
Abstract
This study identified specific feeding and growth topics discussed during 2-, 4-, and 6-month well-child visits. Conversations between mothers (N = 20) and pediatricians (N = 5) during visits were audio-recorded. Conversation segments were classified as pediatrician-initiated guidance, mother-initiated questions/concerns, or updates using directed content analysis. Pediatricians and mothers completed surveys on perceptions of guidance delivered. Feeding clusters included introducing solids/drinks, breast milk/formula amount and timing, feeding in specific situations; and breast milk/formula preparation. Growth clusters included appropriate growth and growth tracking. There was considerable variability in specific topics discussed between and within families across visits. Mothers desired additional guidance around introducing solids (42.1%) and allergen foods (31.6%). Pediatricians (80%) felt the amount of guidance to deliver in a standard visit was too much, and additional guidance outside of visits would benefit caregivers. Future research should investigate strategies to further support families by offering additional guidance during or outside of well-child visits.
Introduction
Positive feeding behaviors during infancy are foundational for optimal growth and development.1,2 Early feeding patterns include what, when, and how much to feed 3 ; yet, not all parents are confident identifying reliable information in these domains, especially with an abundance of information and misinformation readily available.4,5 Pediatric well-child visits are an opportune time to ensure parents are well-supported with evidence-based guidance that empowers them to establish positive feeding behaviors in infancy. 6
Pediatricians are a trusted source of health information and develop relationships with families across frequent well-child visits in the first year of life.4 -6 Bright Futures Guidelines, by the American Academy of Pediatrics (AAP), provides recommendations on the delivery of anticipatory guidance during well-child visits for topics including, but not limited to, infant feeding and growth. 6 However, time is a barrier to delivering in-depth guidance on multiple topics in a typical 10- to 20-minute visit,7 -10 resulting in large variations in time spent discussing feeding (1 second to 1.6 minutes) and growth (2 seconds to 5.3 minutes), 9 specifically. To explore this variation, cross-sectional studies have identified if general topics are discussed or not during well-child visits; yet, these studies lack depth on the diverse sub-topics that can fall within feeding and growth discussions.7,9,11 Furthermore, this design lacks the ability to examine if topic discussions change over time due to age, stage of development, or new caregiver questions/concerns. Research is thus needed to identify more nuanced topics discussed across multiple visits to better understand how discussions evolve and where interventions could be useful.
With limited time and a wealth of information to deliver, pediatricians must prioritize content delivery based on clinical expertise and patient needs. 9 The information pediatricians prioritize may not cover all topics that parents desire guidance around. 12 Currently, it is unclear who initiates discussions around each topic and how initiations change over time, which could be used to inform improvements to health care delivery by identifying common parent questions/concerns, uncover which topics are discussed infrequently or overlooked, and inform additional resources to address topics not sufficiently discussed during visits.
The aim of this study was to identify specific content discussed related to infant feeding and growth during well-child visits across the first 6 months of life. Well-child visits were audio-recorded to capture naturally occurring conversations between mothers and pediatricians. Conversations were characterized as pediatrician-initiated guidance, mother-initiated questions/concerns, or general updates to better understand the nuance of guidance delivered. The aims were to identify: (1) which specific topics around feeding and growth were discussed at 2-, 4-, and 6-month well-child visits, (2) the extent to which mothers and pediatricians initiated these conversations, and (3) mother’s and pediatrician’s perceptions of the guidance provided.
Methods
Study Design
This pilot observational study used mixed methods to collect longitudinal data on infant well-child visits at 2, 4, and 6 months of age. Routine visits were audio-recorded to capture natural conversations between pediatricians and mothers, and later transcribed and coded using qualitative directed content analysis. 13 Additional information was gathered from surveys at baseline and after the 6-month visit (for mothers) and after all dyads had completed the study (for pediatricians). Mothers reported visit satisfaction and identified topics they desired additional guidance on. Pediatricians reported their perception of visits, extent of information covered, and barriers to providing care. All study procedures were approved by the university’s institutional review board (HM20019034) prior to data collection.
Participant Recruitment
Mother-infant dyads (N = 20) were recruited from an academic, safety-net medical center in the southeastern United States. Data queries were developed to scan electronic medical records and extract the contact information of potentially eligible dyads. Data queries identified mothers who were primiparous, ≥18 years of age, had a biological child <2 months of age, and were English-speaking. The research staff referenced the medical records of potentially eligible dyads to determine infant eligibility. Infants had to be singleton, delivered at full-term (≥37 weeks gestational age), and a birth weight of ≥2500 g. The research staff called mothers to verify eligibility and confirm they planned to receive pediatric care within the participating hospital system until their infant was at least 6 months of age, intended to be present at all well-child visits, and had no severe comorbidities or cognitive conditions that would impair their ability to complete the study. Mothers who met inclusion criteria provided consent for themselves and their infant. A screening phone call was conducted for 30 mothers; of these, 22 qualified and provided verbal consent to participate (6 did not qualify; 2 were not interested). Following consent, 2 mothers withdrew from the study, resulting in a final sample size of n = 20. Sample size was determined based on pragmatic considerations, prior research, and information power.14 -16
All attending pediatricians in the general pediatrics clinic were provided with a detailed study overview during a routine division meeting. Pediatricians were informed that the study purpose was to explore how well-child visits impact “infant health and well-being” without specifically mentioning feeding or growth, as not to influence conversations during visits. Informed consent was obtained individually from each interested pediatrician (N = 6).
