
Abstract
HealthySteps is an evidence-based, prevention program for families of children ages 0 to 3 integrated into pediatric primary care. Our objective was to synthesize feedback on local implementation of an enhanced HealthySteps+ program from various stakeholder viewpoints to improve implementation. Qualitative data were gathered from HealthySteps+ team members (n = 14), current clinic staff (n = 15), and a focus group of parents serving on the program’s advisory committee (n = 7). Responses indicate that the core features of the HealthySteps+ program are consultations about typical and atypical child development, facilitated connections to resources, and parent mental health support. Key challenges to implementing the program include retention of skilled staff to sustain trusting relationships with parents and other providers. Based on these findings, the HealthySteps+ implementation team has increased communication with clinic staff at daily huddles, developed orientation materials for new pediatricians, and offered families additional peer support opportunities.
Introduction
HealthySteps is an evidence-based, prevention program that uses an integrated healthcare delivery model to support the healthy development of young children ages 0 to 3. HealthySteps consists of tiered services including varying degrees/combinations of the 4 components: universal screening, developmental guidance, care coordination, and short-term mental health services. 1 There has been a wealth of literature on the benefits of integrating a HealthySteps Specialist (HSS) into the primary care clinic with regard to increased healthy parenting behaviors,2,3 receipt of needed developmental referrals, 4 and preventative health behaviors like well-child visit attendance and comprehensive screening.4,5 Moreover, evidence shows the integration of HealthySteps reduces pediatric medical providers’ (eg, pediatricians, nurse practitioners) job-related stress because the HSS shares some of the workload for caring for families of young children with multifaceted needs. 6
In 2017, HealthySteps was launched at 2 urban pediatric primary care locations serving primarily African American, low-income families experiencing disparate rates of mental and physical health problems compared with the rest of the metropolitan area. 7 The program implemented at these sites, herein referred to as HealthySteps+, incorporated specific staffing features, innovative to HealthySteps at that time, to address the needs identified by pediatricians and clinic staff (via structured surveys) for parent mental health care and facilitated connections to early intervention. First, they hired psychologists as the HSS to integrate parental mental health care as well as child development expertise into pediatric primary care. As licensed mental health clinicians, HSS have the option to deliver clinic-based mental health visits for caregivers to address critical needs in areas such as maternal depression, grief and loss, as well as child behavior management. Second, Family Services Coordinators (FSCs) are part of the HealthySteps+ team and focus on helping families overcome barriers to connecting with external services to whom they are referred by pediatricians–in particular referral to early intervention services for children with or at risk for developmental delays or disabilities. Having the FSCs facilitate referrals allows HSSs to devote their time to providing on-site support services for families and has been shown to increase the rate of successful referrals.8,9
While the evidence-based HealthySteps model was selected and enhanced to address local needs, the subsequent implementation and maintenance of the enhanced HealthySteps+ program has not been measured. Frequent HSS and FSC turnover has been a significant issue for the HealthySteps+ sites, particularly during the COVID-19 pandemic, which also elevated the need to better understand implementation successes and challenges. Recent research on the implementation of similar programs into primary care sites has identified barriers at multiple levels. 10 For example, the need for reimbursement by insurers, shortage of mental health providers in the community, limited clinic space to meet with patients, lack of communication and information exchange between clinic providers, and staff burnout. 11 A qualitative study of a HealthySteps program in Baltimore, serving a racially and socioeconomically similar patient population to HealthySteps+, found that implementation successes included better utilization of families’ time at appointments and greater connection to services when co-located; areas identified for improvement were increased program staffing and funding. 6 Another qualitative study of pediatric medical providers noted that challenges to integrating a psychologist as HSS [for prevention of behavioral health concerns] included physical space constraints and need for differentiation from social workers’ domain, but the providers also emphasized the successes of collaborating with the HSS, families’ receptiveness to services, and desire for even more psychologists on staff. 12
The herein described qualitative evaluation of HealthySteps+ implementation was conducted to understand, from the perspectives of various interested parties, the core features of the program (ie, which services—both what and how—are most appreciated) and the barriers and facilitators of implementing those core features. Our guiding framework for this evaluation is the Consolidated Framework for Implementation Research (CFIR), 13 and thus we explored factors affecting implementation of the core features at the levels of the outer settings (ie, the local community and the healthcare system in which clinics are located), the inner setting (ie, the clinic context) and the individual level (ie, HealthySteps+ program staff). The insights gained from this implementation evaluation are intended to inform other HealthySteps sites (or any integrated pediatric primary care programs) preparing for or iterating on their own implementation.
