
Abstract
Children with congenital heart disease (CHD) often experience limited physical activity due to protective behavior from parents and physicians. This study aimed to assess whether physical activity remains insufficient in children post-CHD treatment. A descriptive study was conducted with 40 children aged 9 to 14 years who had been treated for CHD at least 12 months prior and were clinically stable without medication. A control group of 40 healthy peers was included. Physical activity data were collected using a demographic form and the Physical Activity Questionnaire adapted to the Turkish language. The patient group reported significantly lower engagement in running (P = .013) and gymnastics (P =.014). Also, the difference between the groups in terms of their degrees of engagement in physical education classes in the last 7 days was significant (P = .001). Despite being free from heart disease, these children demonstrated limited physical activity, which in turn underscores the educational objective of enhancing encouragement to foster greater physical engagement.
Introduction
The significant advancements in surgical and interventional treatments for children with congenital heart disease (CHD) in recent years have led to a noticeable increase in their survival rates and life expectancy. 1 That is why many pediatric CHD patients can reach adulthood. Physical inactivity, which is a global problem, becomes more prominent in patients with CHD. On top of that, these children’s parents and physicians are overprotective. 2 Hence, their concerns may limit the children’s physical activity regardless of their having received treatment.
Consequently, these children adopted a sedentary lifestyle. Therefore, as a part of the clinical follow-up program of children with CHD, it is recommended to routinely assess their physical activity levels and provide them with physical activity counseling sessions accordingly. 3
Some studies have objectively assessed the daily physical activity levels of children with CHD using various devices.3,4 However, such assessments are difficult and costly.
For this reason, as an inexpensive alternative to the objective measurements of physical activity, questionnaires are usually administered at home or in the hospital. Despite having some limitations, well-designed questionnaires are capable of even measuring teamwork skills in team sports.5-7 One of these questionnaires is the Physical Activity Questionnaire for Older Children (PAQ-C). 8 Studies in the literature using PAQ-C have been conducted with pediatric CHD patients. In contrast, this study aims to use PAQ-C to measure participation in sports and physical activities’ levels among children who had received treatment for CHD at least 1 year prior to the date of the study and did not have any clinically relevant residual heart problems.
Material and Methods
The aim of this study was to evaluate the self-reported physical activity levels of children in the age group of 9 to 14 years who had received treatment for CHD at least 1 year prior to the date of study. None of the children had any residual cardiac lesions, which would affect their physical activity. Also, their complete blood count and brain natriuretic peptide (BNP) levels were normal. Patients who received surgical/invasive treatment within 12 months prior to the date of the study were not involved in this study. Also, patients who had a condition that would impair their physical activity were excluded (ie, Down syndrome, etc).
This study included a total of 80 children aged 9 to 14 years, of whom 40 children were treated for CHD and the rest of participants were healthy children who admitted to pediatric outpatient clinic. Neither the control nor the study group was informed about the study or encouraged to do physical activity in order to avoid bias between groups.
Among the participants who agreed to take part in this study, we ruled out the ones with any physical or mental deficits that could affect physical exercise, any chronic diseases of other systems (eg, allergic, neurological, renal, and gastroenterological), and any residual heart problems.
The purpose of this study was explained to participants and their families, and their consent was acquired. Thereafter, PAQ-C was administered to the participants, which was developed by Kowalski et al 4 and adapted to Turkish and tested for validity and reliability by Sert and Temel 5 and Erdim et al. 7
The PAQ-C has 9 main items designed to examine the physical activities performed by the child and the frequencies of these activities in the last 7 days. This questionnaire investigates if the child has performed any of the questioned activities (eg, hopscotch, football, basketball, and gymnastics), participation in physical education classes, activities performed during recess, lunch breaks, after school, in the evening and in the weekend, and activities in their spare time (sports, play, dancing, and other physical activities).