Audio Recordings of Well-Child Visits
Before each 2-, 4-, and 6-month well-child visit, a researcher met the mother in their exam room. Two audio recorders were placed on the counter. The researcher left the room and did not re-enter to collect the devices until the visit was over and both the mother and pediatrician had left the room. The visit was recorded in its entirety, but only conversations between the mother and pediatrician were used for analysis. Pre-exam or post-exam conversations with nurses or other staff members were not analyzed.
Online Surveys
Sociodemographics
Upon enrollment, mothers completed a baseline survey using the Research Electronic Data Capture (REDCap) platform. 17 Survey items included sociodemographic information on mothers’ and infants’ race, ethnicity, and gender. Mothers reported their income, education, employment, and marital status. Additional demographic information on mother’s age and infant birth weight and length were obtained from medical records.
Mother’s exit survey
After the 6-month visit, mothers completed an exit survey evaluating perceptions of the quality and quantity of health topics addressed during their previous well-child visits. Questions specific to feeding and growth were used in these analyses. The topics were based on those most pertinent to feeding in well-child care 6 including (1) breastfeeding; (2) formula feeding; (3) transitioning to solid foods; (4) introducing allergenic foods; (5) identifying hunger cues; (6) establishing feeding routines; (7) use of food to soothe; and (8) infant growth rate. On Likert scales, mothers rated the extent to which each topic was discussed (1 = not at all to 5 = always), how well each topic was discussed (1 = very poor to 5 = very good), and the extent to which more guidance was desired (1 = none to 4 = a lot more). During analysis, response options were collapsed into 3 categories (eg, not at all/slightly vs neutral vs frequently/always). In addition, mothers were asked to rate the amount of guidance they received (too much, just right, too little) and whether additional guidance in an ancillary visit would be valuable (1 = strongly agree to 5 = strongly disagree).
Pediatrician’s exit survey
Pediatricians completed an exit survey assessing their perception of well-child visits after all dyads completed data collection. This included sociodemographic information (eg, age, gender), years of clinical experience, and an assessment on the same feeding and growth topics presented in the mother’s survey. Pediatricians rated how often each topic was typically covered during well-child visits on a Likert scale (1 = never to 5 = always), how well each topic was typically discussed (1 = very poor to 5 = very good), and the importance of discussing these topics across the first 6 months (1 = not important at all to 5 = very important). During analysis, the scale options were collapsed into 3 categories, as previously described. Pediatricians were asked additional questions assessing their perceptions of barriers to providing optimal care and the value of offering an ancillary visit for additional guidance following each well-child visit.
Data Analysis
Qualitative analysis
Study personnel trimmed the audio files to capture conversations between the time the pediatrician entered and exited the room. Recordings were transcribed using Rev.com and further reviewed by study personnel for accuracy. Any identifying information was removed before beginning the coding process. Transcripts were analyzed using QSR NVivo (Cambridge, Massachusetts, 2010).
Two members of the study team used directed content analysis, similar to previous studies, to identify emergent clusters around feeding and growth.13,18 Researchers independently coded conversation segments, starting with the 2-month visits. A few transcripts were coded at a time, before meeting to compare and resolve discrepancies. Minimal discrepancies were found. Conversation segments were grouped into similar categories, which later formed clusters. Within a given category, conversation segments were further classified as pediatrician-initiated guidance, mother-initiated questions/concerns, or general updates (see Figure 1). Pediatrician-initiated guidance occurred if the pediatrician offered advice, without the mother prompting. Mother-initiated questions/concerns occurred if the mother was the first to mention the topic as a question/concern. Conversations were classified as general updates if either the mother or pediatrician made a general statement in relation to a certain topic.
