
Abstract
Objective:
To establish whether infants with macrocephaly and non-acute subdural hematomas (SDHs) had missed opportunities for measuring fronto-occipital circumference (FOC) and obtaining neuroimaging prior to diagnosis. Macrocephaly due to SDH in infancy is initially detected by FOC measurements and/or neuroimaging, as neurologic symptoms may be subtle or missed.
Methods:
Retrospective chart review of infants with macrocephaly and non-acute SDHs referred to child abuse pediatricians for suspected abusive head trauma (AHT) over an 8-year period. A study sample of 35 infants met inclusion criteria and had complete prior medical records which were reviewed for missed opportunities for earlier SDH diagnosis. Four types of missed opportunities were identified: not initiating a workup for nonaccidental trauma (NAT) with a history or exam finding of a sentinel injury, not obtaining FOC when presenting with nonspecific neurologic symptoms, no neuroimaging for macrocephalic infants, and incomplete or delayed workup for macrocephaly.
Results:
Most (91%) infants had missed opportunities for earlier diagnosis of macrocephaly and/or SDH. The most common missed opportunity was no neuroimaging when macrocephalic (N = 28; 54%). Other missed opportunities included not obtaining FOC on a symptomatic infant (N = 10), macrocephaly with incomplete or delayed workup (N = 9), and no NAT workup with a sentinel injury (N = 5). Most of these 35 infants (77%) were diagnosed with concerns for abuse and 43% required surgery upon diagnosis with SDH.
Conclusion:
Measuring and reviewing FOC, especially in infants with nonspecific neurologic symptoms or infants with sentinel injuries, may facilitate earlier assessment for AHT. An earlier diagnosis of AHT will assist in developing appropriate safety and treatment interventions.
Article Summary
Obtaining head circumference measurements in infants with nonspecific neurologic symptoms may facilitate earlier assessment for abusive head trauma and assist in safety and treatment interventions.
What is Known on This Subject
Neurologic signs of abusive head trauma (AHT) may be subtle or missed. These nonspecific symptoms have been well described as have delays in AHT diagnosis. Sentinel injuries and nonaccidental trauma workup are also well described.
What This Study Adds
Obtaining, plotting, and reviewing head circumference measurements for infants presenting for medical care, including those with nonspecific neurologic symptoms and/or sentinel injuries may facilitate earlier detection of subdural hematomas and management, including appropriate safety interventions.
Introduction
Abusive head trauma (AHT) is the leading cause of death among infants and young children who are physically abused.1-5 Symptoms of AHT are sometimes subtle and nonspecific and include fussiness, irritability, poor oral intake, or emesis.6-8 Infants with subtle signs of AHT may be initially misdiagnosed with gastroenteritis, accidental head injury, or infection.6,9 Diagnosis of AHT may be delayed up to 25 weeks. 9
Subdural hematomas (SDHs) are commonly associated with AHT. 10 An acute SDH may become chronic over weeks, and the intracranial volume may expand, with an accelerated growth in head circumference. Other causes of accelerated fronto-occipital circumference (FOC) measurements include expanded subarachnoid spaces, hydrocephalus, benign familial macrocephaly, and other macrosomic conditions.11-14 When AHT is suspected, serial FOC measurements can be helpful in determining a time frame for intracranial injury. Macrocephaly has been defined as FOC measurements crossing more than 2 growth percentiles 15 and as an FOC measurement greater than the 85th percentile.5,16 Neuroimaging including head ultrasound (HUS) is indicated for infants with macrocephaly.15,17
Measuring and plotting the FOC is easy, quick, and cost-free, yet not done routinely at all infant health and sick visits. The American Academy of Pediatrics (AAP) recommends measuring and plotting all growth parameters at infant health maintenance visits. 18 In infants who have developed chronic SDHs and macrocephaly following AHT, an earlier diagnosis of SDH could prevent subsequent trauma. However, there are currently no known guidelines for measuring head circumference outside of well-child visits.
Because symptoms of AHT can be subtle,6-9,19 FOC measurements could be an important adjunctive tool for identifying infants with macrocephaly that require neuroimaging as well as an assessment for abuse. This assessment should include an examination for sentinel injuries (unexplained bruising and bleeding in a premobile infant),20,21 radiographic skeletal survey, screening laboratory evaluation for evidence of visceral injury or metabolic disease, and screening tests for coagulopathy.22,23
This study aims to evaluate whether there were missed previous opportunities to diagnose macrocephaly in infants who were referred to the child abuse pediatric (CAP) team with suspected AHT. We examined previous health maintenance and sick visits to establish whether FOC was measured, neurological symptoms or sentinel injuries were documented, neuroimaging was done when FOC was >85% or crossed 2 percentiles, and whether medical and/or surgical intervention was needed at the time SDH was diagnosed.
Method
This study is a retrospective chart review of infants less than 12 months of age with non-hyperdense SDHs and a head circumference greater than 85% or that crossed 2 major percentiles. Patients were referred to child abuse specialists for concerns of maltreatment and were evaluated between November 2014 and July 2022. Hospital protocols recommend child abuse consultation for all infants with an unexplained serious injury or unexplained intracranial injury. This study met criteria for Institutional Review Board (IRB) exemption approval.