Methods
This evaluation used a descriptive, qualitative, cross-sectional design to understand the perspectives of various groups involved in implementation: HealthySteps+ program staff, other clinic staff, and parents receiving HealthySteps+ services. Procedures were deemed by the healthcare system’s institutional review board as a quality/performance improvement project. All participants verbally consented for their voices to be recorded and for anonymized quotes to be used in reports.
Intervention—HealthySteps+ Program
In accordance with the national HealthySteps model and theory of change, HealthySteps+ delivers the 4 components in a tiered model, but with distinct roles played by HSSs and FSCs. All families of children 0 to 3 years of age seen for well-child care receive (1) comprehensive screening of child development, social-emotional skills, and postpartum depression and social determinants of health. Families who have elevated scores or are otherwise identified by pediatricians as needing HealthySteps+ support services are designated as Tier 2, which involves (2) consultation with the HSS including positive parenting guidance and early learning resources and (3) system navigation/care coordination (provided by FSC) for referrals to early intervention or other community resources. Families identified as needing long-term support are designated as Tier 3 and receive (4) additional mental health support [between pediatric medical visits] for parents, provided by the licensed HSS.
HealthySteps+ was implemented in 2 pediatric primary care clinics that together provide well-child care to approximately 4000 children age 0 to 3 years annually (as of July 2022-June 2023); 85% of the patients are insured with Medicaid, 7% are commercially insured, and 8% self-pay; 94% are African American, and 3% are Hispanic. During this 12-month period, the HealthySteps+ team served 766 patients in Tier 2 and 91 in Tier 3.
From December 2019 through December 2021, 1 clinic did not have a HSS and only had an FSC starting in April 2021. The other clinic was similarly without a HSS from mid-2020 through mid-2021. When not fully staffed, 1 HSS had to split time between both clinics, or, when there was no HSS at all, the FSCs were facilitating referrals to other internal mental health staff for acute parent mental health concerns. When this qualitative study began in the fall of 2022, it was the first time there was a full HealthySteps+ team (1 HSS and at least 1 FSC per clinic site) since 2019. However, since launch in 2017, each site has consistently been served by a clinic [physician] champion—a pediatric medical provider who actively promotes and advocates for the program, helping ensure successful integration by coordinating with the HealthySteps+ team and clinic staff.
Participants and Recruitment
Data were gathered through individual interviews with HealthySteps+ team members (n = 14), both past and present, other clinic staff (n = 15) currently working at both sites, and a focus group with parents serving on the program’s advisory committee (n = 7). For the HealthySteps+ program staff, eligible participants included anyone who currently or previously served as program leads, HSSs and/or FSCs. For clinic staff, the HealthySteps+ team identified specific individuals in various clinical roles—pediatric medical providers (including clinic champions) and other integrated care team members (eg, social workers, psychologists), front desk staff, and lead nurses—who had worked at the clinics during a period of full HealthySteps+ staffing (so that they would be familiar with the HealthySteps+ program).
Nominated clinic staff and HealthySteps+ program staff were invited to participate in interviews via a personalized email from the project team. Ultimately, 15 of the 38 clinic staff members who were invited completed interviews; these included 6 pediatric medical providers (including clinic champions), 4 other integrated care team members (eg, social workers, psychologists), 2 front desk staff, and 3 care coordinators. Of the HealthySteps+ program staff, only 2 could not be reached for an interview; 2 who participated in interviews had only served on the HealthySteps+ team before 2019, whereas all of the others had served during some part of the understaffed period (December 2019-mid-2021) but not exclusively during that time (ie, they had experienced some of the fully staffed period prior or after). Each participant agreed to an audio-recorded interview via Zoom (lasting between 30 and 60 minutes) and received a Target gift card of $25 after completing the interview.
To supplement the staff perspectives, a project team member attended 1 of the regularly scheduled HealthySteps+ Parent Advisory Committee’s Zoom meetings to conduct a focus group to elicit parent feedback on what was learned from the clinic and HealthySteps+ staff. The Committee was first convened in October 2020 to provide feedback on program services and consists of 7 caregivers whose children are enrolled in the HealthySteps+ program at either site. HealthySteps+ team members invite parents with whom they have built rapport to serve on the Parent Advisory Committee, which requires monthly [virtual] meetings for a term of 2 years. The goal is to maintain a committee of at least 10 members representing each of the clinic locations. For attending each meeting, participating parents are given a $50 stipend, electronically added to a ClinCard prepaid Mastercard that was mailed to them upon joining the Committee. Each parent was made aware that their participation in the focus group was completely voluntary and was given the opportunity to abstain from the meeting. Parents were informed that their responses would be anonymized and choosing to abstain from the meeting would not at all affect the care their family received. Each parent verbally agreed to having the focus group audio recorded.