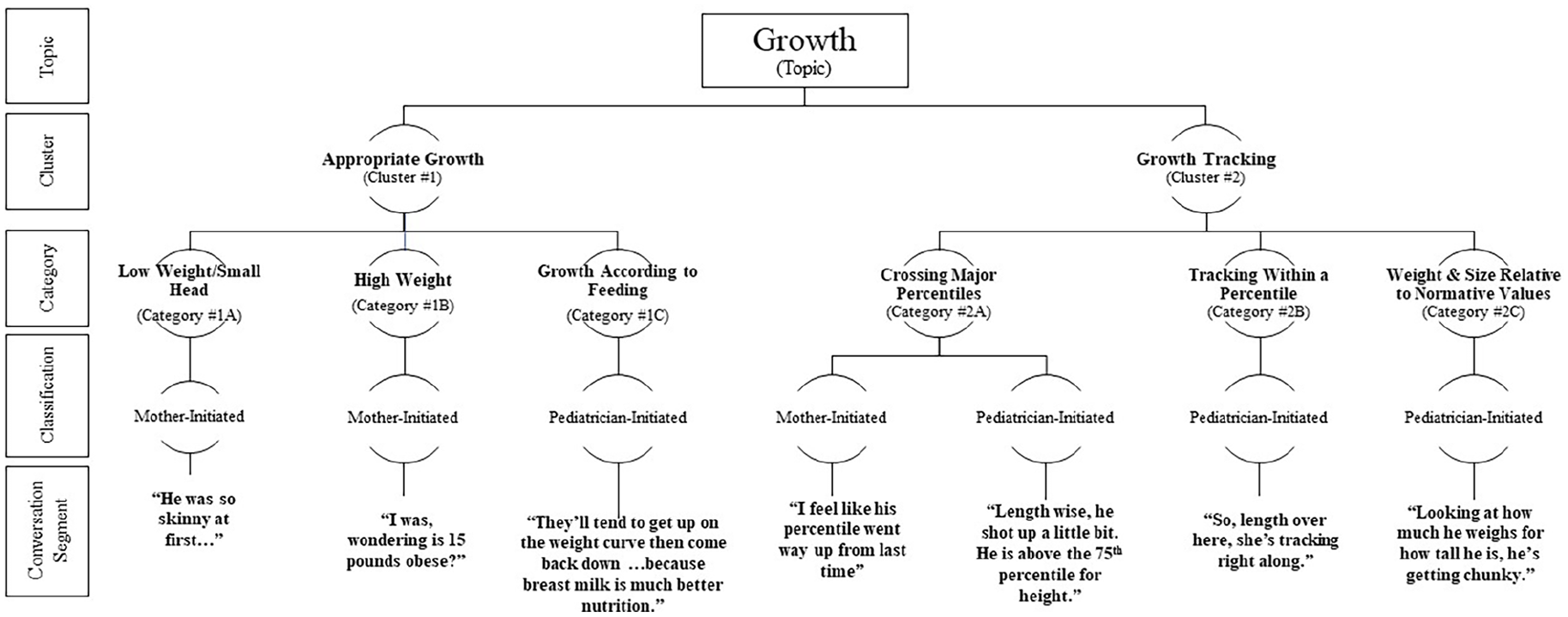
Flow chart of the clusters, categories, and conversation segments that emerged on the topic of growth during infant well-child visit conversations at 2, 4, and 6 months of age. If a pediatrician-initiated or mother-initiated classification is not displayed, then this conversation segment did not emerge for that given classification. General updates emerged in all categories and are not represented on this figure.
After all the transcripts were coded and compared, researchers independently re-reviewed the transcripts to ensure codes had not been missed. A codebook was developed and consistently updated to define each category. To ensure trustworthiness, criteria established by Lincoln and Guba were followed.19,20 Clusters were generated for comparison within and across time points.
Quantitative analysis
Survey responses were analyzed using descriptive statistics. Means and standard deviations were used to report continuous variables, and percentages were used to report categorical variables. Analyses were conducted using SAS Studio version 15.1.
Results
Participant Sociodemographics
Mother and pediatrician sociodemographics are listed in Table 1. Most mothers were White, had a college degree, employed, and married. Most pediatricians were White and identified as female. At birth, infants averaged 37.9 ± 1.5 weeks gestational age, 50.0 ± 2.2 cm in length, and weighed 3.4 ± 0.4 kg.
Demographics of Participating Mothers (N = 20) and Pediatricians (N = 5) Collected From Mother Baseline Surveys and Pediatrician Exit Surveys.