Figure 1 summarizes the selection of the study population. Initially, the Research Electronic Data Capture (RedCAP) database of all consults by child abuse specialists was searched to identify infants less than 12 months of age with an SDH, yielding 292 patients. A chart review was then conducted to identify infants with subdural fluid collections that were described as subacute, mixed density, isodense, hypodense, or chronic; those with only hyperdense SDHs were excluded (N = 163). Patients with an FOC measurement less than 85% or whose FOC measurements did not accelerate at least 2 major percentiles per the World Health Organization’s (WHO) growth curve were further excluded (N = 56). Since the goal of the study was to assess missed opportunities to identify non-hyperdense expanding SDH, we excluded 13 patients who were admitted for further workup immediately following the diagnosis of macrocephaly by the medical provider. In recording the FOC measurements, we were unable to determine whether a nurse or medical provider measured the FOC and whether measurements were validated or repeated.
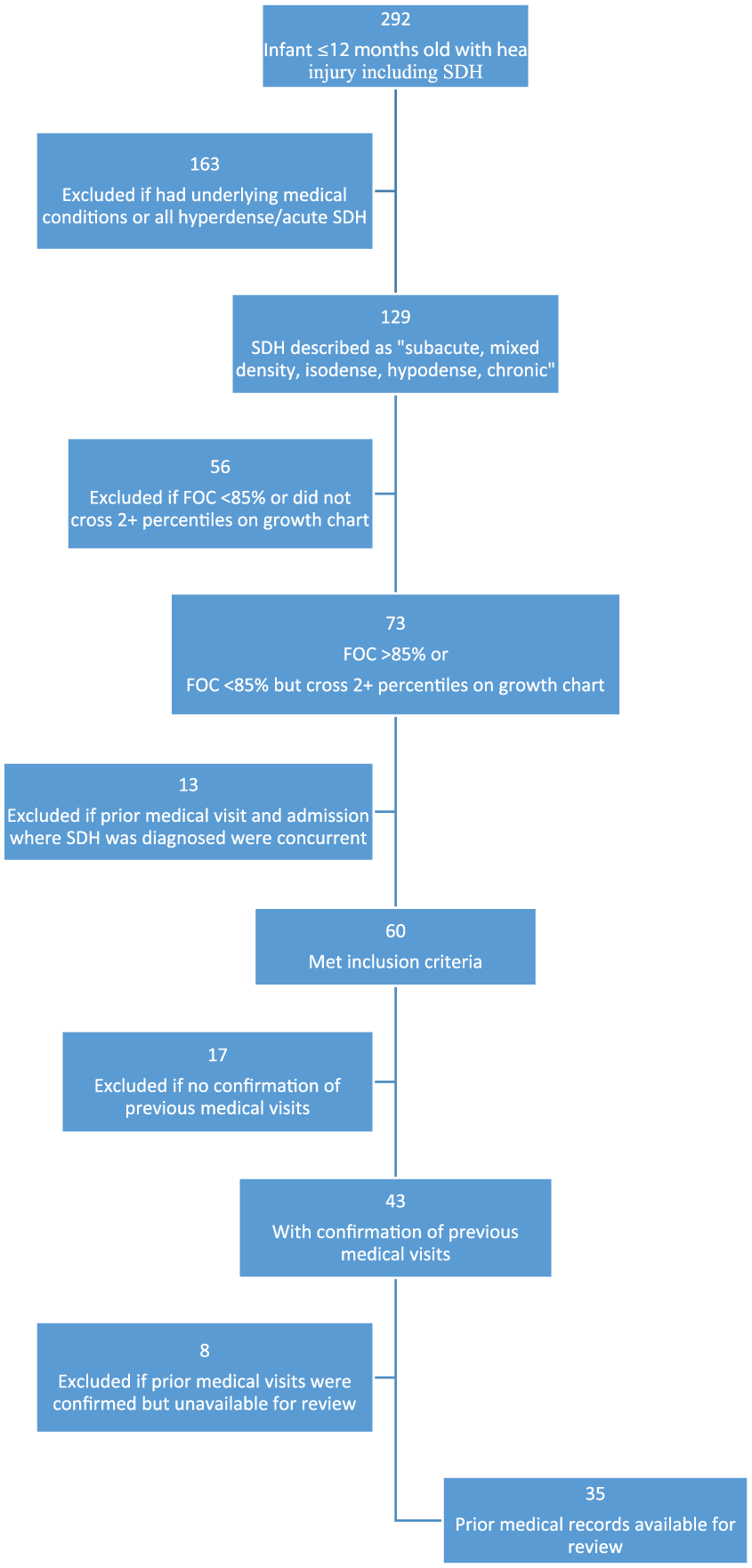
Study patient selection flowchart.
