
Abstract
Prior literature suggests that stress exposure is associated with elevated rates of depressive symptoms in African American adolescents. However, there is substantial within-group variability which may be attributable to differences in adolescents’ individual characteristics (e.g., self-esteem, coping styles), and interpersonal experiences (e.g., peer support). The current study first examined whether active coping, perceived peer support, self-esteem, and stress were associated with depressive symptoms. Then, drawing from the diathesis-stress, transactional stress, and stress-buffering models, we examined whether the effects of stress on depressive symptoms were moderated by self-esteem, active coping, and perceived peer support. Using a sample of African American adolescents (n = 1,163; mean age = 13 years old; 54.2% girls), we found that active coping and stress were positively associated with depressive symptoms in contrast to self-esteem and perceived peer support. Interaction results suggested that active coping and self-esteem moderated the effects of stress on depressive symptoms. Implications are discussed.
The current study’s findings supported the diathesis and transactional stress models, such that the combination of lower self-esteem and higher stress was associated with higher levels of depressive symptoms. Moreover, results indicated that active coping practices attenuated the association between stress and depressive symptoms. These results suggest that clinicians can assess and treat depressive symptoms utilizing active coping strategies and self-affirmative statements to strengthen self-esteem.Significance of the Scholarship Statement
Depression is highly prevalent during adolescence with rates estimated to be around 12% in a 12-month period (Fleming & Offord, 1990). Depressive symptoms can disrupt adolescents’ daily functioning, and are associated with deficits in academic performance, peer and romantic relationships, as well as other adverse long-term outcomes (English et al., 2016). Although the potential negative impacts of depression appear to be ubiquitous, research focusing on mental health disparities indicates that African American adolescents may not only be at greater risk for experiencing depressive symptoms but may also be more vulnerable to its effects (Tynes et al., 2020; Rose et al., 2019). Moreover, investigators have posited that stress exposure is likely to function as one of the primary developmental processes which may account for greater susceptibility to depressive symptoms among African American adolescents (Deardorff et al., 2003; Van der Wal et al., 2003). Despite the negative impacts of stress exposure on depressive symptomology among African American youth, there appear to be significant individual differences, with some youth exhibiting greater sensitivity to stress, and other youth exhibiting greater resilience. Building on this viewpoint, the primary aims of the current study were to investigate whether there are certain factors which may exacerbate or mitigate (i.e., moderate) the potential negative impacts of stress exposure on African American adolescents’ depressive symptoms.
Stress Exposure in African American Adolescents
Stress exposure during adolescence is multifaceted, and for most adolescents, stressful experiences are likely to occur in various social contexts including at home, school and in their communities. For African American populations in particular, the minority stress model and social determinants of health framework have been utilized to explain the processes in which culture and race related stressors may contribute to adverse outcomes among African American adolescents (Craig et al., 2017; Li et al., 2007). More specifically, the legacy of historical segregation and exclusionary policies have resulted in fewer socioeconomic opportunities for African American families (Wickrama et al., 2005). By extension, African American adolescents are more likely to reside in volatile environments and historically neglected communities, and these neighborhood disadvantages are likely to contribute to greater rates of poverty, unemployment, discrimination, homelessness, and societal rejection. In turn, these adverse and stressful life experiences are likely to collectively contribute to greater rates of daily stress exposure and susceptibility to depression (Kim et al., 2019; Lawrence et al., 2023a; Metzger et al., 2021; Utsey et al., 2008).
Although these perspectives highlight how African American youth may be at greater risk for stress exposure and depression compared to their White peers (i.e., between-group differences), it is also important to consider potential sources of within-group variability among African American youth. Stated differently, despite significant cultural and social risk factors, there may be individual differences in how African American youth deal with stressful experiences and their potential impacts on their mental health. Accordingly, in the current study, we evaluated multiple theoretical perspectives, as well as empirical (basic and applied) research, to identify and assess several factors which may reduce the potential negative impacts of stress exposure on African American adolescents’ depressive symptomology.
More specifically, we applied multiple theoretical perspectives including the diathesis stress perspective, transactional model of stress, and stress buffering perspectives. Integrating these theoretical perspectives with the empirical research, we were drawn by the work of researchers and clinicians who have identified several factors which appear to be particularly relevant for adolescents (as well as being potentially malleable intervention targets). First, given the salient developmental changes that typically occur in adolescence relating to autonomy and identity formation, as well as self-systems processes (Bynum & Kotchick, 2006), we evaluated the role of adolescents’ self-esteem. Second, consistent with normative advances in social-cognitive processing during adolescence and increased self-reliance, we examined adolescents coping skills. Third, given the increasing influence of peer groups during adolescence (and less reliance on parents), we also considered adolescents’ perceptions of peer support during this developmental period.
Self-Esteem
The concept of self-esteem refers to individuals’ positive and negative subjective self-appraisals (Coopersmith, 1959; Leary, 1999). Research on self-esteem has differentiated its multiple specific domains, as well as considered global self-esteem which refers to individuals' overall self-worth, in totality (Rosenberg et al., 1995). In the current study, we focus on the latter, as there is evidence that global indicators of self-esteem may be more strongly associated with psychological well-being. Prior literature suggests that adolescents who maintain positive self-evaluations of themselves are less likely to endorse depressive symptoms (Dozois et al., 2012; Kita & Inoue, 2017), and that those who negatively evaluate themselves are more likely to endorse depressive symptoms (Orth & Robins, 2013; Patton, 1991).
