
Abstract
Colonisation continues to impact Aboriginal children and families through perpetual cycles of transgenerational trauma. To achieve culturally safe and effective healing, practitioners working with Aboriginal people must be culturally competent, yet existing research suggests culturally informed practice (CIP) is often poorly understood and implemented by many practitioners. Centring Indigenous perspectives, the present study explored how Aboriginal practitioners in Australia conceptualise and use CIPs when supporting Aboriginal children and families to heal from trauma. Six Aboriginal women practitioners from mental health and social work settings participated in individual research yarns. Reflexive thematic analysis was used to generate four themes, including centring Aboriginal ways, approaches to healing, creating space for healing, and reflexive and responsive practice. CIPs are embedded within Aboriginal approaches to healing, consider the impacts of trauma and colonisation, and require all practitioners to actively engage with Aboriginal people and their ways of knowing, being, and doing.
Culturally safe and effective healing is vital for Indigenous people impacted by trauma. Research on the application of culturally informed practice for Indigenous communities is dominated by the experiences of non-Indigenous practitioners. This study privileges the voices of Aboriginal practitioners who have rich lived experiences and cultural knowledges that guide their culturally informed practices. The insights gained deepen existing theoretical understandings and have practical value for those working with Aboriginal children and families healing from trauma.Significance of the Scholarship to the Public
Indigenous populations across the world hold unique cultural traditions and practices that have maintained their physical, spiritual, and mental health for millennia. The colonisation of Indigenous communities has devasted many Indigenous ways of living, causing immeasurable harm to the health and wellbeing of community members (Paradies, 2016; Silburn et al., 2016). Extensive experiences of trauma, cultural degradation, and human rights violations have resulted in deep wounds (Atkinson, 2002; Duran et al., 1998), which Indigenous people continue to survive and resist. Culturally informed practice (CIP) is a vital competency for practitioners providing mental health and social services to ensure the cultural safety of Indigenous people accessing support, while avoiding further traumatisation. Importantly, CIPs should be led by Indigenous perspectives and honour the unique health and wellbeing needs of each community (Beaulieu & Reeves, 2015; Tujague & Ryan, 2021). This paper explores how Aboriginal practitioners in Australia conceptualise and use CIPs in their work helping Aboriginal and Torres Strait Islander children and families to heal from trauma.
Aboriginal and Torres Strait Islander people (herein respectfully referred to as “Aboriginal people” and “community members”) are an inherently strong and resilient peoples who have lived rich, fulfilling lives on the lands now collectively known as Australia, for over 65,000 years (Atkinson, 2002; Clarkson et al., 2017). The arrival of European colonisers in 1788 marked the beginning of two centuries of invasion, genocide, dispossession, oppression, and cultural degradation, causing physical, emotional, social, and spiritual harm to Aboriginal people (Dudgeon, Wright, et al., 2014). Presently, the enduring impacts of colonisation on Australia’s Aboriginal people are evident in the significantly high rates of grief and loss, abuse, family and domestic violence, child removals, and incarceration (Australian Institute of Health and Welfare, 2020, 2023; Chamberlain, Gray, Bennet, et al., 2022; Wynne-Jones et al., 2016). Although each of these adversities deserves considerable attention, the overarching impact of colonisation is trauma.
Healing from Trauma
In the context of Aboriginal people in Australia, Atkinson (2002) defined trauma as “an event or process which overwhelms the individual, family or community, and the ability to cope in mind, body, soul, and spirit” (p. xi). Encompassing the holistic and collectivist understandings of social and emotional wellbeing (SEWB) held by many Aboriginal people (Gee et al., 2014), Aboriginal experiences of trauma can impact multiple aspects of wellbeing for an individual, their family, and their community. For Aboriginal people, trauma is compounded by experiencing multiple, complex, and interconnected traumatic events, which accumulate over multiple generations (Milroy, 2018). A pertinent example is the Stolen Generations. During the early to late 20th century in Australia, countless Aboriginal children were forcibly removed from their families and subjected to institutionalisation, slavery, sexual and physical abuse, cultural degradation, and disconnection from their family and traditional lands (Commonwealth of Australia, 1997). These traumas severely disrupted Aboriginal SEWB and traditional child-rearing practices, leading to further child removals and a cycle of intergenerational trauma still evident today (Chamberlain, Gray, Bennet, et al., 2022). In response to the ongoing impacts of colonisation and trauma, Aboriginal experts, leaders, and community members have called for community-led, culturally responsive, and trauma-informed approaches to healing for Aboriginal people (Chamberlain, Gray, Bennet, et al., 2022; Milroy, 2018). These approaches must go beyond Western mental health and social services intervention, to effectively address trauma in Aboriginal communities (Menzies, 2019; Tujague & Ryan, 2021; Walker, Schultz, et al., 2014).
Culturally Informed Practice
CIP describes a myriad of considerations and approaches for delivering culturally safe and effective services to Indigenous peoples. A primary focus of CIP is achieving cultural safety, that is, ensuring Indigenous people feel their cultural identity is accepted, free from judgement, and not threatened or compromised when accessing health and wellbeing support (Ramsden, 2002; Smith et al., 2021; Tujague & Ryan, 2021). Founded within Indigenous frameworks for delivering culturally safe health services (Ramsden, 2002), cultural safety is now widely recognised as a practice competency for professionals working with Aboriginal people (Smith et al., 2021; Walker, Schultz, et al., 2014), particularly those registered with accreditation bodies in social work (Australian Association of Social Workers, 2020), psychology (Australian Psychological Society, 2007), and other health professions (Australian Health Practitioner Regulation Agency, 2022). Despite this, there is an evident gap in the appropriate understanding and use of CIP in Australia (The Lowitja Institute [TLI], 2018).
Existing literature suggests that although many non-Indigenous mental health professionals and service providers attempt to adapt Western designed services to be more culturally appropriate, the resulting support can be insufficient and ineffective for Aboriginal people in Australia (Gibson et al., 2020; Kilcullen & Day, 2018; McConnochie et al., 2012; Mullins & Khawaja, 2018). Western approaches and theories often misalign with Indigenous knowledges, beliefs, and practices, creating a power differential that can lead to Indigenous people being unfairly judged, discriminated against, and provided inappropriate and ineffective support (McKendrick et al., 2014; Walker, Fredericks, et al., 2014; Walker, Schultz, et al., 2014). This highlights the importance of privileging Indigenous perspectives and approaches when designing and implementing services for Aboriginal people.