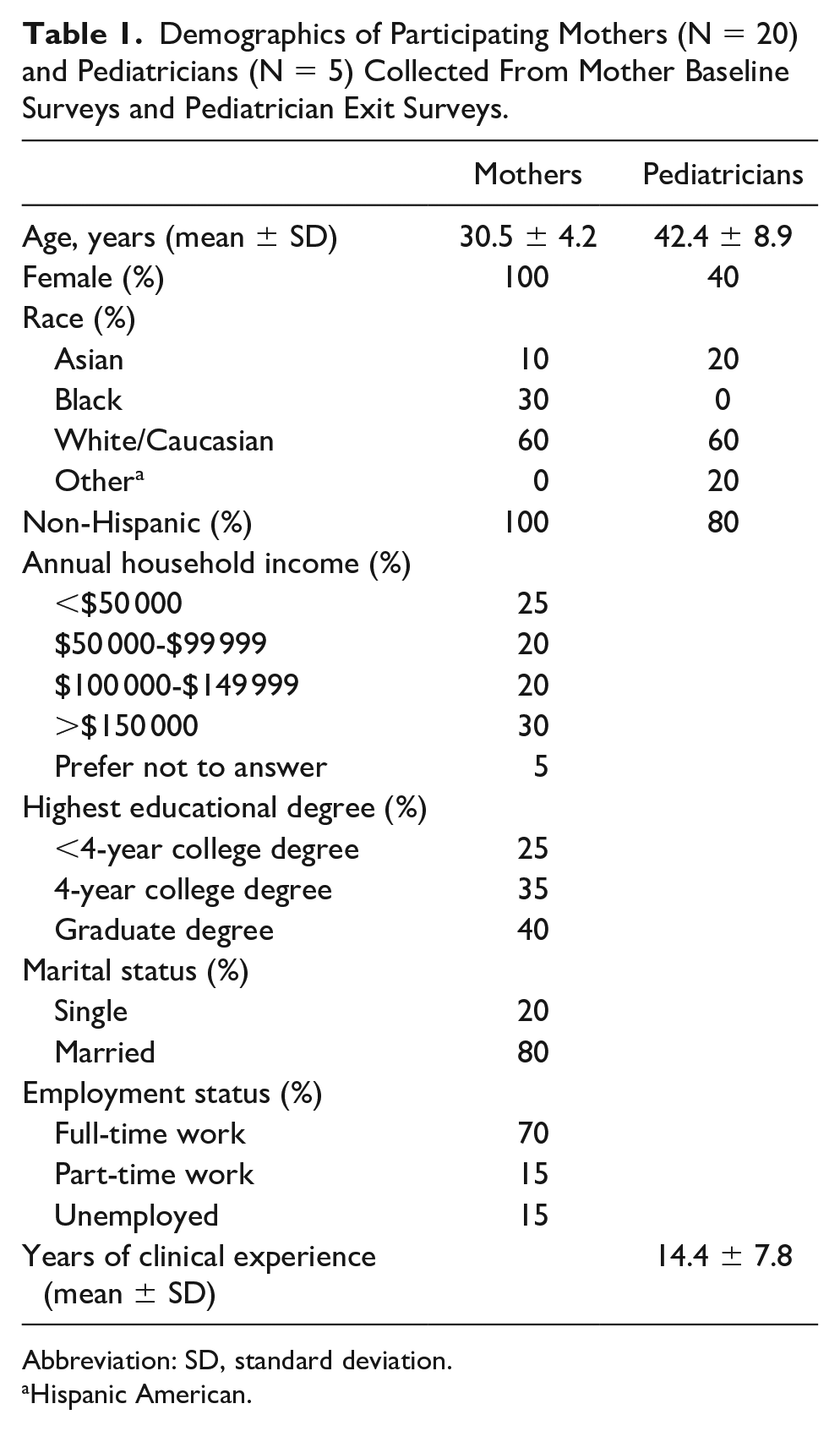
Abbreviation: SD, standard deviation.
Hispanic American.
Feeding Clusters
Four feeding clusters emerged (1) breast milk/formula amount and timing; (2) introduction to solid foods and drinks; (3) breast milk/formula preparation; and (4) feeding in specific situations. Each cluster was comprised of multiple categories, as described in Table 2, with example quotes. Further details on the total number of conversation segments classified as mother-initiated and pediatrician-initiated can be found in Table 3, as well as the number of unique visits for each cluster.
Examples of Conversation Segments Classified as Mother-Initiated Questions/Concerns and Pediatrician-Initiated Guidance Within Each of the 4 Emergent Feeding Clusters, 2 Emergent Growth Clusters, and Subsequent Categories at 2-, 4-, and 6-Month Well-Child Visits.
