
Abstract
Despite strides in vaccinating priority groups against COVID-19, children under 5 years in Vietnam are still under-immunized, emphasizing a significant gap in prioritization. This study aimed to assess parental willingness to vaccinate children aged 6 months to under 5 years against COVID-19 in Vietnam and identify influential factors affecting this willingness. Data were collected via a survey of 5960 parents/guardians between May and June 2022. Multinomial logistic regression was employed to analyze the impact of various factors on parents’ willingness to vaccinate their children, alongside investigating reasons for reluctance or refusal and preferences for vaccine origins. Approximately 50.5%, 30.2%, and 19.3% of parents were willing, hesitant, and unwilling to vaccinate their children, respectively. Primary reasons for reluctance included concerns about vaccine safety, efficacy, and the severity of the pandemic. The most preferred vaccines originated in the United States. Factors significantly influencing willingness included parents’ age, knowledge of COVID-19 and vaccines, residency, education, perception of information sufficiency, children’s comorbidities, and family members’ vaccination status. Promoting child vaccination habits can boost COVID-19 immunization rates. Targeting hesitancy among parents of children with comorbidities is crucial. Enhancing parental knowledge and leveraging fully vaccinated family members are effective strategies.
Keywords
Introduction
Vietnam has achieved an impressive COVID-19 vaccine coverage rate of approximately 89%, 1 prioritizing vaccination for various demographic groups including adults, adolescents, and children aged 5 to 12 years. However, a notable gap exists as children aged 6 months to under 5 years, comprising about 8% of the population, 2 remain unvaccinated. This is concerning considering that as of February 2022, around 490 000 children in Vietnam have contracted SARS-CoV-2, resulting in 97 fatalities.3,4 The situation is compounded by the fact that several countries such as Argentina, Bahrain, China, Hong Kong, Venezuela, Cuba, Chile, and the United States have already approved vaccines for children aged 3 years or above,5,6 with Singapore planning to extend vaccinations to children aged 4 years and under in Q4 2022. 7 Vaccine hesitancy, defined as the delay in acceptance or refusal of vaccines despite the availability of vaccination services, is a growing concern worldwide. It significantly affects the uptake of vaccinations among various populations, including parents of young children. Despite substantial progress in vaccinating priority groups against COVID-19 in Vietnam, there remains a critical gap in vaccinating young children aged 6 months to under 5 years. This gap poses potential risks, as unvaccinated children could serve as vectors for the spread of the virus. 8 Understanding the factors influencing parental decisions regarding vaccinating young children is essential to address this gap effectively. This study aims to assess parents’ willingness to vaccinate children aged 6 months to under 5 years in Vietnam. By examining determinants, reasons behind decisions, and preferences for vaccine origins, the research seeks to contribute to the understanding of parental attitudes toward childhood vaccination against COVID-19. The study’s findings will inform policy interventions and public health strategies aimed at increasing vaccine uptake among young children, ultimately contributing to the mitigation of COVID-19 transmission and safeguarding the health of vulnerable populations.
Research Design, Methodology, and Models
Research Design
Given that the infection rate among children in Vietnam was 19.2% during the surveys, 4 the sample size is determined using methodologies outlined by Lwanga and Lemeshow 9 and Nakagawa and Cuthill 10 as follows:

where n represents the sample size to be calculated,
Stratified sampling was employed for its benefits,11-13 with the primary criterion being the 6 socioeconomic regions: Northern Midlands and Mountains, Red River Delta, North Central Coast and Central Coast, Central Highlands, Southeast, and Mekong Delta. 14 Child proportions from each region guided the selection of children in the age group.
Considering the intricate nature of the study regions, web-based surveys emerged as the most suitable method for data collection.15-17 Google Forms facilitated questionnaire design,18,19 with questionnaire specifics available in the Supplemental Material. A pilot study was conducted in late April 2022 using the same methodology as the primary study. The pilot study aimed to estimate infection rates, assess children’s proportions, and validate the questionnaire items and responses. To prevent multiple submissions from the same individual, Google Forms’ built-in capabilities were used to ensure that each participant could submit their answers only once. In the survey introduction, participants were informed that questions marked with a red asterisk (*) were mandatory and must be answered to proceed to the next questions. These instructions were reiterated in subsequent reminders throughout the survey period. In addition, for questions requiring additional information, respondents were provided with links or images to facilitate their responses. For more detailed information, please refer to the Supplemental Material. In addition, participants did not receive any gift or monetary compensation for their involvement in the study. Questionnaire links were disseminated via email, Facebook, Twitter, Zalo, Viber, and WhatsApp for surveying. Surveys were conducted from May 20 to June 24, 2022. During the data collection process, reminders were sent to respondents to encourage participation and completion of the survey or to thank them for their participation. These reminders were primarily sent as messages through the same channels used for distributing the questionnaires. Responses were downloaded in Excel format for analysis. Ethical approval (no. 192/QĐ-ĐĐNC/YTDP/2022, protocol/ID: 192/04/22) was granted by the Department of Preventive Medicine, Vietnamese Ministry of Health.