Practitioners in mental health settings have described being hesitant to engage in CIP due to inadequate training, and a fear of being culturally insensitive (McConnochie et al., 2012; Sullivan et al., 2022). Further issues include practitioners and services failing to understand Aboriginal concepts of health and the complexities of Aboriginal trauma, leading Aboriginal people to experience cultural unsafety, discrimination, and retraumatisation when accessing Australian mental health and wellbeing services (Baba et al., 2014; Gibson et al., 2020; TLI, 2018). Given the pervasive impact of trauma within Aboriginal communities, understanding how practitioners can support Aboriginal people to heal from trauma in culturally safe and effective ways, deserves considerable attention in the literature. Exploring practitioner perspectives can provide important insight into existing gaps in the understanding and implementation of CIP in these contexts.
Practitioner Perspectives
Existing literature examining practitioner perspectives on culturally safe and effective trauma healing for Aboriginal people is both scarce and limited by a Western mental health lens. Non-Indigenous psychologists have described needing to step outside of their psychology training, as Western psychology models are considered inadequate for meeting the needs of Aboriginal people accessing mental health support (McConnochie et al., 2012; Mullins & Khawaja, 2018). Concerningly, due to lacking appropriate training, psychologists established their own CIP strategies during therapeutic treatment (Mullins & Khawaja, 2018), including through a process of trial and error (McConnochie et al., 2012). This reveals an issue whereby CIP is not always informed by appropriate training, or importantly, by Aboriginal expertise or people themselves. Centring Aboriginal knowledge and experiences is vital for ensuring the effective design and implementation of CIP (Milroy, 2018; Tujague & Ryan, 2021). Despite this, there is a scarcity of literature examining the experiences of Aboriginal practitioners using culturally safe and effective approaches for trauma healing.
Aboriginal Perspectives
Expanding the lens of CIP, existing research provides Aboriginal-led insights into the needs and experiences of Aboriginal people accessing support in social work, child welfare, and healthcare settings. Aboriginal practitioners, experts, and community members accessing support have described the importance of holistic and collaborative approaches; promoting Aboriginal worldviews and cultural practices; providing client choice and control; using flexible, person-centred approaches; engaging in deep, respectful listening; and establishing trusting relationships with service users (Bennett et al., 2011; Blakemore et al., 2021; Chamberlain, Gray, Herrman, et al. 2022; Coombes et al., 2022; Mitchell et al., 2022; Murrup-Stewart et al., 2019). Integrating cultural activities into practice and strengthening connection to culture are considered beneficial to the health and wellbeing of Aboriginal people, by fostering cultural attachment and social identity (Bourke et al., 2018; Hunter et al., 2021). Cultural activities in this sense include activities like traditional dancing, art, and ceremonies that allow culture to be expressed socially (Hunter et al., 2021).
Also identified by Aboriginal service users, is the importance of practitioners using appropriate language and communication (Gibson et al., 2020; Vicary & Bishop, 2005). Additionally, CIP requires practitioners to engage in reflexive and responsive practice through ongoing, critical self-reflection on their therapeutic approaches and their own privilege and cultural positioning, and adjust their approaches accordingly (Menzies, 2019; Smith et al., 2021; Tujague & Ryan, 2021). Although the literature has provided important insights into CIP in health and social service settings, the use of CIP in the context of trauma healing is limited. More in-depth, Aboriginal-led understandings of how CIP can be understood and implemented by practitioners supporting trauma healing, is greatly needed. For example, how practitioners use CIP to promote healing in their therapy and interventions is an important understanding for helping to overcome continuing cycles of trauma in Aboriginal communities (Atkinson, 2013; Milroy, 2018).
Trauma-informed practice (TIP) is another vital consideration for practitioners working with Aboriginal communities (Atkinson, 2013; Tujague & Ryan, 2021). TIP describes a strengths-based, empowering approach to healing that responds to the impact of trauma on an individual, including the need for physical, psychological, and emotional safety (Blignault et al., 2014; Piotrowski, 2020). Although TIP is considered a crucial aspect of CIP, mainstream understanding of trauma has been described as insufficient for addressing the holistic healing needs of Aboriginal people (Menzies, 2019; TLI, 2018; Tujague & Ryan, 2021). Importantly, practitioners must develop their understanding of Aboriginal experiences of colonisation, trauma, and racism, and actively take a stance to address issues of discrimination (Herring et al., 2013). However, how all practitioners can practically respond to these needs in culturally informed ways is not well understood in the current literature. Further exploration, through an Aboriginal lens, is greatly needed to develop existing understandings of appropriate and effective CIP for healing (Menzies, 2019).
Research Aim
Further research is needed to expand on existing understandings of CIP in the context of helping Aboriginal children and families overcome continuing cycles of trauma (Atkinson, 2013; Chamberlain, Gray, Bennet, et al., 2022). Specifically, existing literature lacks the perspectives of Aboriginal practitioners using their unique worldviews and experiences to inform culturally safe and effective healing. The present research aimed to explore how Aboriginal practitioners in Australia conceptualise and use CIP when helping Aboriginal children and families to heal from trauma. The findings are anticipated to provide Aboriginal-led recommendations for culturally informed approaches to healing for those working with Aboriginal communities in Australia.
Method
Ethical Considerations
The study received ethical approval from the Monash University Human Research Ethics Committee (Project ID: 31997). In line with similar research, the term “knowledge holders” was used instead of “participants” to reflect the agency and knowledge ownership of those who contributed (Murrup-Stewart et al., 2021). The research design addressed the National Health and Medical Research Council’s (2018) six core values for research with Aboriginal and Torres Strait Islander people. The first value, spirit and integrity was met by ensuring the project committed to the remaining five values; Indigenous research paradigms were employed to privilege Aboriginal perspectives (cultural continuity); an equal partnership was encouraged throughy arning methods, whereby knowledge holder and researcher collaboratively directed the flow of conversation and therefore the research output (equity); the proposed benefits of participation were clearly outlined, including a thank you voucher, the opportunity to contribute to improvements in practice, and the hope to benefit Aboriginal people (reciprocity). Informed consent was gained by outlining each step of involvement, such as signing consent, the right to refuse questions or withdraw from the study, steps for recording yarns and member checking (respect); and finally, Aboriginal people were consulted throughout the project from conceptualisation to dissemination (responsibility).