There are 5-point Likert-type items that specify the frequency of behaviors. The first item includes 21 activities (eg, hopscotch, football, basketball, and gymnastics). The frequencies of these activities are scored based on the response options of “did not do it (1), did it 1-2 times (2), did it 3-4 times (3), did it 5-6 times (4), and did it 7 times of more frequently (5).” The scores of all activities are added together and divided by the number of activities (21) to determine the item score.
The scores of all 9 main items are added to obtain the total score of the respondent, which ranges between 9 and 45. Item 10 of PAQ-C is not included in the scoring. This item is designed to exclude responses from participants who have had a reason which prevented them from involvement in physical activity in the last week. The form takes approximately 40 minutes to complete.
This study was in compliance with the “Declaration of Helsinki” and was approved by the Ethics Committee.
Statistical Analysis
The collected data from the participants were analyzed using the SPSS (Statistical Package for the Social Sciences) 20.0 package program. Descriptive statistics including frequency analysis, Student’s t-test, and chi-squared test were used in the analysis. Skewness values were checked to determine whether the data were normally distributed. According to the assumption of a skewness range of ±1.5, the data were found to be normally distributed. The level of statistical significance was accepted as P < .05.
Results
The diagnoses of the patients in the patient group before their treatments were ASD in 16 participants (40%), TOF in 7 (17.5%), VSD in 6 (15%), AVSD in 4 (10%), aortic stenosis in 2 (5%), aortic coarctation in 2 (5%), PDA in 2 (5%), and pulmonary stenosis in 1 (2.5%). Table 1 shows the descriptive characteristics of participants.
Demographic Characteristics of the Participants.
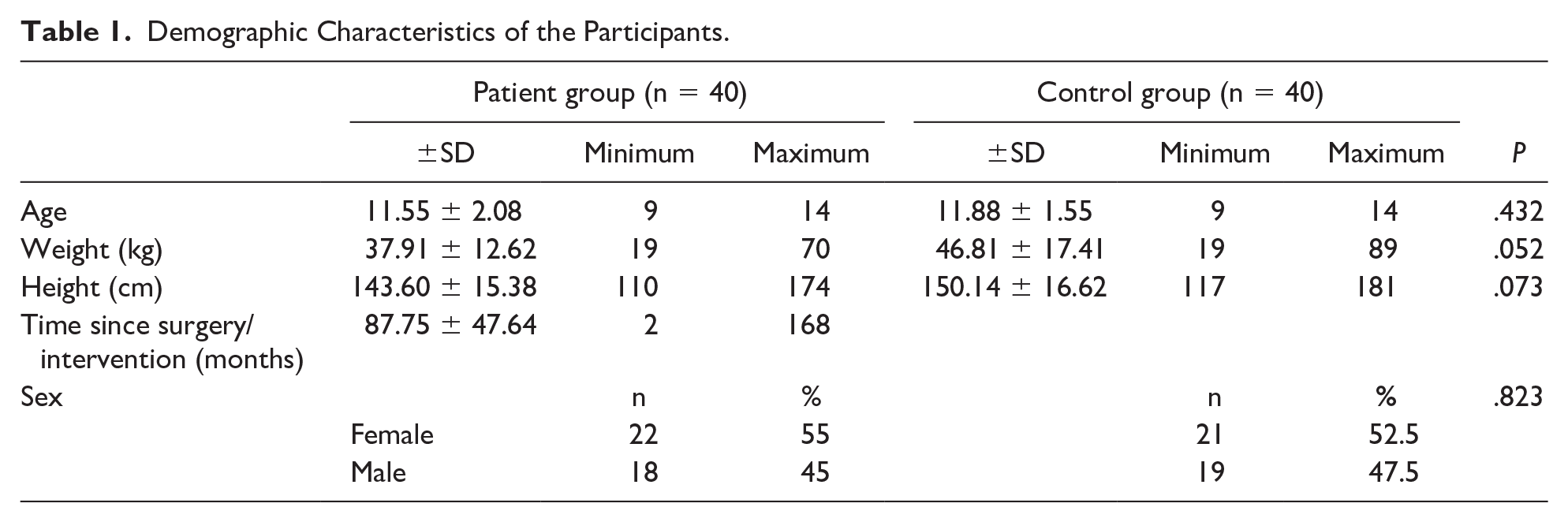
The mean follow-up duration of the patient group after their treatments was 7.3±4 years (range: 0.2-14.0 years). A significant difference was found between the groups in terms of their levels of participation in physical education classes in the last week (P = .001) (Table 2). While 23 participants in the control group stated that they participated in the entirety of their physical education class in the last week, 12 participants in the patient group reported that they hardly ever participated in their physical education class. While 42.5% of the patients stated that they almost never attended physical education classes, this rate was found to be 12.5% in the control group. Although there is no significant difference between the groups in terms of total PAQ-C score, it is observed that the patients do intense physical activities such as “jogging or running” (P = .013) and “gymnastics” (P = .014) less frequently than the control group (Table 3).