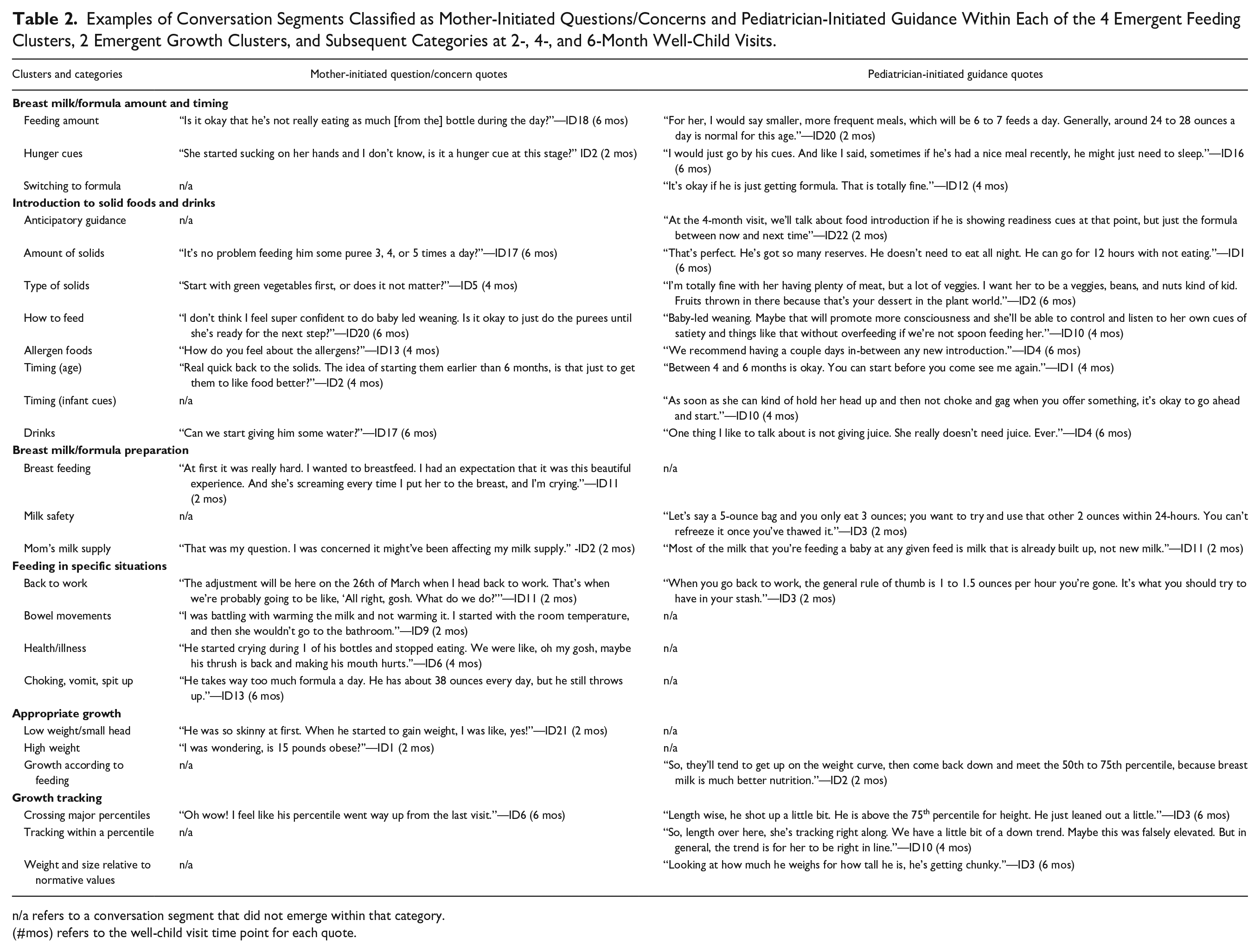
n/a refers to a conversation segment that did not emerge within that category.
(#mos) refers to the well-child visit time point for each quote.
Frequency of Mother-Initiated Questions/Concerns, Pediatrician-Initiated Guidance, and General Updates Across Emergent Feeding and Growth Clusters at 2-, 4-, and 6-Month Well-Child Visits Among Mothers (N = 20) and Pediatricians (N = 5).
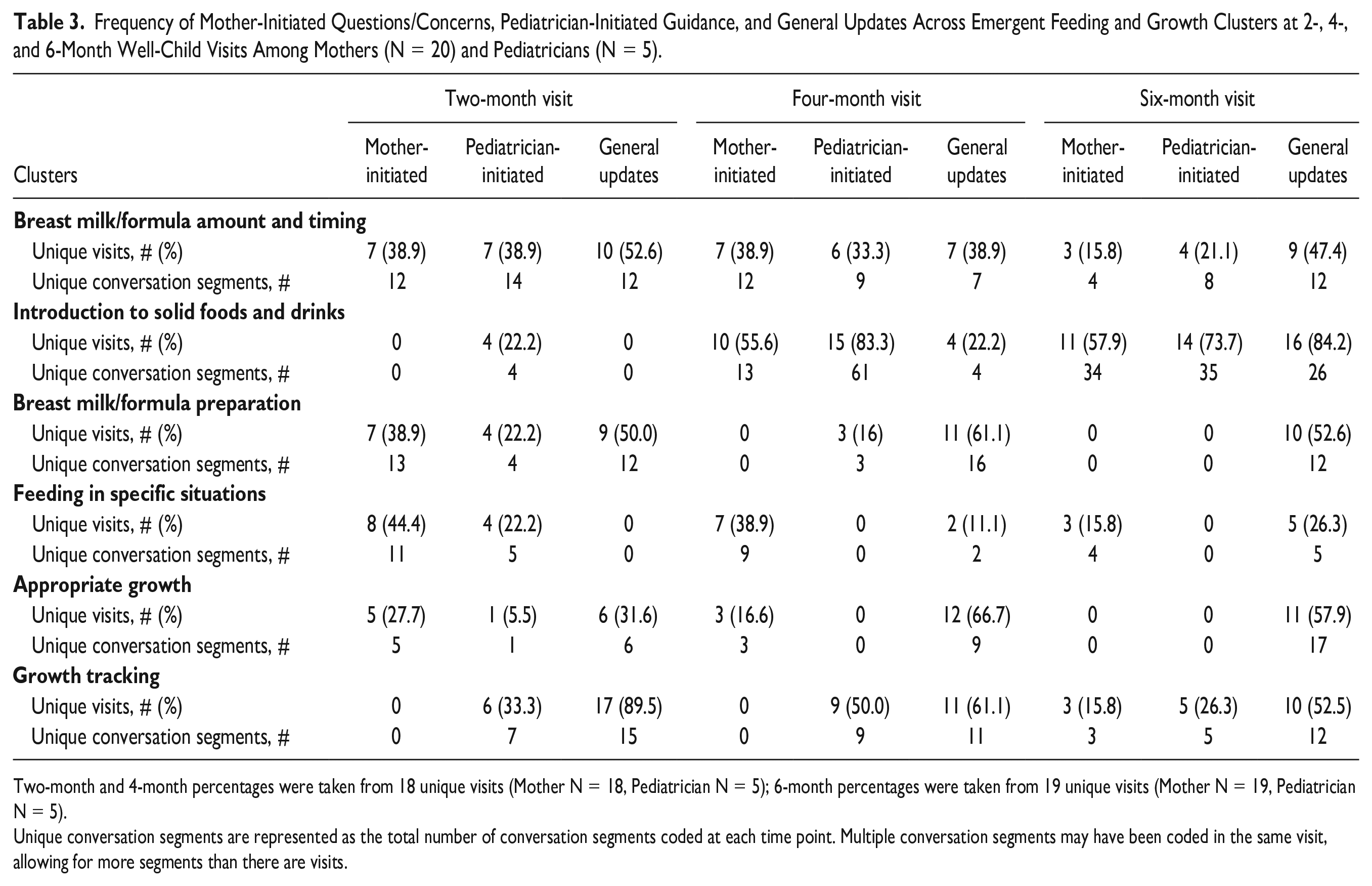
Two-month and 4-month percentages were taken from 18 unique visits (Mother N = 18, Pediatrician N = 5); 6-month percentages were taken from 19 unique visits (Mother N = 19, Pediatrician N = 5).
Unique conversation segments are represented as the total number of conversation segments coded at each time point. Multiple conversation segments may have been coded in the same visit, allowing for more segments than there are visits.
Breast milk/formula amount and timing
Conversation segments were coded within this cluster if mothers or pediatricians discussed feeding schedules or appropriate food volumes. This was the only cluster consistently initiated by both mothers and pediatricians across all time points; however, it was discussed in fewer than 40% of visits at each time point. At 2 and 6 months, pediatricians initiated discussions more often than mothers, but mothers initiated discussions more often at 4 months. Overall, the frequency of mother-initiated questions/concerns and pediatrician-initiated guidance decreased across time points.
Introduction to solid foods and drinks
Conversation segments were coded within this cluster if mothers or pediatricians discussed the introduction or feeding of solid foods. Conversations were more often initiated by the pediatrician (69.2% of visits; 97 of 140 unique occurrences) compared with mothers (30.7% of visits; 43 of 140 unique occurrences). During 6-month visits, more questions/concerns about solid foods emerged, compared to previous visits, with 30 unique mother-initiated conversation segments and 32 unique pediatrician-initiated conversation segments. Contrary to other clusters, the frequency of discussions increased across time points.