Researcher Positionality
The first author identifies as a Jardwadjali Aboriginal woman, with Anglo-Celtic ancestry, living, working, and learning on Wurundjeri and Boonwurrung lands. The author positions themselves within the research as an Aboriginal person working within an Aboriginal community, while completing a Western psychology degree. The author did not grow up connected to their ancestral lands or culture, is privileged by a tertiary education, and walks in two worlds: one shaped by growing up as a White-passing Aboriginal person in a Western society, and a second shaped by ongoing cultural reconnection through engagement with Aboriginal ways of knowing, being, and doing. The first author was supported in this research by the second author, an Aboriginal wellbeing researcher with close ties to Wurundjeri Country and a personal history impacted by Stolen Generations, and the third author, a non-Indigenous researcher of Western European descent from a working to lower class background but privileged by their tertiary education and white racial identity.
Research Paradigm
Indigenous research methodologies honour and validate the voices, oral traditions, and knowledge structures of Indigenous peoples, while aiming to decolonise research and promote cultural safety for Indigenous research participants (Kennedy et al., 2022; Smith, 2021). This research was underpinned by an Indigenous research paradigm, which privileges Aboriginal ways of knowing (epistemology), being (ontology), and doing (axiology), and the relationality between the researcher and the research (Wilson, 2008). As a core principle of Aboriginality, relationality encompasses the paradigm as follows; Aboriginal ways of knowing and being are represented by the forming of mutual realities through relationships, whereas Aboriginal ways of doing maintain accountability to those relationships (Wilson, 2008). Interacting with these principles, the first author’s own sociocultural position and Indigenous standpoint guided the research design (Atkinson et al., 2021; Foley, 2003). This involved reflexive engagement with Aboriginal people and Indigenous research, literature, and frameworks to uphold cultural safety, bolster Aboriginal perspectives, and ultimately benefit Aboriginal people. Adapted from a model developed by Atkinson et al. (2021) and influenced by earlier models from Walter and Andersen (2016) and Wilson (2008), Figure 1 outlines the Indigenous research methodology employed in this study, including the choice of a yarning method. As will be explored further in the following sections, the choice of a yarning method allowed the research to privilege relationality and Aboriginal ways of knowing, being, and doing (Atkinson et al., 2021). Indigenous Research Methodology and Use of Yarning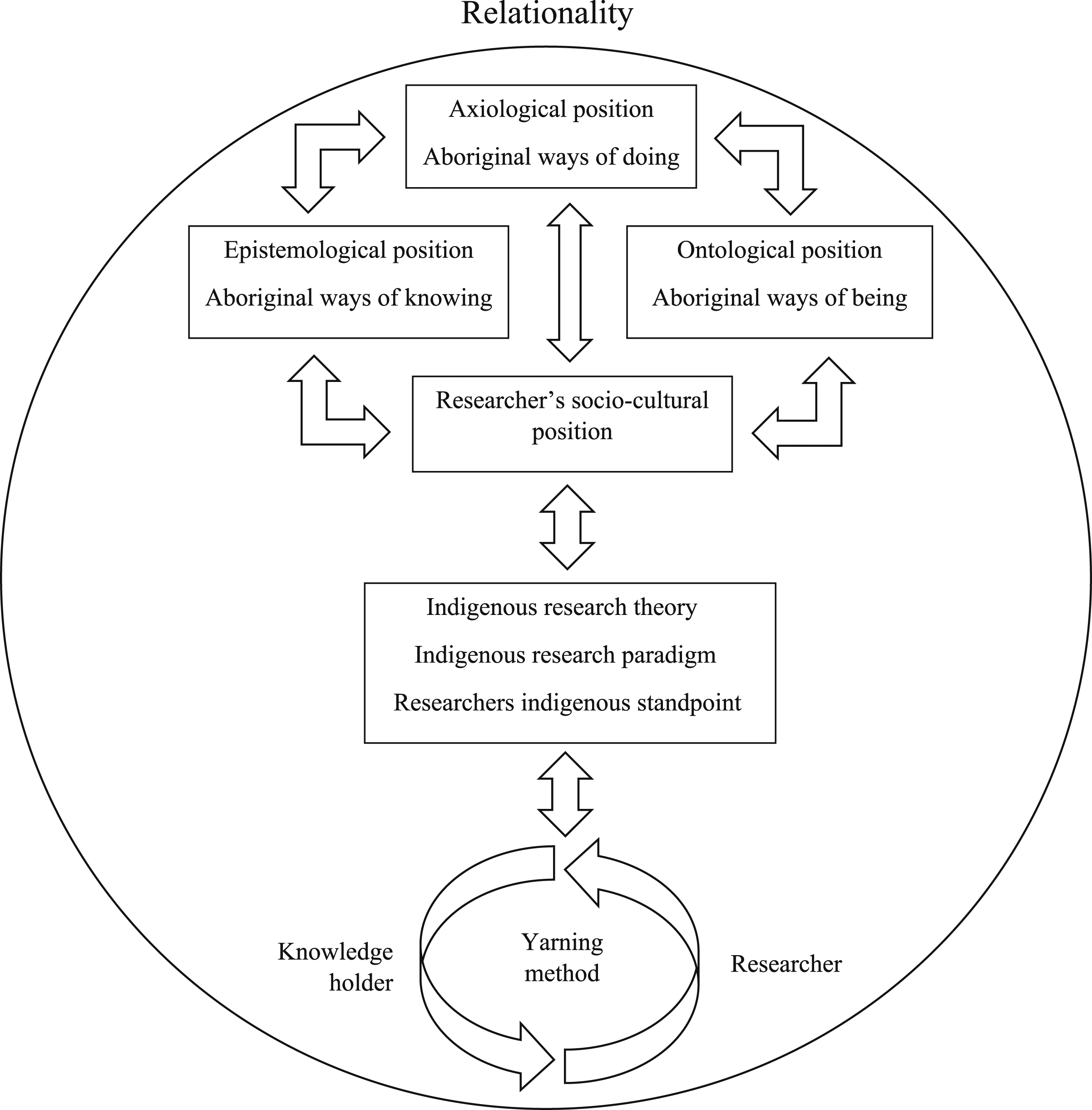
Yarning
Yarning is a formal process of telling used by Aboriginal people to share stories and gather knowledge (Dean, 2010; Walker, Fredericks, et al., 2014). Yarning as an Indigenous research method is underpinned by principles of cultural safety and connectedness, and allows knowledge holders and researchers to contribute toward a shared understanding of a research question as respected equals (Atkinson et al., 2021; Bessarab & Ng'andu, 2010). This study utilised research topic yarning, a fluid research interview method where knowledge holders direct the yarn in ways that are meaningful to them (Bessarab & Ng'andu, 2010). A yarning guideline was developed to guide the yarn through several stages, including social yarning (e.g., building relationality through personal introductions and sharing of experiences), orienting the research topic yarn (e.g., “What kind of experience do you have working with Aboriginal and Torres Strait Islander children and families?”), and beginning the research topic yarning (e.g., “Can you tell me about what [CIP] means to you?”). The authors consulted to develop questions that would elicit understanding and experiences of CIP and identify existing barriers, challenges, and proposed solutions.