Research Methodologies, Models, and Variable Description
Parents were surveyed regarding their willingness to immunize their children if COVID-19 vaccines were free and endorsed by the Vietnamese Ministry of Health (MoH) and health experts. Responses included “willing,” “hesitant,” and “unwilling.” Using a categorical scale (0 = unwilling, 1 = hesitant, 2 = willing), multinomial logistic regression20-23 was applied, with independent variables chosen from prior research:

where Yi represents the willingness of the ith respondent to vaccinate their children. The zero group, comprising parents unwilling to vaccinate their children, served as the base category, with other groups compared accordingly. Thus, regression results for this group are omitted.
Previous studies identified several factors influencing parental willingness to vaccinate children, categorized into characteristics of parents and families, access to information, knowledge or perception of the pandemic, virus, and vaccines, and children’s exposure to the virus. Differences in willingness among respondents were hypothesized to be influenced by their relationship with children (X1, 1 = mother/father, 0 = guardian), gender (X2, 1 = male), age (X4, measured in years), residency (X5, 1 = urban), marital status (X6, 1 = married/cohabitated), and education level (X9, 1 = tertiary or above). The number of children (X3) or dependants (X8, excluding children) in the family might also impact decisions, coded as dichotomous variables. Specifically, X3, X4, and X8 were coded as 1 if below or equal to the mean and 0 otherwise. Income, a common influential factor, was approximated by employment or poverty status.24,25 Parents’ willingness might differ based on their family’s economic status (X7, 1 = non-poor) or employment status (X10, 1 = had a permanent job with income). Fear of discrimination against unvaccinated children (X12, 1 = yes) could also affect parental decisions. In addition, differences in willingness might exist between parents who regularly vaccinate their children (X13, 1 = yes) and those who do not.26-45
It was hypothesized that parental willingness to vaccinate children differed based on their risk exposure. Specifically, parents with children attending kindergartens (X12, 1 = yes) were expected to exhibit different willingness compared to those without. 43 Similarly, parents with family members in vaccine priority groups 46 were anticipated to have different willingness. Having a family member in a priority group (X18, 1 = yes) implied higher risk for children. Parents of children with comorbidities (X19, 1 = yes) might show mixed willingness due to potential health concerns.45,47,48 Children with infected family members or close contacts were perceived to be at higher risk. Therefore, willingness of parents infected (X28, 1 = yes/infected) or with infected close contacts (X29, 1 = yes/infected) was expected to differ from those without such exposures. Likewise, parents with fully vaccinated family members (X30, 1 = yes) or children’s close contacts (X31, 1 = yes) might decide differently. Fear of children contracting the virus (X32, 1 = yes) was anticipated to influence parental willingness.34,49
Differential access to pandemic and vaccine information was expected to influence parental decisions. Access was measured by the frequency of parents receiving news on the pandemic (X14, 1 = daily, 0 = weekly/monthly/other) or vaccines (X15, 1 = daily, 0 = weekly/monthly/other). Daily recipients were deemed well-informed and likely to decide appropriately. Perception of information sufficiency (X16, 1 = sufficient for pandemic, X17, 1 = sufficient for vaccines) was also considered. Parents rating received information as “sufficient” were coded 1, else 0.26,28,29,38,44,45,49-51
Knowledge enhances parental understanding of the COVID-19 pandemic and SARS-CoV-2 virus, aiding informed decision-making. Parents with sufficient knowledge of COVID-19 symptoms (X20) or vaccine side effects (X27) were expected to decide differently from those with insufficient knowledge. Similarly, willingness varied among parents with sufficient knowledge of virus transmission (X21), spread speed (X23), or fatality (X24). For instance, understanding transmission modes or virus fatality influenced vaccination decisions. Likewise, decisions differed based on knowledge of preventive measures (X22), vaccine immunity longevity (X25), or herd immunity (X26). For example, awareness of preventive methods or vaccine limitations shaped vaccination choices.29,30,33,38,49,52 These factors are briefly illustrated in Figure 1, which was adapted from Sun et al. 53 In addition, 2-sided t-tests to compare the means of different groups were conducted. A P-value of less than .05 was considered statistically significant. In addition, chi-square tests were used to assess the association between categorical variables.