Physical Education Class Participation Statuses of the Participants.
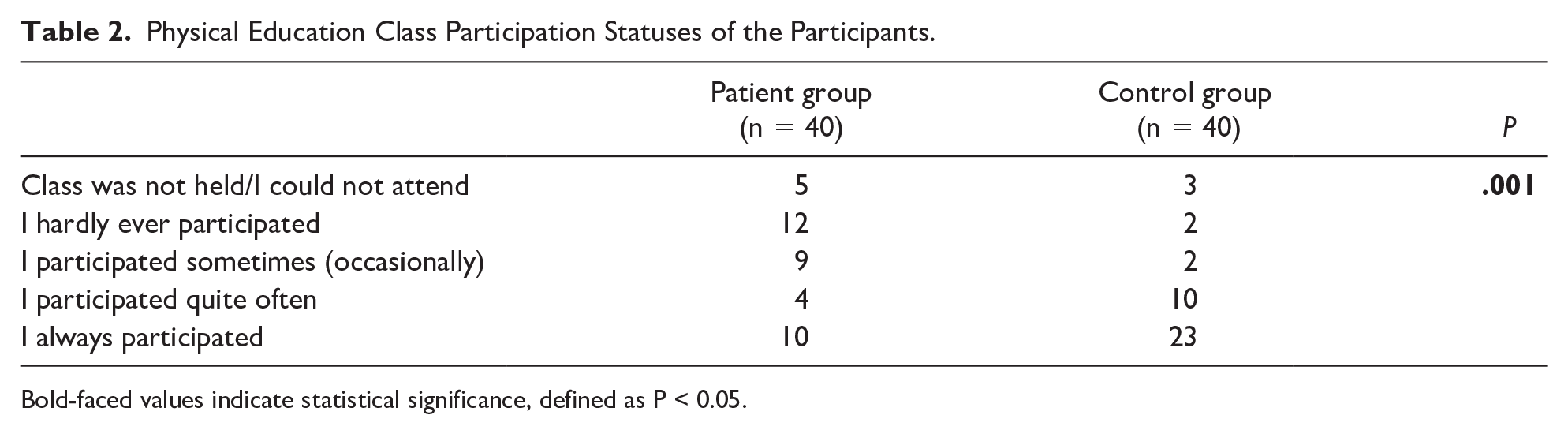
Bold-faced values indicate statistical significance, defined as P < 0.05.
Comparison of the Activities of the Participants in the Last 7 days.