Knowledge Holders
Aboriginal and/or Torres Strait Islander professionals aged 18 years and over with experiences working with Aboriginal and/or Torres Strait Islander children and/or families to heal from trauma were eligible to participate. The first author employed convenience sampling methods by directly emailing or messaging eligible personal and professional connections on social media platforms. Snowballing also occurred, whereby three of the author’s connections contacted known prospective knowledge holders, who consented to be contacted by the author over phone or email. These were considered culturally appropriate recruitment methods, given the importance of establishing relationality, trust, and safety between the researcher and knowledge holders (Bessarab & Ng’andu, 2010; Dean, 2010; National Health and Medical Research Council, 2018). Twelve practitioners were invited to participate. Four declined to participate and two did not respond. Six Aboriginal women aged 32 to 50 (M = 40.16) participated. Knowledge holders worked predominately with Aboriginal women, children, and families in child and family welfare, family violence, counselling, and psychology settings. Due to the specificity of the sample and small cohort, anonymity could not be guaranteed without omitting further demographic details.
Yarning Procedure
Individual yarns were held between the first author and each knowledge holder. Yarns were held over phone or Zoom calls and were audio recorded. Cultural communication protocols were followed within the social yarning before recording began, signalling the start of the research topic yarning. Yarn recordings ranged from 54 to 84 minutes (M = 71.97) and were transcribed by the first author. All knowledge holders were given the opportunity to review transcripts for accuracy and provide feedback on meaning, with one providing additional clarity.
Knowledge Analysis
The data was analysed using reflexive thematic analysis (RTA), a coordinated yet flexible analysis method used to explore patterns and potential meaning in a qualitative data set (Braun & Clarke, 2019). This approach allowed the first author’s own positioning as an Aboriginal Australian and practitioner to validate and shape a meaningful interpretation of the data (Braun et al., 2019). Using their knowledge and experience, and reflecting on the knowledge holders’ contributions, the first author made informed decisions about what data was significant towards addressing the research topic. Importantly, the flexibility of RTA helped to decolonise the analysis by honouring yarning as a valid form of gathering Aboriginal knowledge, creating shared meaning, and privileging the perspectives and knowledges of those participating (Gibson et al., 2020; Kennedy et al., 2022).
The six stages of RTA (Braun et al., 2019) were followed. Familiarisation occurred through the first author participating in, then listening to yarn recordings twice during transcription. The first author then read through printed transcripts twice over, while highlighting and writing reflective notes about possibly meaningful data. Coding involved the first author handwriting short, representative phrases or labels (codes) onto printed transcripts for segments of the yarn which addressed the research topic. A second sweep occurred whereby codes were digitised into an Excel spreadsheet and further developed to improve meaning.
Themes were generated through an iterative process of organising codes into cohesive groups that shared patterned meaning and ascribing labels (themes) to these groups. Multiple iterations of labelling and organising occurred until each code fit within a narrow subtheme, and a broader, more overarching theme. Themes and subthemes were further revised and refined by scribing different variations onto paper, using digital mind mapping, and pooling several transcript quotes against each subtheme within Excel to check that subthemes reflected the raw data. The authors consulted each other during the development of the themes, including the second author completing transcript checking by independently reviewing two transcripts and meeting with the first author to discuss and further refine themes.
Findings
Themes and Subthemes
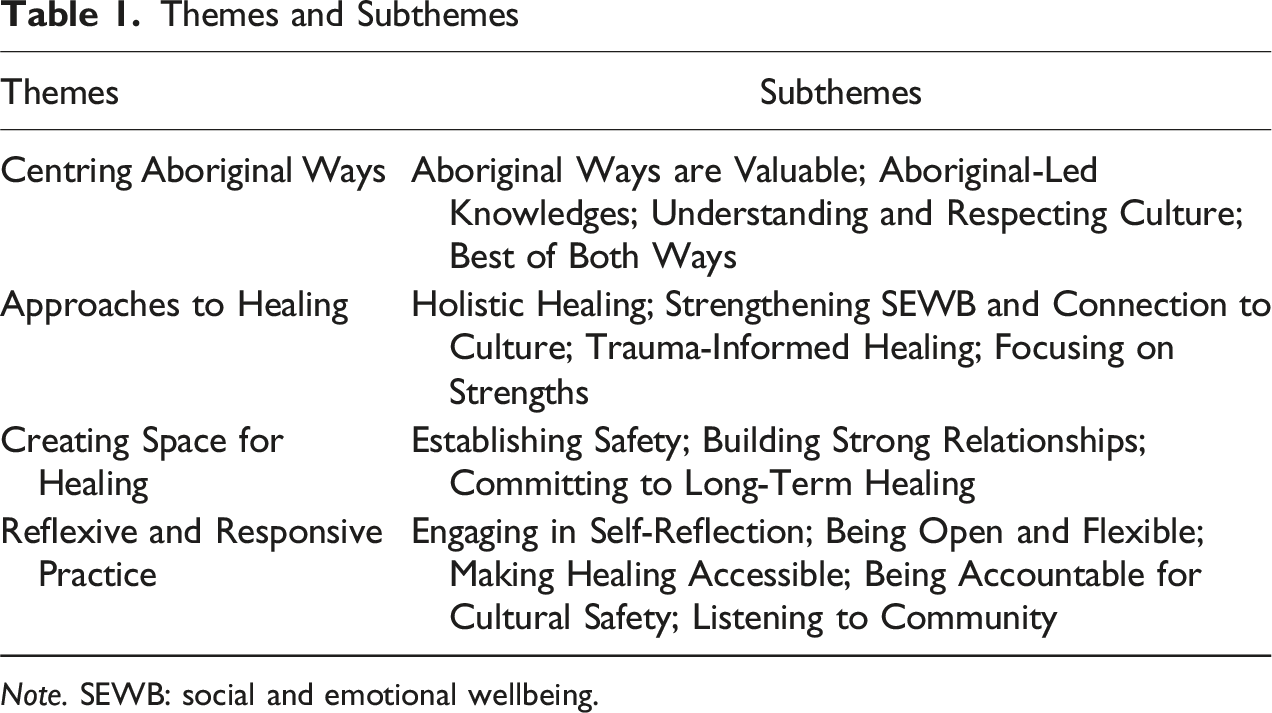
Note. SEWB: social and emotional wellbeing.