While 60 infants met inclusion criteria, only 35 had prior medical records available for review. Data extracted included: signs of abuse on admission (including bruises, fractures, and retinal hemorrhages), medical intervention (anti-epileptic medications and respiratory support), cranial surgical intervention, previous symptoms suggestive of neurological injury, and documentation of FOC during prior medical visits. Symptoms suggestive of neurologic injury were based on those described in previous studies of missed AHT.6,9
Medical records were also reviewed for documentation of sentinel injuries including bruising and intraoral injuries in a pre-mobile/pre-cruising infant when the explanation was implausible or absent.20,24
During review, we defined 4 types of missed opportunities to identify SDHs prior to diagnosis, including (1) not initiating a workup for nonaccidental trauma (NAT) when there was history or exam findings of a sentinel injury; (2) not obtaining head circumference measurement when presenting with nonspecific neurologic symptoms; (3) lack of neuroimaging when infant was noted to be macrocephalic; and (4) incomplete or delayed workup for macrocephaly. The determination of an incomplete or delayed workup was made when neuroimaging was documented as a potential next step, but not obtained due to no order placement, lack of provider follow-up, or caregiver delay or non-compliance with imaging appointment.
Results
Descriptive Analysis
Demographics
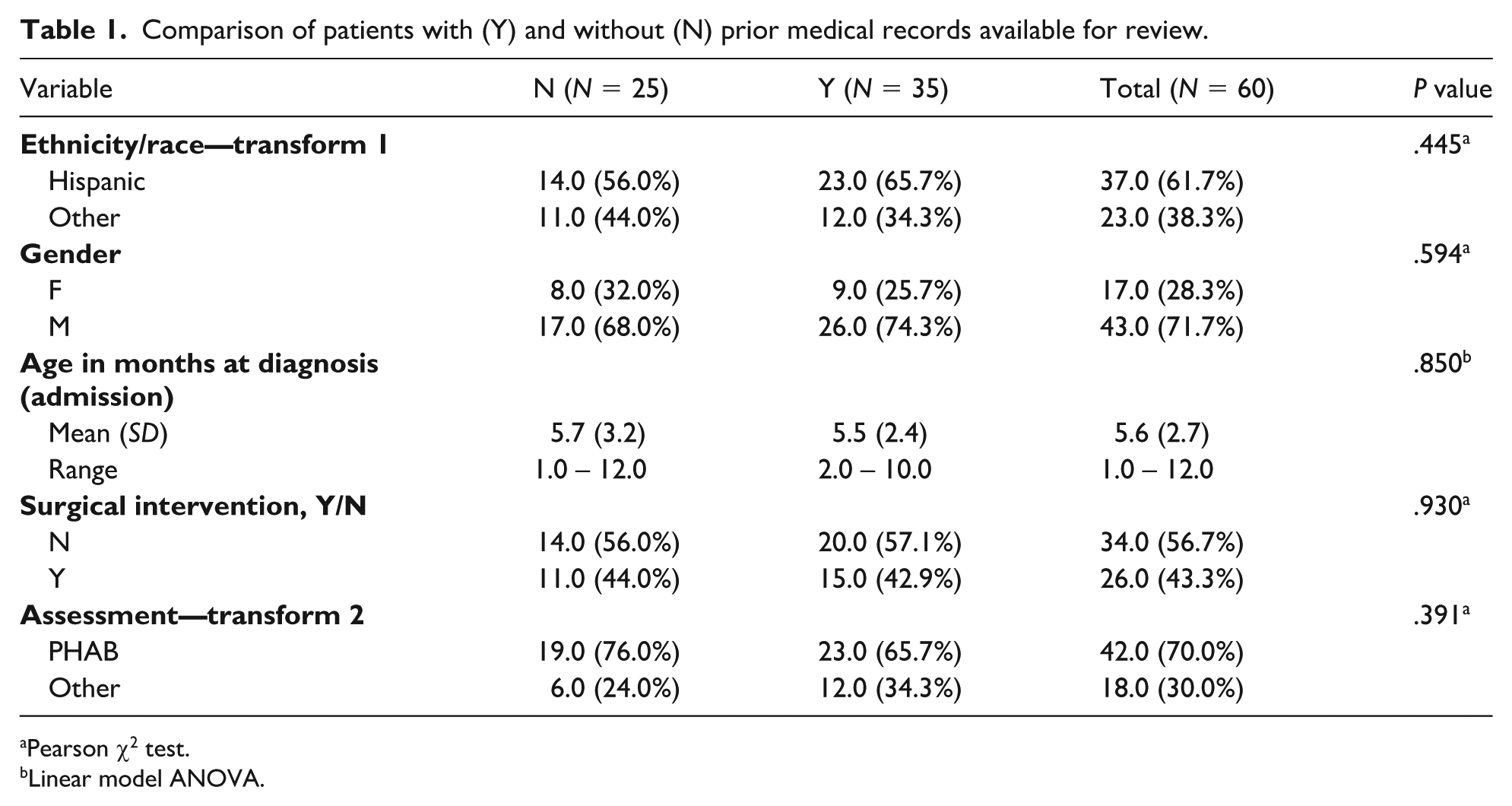
Among the 35 patients for whom medical records were available, ages ranged from 2 to 10 months old with a mean age of 5.5 months (SD = 2.8 months) at time of diagnosis with SDH. Most (26; 74%) were males. The 25 patients without medical records were not found to be significantly different from the 35 patients with medical records with regards to gender, ethnicity, age, need for surgical intervention, or level of concern for abuse. These findings are described in Table 1. Using Pearson χ2 test, it was determined that there was no statistical significance between Hispanic ethnicity compared with others (P = .445), female compared with male gender (P = .594), or assessment concerning for physical abuse (PHAB) compared with other (P = .391). There was also no statistical significance between the ages at diagnosis (P = .850) when calculated using the linear model analysis of variance (ANOVA).