Data Collection Procedures
Using a semi-structured interview guide (Supplemental Appendix A), 2 project team members trained in qualitative data collection methods conducted and audio-recorded interviews via Zoom. The parent focus group guide (Supplemental Appendix B) was developed after analysis of the HealthySteps+ program staff and clinic staff interviews, as a form of member checking.
Each interview and the focus group were transcribed through Zoom. The transcripts were anonymized, corrected for accuracy, and then uploaded into nVivo (Release 1.7.1) software for coding and analysis. The data underlying this article cannot be shared publicly due to the potentially identifiable personal opinions expressed; limited data will be shared on reasonable request to the corresponding author.
Qualitative Data Analysis
A codebook was derived deductively from the CFIR and then inductively by specifying codes related to the HealthySteps+ program and its outer settings. With the CFIR in mind (Figure 1), 4 members of the project team independently reviewed 3 transcripts each and inductively derived preliminary codes. Then, an updated codebook was discussed, refined as a project team, and subsequently used by 1 coder for each transcript (including recoding of original 12 transcripts with updated codebook).
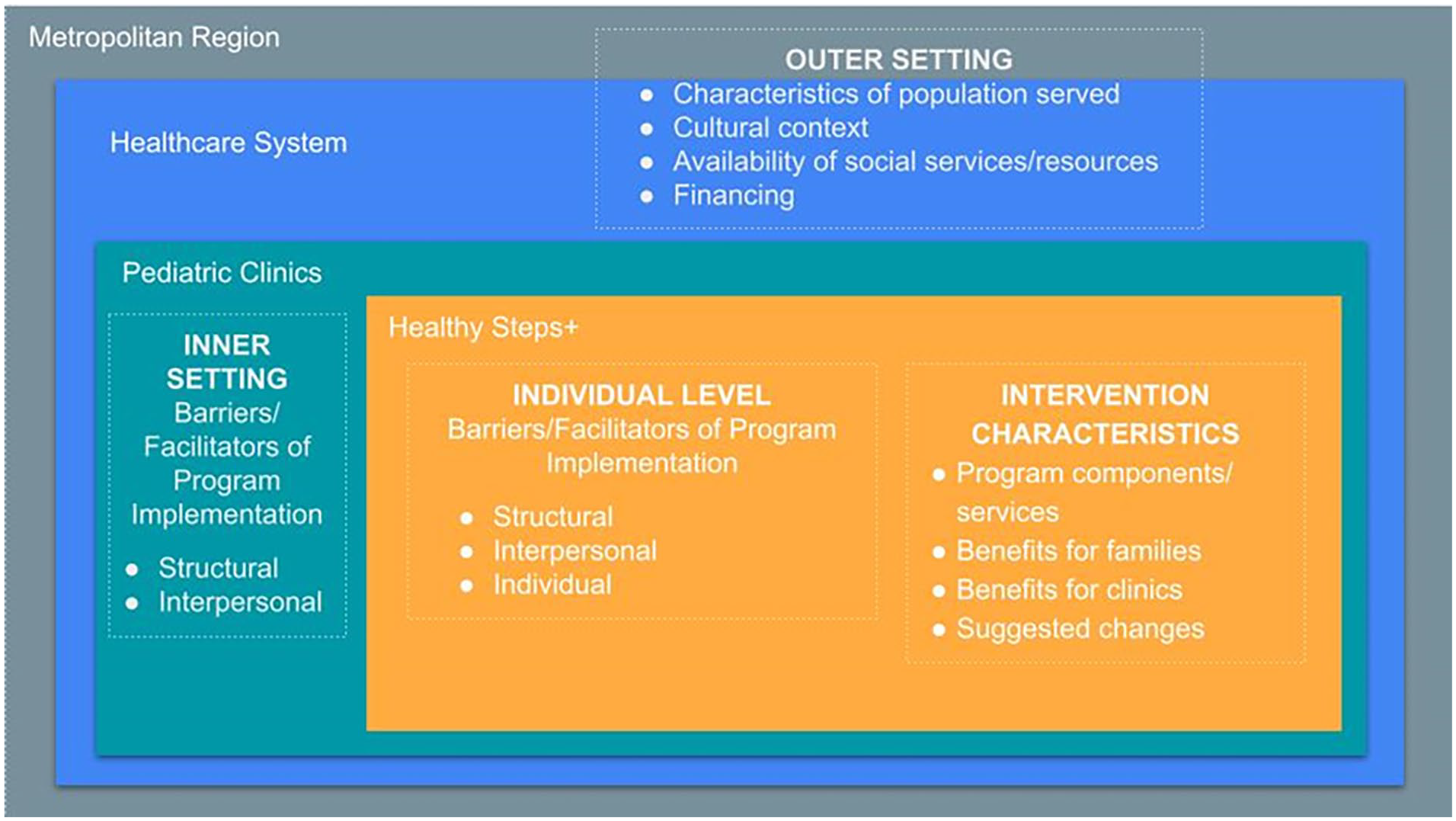
Constructs from the consolidated framework for implementation science applied to HealthySteps+ for qualitative coding.