Centring Aboriginal Ways
This theme encapsulated a foundational importance of valuing and privileging Aboriginal ways of knowing, being, and doing to achieve CIP. Both in their principles and practices, knowledge holders reflected the importance of; acknowledging Aboriginal ways of working as valid and valuable approaches; being led by Aboriginal people, knowledges and resources; and developing one’s understanding of, and respect for, Aboriginal culture. Knowledge holders also reflected the value of utilising Western models of healing, if they were deemed by Aboriginal people, to be appropriate or beneficial for Aboriginal people.
Aboriginal Ways are Valuable
This subtheme tied closely to their core values and worldviews, all knowledge holders described CIP as understanding, valuing, and being grounded in Aboriginal epistemologies. For example, Lyla reflected, “relationship, and trust, and respect, and reciprocity … we know that we are operating in a culturally responsive way … because we’re coming back to Indigenous ways of knowing, being, doing.” Aboriginal values, knowledges, and practices were seen as equally, if not more valuable, valid, and effective approaches to practice compared to Western approaches. Knowledge holders reflected that feeling the opposite was true for many non-Indigenous practitioners, services, and systems, and considered this a missed opportunity for best practice when supporting Aboriginal people.
Aboriginal-Led Knowledges
All knowledge holders emphasised the importance of their practice being informed by Aboriginal people and knowledge. Celeste shared how “The real work is done by community, with community, in community.” Examples included Aboriginal-led service design and provision, utilising resources, assessments, and trainings developed by Aboriginal people, and acknowledging Aboriginal people as experts in their own trauma. Western theories and frameworks, such as psychology and social work disciplines, were utilised and adapted when deemed appropriate and safe by Aboriginal people.
Understanding and Respecting Culture
Knowledge holders described the need for practitioners to learn about and respect each community member’s distinct cultural values, customs, and protocols, such as men’s and women’s businesses, respect for Elders, grieving rituals, and Aboriginal family and kinship structures. Several knowledge holders described perceptions that non-Indigenous understandings of CIP were limited to doing cultural activities in therapy sessions. Celeste described how “People get a very messed up idea of what culture is … we have to be very ‘visibly’ practicing it”, whereas Aboriginal values, knowledges, and ways of being were less recognised as cultural practice. Additionally, Lyla reflected, “There’s so much diversity in Aboriginal and Torres Strait Islander peoples and culture … it’s important to recognise what contemporary forms of culture look like as well.” Nellie described how non-Indigenous people fail to understand the complexities of a post-colonial connection to culture “because nobody forcibly took your culture from you.” Reflexivity was considered important for all practitioners to deepen and broaden their understanding of culture and CIP in the context of the specific communities they worked within. Lyla said, “We might directly learn about that history from you know, the families or the person themselves … or it might be an Elder or cultural advisor.”
Best of Both Ways
Knowledge holders utilised Aboriginal and Western ways of working when considering each community member’s therapeutic needs and preferences. Lyla shared, “It’s not whether a particular treatment modality can, or can’t be used … it’s about examining with your Aboriginal and/or Torres Strait Islander client what treatment modalities, strategies, interventions make sense to them, to meet their needs.” For example, Celeste described seeing how Western medications in isolation did not promote deeper healing, however, it may be “useful for getting you in a space where you can start doing the healing work.” While cautious of possible harms, Western-designed assessments, interventions, and resources were considered useful when carefully applied to benefit Aboriginal people. Rosie reflected, “How do we make [Western] assessments and measures work in our favour? None of it’s designed for us … how do we make it work?” Further examples included Western university degrees providing a starting point to adapt for use in community, combining Western psychology with an Aboriginal SEWB framework, and using Western systems to advocate for change. Corina described seeing the benefit of adapting Christian religious frameworks and using church spaces for women to come together to heal and express their traditional spiritual beliefs.
Approaches to Healing
Knowledge holders described several interconnected approaches that were used simultaneously for culturally safe and effective healing. The approaches were both conceptual frameworks and practical approaches that informed the knowledge holders use of CIP. Each subtheme represents an important approach within CIP, and were considered inherently Aboriginal ways of working that centred Aboriginal values and epistemologies.
Holistic Healing
Knowledge holders commonly referred to “whole of self” and “whole of family” approaches, where individuals were seen as inseparable from their family, making wraparound support an important part of CIP. Corina shared “It’s not just the child you have to support, it’s the whole family.” Several knowledge holders described siloed treatments as insufficient and emphasised the benefit of interdisciplinary collaboration. Referencing the benefits of an Aboriginal health service, Nellie described “OTs [occupational therapists], social workers, psych [psychologist], nurse, everything all working together … there was financial counsellors, there was doctors … that makes it so much easier for people to step in the door.” Celeste explained how “you can’t just talk about us (in) sections, you have to take us as a whole,” and despite Aboriginal people “building these great little healing communities that work,” the Western world often “doesn't see the benefit.”