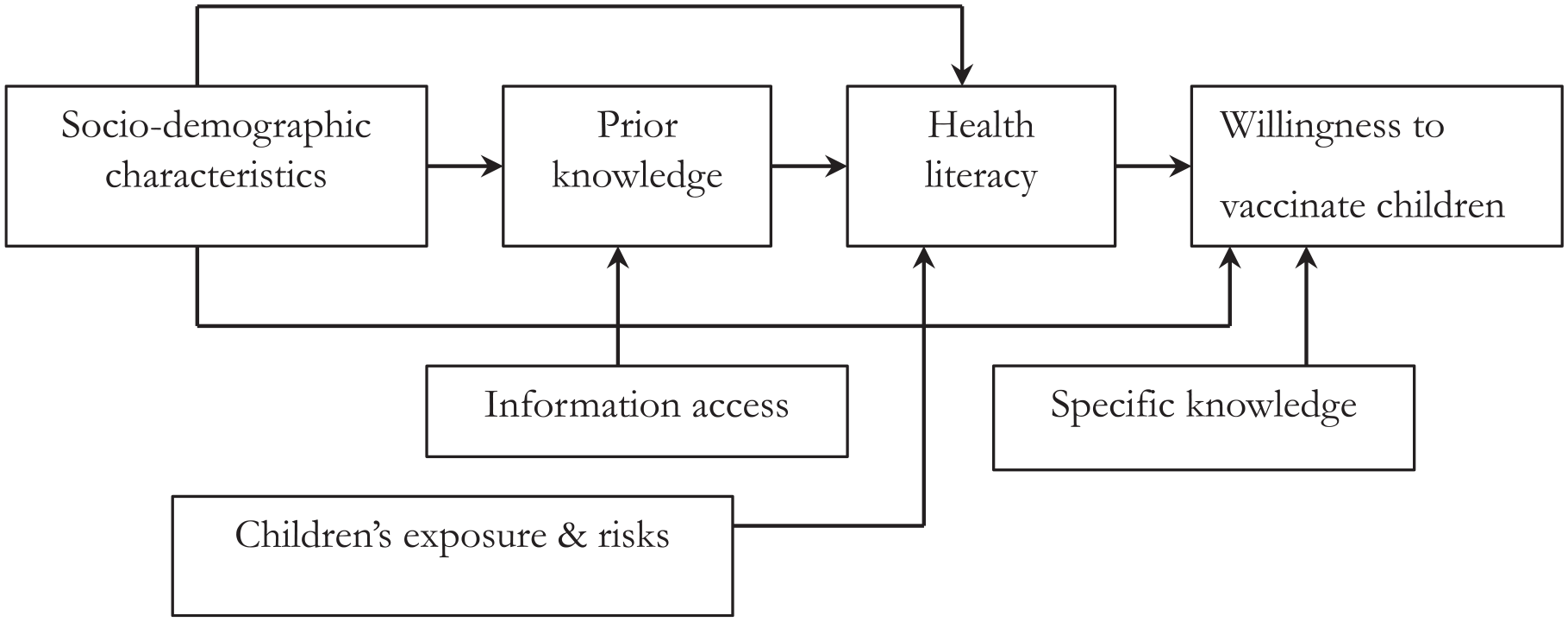
Conceptual framework on the parents’ willingness to vaccinate their children aged from 6 months to under 5 years.
Results
To account for potential invalid or unanswered responses, 6300 questionnaires (approximately 105% of the estimated sample size) were distributed. A total of 6125 responses were returned, but only 5960 responses submitted within the specified timeframe (May 20 to June 24, 2022) were included in the analysis.
Parents’ Willingness to Vaccinate Their Children Aged From 6 Months to Under 5 Years
The data show that 50.5% of surveyed parents agreed to vaccinate their children. In contrast, 30.2% of parents were hesitant, expressing uncertainty and concerns about the vaccination. In addition, 19.3% of the parents were unwilling to immunize their children, highlighting a significant portion of the population that remains resistant to vaccination efforts.
Details of parents’ willingness with different sociodemographic characteristics to immunize their children are presented in Figures 2–5.