Comparison of patients with (Y) and without (N) prior medical records available for review.
Pearson χ2 test.
Linear model ANOVA.
Neurologic symptoms and exam findings on admission
Most (49; 81.67%) of the 60 infants with macrocephaly and SDH and potential prior missed opportunities for diagnosis had neurologic symptoms at the time the SDH was diagnosed. Some patients had more than 1 symptom, including altered mental status (27), seizures (18), emesis (12), apnea (5), poor feeding (8), irritability (11), and “other neurologic symptom,” such as eye deviation (3). Approximately, half (31; 51.6%) had skin findings/bruises (17), fractures (15), and/or retinal hemorrhages (21) that were concerning for abuse. Fractures included ribs (6), spine (2), classic metaphyseal lesions (4), skull (5), and long bones (5). Long bone fractures were further characterized as buckle, greenstick, spiral, or comminuted. One infant had an intraoral injury and 3 had subconjunctival hemorrhages.
Interventions
Among the 35 patients with macrocephaly, SDH, and prior medical records available for review, 8 received medical intervention, 9 required surgical intervention, and 6 required both medical and surgical interventions. Only 12 did not require medical or surgical intervention.
Frequency of head circumference measurements and recommendations for neuroimaging
Up to 3 visits prior to admission were reviewed. These visits were recorded as visit 1 (visit most proximal to SDH diagnosis), visit 2 (visit preceding visit 1), and visit 3 (visit preceding visit 2).
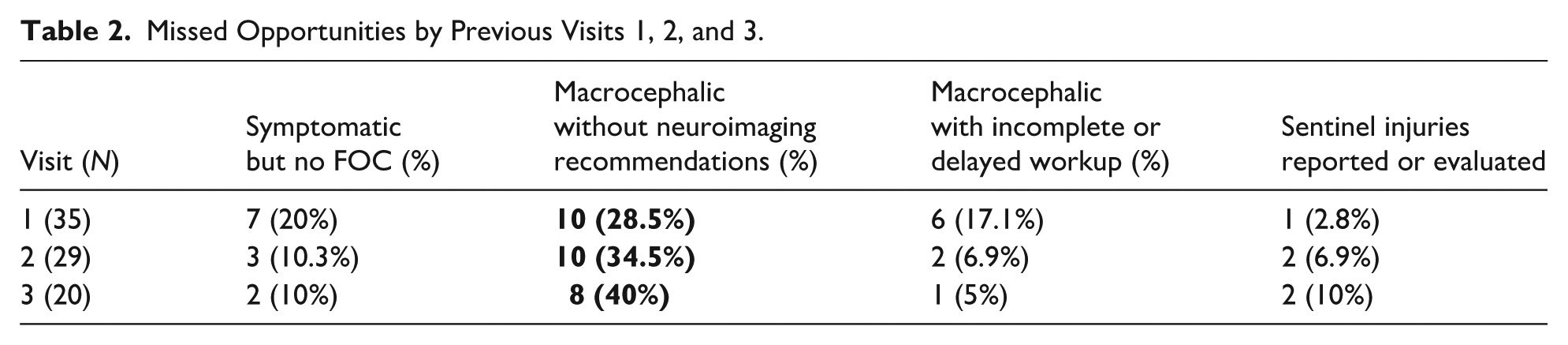
Of the 35 patients with visit 1, only 24 had FOC measured, with 17 of those measuring >85%. Of the 17 with FOC > 85%, 2 also had FOC cross 2 or more major percentiles from prior visits. Only 6 of these 17 had neuroimaging recommended by the medical provider, but none had neuroimaging completed prior to hospitalization. Two patients had FOC < 85% but had crossed 2 or more major percentiles; neither were recommended for neuroimaging. Ten patients were symptomatic but only 3 had FOC measured, and none were recommended for neuroimaging.
For visit 2, there were 29 patients; 21 had FOC measurements, with 12 measuring >85%. A plan for neuroimaging was documented for 3 of the macrocephalic infants but was not completed prior to hospitalization. In visit 2, there were 8 symptomatic patients and 5 had FOC measured; none were recommended for imaging.
At visit 3, there were 20 patients; 14 had FOC measured with 9 measuring >85%. Neuroimaging was planned but not completed for only one of the macrocephalic infants. Two infants were symptomatic, and neither had FOC measured, nor was a plan for neuroimaging documented. The above is summarized in Table 2.
Missed Opportunities by Previous Visits 1, 2, and 3.