Strengthening Social and Emotional Wellbeing and Connection to Culture
Closely connected to Holistic Healing, most knowledge holders referenced an understanding of SEWB as integral to CIP. Knowledge holders described the healing nature of strengthening community members’ connections to culture, Country (traditional lands), community, family, spirituality, body, and emotions. Providing opportunities for community members to come together to yarn, laugh, play, eat, and engage in cultural activities was considered vital for healing. For example, Merinda described how “one activity of dancing … especially if it’s like, cultural … and with … an Aboriginal, you know, instructor” can address multiple social-emotional wellbeing domains. Further examples included participating in traditional ceremonies, connecting with Elders and Aboriginal role models, and attending community programs, each of which helped strengthen cultural identity, belonging, and pride.
Trauma-Informed Healing
Trauma-informed practice was also considered vital for healing and often described as inseparable from CIP. Knowledge holders understood many cultural activities, such as dancing, singing, painting, weaving, smoking ceremonies, yarning circles, and grieving rituals, to be inherently healing. Nellie explained how “connection to culture, you know, you’re healing … when you think about things like … neurosequential models of trauma… there’s plenty of cultural activities and healing practices that are actually part of that (trauma-informed practice).” Knowledge holders also described trauma-informed practice as inseparable from understanding the impacts of colonisation. Lyla reflected, “you kind of can’t talk about how to do culturally safe and, and trauma safe practices without knowing … Australia’s colonial history and the ongoing impact of colonial trauma.” Importance was placed on practitioners acknowledging social injustices, ensuring community members were not burdened with educating practitioners about colonisation, and understanding the unique trauma experiences of Aboriginal people. Further examples included increasing community members’ knowledge about trauma, normalising the impacts of trauma, reducing feelings of self-blame and shame, facilitating storytelling, and honouring community members’ choices.
Focusing on Strengths
Knowledge holders considered strengths-based assessment, intervention, and language, to be important for CIP. Rosie reflected, “We already know what’s wrong with us … let’s talk about what’s good about us.” For instance, creating positive and fun therapy experiences supporting community members to see their Aboriginality as a strength, shifting the focus from risks to coping skills, and from intergenerational trauma to intergenerational survival and healing. Corina noted that “We don’t hear enough about intergenerational healing. Now is the time to put that into action.” Reflecting on community members they worked with, Celeste noted “they’ve survived through quite a lot and recognising those particular skills … really acknowledging all of the strengths … they’re the things that you can work with.” Practitioners reflecting on and shifting their lens from one of deficit to strength, was described as imperative for CIP.
Creating Space for Healing
This theme included several important principles and practices that knowledge holders emphasised as important for ensuring community members had the capacity to engage in healing. Knowledge holders described CIP as being aware of and supporting community members with their needs for safety and stability in their life, strong and trustworthy relationships, and enough time to engage in healing. Knowledge holders described the importance of meeting these conditions for healing to be possible.
Establishing Safety
Knowledge holders highlighted the importance of community members having their basic needs met to effectively engage in trauma healing. This involved supporting community members in accessing resources like food, water, funding, and stable housing by linking them to appropriate services and supports. Nellie described how “Paying your bills so the lights aren’t going to get turned off, that is safety.” Where ongoing risks to physical and emotional safety were identified, Celeste reiterated “We need to really just work on the safety side of things” before healing could begin. Safe healing environments were established by meeting community members in settings familiar to them. Corina reflected, “We have to meet them where they’re at,” with examples including meeting in Aboriginal community spaces, on Country, in a community member’s home, yard, or even standing by their car. Closely connected to building strong relationships, knowledge holders also described establishing safety through relational and interpersonal skills. These included developing trust and rapport, modelling equality, and displaying positive regard and nonjudgement. Nellie described the importance of “helping people … feel comfortable, feel safe, feel like they belong, and that they’re welcome.”
Building Strong Relationships
All knowledge holders explained how building strong relationships with community members was a vital aspect of CIP. Celeste reflected, “Our intervention needs to be the relationship.” This relationship between the practitioner and community member was described as a tool to facilitate learning about trauma, modeling healthy relationships and wellbeing practices, and enabling community members to feel heard. Knowledge holders utilised interpersonal skills, including developing trust and rapport, modelling equality in the relationship, and displaying positive regard and nonjudgement.
Establishing such strong relationships was considered equally important to mitigating risks and undertaking assessments and interventions. Through the therapeutic relationship, knowledge holders determined what approaches and assessments would be appropriate for individual community members. Rosie described how “engagement’s actually more important … let me get a sense of you … then I can go okay, I’m comfortable with doing [specific assessment] now.” Practitioners also described supporting community members to build up their personal relational networks to ensure lasting support and connection. Celeste explained, “we try to link them with mentors and mob (one’s identified group of family, clan or community members) … with like an aunty- or an uncle-type figure that they can relate to.” Strong relationships with practitioners, family, and other community members provided long-term stability for healing.
Committing to Long-Term Healing
All knowledge holders described the importance of long-term support for community members to heal. This was imperative to Aboriginal ways of forming relationships and addressing the lasting impact of trauma. Merina reflected, “six to 10 sessions … our mob … might have some intergenerational trauma, some financial distress, an incarceration in the family … all that trauma … it takes that long just to build trust sometimes.” One illuminating example described an intensive healing camp where women returned to Country for 8 weeks. Long-term funding, investment, and service delivery, alongside preventing practitioner turnover and burnout, were identified as highly important for CIP.
Reflexive and Responsive Practice
Finally, this theme reflected several culturally informed principles and practices that required active reflection and subsequent responses from practitioners. Knowledge holders described the importance of practitioners being able to self-reflect, be open and flexible, take appropriate action, hold themselves and others to account, and listen deeply to Aboriginal community members. Closely tied to creating space for healing, which focused on meeting the needs of the community member, reflexive and responsive practice represented the needs of practitioners to engage in CIP.
Engaging in Self-Reflection
Several knowledge holders described the importance of practitioners reflecting on their own cultural, political, and social positioning, and critically examining their beliefs, attitudes, and experiences concerning their practice and engagement with Aboriginal people. Lyla described how as a practitioner, “I need to look at my culturally responsive practices and culturally safe practices,” while engaging in ongoing “learning and critical reflection.” Examples included evaluating their practices and client relationships, having reflective conversations with other professionals, and engaging in personal therapy and supervision. Self-reflection extended beyond professional contexts, involving a deeper reflection on one’s personal connection to Aboriginal people and culture. Rosie expounded that it’s about “bringing [non-Indigenous professionals] back to their own culture and family.”