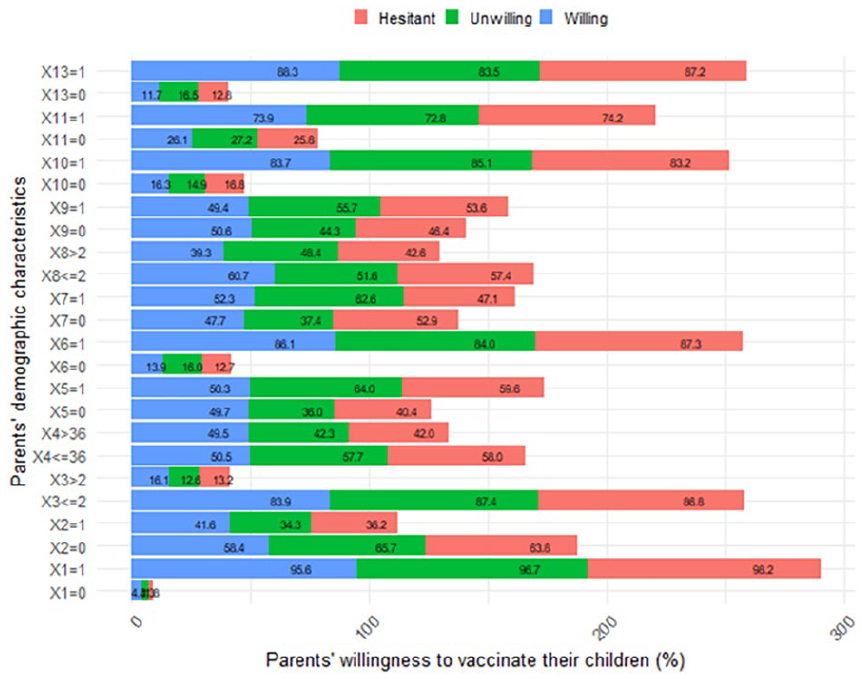
Characteristics of the parents and their families and their willingness to vaccinate their children aged from 6 months to under 5 years (measured in percentage).
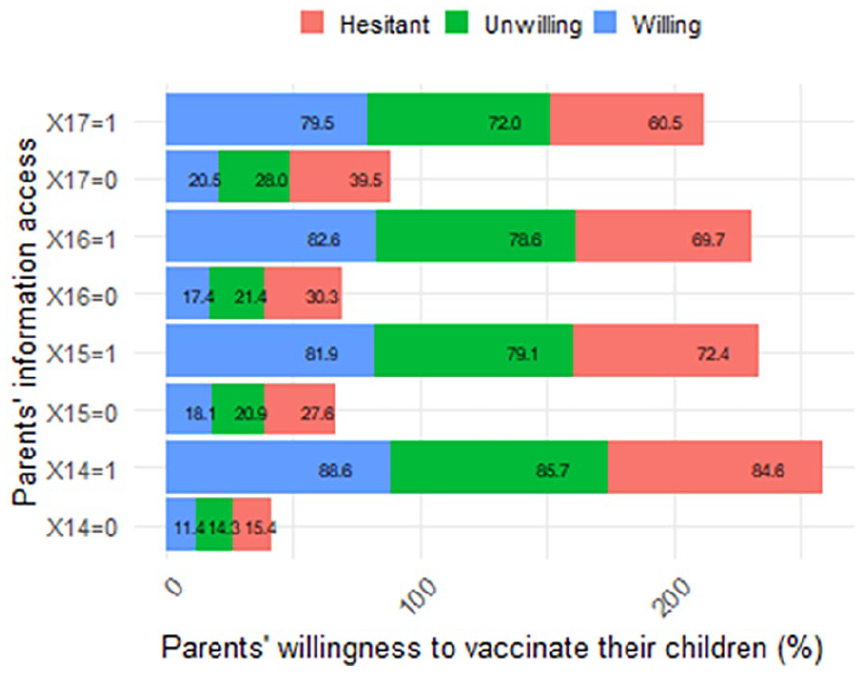
Parents’ information access and their willingness to vaccinate their children aged from 6 months to under 5 years old (measured in percentage).