nVivo was used to query codes with the most breadth and depth according to number of times referenced and number of participants referencing (Table 1). The coding team met to analyze themes across the 4 highest referenced codes first, and less frequent codes were reviewed in a second (17 codes) and third phase (6 codes) to identify any new themes. The themes that were noticed across multiple codes [and participant groups] are presented herein, with exemplar quotes.
HealthySteps+ Themes (By # of Participants Who Reference Themes and Total # of References Across All Participants).
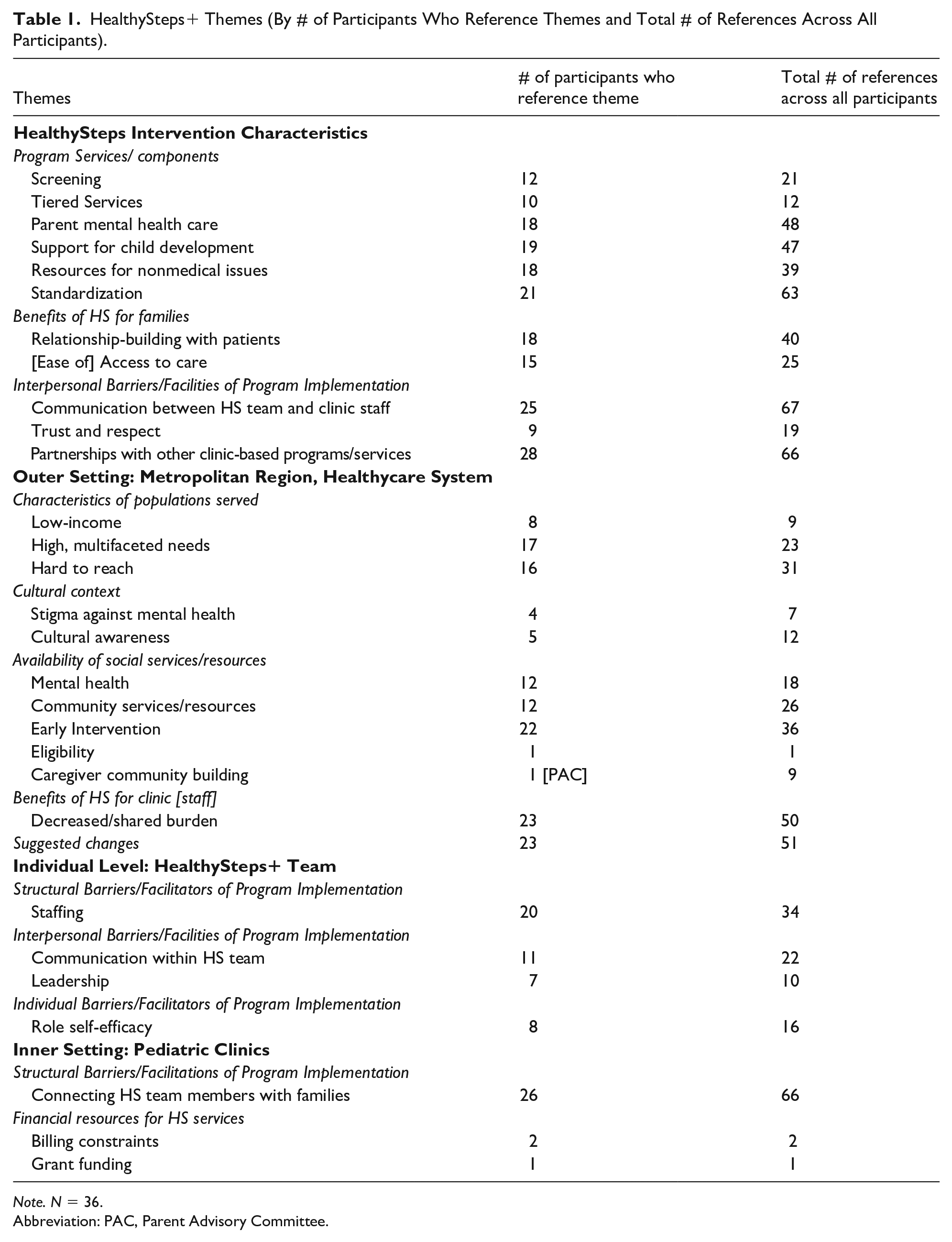
Note. N = 36.