Self-esteem not only affects how an individual evaluates oneself, but it may also impact how an individual engages in challenging or stressful experiences (Baumeister et al., 1989; Heimpel et al., 2006). For instance, individuals with higher self-esteem are often better adjusted when encountering stressful situations (Orth et al., 2009). In contrast, individuals with low self-esteem often negatively evaluate themselves and avoid challenges to protect themselves from possible harm (Baumeister et al., 1989; Heimpel et al., 2006). Research on African American adolescents indicates that self-esteem may function as a mediator between their exposure to stress and subsequent depression (Prelow et al., 2006). Thus, it appears that self-esteem is not only associated with self-perceptions related to “readiness” to approach stressful situations; it may be an important underlying mechanism related to the linkages between stress exposure and depression among African American youth.
Building on these findings, in the current study we applied a diathesis stress perspective and examined whether self-esteem may also function as a moderator between stress and depressive symptoms. According to this perspective, individuals have dispositional traits (or vulnerabilities) that increase their susceptibility in developing psychopathology under conditions of high stress exposure (Monroe & Simons, 1991). Thus, we hypothesized that lower self-esteem would not only function as an individual vulnerability which may increase risks for depressive symptoms (i.e., a potential main effect), but that its association with depression is likely to be exacerbated under conditions of high stress exposure (i.e., a self-esteem by stress interaction effect). More specifically, African American adolescents with lower self-esteem were expected to be less confident in adjusting to stressful experiences (compared to those with higher self-esteem), which would exacerbate their depressive symptoms.
Active Coping
Coping refers to goal intended thoughts and behaviors that are used to reduce or mitigate the effects of daily stress (Carver et al., 1989). Traditionally, coping has been conceptualized as a two-dimensional construct including active and passive techniques, which have varying effects on mental health. Specifically, active coping typically refers to problem-solving behaviors, self-determination, and seeking social support from friends and family (James, 1994). In contrast, passive coping is characterized by avoiding stressors with the goal to indirectly reduce emotional tension (Suls & Fletcher, 1985). Further, individuals who use passive coping strategies often perceive that the stressor cannot be altered, thus, less motivated to engage in problem solving behaviors (Blalock & Joiner, 2000).
Understandably, when encountering stressful events, these coping strategies may have differing effects on depressive symptoms among African American youth. Prior literature applying the transactional model of stress (Lazarus & Folkman, 1987) has posited that although negative appraisals of external stressors increase emotional disturbances, active coping techniques may protect against emotional disturbances and depressive symptoms (McDonough-Caplan et al., 2018). More specifically, according to this model, stress is a response to the subjective appraisal of the internal and external precipitants of stress. When faced with stress, individuals first evaluate the relevance of the stressor (primary appraisal) and then assess their own personal resources to overcome the stress (secondary appraisal). Primary and secondary appraisal often impact coping techniques chosen by the individual, which directly influences psychological well-being (Lazarus & Folkman, 1987; Zimmer-Gembeck, 2016). Specifically, when confronted with stress, adolescents who utilize active coping techniques reported fewer depressive symptoms (Compas et al., 2004; Rodríguez-Naranjo & Caño, 2016; Yin et al., 2017). This suggests that during stressful moments, the initial appraisal of the stressor could trigger active coping techniques (i.e., problem-solving, reappraising emotions, and seeking social support) that serve as protective agents against emotional disturbances. Thus, the interactive association between stress and active coping could create a protective mechanism against depression in which African American adolescents who adopt problem-solving coping strategies increase their flexibility in adapting to stressful encounters and reduce their risks for exhibiting depressive symptoms (i.e., a coping by stress interaction effect).
Although the research on active coping techniques indicates that they are generally associated with fewer depressive symptoms (Lawrence, 2022a; Mekawi et al., 2022), research on African American populations indicates that certain types of active coping strategies may have potentially detrimental or maladaptive effects. For instance, African Americans may engage in John Henryism active coping, which is conceived as a high-effort active coping technique to deal with external stressors, particularly in the context of racial discrimination (Hudson et al., 2016; James, 1994; Jones et al., 2019). Although this technique appears to have short-term advantages, it may be particularly maladaptive among African American youth with high levels of stress due to the extensive amount of personal and cognitive resources that are required to persistently maintain this coping style. Thus, consistent with this viewpoint, we evaluated the alternative hypothesis that active coping may be positively associated with depressive symptoms in the context of high stress exposure.
Perceived Peer Support
Feelings of peer support and acceptance are often associated with positive outcomes and resilience among adolescents (Ahmed et al., 2010; Chu et al., 2010). Perhaps, this is typically the case during adolescence when peer relationships are important in prompting independence from parents and cultivating self-identity (Barber & Erickson, 2001). Moreover, it is plausible that youth who perceive their peers to be supportive are also likely to feel a greater sense of connectedness and belonging at school. Despite this reasoning, the empirical evidence establishing a link between peer support and depression remains mixed. On the one hand, prior research with African American adolescents has shown that positive appraisals or evaluations pertaining to having supportive friends are associated with fewer depressive symptoms (Lindsey et al., 2010b). On the other hand, studies have also shown that peer support independently does not predict depressive symptoms among adolescents (Operario et al., 2006; Young et al., 2005).