Breast milk/formula preparation
Conversation segments were coded within this cluster if mothers or pediatricians discussed preparation of breast milk or formula. This cluster emerged in at least 1 visit, at each time point, but was the least prominent compared with the other clusters. This topic was most frequently discussed at 2 months and initiated by mothers in 62.9% of the 2-month visits. Conversation during the 4-month visit was exclusively initiated as guidance from the pediatricians.
Feeding in specific situations
Conversation segments were coded within this cluster if mothers or pediatricians discussed feeding in specific circumstances, such as when infants were sick or when mothers returned to work. This cluster emerged across all visits, with 64.1% (25/39) of unique conversation segments being mother-initiated. All conversations in the 4-month and 6-month visits were mother-initiated.
Growth Clusters
Two growth clusters emerged: (1) growth tracking and (2) appropriate growth. The categories within each cluster are displayed in Table 2, with example quotes. The total number of conversation segments classified as mother-initiated and pediatrician-initiated, as well as the number of unique visits each cluster emerged in, can be found in Table 3.
Growth tracking
Conversation segments were coded within this cluster if discussions included growth chart percentiles and normative values. This cluster was present at each time point, but only discussed in 33.3% of 2-month visits and 50% of 4-month visits, and exclusively initiated by pediatricians. It was not until the 6-month visits that 15.8% of mothers initiated these conversations.
Appropriate growth
Conversation segments were included if mothers or pediatricians discussed general growth, rather than specifically referencing growth charts. This topic was initiated by both mothers and pediatricians, only during the 2-month visits. Mothers initiated conversation around their infant’s weight (high weight/low weight), where pediatricians provided guidance on appropriate growth according to feeding patterns.