Abbreviation: PAC, Parent Advisory Committee.
The project team attempted to minimize bias by adopting a reflexive stance and examining differences in their own experiences, training, and cultural differences from those of participants. The team also kept in mind site level differences, the larger organizational culture of the primary care network that the program operates within, and the community context, which has a long history of racial and economic disparities.
Results
The herein reported themes are organized to tell a coherent story about the HealthySteps+ implementation process in alignment with CFIR. First, looking at the program itself (ie, intervention characteristics), 2 core features were noted: specialized services pediatric medical providers are typically unable to provide and unique expertise and qualifications of the HSSs. Second, several factors in the inner setting of the healthcare clinics (eg, how HealthySteps+ services are communicated amongst clinic staff) and the outer setting of the communities served (eg, limited resources in surrounding neighborhoods) are presented as facilitators and/or barriers to program implementation.
Core Features of HealthySteps+
HealthySteps+ offers specialized services that medical providers in pediatric primary care typically do not have time or expertise to provide
There are 3 specific services mentioned by participants as uniquely available to patients because of HealthySteps+. First, consultations about typical and atypical child development, which pediatric medical providers value but often cannot provide due to time limitations. Parents appreciated the anticipatory guidance HealthySteps+ shared via handouts and a text messaging platform: My [next] youngest is 10 years old, so I forgot everything. Learning how to do all that all over, and then the little [text] messages that I get—I believe it’s like once a week or something like that—from HealthySteps. I get them messages because I gotta remember everything all over again. (HS Parent C)
The second specialized service noted was facilitated connections to resources—both goods and services. The HealthySteps+ FSCs focus on connecting referred children to early intervention providers, but they also provide families with tangible resources like diapers (stored on-site, picked up by FSCs from a local diaper bank), bottles, and for the Parent Advisory Committee, ClinCard stipends.
Third, and most often referenced by clinic staff, was the parent mental health support provided by licensed HSSs. Parents are not typically the focus in pediatric care, so HealthySteps+’s parent mental health services represent a distinct integrated care component: When I took her to her first appointment, I was kind of battling postpartum depression and didn’t want to admit it. But [HSS], she came into the room, and she asked me how was I doing. Would I be interested in the program? She also provided diapers and wipes, which helped because I was on maternity leave and pay was cut. (HS Parent E)
What the HealthySteps+ staff—individually and as a team—bring to the work is critical to the efficacy and scope of program services
What is most valued by clinic staff is the HSS’s qualifications for treating postpartum depression. What is most appreciated by parents is the HealthySteps+ team members’ ability to create a space where parents feel safe and validated. Each of these capacities affects the degree to which providers refer families to HealthySteps+ and families accept the services offered: [HS Staff] or my son’s doctor at Children’s never made me feel any type of way or never made me feel less about myself . . . they didn’t make me feel crazy about reaching out for help. (HS Parent D)
The noted key ingredient of HealthySteps+ is the social support it offers parents through relationships
The HealthySteps+ team has positive relationships with parents because they are respectful, and this in turn enhances the relationship families have with the clinic, in part by opening up communication. HealthySteps+ has also provided much-appreciated ways for parents to build relationships with each other, forming a peer network of support, for example through a pilot support group for mothers: I remember specifically like someone like they put the clipboard away. Because usually when you’re with a nurse and a doctor or provider or something like that, they have like a checklist or something. They’re looking at a computer. That’s one of my biggest pet peeves now with providers, they’re in—the first thing they do is they say “Hello” and then they look at their computer or their pamphlet or their pad. They’re not looking at you in the eyes. So that’s very important to me, like I don’t like feeling like I’m a number on your like checklist. Like look me in the eyes, look at my partner in the eyes, look at my child in my eyes, and like have a real dialogue with me as as I’m a human. Because a lot of us are taking time out of their day to make sure that we’re doing what we need to do in our pregnancy, and we’re doing what we need to do for our children. (HS Parent B) I feel like [HealthySteps] kind of makes the clinic like more of a home. I feel like it’s more homey with HealthySteps. . . I used to go to the doctors as a kid and, of course you’re a kid so you don’t think about this type of stuff, but I don’t remember anybody coming into the room talking to me, offering me things, offering my mother things, you know my parents. So I feel like it feels kind of homey that you have somebody else coming in outside of the doctor, just talking to you about your child, you know laughing with you, listening to you. (HS Parent D) I felt like [virtual parent support group] was a safe space because I was able to talk to other people. I was also going through personal issues and in the process of joining the PAC, I also lost my grandmother, and then a month later, I lost my father. So it was therapeutic for me in that time to connect with other mothers, and they were going through the same issues, or similar issues I’ll say, as I was, because I was becoming a single parent at the time. (HS Parent E)
Factors Affecting Implementation of the HealthySteps+ Core Components
Child development is closely related to caregiver mental health