Symptomatic patients
Twelve patients had nonspecific neurologic symptoms during a prior medical visit; none of them were recommended for neuroimaging prior to diagnosis. Symptoms included irritability (12), emesis (9), poor feeding (6), and apnea (1). Overall, 83% (10/12) symptomatic patients had a head circumference measurement on at least one prior visit with 4 measuring above the 85th percentile. Seven were symptomatic on more than 1 visit; there were 20 total visits with documented symptoms. Fronto-occipital circumference was measured at 8 of the 20 visits. These measurements were obtained at 5 primary care provider (PCP) well-child visits, 1 PCP sick visit, and 2 emergency department (ED) visits. The 12 visits of symptomatic infants without FOC measurements were 1 PCP well child, 9 PCP sick, and 2 ED.
Missed opportunities
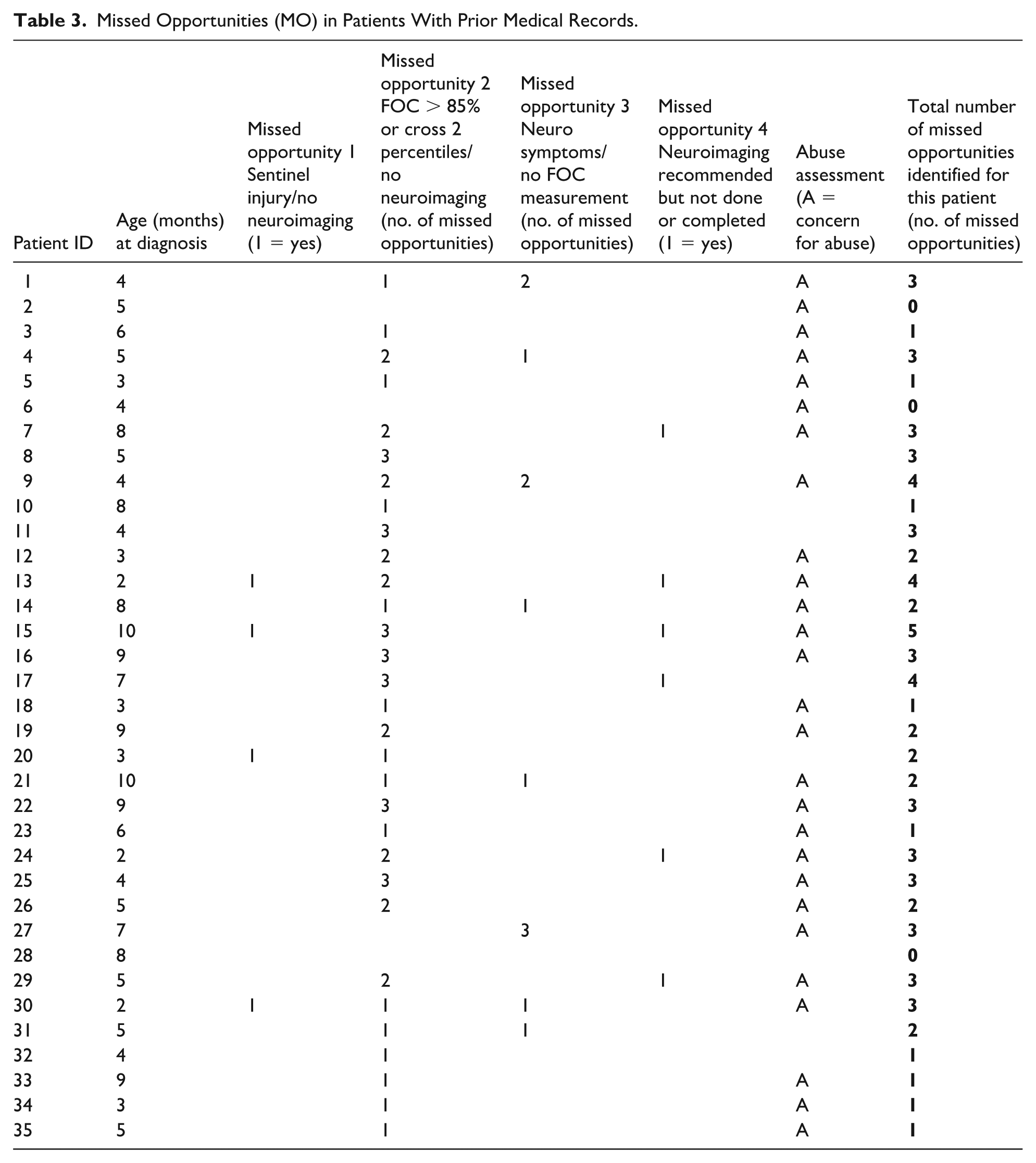
The 4 major missed opportunities for further evaluation in which SDH could have been identified sooner and further abuse potentially prevented is summarized in Table 3. The missed opportunities identified in this study included (1) not initiating a workup for NAT when there was history or exam findings of a sentinel injury; (2) not obtaining head circumference measurement when presenting with nonspecific neurologic symptoms; (3) lack of neuroimaging when infant was noted to be macrocephalic; and (4) incomplete or delayed workup for macrocephaly. In this study, only 3 patients had no missed opportunities prior to their diagnosis of macrocephaly and non-acute SDHs. Of the 27 patients with an assessment concerning for abuse, only 2 of these patients had no identifiable missed opportunities in the records reviewed.
