditional masculine norms, and internalized mental health stigma all inhibit crisis line use; furthermore, concerns about who might respond to a sensitive crisis may prevent undergraduate men of color from accessing services when they most need them. Therefore, efforts to destigmatize conversations around mental health, suicide, and help-seeking are paramount among psychologists serving this population to advance access to life-saving interventions.
Footnotes
Ethical Considerations
The Institutional Review Board at Georgia State University approved our study (approval: H24104) on August 31, 2023.
Consent to Participate
Respondents gave written informed consent before taking the questionnaire.