Often families have multiple, interrelated needs, so attaining healthy child development requires providing support to parents. Getting families needed support is hindered by several social determinants of health: poverty and associated physical needs are more of a priority than mental health, transportation barriers limit what services they can get to, multiple caregiving responsibilities exclude self-care, and depression and anxiety symptoms in and of themselves make seeking care difficult: I hate when people tell us “oh, it’s not about you, it’s about the kid or about the family.” No, as a person, if you’re not good, you can’t be good for your child. . . (HS Parent D) It has been time where I just wanted to talk to [HSS]. But like I said, because it’s I’m taking care of a little person and an elderly person, and . . . I try to keep it on a time schedule. So it’s been times that I wanted to talk but couldn’t. (HS Parent D) Some of them, if I talk to them, and I say you can come in outside of the appointment, they’ll say, like I don’t drive, or I don’t have a way up there. They’ll say something like that, so I think sometimes for a lot of them it could be transportation. You know maybe they don’t have money to get in an Uber or get on the bus. They need to ride from someone they depended on, or something that they couldn’t, you know, get one from. (HS Staff)
Certain needed resources have limited availability in the neighborhoods served by these clinics
In terms of mental health care, parents do not get needed/wanted services due to long waitlists for therapy or only short-term therapy available, insurance restrictions, and concern that therapists will not be culturally sensitive to women of color. Co-location of parent mental health and pediatric primary care helps address access barriers and the shortage of culturally sensitive, timely mental health care in the neighborhoods surrounding these clinics. However, given the high number of 0 to 3 years old empaneled at these clinics and the high need for parent mental health care, HSS do not have the bandwidth to meet all of the long-term care needs: Even if you’re someone who has health insurance, navigating and finding someone is hard. So I think as a woman of color trying to find a therapist that understands certain things that you go through as a woman of color, and as a mother, is different. It’s not a one size fits all kind of scenario. (HS Parent B)
Also frequently mentioned was that affordable housing is a major stressor to parents of young children, and that there are few service providers thus long wait times for autism testing/treatment: Autism resources, because we have run into a lot of kids that are getting referrals for autism, and [early intervention agencies] are NOT a guaranteed resource for those children. We need other resources and other programs for autism, quite honestly. . .Because, just having [internal specialty clinic] and parents on a waiting list forever, you know, to get their kids seen, I feel like that’s really prolonging the help the child needs. (HS Staff)
On the other hand, in this healthcare system, clinics have other, often similar holistic care programs co-located with HealthySteps+
The plethora of on-site services (eg, legal, social work) is valuable to parents, even if they do not know exactly who is providing them with what. The overlap and unclear distinctions is more problematic for pediatric medical providers who can get confused about where to send referrals: So oftentimes I’ve had parents say, “we talked to social work.” Really was it social work? And I’ll look and it was HealthySteps. Or they’ll say, “the psychologist or the psychiatrist came and talked to me.” And I’ll look, and I’ll say, “Oh, it’s HealthySteps.” (Clinic Staff)
Yet the program staff themselves seem to understand how to complement and collaborate with one another regardless of who receives the referral: There is a lot of overlap between all of the other programs, too. I can’t speak to that as much. I just go to the program that I think is the right one for the person, and then they all kind of figure it out if it’s not the right one [laughs]. (Clinic Staff)
Pediatric medical providers and other clinic staff request consistent communication about what HealthySteps does
Due to staff turnover on multiple fronts—when shifting HealthySteps+ team members changes what services are available or when the clinics experience their own turnover in medical providers and/or pediatric residents—the clinic staff relies upon frequent communication from the HealthySteps+ team about who, what and how services are available: I think one thing is periodically, just them remembering that the staff changed a lot. So, being in that all staff meeting, just to kind of refresh people on exactly what HealthySteps does and what the referral does, and what they offer families. (Clinic Staff)
Pediatric medical providers also very much appreciate communication about patients they referred to understand how they can continue to collaborate to meet families’ needs: I love the closed loop feedback, because I think that builds confidence with providers that they get used to how long things take after a referral and things like that. There was a time when we weren’t getting that, and that certainly weighs on if I send someone, especially with an issue that might be sensitive like mental health concerns or case management issues, and I don’t hear back. I don’t want the patient to feel like I wasn’t listening or I wasn’t helping them. And so it’s really nice to get closed loop communication and know that [HealthySteps+] is right there on-site helping them in a timely manner. (Clinic Staff)
Clinic staff also noted that the HealthySteps+ staff’s consistent physical presence in the clinic serves as a vital reminder that they are available to receive referrals: More physical presence by the team as much as they can sit out in the pod, or really just be visibly present and just get to know everyone. (Clinic Staff)
Effectiveness of care coordination services offered by HealthySteps depends on relationships—both with community organizations and with parents
Parents prefer a warm handoff to referral sites, even if that occurs by the FSC making a phone call to the organization/service provider in the parent’s presence: Really giving a soft hand off rather than a cold hand off [to a] number, where you can really engage and say “this is ___. She’s been going through X, Y, and Z. This is what we’ve talked about so far. I think what she really needs is X, Y . . .” (HS Parent B)
Such a warm handoff is more likely to be welcomed by the referral site if the FSC has built a relationship with staff at those organizations, and such a relationship is helpful to ensure collaboration in troubleshooting any other difficulties getting families connected. For example, an early intervention intake specialist who knows the FSC is more likely to call to discuss obstacles to reaching the parent instead of just closing the referral.