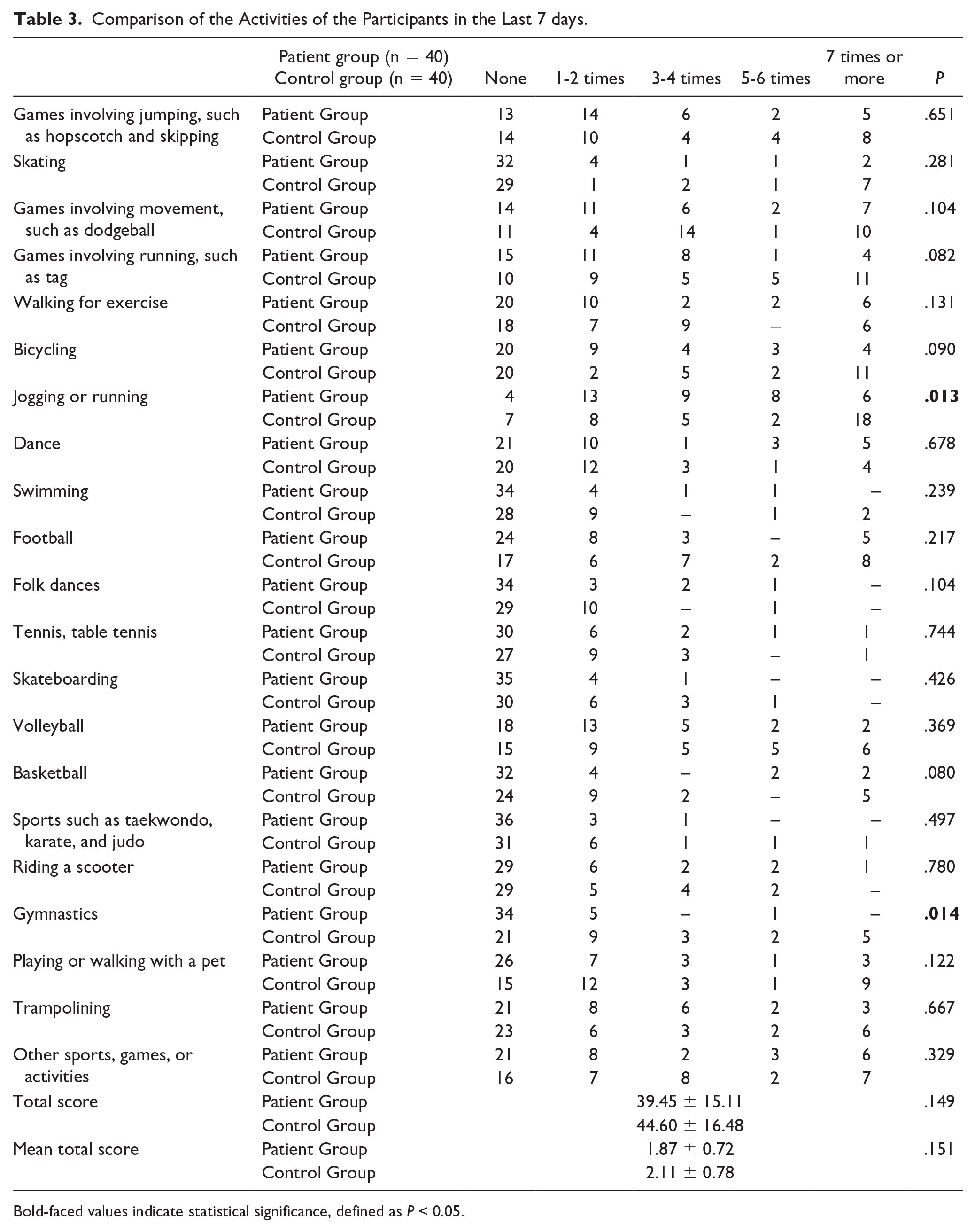
Bold-faced values indicate statistical significance, defined as P < 0.05.
Regarding the activities they did during the lunch break other than eating, 20% of the participants in the patient group stated that they ran and played more or less, while this rate was found to be 47.5% in the control group (P = .024) (Table 4). Although there is no significant difference between the control group and the patient group in terms of self-reported physical activities’ intensity on weekdays, it is seen that the control group showed more intense physical activity on Saturdays (P =.047) and Sundays (P = .046) (Table 5). No significant difference was found between the patient and control groups based on their physical activities after school or in their spare time (P = .05).