Missed Opportunities (MO) in Patients With Prior Medical Records.
Case 13 highlights a missed opportunity with a sentinel injury
Case 13 term infant was born via uncomplicated repeat Cesarean section with an FOC of 36.5 cm (99%). She was discharged with instructions to see PCP within 3 to 5 days. Family presented to PCP at 4 weeks of age to establish care. Fronto-occipital circumference at this visit was 38.6 cm (98%) and examination findings included “linear bruise 3 mm × 7 mm on L abdomen, lateral to that 2 areas of bruising, also linear and similar size but more faded.” She was discharged home with instructions to follow-up at 2 months of age. On her well-child evaluation 5 weeks later, FOC was 44 cm (>99%). Caregiver reported persistent fussiness which was attributed to gas and discomfort from formula. Examination was notable for “normocephalic, atraumatic, wide open full anterior fontanelle, large head, closed posterior fontanelle” with “? Slight sundowning.” Due to the macrocephaly with “dramatic increase at 2 months” an HUS was scheduled for the following day with follow-up at 4 months “or pending head ultrasound visit.” Head ultrasound showed a large bilateral subdural fluid collection with mass effect. An emergent head computed tomography (CT) demonstrated mixed-density bilateral SDHs and the infant was admitted. During hospitalization, ophthalmology exam revealed bilateral multilayered retinal hemorrhages. This infant required surgical intervention. The final diagnosis for this 2-month old was PHAB.
This case illustrates a delay in arranging appropriate diagnostic imaging and therefore a suspected missed opportunity. While there were no previous medical records outside of hospitalization available for this case, parents provided a detailed history of events prior to the diagnosis of SDH.
Term infant, born at 41 weeks via uncomplicated spontaneous vaginal delivery without instrumentation. Parents reported increase in head circumference at 1 month and reported concerns to PCP at 2.5 months of age. A skull radiograph demonstrated brachycephaly with abnormal suture closures. The PCP notified the family of the X-ray results 1 week later and referred the infant for a helmet. The following week, they went to the helmet-fitting appointment where specialists notified parents that additional workup was needed. Two weeks after the specialty appointment, the PCP ordered a head CT where large bilateral subdural hygromas were noted. Primary care provider referred to neurosurgery where they were seen 2 weeks after initial imaging. Repeat head CT per neurosurgeon was completed 1 week later; then magnetic resonance imaging (MRI) was obtained a week after this CT scan. Imaging was notable for bilateral chronic SDHs. One week after the MRI, the infant was admitted for surgical intervention and nonaccidental trauma workup. A total of 9 weeks had passed from the initial skull radiograph to hospital admission. There were no other findings during NAT workup. The case for this 5-month old was assessed as nonspecific for PHAB as other explanations for the SDHs were possible.
Sentinel injuries
Of the 35 cases reviewed, 7 patients (20%) had previous sentinel injuries observed by a caregiver; most of the sentinel injuries were first documented during the evaluation that resulted in the diagnosis of SDH. The age ranges for infants with sentinel injuries, all of whom were premobile, were from 2 to 6 months with a mean age of 5.1 months.
Six infants with a history of a sentinel injury were ultimately diagnosed as concerning for PHAB. Two patients had medical provider documentation of a sentinel injury, but only 1 had FOC measured during their well-child visit. Because most sentinel injuries were reported by caregivers on admission and not all medical records were available, we were unable to completely determine if FOC measurements were obtained when sentinel injuries were present or reported. In the 7 cases where there was a sentinel injury, 71% (5) required either medical and/or surgical intervention. These cases are described in Table 4. Of note, 1 additional infant had right humerus spiral fracture at 1 month of age attributed to a 2-year-old sibling pulling on the arm, but the infant was not evaluated for abuse nor reported to child protection.
Sentinel Injuries in Infants With Macrocephaly and SDH.