Being Open and Flexible
Several knowledge holders described the need for practitioners to be open-minded and flexible about what approaches would be effective for each community member. This often involved breaking down the personal and professional walls built by mainstream Western concepts of boundaries and scientific superiority. For example, dropping therapy agendas, allowing for unstructured healing time by sitting in silence, and talking about topics unrelated to healing. Celeste described, “just going in to yarn and play … and see what comes out of that space … [that] is much more important than trying to control that space.” Flexibility involved practitioners adjusting and individualising their approaches to each community member, by combining different approaches and diversifying their practice. Reflecting on their interventions, Merinda shared, “You’re creating it and being eclectic as you go.”
Making Healing Accessible
Knowledge holders described the need for practitioners to take direct action to reduce barriers and improve access to support. Referencing long waitlists, Corina explained, “I’m not here to have my, my people still put on a … waiting list, when we’ve been put on a list for generation and generation.” Likewise, broadening referral criteria, avoiding strict cancellation policies, or holding sessions outside of therapy rooms was articulated as important. Nellie described an example of reducing a barrier by allowing parents to bring children to sessions, “They can come in with their child or they won’t come at all. So even having rooms set up well for that.”
Being Accountable for Cultural Safety
Knowledge holders described the importance of practitioners being personally accountable for cultural safety by acknowledging issues, advocating for community members’ needs, and taking action to create change. Knowledge holders suggested this could be achieved through actions such as identifying culturally unsafe and biased assessments, processes, and systems, and holding other professionals to account for their roles in unsafe practices. To this regard, Rosie reflected on the importance of “lobbying and sharing that information with everybody … we need to start making people accountable.” When it came to culturally safe and effective practice, Merinda reflected how Aboriginal practitioners “care so much more,” “go the extra mile,” and tend to “be more creative” than non-Indigenous practitioners. Knowledge holders all emphasised the importance of accountability for improving the understanding and use of CIP in all practitioners.
Listening to Community
Knowledge holders described the importance of engaging with Aboriginal experts, Elders, and community to develop their knowledge, as reliance on education and cultural awareness training was considered insufficient. Corina lamented how non-Indigenous professionals were often “getting their information from textbooks … What about our mob sitting down on the ground?… That’s where you’ll learn the most from.” Given the diversity of Aboriginal people, practitioners needed to build meaningful connections with local communities, consult Aboriginal colleagues, seek cultural supervision, and diversify their knowledge sources. Furthermore, knowledge holders described the importance of listening to deepen practitioners’ understandings of the experiences, stories, values, beliefs, and needs of community members. This concept of listening went beyond Western understandings, referring to processes of slowing down, sitting with community members, and being fully present with people and nature. Celeste shared the following knowledge: It’s in all of our languages and cultures, is that ability to be quiet and still and actually hear what somebody’s saying, sort of be changed by that process, and they’re changed by the, the process of being deeply listened to.
Discussion
The present research aimed to explore how Aboriginal practitioners conceptualise and use CIP when supporting Aboriginal children and families to heal from trauma in Australia. The knowledge holders in this research described CIP as a myriad of interconnected understandings, approaches, and practices, which were foremostly informed by Aboriginal people and knowledges. These findings provide important guidance for how CIP can be understood and applied by all practitioners working with Aboriginal children and families impacted by trauma in Australia. Although the findings leaned heavily towards the conceptualisation of CIP, it is precisely this theoretical grounding that informs the limited but salient examples of CIP usage in trauma healing. The conceptual principles described by knowledge holders guided the highly context-dependent and reflexive practices used to promote trauma healing. Simply providing examples of use may not be an effective way to promote CIP, as practices were context-, client-, and practitioner-dependent, and therefore may not always be transferrable. The conceptual framework of CIP described in this research therefore serves as a guiding force for its practical application.
When it comes to trauma healing, our findings highlight the importance of valuing and utilising Aboriginal ways of knowing, being, and doing, which existed long before colonisation. This echoes previous findings that understanding and valuing Aboriginal knowledges and worldviews are important approaches in social work (Bennett et al., 2011), perinatal care (Chamberlain, Gray, Herrman, et al., 2022), healthcare (Baba et al., 2014; Mitchell et al., 2022), and psychology settings (McConnochie et al., 2012; Mullins & Khawaja, 2018). However, where previous research has emphasised the need to develop CIP to make Western wellbeing models and practices more culturally safe and responsive (Coombes et al., 2022; Kilcullen & Day, 2018; McConnochie et al., 2012; Mullins & Khawaja, 2018), these findings demonstrate the reverse; CIP was foundationally grounded in Aboriginal ways of working, with Western practices considered as additive and applied when they were of benefit to Aboriginal people. This has implications for many Western designed social work and mental health services in Australia by highlighting the importance of embedding Aboriginal ways of working within the foundations of service delivery, and in the training of professionals working with Aboriginal people (Walker, Schultz, et al., 2014). This research supports a need for Western-designed services and Western-trained practitioners to critically examine their understanding and use of CIP. Additionally, the findings provide insight into how practitioners can work towards culturally safe and effective healing, and strengthen their understanding of the cultural, spiritual, and social wellbeing needs of their Aboriginal clients.
This study expands upon previous findings examining Aboriginal perspectives (Bennett et al., 2011; Chamberlain, Gray, Herrman et al., 2022; Vicary & Bishop, 2005), highlighting the importance of engaging in critical self-reflection to navigate effective CIP. The broad and flexible understandings of culture and CIP shared by knowledge holders can be considered in comparison to non-Indigenous understandings of CIP, which were identified as being too narrow, and overly reliant on the use of cultural activities in therapy. Overemphasis on these activities may lead practitioners to neglect other important aspects of CIP and subsequently fail to achieve cultural safety for Aboriginal clients (Walker, Schultz, et al., 2014). To simplify, CIP cannot be achieved through incorporating cultural activities alone but requires a deeper understanding of the complexity of Aboriginal perspectives of wellness, the influence of bias and systemic oppression on Aboriginal wellbeing, and the impact of colonisation on individual cultural connectedness. The present study highlights a need for all professionals working with Aboriginal people to critically examine their understandings of culture, CIP, trauma, and healing through the use of lifelong learning (Murrup-Stewart et al., 2021) and reflexivity (Smith et al., 2021). The development of reflexivity as a skill should be an important focus for mental health and wellbeing practitioners, and similarly for training institutions and regulatory bodies who support practitioners in developing such competencies. Crucially, this research highlights the importance of such steps being led by Aboriginal people and knowledges.