Comparison of the Activities of the Participants Other than Eating During their Lunch Break.
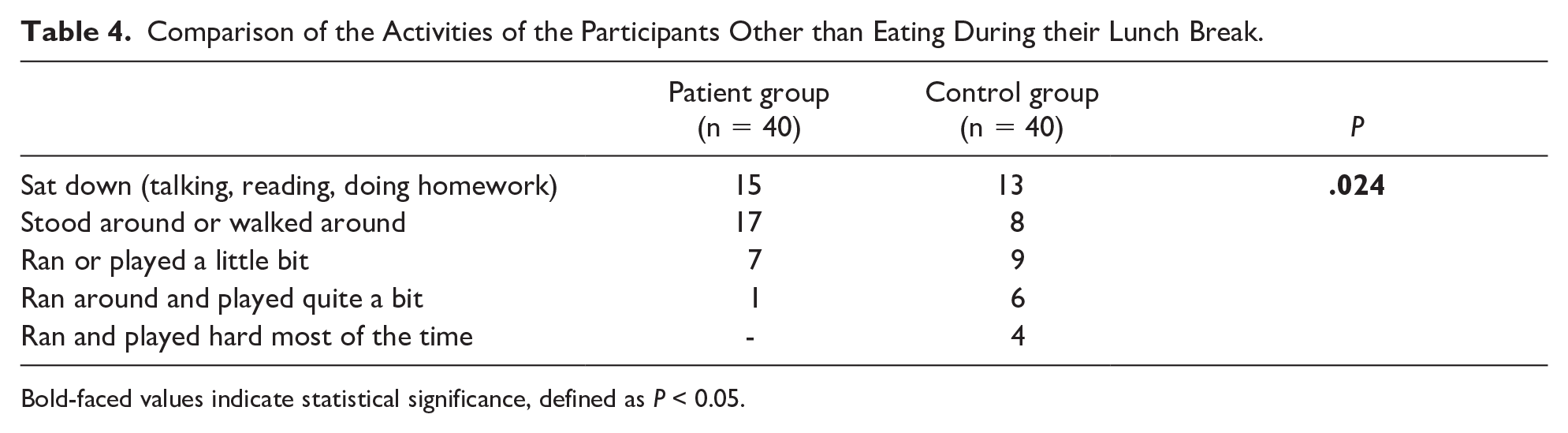
Bold-faced values indicate statistical significance, defined as P < 0.05.
Comparison of the Participation Frequencies of the Participants in Sports, Games, Dance, and Other Activities Throughout the Week.