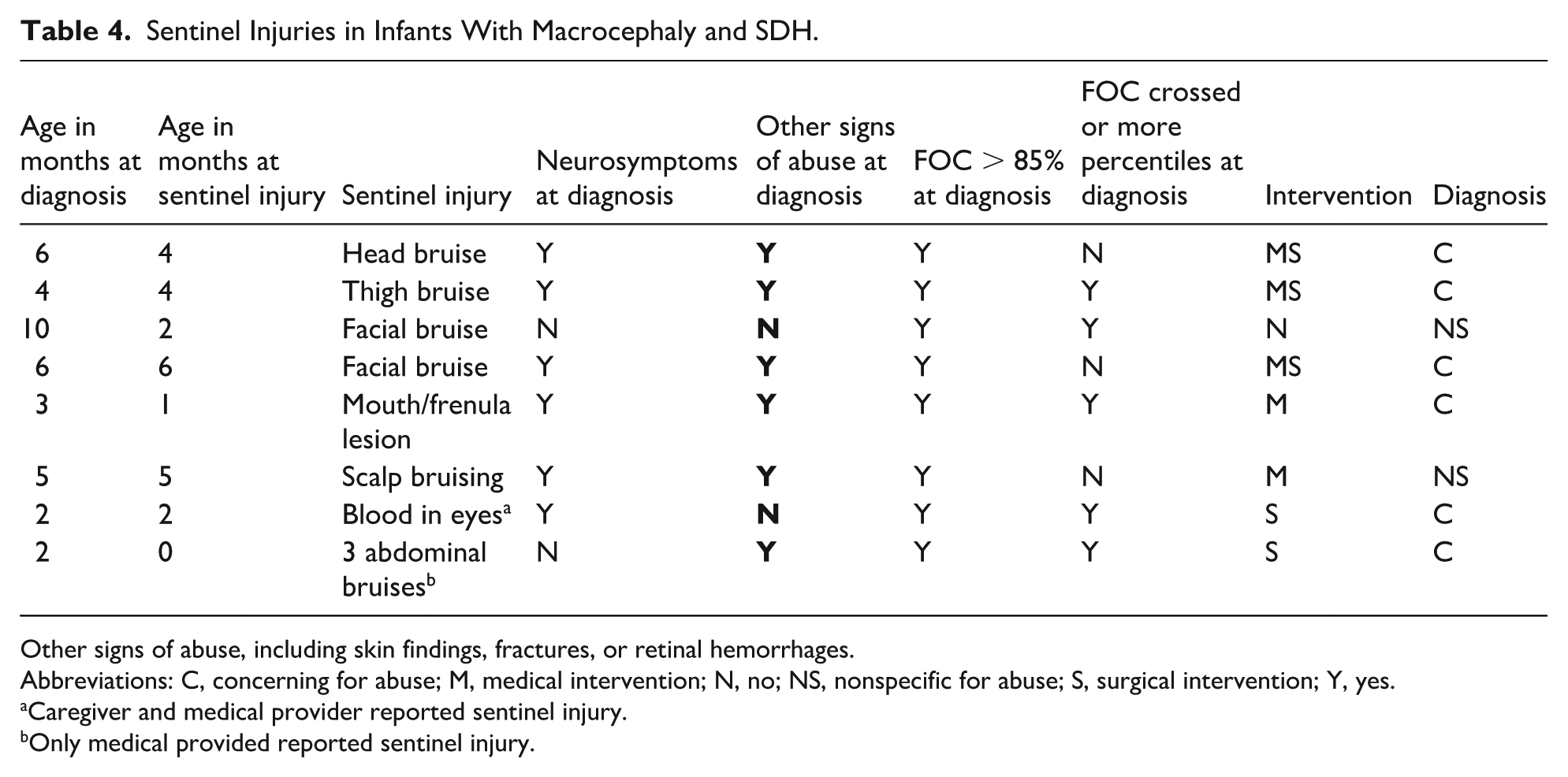
Other signs of abuse, including skin findings, fractures, or retinal hemorrhages.
Abbreviations: C, concerning for abuse; M, medical intervention; N, no; NS, nonspecific for abuse; S, surgical intervention; Y, yes.
Caregiver and medical provider reported sentinel injury.
Only medical provided reported sentinel injury.
Discussion
Most of the infants in our study sample had at least 1 missed opportunity at a prior medical encounter to measure FOC, diagnose macrocephaly, or to expedite neuroimaging, potentially delaying the diagnosis of SDH. Most (77%; 27/35) were ultimately diagnosed with PHAB. Measuring FOC in infants during medical visits and especially when sentinel injuries or subtle neurologic symptoms are present could facilitate earlier diagnosis and treatment, including safety interventions.
Few publications discuss the importance of obtaining FOC outside of well-child visits when symptoms are present. 15 While FOC measurements are recommended for health maintenance visits in the first year of life, 18 it is unknown whether these data guide decisions regarding neuroimaging, nor is it known how often FOC data are obtained at acute visits of children with neurologic symptoms. In this study, there were 2 infants who did not have FOC measured at well-child visits, although this is an AAP recommendation. Neuroimaging should be considered in infants when the head circumference grows rapidly or crosses 2 or more percentiles in a short time,15,17 when there are other concerns for abuse, including sentinel injuries,20,21 or when there are symptoms that may indicate intracranial injury.6,9 Because neurologic symptoms are often mild and nonspecific,6,9,19 and sentinel injuries are minor and sometimes dismissed,20,21 measuring and plotting head circumference may be helpful in the decision to obtain neuroimaging. In our study, most patients who were symptomatic at a prior medical visit had FOC measured and nearly half had an FOC measuring >85%, but neuroimaging was not recommended at the time. The American College of Radiology (ACR) has a published appropriateness criteria recommendations for imaging in cases of suspected child abuse which is categorized into 5 variants. Variant 3 describes recommendations for “child with 1 or more of the following: neurologic signs or symptoms, apnea. . .or injuries highly suspicious for child abuse.” Under this variant category, it is “usually appropriate” to obtain CT head without intravenous (IV) contrast and/or MRI head and cervical spine without IV contrast, in infants, such as those in our study with nonspecific neurologic symptoms. Under this variant, MRI of the complete spine “may be appropriate.” 25
The reasons for delayed neuroimaging in infants with macrocephaly are unclear. Clinicians may have delayed imaging because the data were not reviewed on a growth chart, the FOC measurement was not considered to be reliable, or because the infant appeared to be well. We were unable to determine whether FOC measurements were validated. In our study, inconsistencies regarding FOC measurements at both sick and well-child visits were noted; for example, 1 infant was symptomatic at a well-child visit and did not have FOC measured. Of the 20 previous visits where infants were symptomatic, a total of 8 had FOC measured during a sick visit (3) or a well-child visit (5). It is unknown whether these symptomatic infants without FOC measurements had macrocephaly at the time of these visits, but these visits do represent a possible opportunity for an earlier diagnosis of macrocephaly and earlier neuroimaging.