Survey Results
Mother surveys
All mothers (100%) reported infant growth and transitioning to solid foods as frequently discussed topics; yet, only 58% to 74% of mothers reported a high frequency of discussions around breastfeeding, formula feeding, introduction to allergenic foods, and establishing feeding routines. The use of food to soothe was the least discussed topic, with 52.6% of mothers reporting this was rarely/never mentioned.
Most mothers were satisfied with discussions around infant growth rate (94.7%) and transitioning to solid foods (100%), whereas 63% to 74% were satisfied with discussions around breastfeeding, formula feeding, introduction to allergenic foods, identifying hunger/fullness cues, and establishing feeding routines. Lower satisfaction was reported for the use of food to soothe (47.4% reported average satisfaction; 15.8% reported very poor/poor).
Most mothers (68% to 85%) felt that no additional guidance was needed regarding breastfeeding, formula feeding, identifying hunger/fullness cues, and the use of food to soothe; yet, many wanted additional guidance on transitioning to solid foods (42.1%) and introducing allergenic foods (31.6%). Mothers (94.7%) felt the amount of guidance provided during visits was “just right,” with few reporting an ancillary visit would be of value to them (15.8%). Additional details are provided in Supplementary Table 1.
Pediatrician surveys
Most pediatricians (80%) felt the amount of guidance to deliver during well-child visits was too much, and all (100%) mentioned time as a barrier to delivering optimal care. Pediatricians felt the topics of breastfeeding, introducing solid foods, establishing feeding routines, and infant growth rates were the most important topics to discuss. Overall, pediatricians were satisfied with discussions around growth and feeding, but felt discussions on feeding routines, using food to soothe, and hunger/fullness cues could improve. Most pediatricians (80%) felt that providing additional guidance in ancillary visits would be valuable to parents (see Supplementary Table 2).
Discussion
This study identified specific topics of discussion between mothers and pediatricians around infant feeding and growth during well-child visits across the first 6 months of life. Although previous studies have identified if general topics are discussed or not using medical records, checklists, and pediatrician self-report, these analyses lack the specificity this study provides.7,9,11 Using directed content analysis of audio-recorded visits, this study identified more nuanced topics discussed, when they were discussed, and who initiated these discussions over time.
Pediatricians reported feeding as an important topic to discuss, but some feeding topics were more important than others. Pediatricians prioritized breast/formula feeding discussions at 2-month visits and solid food introduction at 4-month and 6-month visits.7 -10 Specifically, breast milk/formula amount and timing were consistently discussed across time points. Breast milk/formula preparation was discussed at 2-month visits but lessened over time as introducing solids became a priority at 4-month and 6-month visits, aligning with the AAP guidelines. 6 Conversation around introducing solids focused on when to introduce at 4 months and the types of foods to introduce at 6 months. A unique aspect of this study was identifying who initiated these specific topics. At 2 months, feeding discussions were heavily driven by mothers, often concerned their infant was eating too much or too little; for a few mothers, pediatricians recommended listening to their infant’s hunger and fullness cues, whereas other mothers were left without direct guidance in this regard. Mothers consistently initiated conversation around breast milk/formula amount and timing, indicating this topic was a priority, whereas pediatricians lessened these initiations over time. Specifically, mothers increasingly had questions around supplementing with formula, which is expected given breastfeeding rates decline over time.21,22
Four-month and 6-month conversations were mostly pediatrician-initiated and focused on introducing solids. Pediatricians stressed the importance of infant readiness cues, repeated exposure, and the early introduction of allergens. Mothers had few questions/concerns related to solids at 4-month visits but almost 3 times the number of questions/concerns at 6-month visits, likely due to caregivers starting solids between 4 and 6 months or anticipating an introduction shortly thereafter. Although solids were discussed in detail, not all aspects were covered with each family, thus highlighting a key area for supplemental intervention. Indeed, both mothers and pediatricians mentioned that additional guidance/information around introducing solids would be valuable; thus, research should explore strategies to supplement guidance provided during visits, such as handouts/brochures, online patient portals, or additional time with other health care providers/staff to address questions/concerns. These opportunities could allow for more in-depth guidance specific to introducing solids and allow for more time during visits to address topics discussed less frequently.