A “one-stop-shop” model is the only guaranteed way to provide HealthySteps+ services
By one-stop-shop we mean the family meeting with the HealthySteps+ staff in-clinic (not via telemedicine) at the time of the child’s appointment (not at a separately scheduled visit). This service delivery mechanism is important for several reasons. First, some families may express acute needs that require immediate attention. Second, and related, needs may become less salient or superseded by other concerns once families have left the clinic. And third, remote contact methods may be unreliable, for example cell phone service being terminated or phone numbers changing: I think sometimes for me, it may be worse if I try to talk to [HealthySteps+] after the appointment. Because sometimes you may not remember everything that you need to, that you want to talk to them about. So I find it helpful that they come into the room before or after the appointment, and I get to talk to them. As opposed to me not seeing them and I go home and then I just totally forget. (HS Parent E)
Implementation Recommendations
There were several other less frequently mentioned implementation recommendations that did not meet the criteria of a cross-cutting theme but seem noteworthy for improving implementation of HealthySteps+’s core components.
Consultations are intended to take place during well-child care visits, but there are logistical challenges with regard to the timing and location of the HealthySteps+ team meeting with families. Many pediatric medical providers said they would like all young children in their clinics to receive HealthySteps services. A large part of the challenge is that there are more medical providers than HealthySteps+ staff, so HealthySteps+ cannot conduct team-based well-child visits alongside all providers seeing 0 to 3 years old patients: I would recommend that they are part of every visit, every single visit if they can be. And if they can’t, then maybe put some—because that’s a lot of visits, right. We have a lot of providers. I get that—and if they can’t, then put some, I don’t know some flags in that would identify people at the highest risk. Either hire more people into their team or they say that every patient in this zip code or every patient with this score. (Clinic Staff)
As currently staffed, pediatric medical providers often need to “call-in” HealthySteps+ staff to meet with a family as needed [instead of prospectively scheduling a team-based well-child visit], and several participants recommended use of technology, particularly asynchronous chat features (eg, Microsoft Teams) more so than electronic medical record referral documentation. Also, ideally HealthySteps+ staff would consult families in a child-friendly room that is not otherwise needed for medical encounters, but that means added time transitioning families from an exam room: Space was one of the major challenges that we faced, because, you know, pediatricians had their assigned space. Then you’re going in with the pediatrician, but then they have to exit, and they need that room for the next patient. But you’re still with that patient. So where do you take that patient and go to continue to see that patient while the pediatrician moves their next patient into the space? (HS Staff)
Another recommendation was for HealthySteps+, and the clinic generally, to engage and support fathers more: I think, making it co-ed. So I think the way you guys kind of introduce the program—I remember they specifically talked to ME about the program while my partner was there . . . [talking to fathers] also puts the onus on both parents to be on this journey together, you know, whether you’re with your partner or you’re co-parenting. I still think by having the HealthySteps person and the doctor say, like, “hey, this is something that you can benefit from.” Make sure that both people are going on their journey. (HS Parent B)
Discussion
This qualitative evaluation found that the core features of the HealthySteps+ program are the provision of specialized services that medical providers in pediatric primary care typically do not have time or expertise to provide—specifically, consultations about typical and atypical child development, facilitated connections to resources, and parent mental health support from licensed professionals. Respondents noted these specialized services depend on the particular expertise and skills of the HealthySteps+ team members as well as the relationships they build with families and clinic staff, which have also been highlighted by Hershberg and Briggs 14 in their discussion of the integrated childhood behavioral health workforce and are reflective of the Core Competencies of HSSs. 15 Our findings are also consistent with past research that shows HealthySteps implementation increases preventive behavioral health services offered to patients and families, 5 helps alleviate the time and reimbursement constraints associated with added counseling by providers, 4 and provides a holistic approach to patient care that providers alone could not easily support. 8