Head ultrasound is recommended to screen for intracranial pathology in asymptomatic macrocephalic infants because radiation exposure is lower and no sedation is required.15,26 However, there is no formal recommendation regarding imaging guidelines for macrocephaly per the AAP or the ACR. 27 While the recommended workup for AHT is well described, there are no current guidelines for further evaluation of asymptomatic infants with macrocephaly when subdural fluid found on HUS. 28 One study proposed an algorithm for NAT workup that includes an FOC measurement of greater than the 85th percentile. 16 Head ultrasound is considered diagnostically insensitive for detecting AHT and is not a sufficient diagnostic neuroimaging modality in suspected AHT. 29 It is recommended that infants and children with suspected intracranial injury undergo head CT, MRI, or both.28,30 As per the ACR, a head CT in infants less than 1 year of age carries a cancer mortality risk of up to 0.07%; 31 while the prevalence of AHT is unknown, mortality is 10% to 20% among infants who are diagnosed with AHT.32,33 In this study, some infants had previous HUS where subdural fluid were first detected, but all infants underwent further evaluation with head CT. Some of these patients had subsequent brain MRI which confirmed the findings of older or chronic subdural fluid collections. In addition, the gold standard for evaluation of an older appearing subdural collection is MRI as it is more sensitive than CT scans in detecting neomembranes, which are commonly associated with chronic SDHs.19,34
Sentinel injuries were confirmed in approximately one fifth of the study population. Any visible injury, however minor, in premobile infants warrants a complete evaluation for NAT, including a head CT.20,21 Identifying a sentinel injury requires close inspection of all body surfaces of the infant as such injuries can be subtle, small, and missed easily. This study supports not only the necessity for a NAT evaluation (including a head CT) in premobile infants with unexplained neurologic symptoms and injuries, but also the necessity of carefully screening for these symptoms and injuries at every visit.
Overall, 43% (26/60) of these patients required surgical intervention at time of diagnosis with chronic SDH. Only 27% (16/60) did not require either medical or surgical intervention. It is unknown whether earlier diagnosis may have prevented the need for surgical intervention, but earlier diagnosis of abusive injury could prevent repetitive abuse with rebleeding and expansion of SDHs.
There were several limitations to this study. The cases reviewed were referrals to the CAP team due to concerns for maltreatment, so that there is potential for referral bias. In addition, it is possible that not all infants with macrocephaly and chronic SDHs treated at our institution were referred to child abuse specialists or included in the study. Another limitation in this study was inconsistency in the workup an infant received when presenting with macrocephaly and/or nonspecific neurologic symptoms. In our study, not all cases identified by our inclusion criteria had prior or complete medical records available for review; however, the infants who did have prior medical records did not differ from the infants without prior records.
Conclusion
This study highlighted 4 types of missed opportunities for clinicians to identify expanding SDHs and in most cases to potentially prevent further abuse. The majority were macrocephalic infants, many with nonspecific neurologic symptoms, who presented for medical evaluation outside of well-child exams.
Current AAP recommendations include measuring and plotting all growth parameters at infant health maintenance visits. The results of this study suggest including measuring and reviewing FOC growth trends in infants less than 12 months who present with sentinel injuries or symptoms of irritability, emesis, poor feeding, or changes in alertness may result in earlier identification of those who need neuroimaging. Premobile infants should be inspected carefully and thoroughly for sentinel injuries at each medical visit, and a NAT evaluation, including head CT and FOC measurement should be considered when sentinel injuries are identified. Identifying sentinel injuries (through examination or parent history) and macrocephaly in young infants optimizes management, including prevention of further injury.
Author Contributions
MAG: Conceptualized and designed the study, drafted the initial manuscript, designed the data collection instruments, collected data, carried out the initial analyses, completed the descriptive analysis on the collected data, and critically reviewed and revised the manuscript.
NDK: Conceptualized and designed the study, drafted the initial manuscript, designed the data collection instruments, collected data, carried out the initial analyses, and critically reviewed and revised the manuscript.
WK: Completed statistical analysis on the collected data.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Footnotes
Ethical Considerations
IRB approval for Exempt Research by the Office of Clinical Research at UT Health San Antonio (protocol number 20220184EX) was granted on 05/06/2022.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.