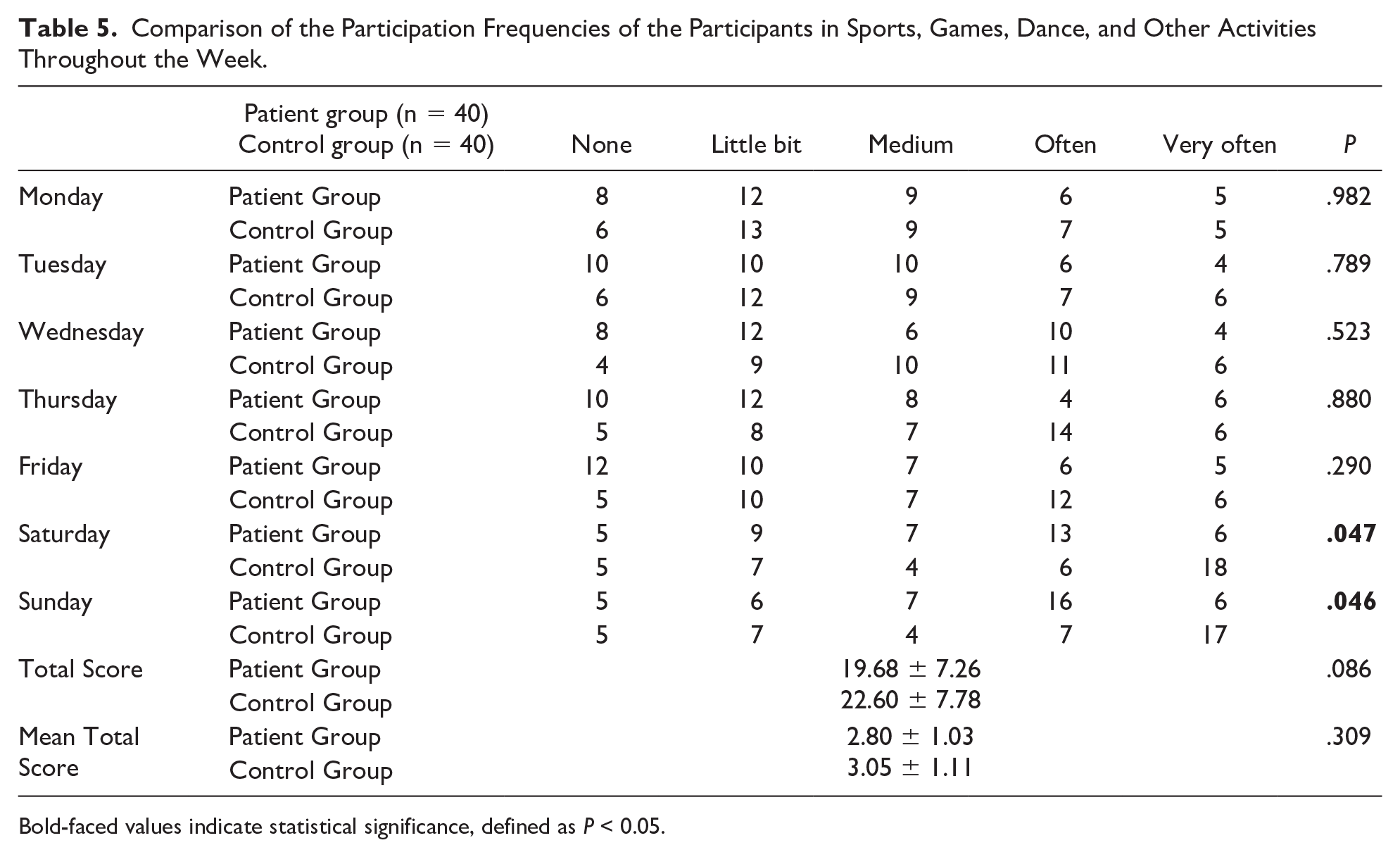
Bold-faced values indicate statistical significance, defined as P < 0.05.
Based on the assessment of whether the participants had any reason in the past week that had affected their physical activity, including sickness, the 2 groups were not significantly different (P = .05).