One possible explanation for these inconsistent findings is that perceived peer support may have a more beneficial effect under conditions of high stress. Consistent with this viewpoint, the stress-buffering hypothesis suggests that social support may attenuate the effects of stress exposure and function as a protective factor against pathogenic consequences such as depression (Cohen et al., 1983). Thus, we evaluated the hypothesis that the direct effects of peer support on depressive symptoms may be qualified by the interaction between peer support and stress (stress interaction effect), in which perceived peer support has a more pronounced (buffering) effect on depression in contexts of high stress.
Current Study and Hypotheses
The first aim of the current study was to test whether self-esteem, active coping, perceived peer support, and daily stress exposure were associated with depressive symptoms among a sample of African American adolescents. Towards this end, we proposed the following hypotheses (i.e., main effects):
Stress was positively associated with depressive symptoms.
Self-esteem was negatively associated with depressive symptoms.
Active coping was negatively associated with depressive symptoms.
Perceived peer support was negatively associated with depressive symptoms. The second aim of this study was to investigate whether self-esteem, active coping and perceived peer support moderated the effects of stress on depressive symptoms (i.e., interaction effects). Because prior literature has shown that gender variability often exists in the degree to which African American adolescents develop depressive symptoms, we also controlled for gender differences to account for potential confounding effects. Then, drawing from the diathesis-stress, transactional stress, and stress-buffering perspectives, we investigated whether the interactions between self-esteem by stress, active coping by stress, and perceived support by stress were associated with depressive symptoms. We hypothesized that higher levels of active coping, self-esteem, and perceived peer support would buffer (attenuate) the effects of stress on depressive symptoms.
Method
Sample
Data were drawn from the National Survey of American Life Adolescent Supplement (NSALA-A) 2001–2004. The NSALA-A was administered by the University of Michigan’s Institute for Social Research (Jackson et al., 2004), and consisted of data gathered from a sample of African Americans, Caribbean Americans, and non-Hispanic Whites (N = 3,570). One of the primary aims of the NSALA-A was to use data from a nationally representative survey to examine prevalence rates and effects of adolescent mental health disorders (Jackson et al., 2004). For the aims of the current study, the sample included 1,170 adolescents (Mage = 13 years) who identified as African Americans (n = 810), or Black Caribbeans (n = 360). In the sample, there were slightly more girls (54.2%) than boys (45.8%). In addition, the median family income was $38,829. Pertaining to religion, 27% reported as Catholic, 23.9% Protestant, 16.5% Pentecostal, and 13.7% nondenomination. The final sample size excluded seven respondents having no available data on the measures used in the current study (n = 1,163).
Prior to participation, informed consent was obtained from the adolescent’s legal guardian and assent was obtained from the adolescent. Interviews were primarily done face to face using computer assisted instruction in the participant’s home, and approximately 18% were conducted by phone. The interview time averaged 1 hour and 40 minutes. Upon completion, participants were paid $50, and the overall response rate was 80.6%.
Measures
Depressive Symptoms
Depressive symptoms were measured using 12 items from the Center for Epidemiologic Studies Depression Scale (CES-D) inventory (Radloff, 1977). This scale measures the degree to which individuals endorsed depressive symptoms over the past week. Example items are, “I felt depressed” and “My sleep was restless”, measured on a 4-point Likert-type scale ranging from 0 (rarely or none of the time) to 3 (most or all the time; 5–7 days). Items were reverse scored, when necessary and a mean score was estimated based on the 12 items, with higher scores indicating greater depressive symptoms (α = .71).
Stress Appraisal
Adolescent stress was measured using the Cohen’s Perceived Stress scale (Cohen et al., 1983), which measures subjective stressful life events within the last month (e.g., “In the past month, how often have you felt nervous and “stressed”?). This measure is a 14-item scale, and a sum score was estimated reflecting higher levels of perceived stress (α = .79).
Self-Esteem
Self-esteem was measured using the Rosenburg Self-Esteem Scale (Rosenberg, 1965), which is a 10-item scale, assessing global self-esteem on a 4-point Likert-type scale ranging from 1 (strongly agree) to 4 (strongly disagree). Example items are, “I am satisfied with myself” and “I feel that I have a number of good qualities.” Because the items were worded to reflect both positive and negative self-evaluations, items were reversed scored when necessary and a mean score was estimated reflecting higher levels of self-esteem (i.e., more positive evaluations; α = .72).
Active Coping
Active coping was measured using the John Henryism scale (James, 1994). This scale comprises of 12-items specifically designed for African American populations that gauge the propensity of individuals to actively cope with unique psychosocial stressors that are often experienced among African American populations. Further, the scale considers cognitive and physical rigors required to enhance commitment to achieve one’s goals (James, 1994). An example item includes, “When I am upset, I do not let emotions interfere with tasks.” Items were scored on a 4-point Likert-type scale ranging from 1 (completely true) to 4 (completely false). Items were reverse scored when necessary and a mean score was estimated representing more frequent utilization of active coping techniques (α = .70).
Perceived Peer Support
Peer support was measured using the composite score of three items that asked participants to indicate whether their friends and peers acted in supportive ways. Participants responded to each item using a 4-point Likert-type scale ranging from 1 (never) to 4 (very often). Example items are, “How often do your friends make you feel loved and cared for?” “How much would friends help you if you are ill?” and “How much would friends help you with problems?” Items were aggregated to form a composite scale score (α = .71), with higher scores indicating stronger perceived peer support.