Participants also noted several challenges to implementing these core components—both the specialized services and delivery best practices (ie, skilled staff, relationships). First, caregiver mental health concerns add complexity to the care families need and can be a barrier to accessing services. Moreover, there is limited access to culturally sensitive mental healthcare that increases the demand for mental health services provided by HealthySteps+. While the integration and co-location of HealthySteps+ makes the services more accessible for families, there is also a challenge in distinguishing which co-located service should take the lead on case management. In addition to collaborating with other co-located services, the HealthySteps+ team has to effectively and frequently communicate with the medical providers to ensure timely and effective response to patient needs. All of this communication—amongst clinic staff and with families—is best done in-person at the time of scheduled [well-child care] appointments. 16
This evaluation adds important information when considering the barriers and benefits of HealthySteps+ implementation. First, unlike some similar studies, this implementation evaluation incorporates the feedback from multiple invested parties: HealthySteps+ team members, patients’ caregivers, pediatric medical providers, and other clinical staff. 12 Second, it was also conducted years into implementation, after multiple iterations of integrating the program into clinic workflow. COVID-19 and staffing turnovers were very disruptive to these teams, but clinic staff and parents still found many aspects of HealthySteps+ valuable to the clinical experience. Indeed, despite or because of these interruptions to implementation, participants expressed a strong preference for more on-site clinic coverage from the HealthySteps+ team.
This project also has limitations. Unlike other studies that focus on benefits of HealthySteps implementation, this evaluation does not investigate patient outcomes or parenting outcomes.6,12 These data are purely qualitative and do not attempt to quantify the amount or quality of the intervention.
Conclusion
In reflecting on the feedback in this qualitative evaluation, the HealthySteps+ team has already been strategizing how to amplify the program benefits and overcome implementation challenges. To continue culturally sensitive parental support and elevate racial equity, the team has prioritized developing parent leadership within the Parent Advisory Committee and has begun offering peer-to-peer support in Parent Cafés, with host training offered to HealthySteps+ parents and plans to intentionally recruit fathers. They are also restarting a virtual support group for mothers which was previously piloted in these clinics. 17 To continue to clarify role definition, increase visibility of the team within the clinic, and remind medical providers of program workflows, the HealthySteps+ clinic champions are increasing the frequency of reminders/awareness/advertising of the program offerings to clinic staff through email and daily huddles. The HealthySteps+ team has also developed a brief presentation to orient new clinic team members (eg, pediatricians, interns) to the HealthySteps+ program. To continue to increase confidence in the program and encourage engagement, monthly staff meetings are used to share data on referral outcomes. Future studies will measure the effectiveness of these program enhancements, especially peer-to-peer supports, and quantitatively assess the impact HealthySteps+ core features have on young children and their families.
Author Contributions
Stephanie J. Mitchell contributed to conception and design of the study as well as analysis and interpretation of data, drafted the manuscript, gave final approval and agrees to be accountable for all aspects of work, ensuring integrity and accuracy. Karan Buddala and Amanda Feinberg contributed to conception and design of the study; contributed to aquisition, analysis and interpretation of data; drafted the manuscript; gave final approval; and agree to be accountable for all aspects of work, ensuring integrity and accuracy. Deborah F. Perry, Claire Boogaard, and Nia I. Bodrick all contributed to conception and design of the study as well as interpretation of data, critically revised the manuscript, gave final approval, and agree to be accountable for all aspects of work, ensuring integrity and accuracy. Sophia Lavie contributed to aquisition and analysis of the data, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of the work, ensuring integrity and accuracy.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228251370564 – Supplemental material for Qualitative Evaluation of HealthySteps Implementation in Urban Pediatric Primary Care Clinics
Supplemental material, sj-docx-1-cpj-10.1177_00099228251370564 for Qualitative Evaluation of HealthySteps Implementation in Urban Pediatric Primary Care Clinics by Stephanie J. Mitchell, Karan Buddala, Amanda Feinberg, Sophia Lavie, Deborah F. Perry, Claire O. Boogaard and Nia I. Bodrick in Clinical Pediatrics
Footnotes
Ethical Consideration
The Institutional Review Board of Children’s National Hospital waived the need for ethics approval and patient consent for the collection, analysis and publication of these anonymized data for this noninterventional study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the J. Willard and Alice S. Marriott Foundation and the A. James and Alice B. Clark Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due their qualitative nature but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.