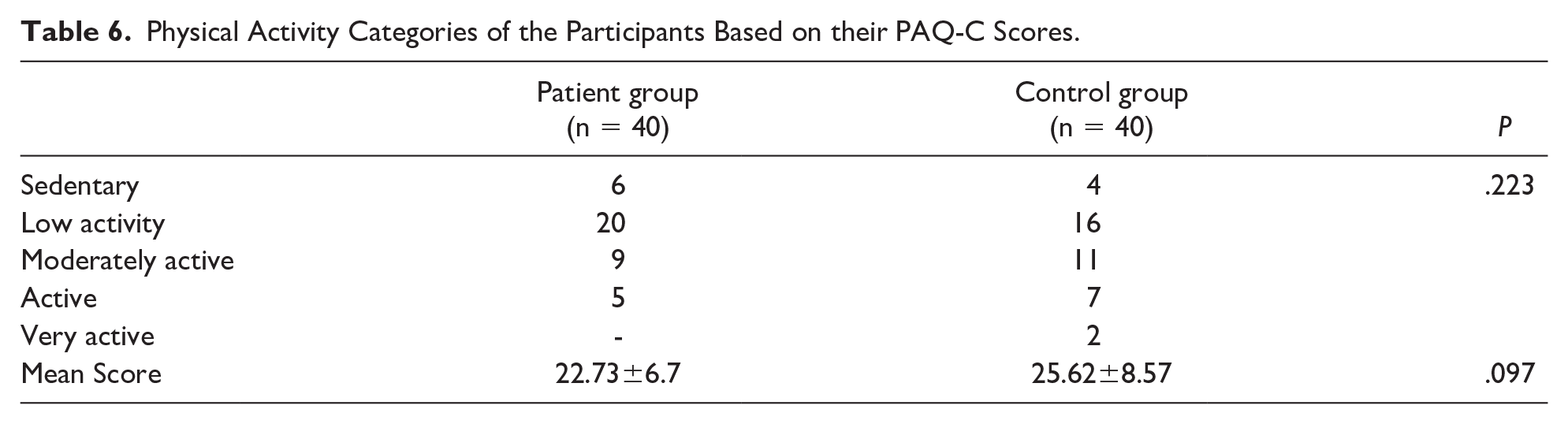
Based on their PAQ-C scores, the participants were divided into groups that designated their physical activity levels as sedentary, low activity, moderately active, active, and very active. There was no significant difference between the patient and control groups in terms of their physical activity levels measured using PAQ-C (P = .05) (Table 6).
Physical Activity Categories of the Participants Based on their PAQ-C Scores.
Discussion
Physical activity is required for the physical, emotional, and psychosocial development of children with a history of CHD. However, many parents, educators, and health care professionals have doubts about whether or not physical activity is suitable for children with a history of CHD. If children with CHD reduce their physical activity levels, they also reduce their exercise capacity. 9 Nowadays, children with CHD are diagnosed earlier, and they reach adulthood with quick and effective treatment. With improvements in the life expectancy of children with CHD, sufficient physical activity is important to increase their quality and reduce their cardiovascular risks. Studies conducted in this field have shown increased rates of type 2 diabetes, dyslipidemia, obesity, hypertension, osteoporosis, and atherosclerosis among individuals with a sedentary lifestyle. 1 Therefore, physicians need to be aware of the negative effects of a sedentary lifestyle and recommend appropriate physical activity for each individual. 9
Excessive restriction of physical activity in children with cardiac malformations brings about a set of physical and psychological challenges. The purpose of the promotion of physical activity, which is also known as cardiac rehabilitation, is to reintegrate the child into society and bring their restricted physical activities to a normal level. As a part of the clinical follow-up in this patient group, it is recommended to perform routine evaluations of physical activity. They should also be provided with physical activity counseling according to these evaluations.
Unfortunately, a sedentary lifestyle, which affects children as much as adults worldwide, is prevalent today. Survey studies revealed that only one in every 10 children in the United States and Canada live in compliance with the recommendations of the relevant guidelines suggesting at least 60 minutes of moderate physical activity per day.10,11
Several researchers have focused on the measurement of physical activity levels among children with CHD. There is a study that investigates the possibility of improving cardiopulmonary exercise capacity and daily physical activity in young adults and children with corrected tetralogy of Fallot or Fontan circulation conditions with exercise training. In this study, 56 patients at the ages of 10 to 25 were included in the exercise group, while 37 patients were in the control group, and their data were compared. Peak oxygen uptake and workload increased significantly in the exercise group, while these parameters did not increase in the control group. Consequently, it was stated that aerobic exercise training increased cardiopulmonary vitality in the patients with corrected tetralogy of Fallot conditions but not in those with Fontan circulation. Also, exercise training did not have an effect on daily physical activities in either group. 12
Voss et al analyzed the validity and reliability of the Physical Activity Questionnaire (PAQ-C/PAQ-A) among adolescents and children with CHD. They determined that these patients took part in moderate-intense physical activity for a mean duration of 46.9 minutes per day. The PAQ scores were found to be significantly related to physical activity data obtained with an accelerometer and sedentary behaviors (P < .01). The authors emphasized that PAQ can provide valid estimates regarding general physical activity levels, and it could be a useful tool to assess time-dependent changes in physical activity in children and adolescents with CHD. 8
In our study, based on the results deducted from comparing the patient and control groups according to their physical activity levels and PAQ-C scores, there were no significant differences between the 2 groups. However, the patients group did less intense physical activities such as “jogging or running” and “gymnastics” when compared with the control group.