Control Variable
Gender was measured asking participants their gender, which were measured as male = 0 and female = 1.
Analytic Strategy
First, using a multiple linear regression analysis, we examined whether self-esteem, active coping, perceived peer support, and stress were associated with depressive symptoms (i.e., a main-effects model). Second, moderation analyses were conducted by using Andrew Hayes PROCESS macro for SPSS (Hayes, 2017). In addition to the main effects model (Model 1), three models were specified which estimated the interaction effects of stress and self-esteem on depressive symptoms (Model 2), stress and active coping on depressive symptoms (Model 3), and stress and perceived peer support on depressive symptoms (Model 4). All three models controlled for gender. In these models, participants with incomplete responses were removed (n = 7); however, this represented a very small number of participants (< 1%), thus missing data was unlikely to impact the overall findings.
Results
Bivariate Correlations among Primary Constructs
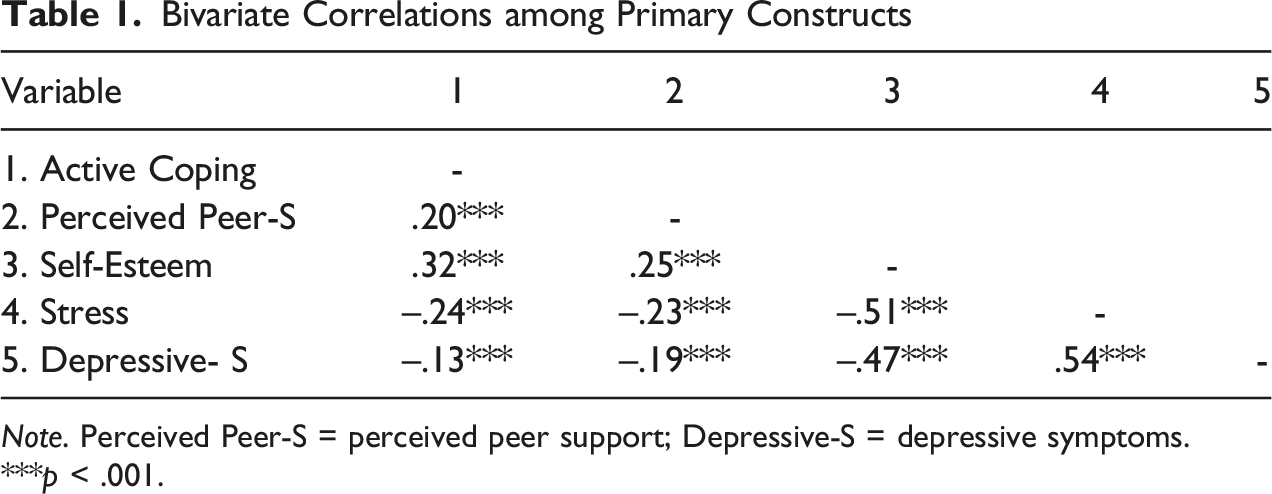
Note. Perceived Peer-S = perceived peer support; Depressive-S = depressive symptoms.
***p < .001.
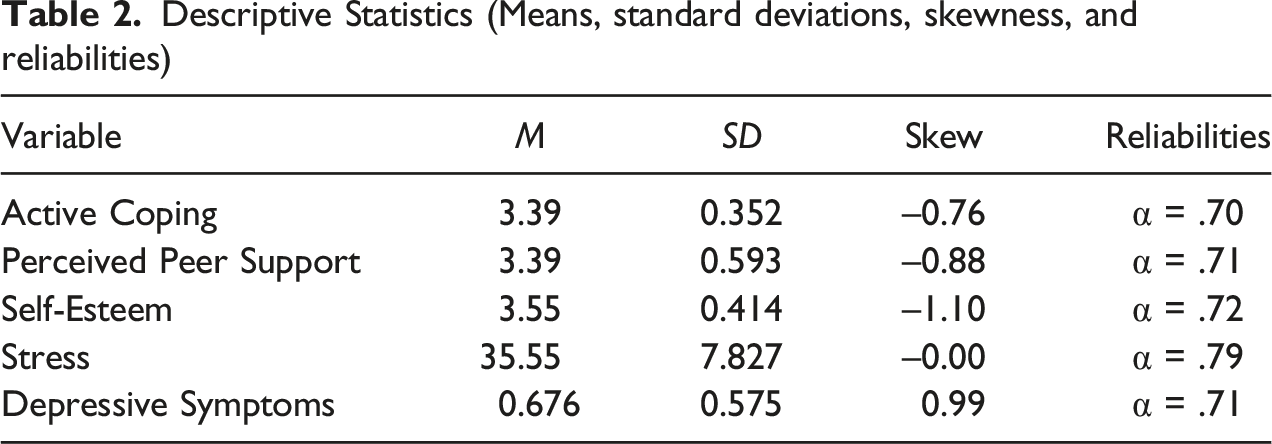
Descriptive Statistics (Means, standard deviations, skewness, and reliabilities)
Linear Regression and Moderation Results
Regression Analyses Examining Adolescents’ Depressive Symptoms
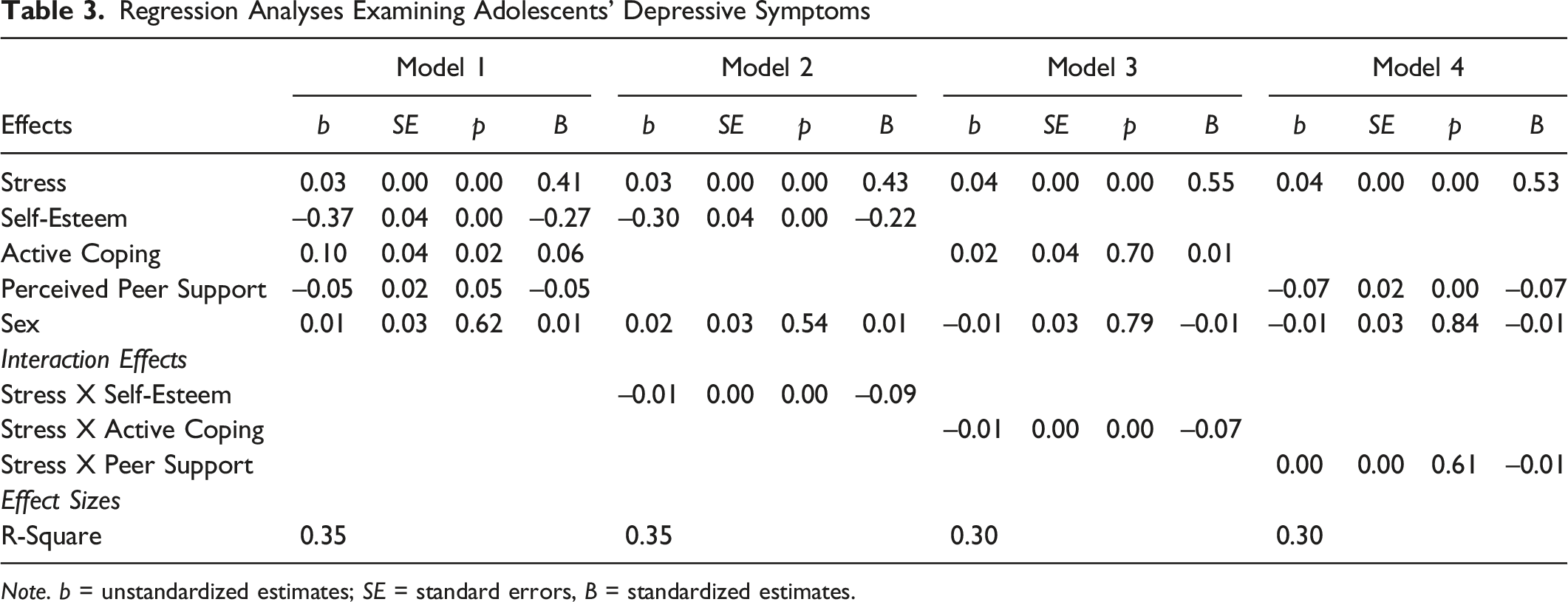
Note. b = unstandardized estimates; SE = standard errors, B = standardized estimates.
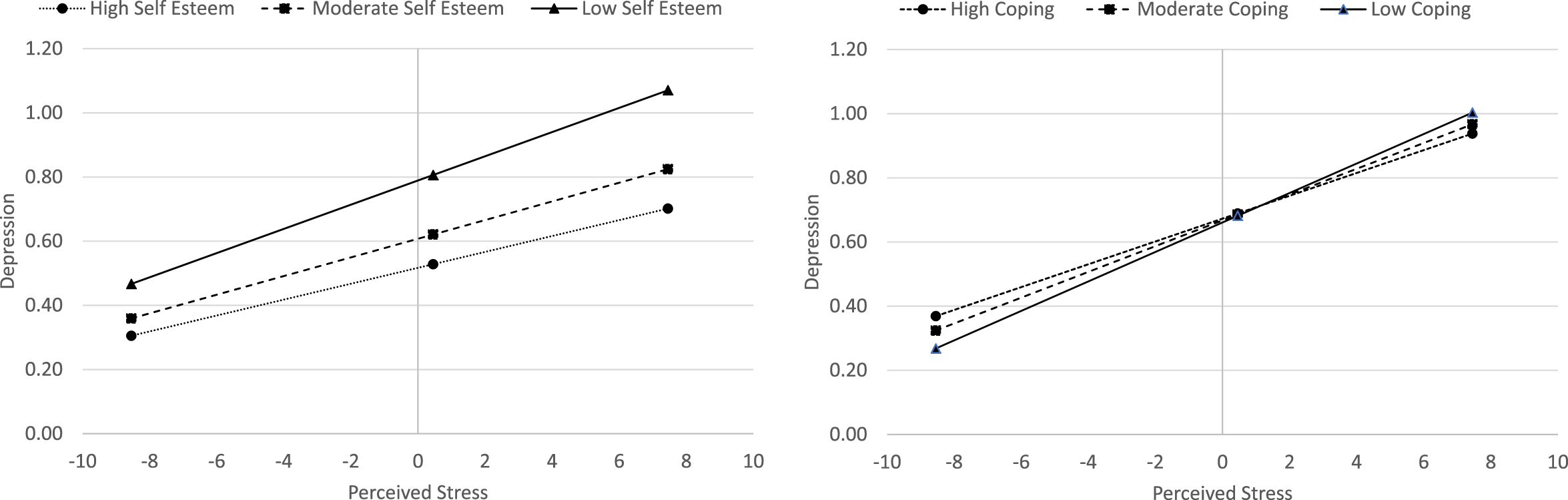
Interaction Effects Examining Effects of Stress on Depressive Symptoms at Varying Levels of Self-Esteem (1a) and Coping (1b).