In line with Aboriginal perspectives on CIP in health and social services settings (Bennett et al., 2011; Chamberlain, Gray, Bennet, et al., 2022; Coombes et al., 2022; Cubillo, 2021), the findings highlight the importance of practitioners in mental health and wellbeing settings utilising holistic support, whole of family and multidisciplinary collaboration, being open and flexible in their approaches, providing long-term support, and building authentic relationships. These approaches may be challenging for practitioners working within mainstream settings that provide a one-size-fits-all service (Dudgeon et al., 2014; TLI, 2018). Additionally, many mental health services in Australia are short-term, resource limited, and promote professional boundaries that may impede these aspects of CIP. This research highlights the important role practitioners play in overcoming these limitations and advocating for change. For example, to honour Aboriginal concepts of relationships, practitioners in this research challenged mainstream understandings of therapy session structures and boundaries within the client–therapist relationship. This may be a point of tension for non-Indigenous practitioners whose Western training and regulatory requirements promote professional boundaries between practitioners and clients, and caution multiple relationships (Australian Association of Social Workers, 2020, Australian Psychological Society, 2007). The findings must therefore be considered by practitioners working on the ground, and by those designing practice guidelines in relevant regulatory bodies.
Although elements of these challenges are systemic in nature and require top-down structural policy changes, the findings contribute numerous ways of overcoming these barriers, which all practitioners can embrace at an individual level. Minimally, they suggest that for effective CIP, practitioners working with Aboriginal people must build authentic relationships with community members, engage in continued learning and development, and advocate for practice improvements within their workplaces and disciplines. Without action to embrace Aboriginal ways of working and overcoming existing barriers to healing, practitioners may be complacent to inappropriate support, or contribute to delays in culturally safe and effective healing for Aboriginal children and families impacted by trauma (Milroy, 2018).
Future Directions for Culturally Informed Practice
This research provides valuable insight into how Aboriginal practitioners in mental health and wellbeing settings implement CIP in their work with Aboriginal children and families impacted by trauma. The strong focus on conceptualisation should be seen as a precursor to more detailed research on the use and effectiveness of CIP in trauma healing. As the field advances, the concepts outlined here can serve as foundational elements that guide more targeted studies on the application of these CIPs. Although some of the approaches, such as trauma-informed practice, have been subject to important exploration in existing research and practice with Aboriginal people (Atkinson 2013; Cubillo, 2021; Tujague & Ryan, 2023), other approaches, including strengths-based practice, holistic healing, and practitioner reflexivity, are less developed areas of focus in the context of Aboriginal healing. Each of the approaches identified will benefit from more in-depth exploration that was beyond the scope of this research. Furthermore, future research could employ similar Indigenous research methods to explore Aboriginal perspectives on CIP in specific disciplines or services, such as psychology, and expand existing understandings of the impact of CIP, by investigating the experiences of Aboriginal families and individuals accessing these services.
Further considerations for best practice approaches need to include the capacity of all practitioners and services to implement effective CIP. This could include appropriate resourcing for service funding, design, and delivery to enable flexible, individualised, and long-term support, that allows practitioners to fully facilitate culturally informed approaches to trauma healing. In particular, long-term and sustainable funding of Aboriginal-led services is vital for effective healing, as Aboriginal people themselves can effectively create and deliver services that embed Aboriginal ways of working, as best practice for trauma healing (TLI, 2018). Appropriate funding is also important for the development of Aboriginal-led resources and trainings that can be utilised by all mental health and wellbeing practitioners, and for overcoming practice issues such as long waitlists, capped amounts of subsidised therapy sessions, and setting up appropriate therapeutic spaces. From the Aboriginal perspectives explored in this study, more must be done to embrace Aboriginal ways of working, improve access to healing, and critically reflect on, and respond to, the needs of Aboriginal people healing from trauma in Australia.
Limitations
Although recruiting efforts were inclusive of both Aboriginal and Torres Strait Islander people, this study lacked important and possibly differing perspectives of Aboriginal men, and Torres Strait Islander people. Aboriginal men play vital roles in the cultural strengthening and healing of their communities (Aboriginal Health Council of South Australia Ltd., 2019; Prehn et al., 2021), with important research highlighting their unique healing and support needs (Bulman & Hayes, 2011; McCalman et al., 2010; Prehn & Ezzy, 2020). Likewise, Torres Strait Islander people hold unique cultural and spiritual values and experiences of trauma, that may inform different understandings and use of CIP in their communities (Lui-Chivizhe, 2022; Tickner, 2001). Future research into the role of CIP in these spaces, ideally led by members of these populations, would be greatly beneficial.
Concluding Remarks
Contrary to Western approaches to mental health and social services, which often fail Aboriginal people in Australia, it is Aboriginal ways of knowing, being, and doing, which have ensured the SEWB of Aboriginal people for millennia. Aboriginal people are best placed to inform their healing needs, as they have lived through, resisted, and survived the trauma caused by colonisation for many generations. Through the representation of Aboriginal practitioner perspectives on the understanding and implementation of CIP, this research offers detailed insight into culturally safe and effective trauma healing that is grounded in Aboriginal knowledges and culture. This research implores all practitioners working with Aboriginal children and families, to embrace Indigenous models of holistic health, engage in reflexive and responsive practice, and utilise long-term, trauma-informed, and strengths-based approaches to healing (Atkinson, 2013; Chamberlain, Gray, Bennet, et al., 2022; Tujague & Ryan, 2021). The insights gained stand to improve existing understandings and practices for culturally safe healing in Australia and beyond. Aboriginal voices, knowledges, and cultures must continue to be privileged in the efforts to heal their communities from trauma.
Footnotes
Author’s Note
The use of Australian spelling has been intentionally used throughout this article to honour the voices of Indigenous participants in this research.