In our country, courses for intense physical activities such as football, dance, basketball, and swimming are held on weekends. The reason why the control group reported more intense physical activity on the weekends shows that healthy individuals participate in these activities more than patients.
Also, the participants in the control group showed significantly more participation in physical education classes compared to those in the patient group. Regarding activities other than eating during the lunch break, while 47.5% of the children in the control group preferred to run and play, 80% of the children in the patient group preferred to sit and walk around the garden.
Based on these findings, one can conclude that children with a history of treatment for CHD, despite having no permanent health problems, are less physically active than their peers. It is important to consider the socio-economic status of these children while counseling. Their limited physical activity may be due to their anxiety about keeping up with their friends’ skill levels. In addition, parents should be prepared to encourage physical activity and work closely with their physicians to determine whether physical activity restriction is necessary or not (13).
Relevant literature regarding the physical activity levels of children with CHD has shown that children diagnosed with CHD are not sufficiently physically active. This study’s results support these findings. It was observed that most of the children in this study were inactive or had low physical activity levels. Other studies have also emphasized that physical activity levels should be increased unless there are complications.
Limitations
There are several limitations in this study. In light of obvious sex-age differences, it was unfeasible to explore whether PAQ-C scores differed by CHD disease complexity. Furthermore, it was impractical to determine detailed PAQ-C score cut-points that correspond to physical activity guidelines according to sex and age. Another limitation of this study is the location where the research was carried out. Because the city where this study was conducted is located at a height of roughly 800 meters above sea level, the study’s geographic location may have had an impact on the results regarding activity levels. The relatively small sample size can also be considered as a limitation. The fact that participants took the PAQ-C at an outpatient clinic might potentially be viewed as a limitation of the study. This is because patients were relatively stressed at a hospital setting, which might have influenced their responses. In addition, the fact that we did not differentiate between surgical and transcatheter therapies due to the small number of cases in our patient group might be seen as a limitation. This study was also unable to assess communication between personal and environmental components, which are thought to contribute to physical activity. 13 In order to sustain an active lifestyle in childhood, it is well established that enjoyment of physical activity is crucial. 14 Consequently, even though we attempted to quantify a child’s daily essential physical activity for our study, we were unable to determine whether the child engages in this activity in a pleasant setting. 13
Conclusion
A questionnaire can be a convenient and affordable substitute for time-consuming and tedious objective measurements when determining the general levels of physical activity in CHD children and adolescents as well as tracking changes over time. In this unique community, there is growing interest in this field of study. Children in our research no longer had any cardiac problems. However, they still reported little physical activity. Children with CHD should have more physical exercise if there are no complications. Concerns which include encouraging healthy lifestyle choices, maintaining activity levels and psychological well-being as well as avoiding overly protective behavior on the part of parents and doctors, must be taken into account for this specific population.
Author Contributions
All authors agree to be accountable for all aspects of work ensuring integrity and accuracy. All authors contributed to the study conception and design. All authors read and approved the final manuscript.
Footnotes
Acknowledgements
The authors declare that there are no acknowledgments to be made for this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Gazi University Faculty of Medicine Ethics Committee.
Informed Consent
Written informed consent was signed by parents of all children.