Discussion
Applying multiple theoretical perspectives relating to the role of stress on adolescent’s depressive symptoms (i.e., diathesis-stress, stress buffering, and transactional stress perspectives), this study sought to elucidate how individual differences in adolescents’ self-esteem, active coping responses and perceptions of peer support functioned as protective factors and attenuated the effects of stress exposure on depression. Moreover, there has been an increasing interest among researchers and clinicians to investigate racial and ethnic disparities in adolescent mental health outcomes, and the findings of this study contribute to the growing body of research focusing on disproportionate rates of depression among African American youth. Specifically, there were two primary aims of the current study. The first aim was to test whether stress, active coping, perceived peer support, and self-esteem were associated with depressive symptoms. Overall, the results indicated that stress was positively associated with depressive symptoms, consistent with our initial hypothesis (Hypothesis 1). These findings are consistent with a large body of literature pertaining to the detrimental effects of stress exposure on adolescents’ depressive symptoms (Deardorff et al., 2003; Van der Wal et al., 2003). To expand on this general pattern of findings, and corresponding with the second aim of this study, we further evaluated whether self-esteem, active coping, and perceived peer supported moderated the effects of stress exposure on depressive symptoms. These findings are discussed below for each of these constructs.
Self-Esteem
The results provided support for Hypothesis 2, which stated that self-esteem would negatively associate with depressive symptoms. Consistent with extant evidence, African American youth with higher self-esteem were less likely to endorse depressive symptoms (Gaylord-Harden et al., 2007). Furthermore, these findings were qualified by an interaction effect between self-esteem and stress on depression. That is, consistent with the diathesis stress model, we found that lower self-esteem exacerbated the association between stress and depressive symptoms. Thus, it appears that low self-esteem may function as an individual vulnerability (diathesis) that not only has direct effects on adolescents’ depressive symptoms, but also exacerbates the effects of stress. In contrast to low self-esteem which may function as an individual vulnerability, high levels of self-esteem my confer greater individual resiliency and facilitate greater levels of confidence and self-compassion in handling stressful situations, which in turn may reduce the effects of stress on depression. During the adolescent developmental period, African American youth are particularly vulnerable to experiencing undue stress that is often characterized as the “storm and stress” period (Choe et al., 2014), our results suggest that maintaining a positive self-image could reduce the likelihood of endorsing depressive symptoms and buffer against the chronicity of stressors (Mandara et al., 2009).
Active Coping
The results were not supportive for Hypothesis 3, which stated that active coping would negatively associate with depressive symptoms. Rather, the results showed that active coping was positively associated with depressive symptoms. Although the positive association between active coping and depressive symptoms is inconsistent with the broader literature pertaining to the adaptive nature of active-coping techniques (Cong et al., 2019; Gomez & McLaren, 2006; Murphy et al., 2000), research which has focused on John Henryism (JH) active coping has been less consistent. On the one hand, several studies indicate that JH active coping is adaptive, similar to other forms of active coping (Bonham et al., 2004; Bronder et al., 2014; Jones et al., 2019). On the other hand, similar to our findings, researchers have noted a potentially maladaptive effect, positively linking higher JH active coping with depressive symptoms (Hudson et al., 2016). These findings have been attributed to the potential adverse effects of persistent high effort coping, suggesting that because African Americans often experience uncontrollable psychosocial stressors and racial discrimination, they are more at risk for exhausting their cognitive coping resources which may ultimately undermine their mental health. Notably, much of this existing research on the associations between JH active coping and health indicators has been done with samples of African American adults, and additional research is needed to investigate these associations among adolescent samples. Nonetheless, these findings suggest that JH active coping may be maladaptive for African American youth as well.
Regarding the interactions between stress and active coping, we found that greater endorsement of active coping resulted in lower levels of depressive symptoms under conditions of high stress, but not low stress. Thus, this interaction effect helps to qualify the initial (main effect) findings which indicated a positive association between active coping and depression. Stated differently, it appeared that active coping was associated with higher levels of depressive symptoms, but only when children reported low levels of stress. In contrast, active coping functioned as a buffering factor when adolescents experienced higher levels of stress. At face value, these findings seem to be at odds with the JH hypothesis which argues that prolonged high-effort coping may be associated with negative health outcomes under conditions of high stress (Bennett et al., 2004). However, it is important to note that this hypothesis has been primarily applied to adult samples, who have conceivably been engaging in these high effort practices for a considerably longer timeframe (compared to adolescents). Thus, our findings suggest that this hypothesis may not extend to adolescents, and during this period, it may still exhibit potential short term adaptive benefits (i.e., lower depressive symptoms) under conditions of high stress.
Perceived Peer Support
The results were supportive of Hypothesis 4, which stated that perceived peer support would be negatively associated with depressive symptoms. There are two possible explanations of these results. First, because anticipatory peer social support often serves as a protective factor against emotional disturbance particularly among African American adolescents (Hurd et al., 2013), the sense that peers would aid in confronting stressors, when necessary, led to fewer depressive symptoms. Second, it is possible that adolescents associated with prosocial peers who were comforting and reassuring, subsequently protecting against depressive symptoms. Consistent with prior literature, positive support from peers often negatively predicted depressive symptoms among adolescents (Ellonen et al., 2008; Holfeld & Baitz, 2020; Vaughan et al., 2010).