Findings from this study highlight frequently discussed topics and common questions/concerns to inform intervention targets that can supplement guidance provided during well-child visits. At 2 months, mothers had concerns about feeding in specific situations, such as when returning to work or during infant illnesses. Thus, clinician referrals to reliable sources (eg, evidence-based web sites and support groups) for working and/or first-time mothers may be useful for situation-specific questions that arise for some, but not all, parents to provide supplementary support and optimize time during visits.23,24 Few pediatricians reported hunger and fullness cues as an important topic to address, also reflected by infrequent discussions across visits. Additional guidance is warranted, as a growing body of evidence supports identifying and responding appropriately to infant hunger and fullness cues has been linked to positive health outcomes throughout infancy.2,25,26 Conversely, when positive feeding behaviors are not established, this may lead to suboptimal dietary habits, chronic diseases such as obesity, and/or oral health problems. 2 Given the emerging nature of this evidence, mothers may have limited knowledge of responsive feeding practices and pediatricians may not prioritize this guidance as standard of care. 27 Future efforts are needed to support strategies that deliver additional evidence-based guidance, both within clinic settings and throughout additional avenues, such as home visitation programs, nutrition education settings (eg, Women, Infants, and Children visits) or via evidence-based resources (eg, flyers, online modules).25,28
Pediatricians reported growth as an important topic to discuss, with growth tracking (eg, following a percentile curve) discussed more often than size references (eg, too big). Despite pediatricians reporting high importance for growth discussions, in-depth conversations were sparse and often came in the form of updates, leaving some mothers with little guidance. Although a brief mention of infant growth percentiles may be sufficient for some families, providing updates alone may limit opportunities for engagement in more in-depth discussions to address questions/concerns or provide evidence-based guidance. Given the strong link between infant growth rates and future health outcomes, it is critical that pediatricians prioritize these discussions and provide ample in-depth guidance as early as possible.29 -31 Equipping mothers with a deeper understanding of the factors that influence growth can facilitate opportunities for closer monitoring and disease prevention. 32 This is particularly important for first-time mothers, who are often less familiar with developmental milestones and growth charts, compared with multiparous mothers.32,33 Thus, future research should investigate optimal avenues to provide parents with additional evidence-based guidance around growth and the ability to ask in-depth questions.
Previous studies are limited by cross-sectional designs, self-report bias, and limited depth on the general topics discussed.7,9,11 In this study, audio-recorded conversations and a longitudinal design allowed for a more detailed and rigorous analysis, with comparisons drawn on topics discussed within and across visits. This study provides a unique lens by identifying who initiated specific topics over time. Limitations include a small sample size recruited from a single pediatric clinic. Future research should examine multiple clinics, different geographical areas, and various populations (eg, lower-resourced families, fathers). Furthermore, clinics often use modalities to supplement guidance provided during visits, such as online patient portals or paper handouts, which were not captured in this study and may have influenced discussions during visits.
Conclusion
Mothers and pediatricians engaged in varied discussions around a multitude of feeding and growth topics. Certain topics were discussed more frequently than others, leaving some mothers with little guidance on certain topics. While overall, mothers were content with the amount of guidance provided, most pediatricians felt the guidance to cover during well-child visits was too much to deliver optimal care. Further investigation is needed to identify effective strategies to bolster content delivered during time-limited well-child visits to ensure mothers receive comprehensive guidance. Results from this study can inform future work to tailor and prioritize specific feeding and growth guidance by highlighting common questions/concerns and topics not thoroughly addressed. Overall, this study provides initial information to inform future interventions that can supplement the guidance provided during well-child visits to increase the delivery of evidence-based information and support.
Author Contributions
ELA, MKB, LJC, and RW conceptualized the study. Funding acquisition was obtained by ELA and MKB. ELA, MKB, and LJC performed data curation. Formal analysis was conducted by ELA and MCS. Project administration was led by ELA, with supervision by MKB. MCS wrote the original draft of this manuscript. All authors reviewed and approved the final version.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228241287629 – Supplemental material for A Directed Content Analysis of Discussions Between Mothers and Pediatricians Around Feeding and Growth Topics During Infant Well-Child Visits
Supplemental material, sj-docx-1-cpj-10.1177_00099228241287629 for A Directed Content Analysis of Discussions Between Mothers and Pediatricians Around Feeding and Growth Topics During Infant Well-Child Visits by Meghan C. Savidge, Melanie K. Bean, Laura J. Caccavale, Romesh Wijesooriya and Elizabeth L. Adams in Clinical Pediatrics
Supplemental Material
sj-docx-2-cpj-10.1177_00099228241287629 – Supplemental material for A Directed Content Analysis of Discussions Between Mothers and Pediatricians Around Feeding and Growth Topics During Infant Well-Child Visits
Supplemental material, sj-docx-2-cpj-10.1177_00099228241287629 for A Directed Content Analysis of Discussions Between Mothers and Pediatricians Around Feeding and Growth Topics During Infant Well-Child Visits by Meghan C. Savidge, Melanie K. Bean, Laura J. Caccavale, Romesh Wijesooriya and Elizabeth L. Adams in Clinical Pediatrics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Children’s Hospital Foundation at Virginia Commonwealth University and the National Center for Advancing Translational Science (Award No. UM1TR004360) awarded to Virginia Commonwealth University. Additional support was provided by the National Institute of General Medical Science (P20GM130420) and the National Cancer Institute (2T32CA093423) for ELA effort, as well as the National Institutes of Diabetes and Digestive Kidney Diseases (K23DK131368) for LJC effort.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.