Pertaining to the effects of stress and perceived peer support on depressive symptoms, we found null results of this interaction. Although these results are contrary to the stress-buffering hypothesis (Cohen & Wills, 1985), the significant negative main effect of perceived peer support on depressive symptoms suggests that greater perceptions of peer support may be associated with lower levels of depressive symptoms irrespective of adolescent’s levels of stress exposure.
Implications for Practice, Advocacy, Education and Training, and Research
Considering the findings, we propose several practical, advocacy, training, research and theoretical implications. From a practical standpoint, we consider the findings from a multi-systems perspective and propose three general strategies to disrupt the pernicious effects of stress exposure on adolescents’ depressive symptoms, involving adolescent’s parents, peer relationships, and utilization of community based professional clinical or counseling services. First, family-systems perspectives highlight the importance of strategies which incorporate parents. For instance, strategies in which a healthy parent–child relationship is fostered may be essential for parents to reinforce healthy coping strategies that facilitate how adolescents cope with stressful situations (Lawrence et al., 2022; Willemen et al., 2009). Pertaining to self-esteem, as results showed that higher self-esteem could negatively associate with depressive symptoms, parents should also continuously identify positive qualities of their child, promoting self-compassionate practices, and cultivating resilience against developing depressive symptoms.
At the same time, when parents lack the internal resources or capacity to provide sufficient support for their child, a second strategy pertains to the important role of parents in locating and identifying community mental health services and clinicians who can provide additional professional supports to assist adolescents in cultivating strategies to assess and treat chronic stress (Lawrence, 2022c). More specifically, interventions can include multiple components such as mindfulness training and utilizing a coping journal, which have been shown to decrease depressive symptoms among adolescents (Kechter et al., 2019; Lawrence et al., 2022; Ramasubramanian, 2017). Furthermore, the moderation effects involving self-esteem indicated that it may also serve to attenuate the effects of stress on adolescent’s depressive symptoms. Thus, these findings attest to the need for clinicians to assess self-systems processes (e.g., self-esteem) to further evaluate whether, for example, low levels of self-esteem may be potentially exacerbating the effects of high stress.
The findings also had several practical implications with respect to stress exposure and coping. Clinicians should assess the level of chronic stress experienced by the adolescent and use evidence-based methods of coping such as problem-solving and utilizing social support agents (i.e., parents and friends), tactics which are intended to address the underlying factors causing stress (Carver et al., 1989; Lawrence et al., 2023b). These coping strategies have been shown to be effective in reducing chronic stress among adolescents (Eschenbeck et al., 2007; Grover et al., 2009). Interestingly, the findings also indicated that specific forms of active coping involving high-effort coping (i.e., JH active coping) was positively associated with depressive symptoms. Although active coping techniques are broadly viewed as being protective against depressive symptoms, it is possible that their adaptive functionality may be more limited for African American youth, and conditional on levels of stress exposure. Thus, the moderation effects could be indicative of the need for clinicians to consider individual differences in terms of therapeutic approaches. That is, the findings indicated that greater utilization of JH coping was associated with lower levels of depression for adolescents who had high levels stress, but not low stress. Furthermore, it may be important to consider whether the potential adaptive benefits are short-term, with potential long-term negative consequences (Jones et al., 2019).
Finally, as the results suggested that positive peer support was negatively associated with depressive symptoms, a third strategy pertains to increasing opportunities for positive peer support which allow youth to associate with compassionate, patient, and supportive peers. For instance, African American youth are likely to benefit from involvement with community resources that are often advantageous in building healthy social connections with peers and adults, such as the Big Brother/Big Sister programs and other community and youth serving recreational centers. Prior literature has shown that adolescents who participated in these programs reported lower internalizing symptoms, healthier self-concept, and enhanced social skills (Herrera et al., 2023).
Implications for Advocacy
In addition to these practical implications, it is critical for clinicians to engage in advocacy practices that are advantageous for their clients. More specifically, we propose several potential areas of advocacy which are both community-based and via digital technology (e.g., social media). With respect to community-based approaches, advocacy efforts should incorporate psychoeducational campaigns that are specific in encouraging mental health literacy. For instance, effective campaigns should comprise of the following aims: (a) knowledge of strategies to prevent mental disorders, (b) knowledge of community resources to prevent mental disorders, (c) knowledge of mental health-seeking behaviors, and (d) first aid strategies of assisting others who endorse symptoms of mental disorders (Jorm, 2012). Mental health literacy programs are often efficacious in assisting African American families with the effects of social strain and detrimental governmental policies (Noonan et al., 2016). Relatedly, because socioeconomic strain often serves as a barrier for African Americans to engage in mental health-seeking behaviors, which could prolong the chronicity of symptoms and increase learned helplessness (Copeland & Snyder, 2011), clinicians can advocate for legislation that promotes the implementation of cost-effective mental health agencies in underserved communities (Lawrence, 2022a).
Although the data for the current study were collected in the early 2000s and psychosocial risk factors pertaining to race, governmental representation, and the progression of interactions between Black, Indigenous, and people of Color (BIPOC) with law enforcement have changed, there are relevant implications of the current zeitgeist that could impact African American families and adolescent mental health. More specifically, because African American adolescents are disproportionality criminalized and are more likely to report contact with police officers than their Caucasian counterparts (Turney, 2021), clinicians can also advocate for prosocial interactions with the police and social justice practices that advance transparency with their local police department, which in turn could strengthen positive attitudes toward police and increase community policing practices (Lawrence et al., 2021).
Finally, prior literature has shown that racial and ethnic identity is often associated with exposure to media sites (i.e., Instagram, Facebook), which could influence peer selection and depressive symptoms among African American adolescents (Joyce et al., 2013; Tynes et al., 2012). Thus, clinicians can campaign and advocate for media coverage of positive African American interrelations that could strengthen the process in which African American adolescents associate with prosocial peers. Indeed, social media coverage could aid in enhancing self-esteem and mental health seeking behaviors (Lindsey et al., 2010a). With the rise of social media influencers, another direction of advocacy could entail utilizing social media platforms to promote psychoeducation about mental health, as well as mental health-seeking behaviors (Pretorius et al., 2022).
Implications for Education and Training
While providing specific individual and family interventions with African American adolescents and their families, clinicians should be culturally competent and have the ability to integrate relevant cultural information into the treatment plan. Though this could serve as a therapeutic challenge, there are recommended strategies for clinicians providing treatment to clients and education to students. For one, because depressive symptoms are often comorbid with conduct disorder among African American adolescents (McDonough-Caplan et al., 2018), continued education should be implemented among trainees in graduate programs, specifically in deciphering the underlying causes of internalizing and externalizing symptoms while considering the cultural functionality of their behavior. While doing so, trainees can consider the differential diagnosis, and advisors can assist in developing treatment plans that are responsive to their client’s symptoms. For two, trainees responsible for assessing and treating African American adolescents should participate in educational didactics that could assist in competency development. Pertaining to educators and psychologists responsible for providing guidance and training to trainees, it is recommended that uninformed or less competent individuals should consult colleagues and participate in continued education that could assist in addressing the training needs of trainees and their own inadequacies.
Limitations and Future Directions
There are several potential limitations of the current study, which may also provide insights for future research directions. First, although we found significant interaction effects, the effect sizes were within the small effect range. It is conceivable there are other factors which were not measured in the current study that could explain a greater variance in adolescents’ depressive symptoms, such as the parent–child relationship. For instance, prior studies have suggested that among African American adolescents who encounter chronic psychosocial stressors (i.e., exposure to community violence and discrimination), a positive and supportive parent–child relationship protects against internalizing and externalizing symptoms (Ceballo et al., 2003; Henry et al., 2015). These associations appear to exhibit larger effect sizes, which underscores the importance of the parent–child relationship on African American adolescents’ mental health. Second, because adolescents often spend a great deal of their day at school, the quality of their interactions with teachers plays a role in their functioning that could moderate the effects of psychosocial stressors on adolescent development (Lawrence, 2022b). For instance, prior literature has shown that maintaining an emotionally close and warm relationship with their teachers may serve as a protective factor associated with lower rates of depression among African American adolescents (Murray & Zvoch, 2011; Voisin et al., 2011). In sum, there are likely other moderating variables that collectively function to attenuate the effects of stress on the development of depressive symptoms among African American adolescents.
With respect to potential methodological limitations, it is important to note that the current study used a cross-sectional design, which precluded us from examining potential longitudinal associations of the primary constructs over time (e.g., to assess changes in depressive symptoms). Therefore, an interesting direction for future research may be to examine whether the moderating effects of active coping techniques and self-esteem may differ over time. Additional methodological considerations may pertain to the measurement of adolescents’ depressive symptoms. More specifically, depression is multifaceted, with various disorders that were not measured in the current study, including disruptive mood dysregulation disorder (DMDD), persistent depressive disorder (dysthymia), and substance-induced depressive disorder. As a result, our findings are less generalizable to these disorders; thus, future studies can address these limitations by exploring whether active coping, self-esteem, and perceived peer support attenuate the effects of stress on the development of variations of depression. Finally, it may also be important for future studies to further distinguish varying types of stressful experiences. Among African American youth, in particular, it may be important to distinguish experiences of racial discrimination from other aspects of daily stressors. Along these lines, an interesting direction for future research may be to examine whether active coping techniques are more (or less) adaptive depending on the type of stress that the adolescent experiences.
Conclusion
Despite these limitations, the current study added to the existing literature by testing the utility and robustness of the diathesis, transactional stress, and stress buffering models among African American adolescents. Moreover, the findings provide several implications for evidence-based practices that can be used to attenuate symptoms of depression among African American adolescents. Overall, our results suggested that increased stress and active coping strategies were positively associated with depressive symptoms. In contrast, perceived peer support and higher self-esteem were associated with lower levels of depressive symptoms. Furthermore, these findings were qualified by interaction effects in which active coping strategies and self-esteem both served as moderators and reduced the risk of stress exposure on depressive symptoms among African American adolescents. Guided by these results, advocacy, training, and future research implications were provided, highlighting strategies to assess and treat African American adolescents and their families using evidence-based interventions that are efficacious among this population.
Footnotes
IRB Statement
We used secondary data from ICPSR. Therefore, we received approval from our university institutional review board (IRB) to proceed with the study.