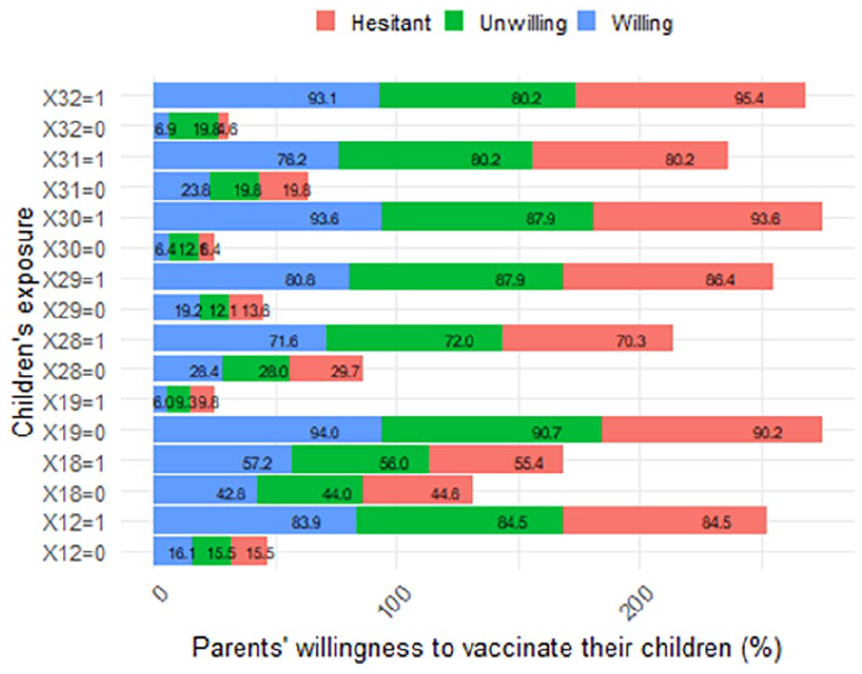
Children’s exposure to the SARS-CoV-2 virus and their parents’ willingness to vaccinate them (measured in percentage).
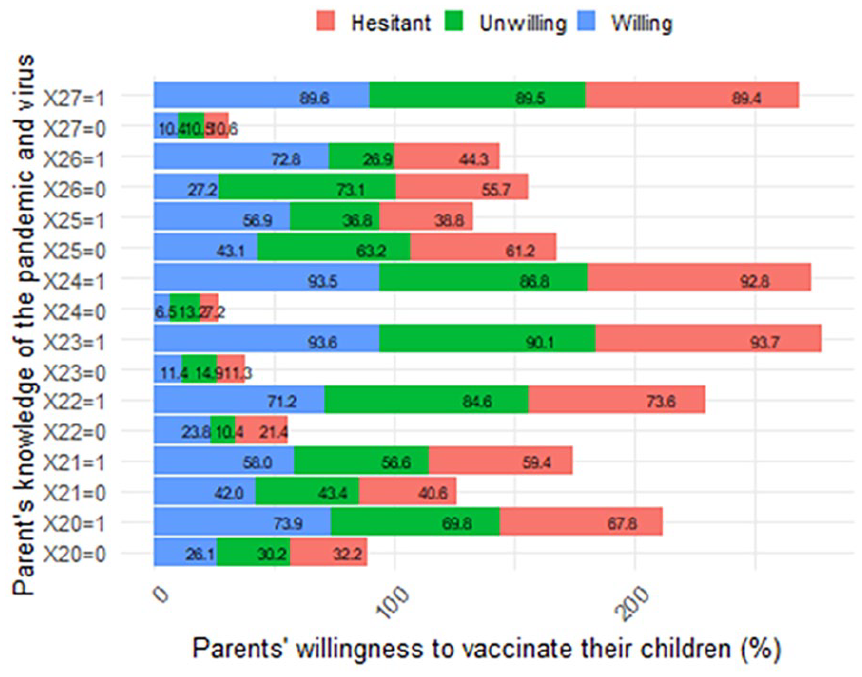
Parents’ knowledge sufficiency (of the pandemic and virus) and their willingness to vaccinate their children aged from 6 months to under 5 years (measured in percentage).
Figure 2 indicates that parents, females, individuals aged 36 years or younger (the mean age), and those married or cohabiting showed higher willingness to vaccinate their children compared to guardians, males, individuals older than 36 years, or those divorced, separated, widowed. Similarly, parents with 1 or fewer children (the mean number) or 2 or fewer dependants (excluding children) exhibited greater willingness compared to those with more children or more dependants. Urban residents and non-poor families displayed slightly higher willingness compared to rural residents or poor families, respectively. In addition, parents with lower education or permanent jobs with income showed higher willingness compared to those with lower education or without permanent jobs and income. Moreover, parents concerned about potential discrimination against unvaccinated children or those who regularly vaccinated their children demonstrated greater willingness compared to those without such concerns or irregular vaccination patterns, respectively. Further details are available in Table A1 in the Supplemental Material.
Figure 3 demonstrates that parents who received daily news on the COVID-19 pandemic or vaccines displayed higher willingness to vaccinate their children compared to those receiving news less frequently. Similarly, parents who rated information on the pandemic or vaccines as “sufficient” exhibited greater willingness to accept vaccines for their children compared to those rating it as “insufficient.”
Figure 4 illustrates that parents whose children attended kindergarten or had family members in vaccine priority groups showed greater willingness to vaccinate their children compared to those whose children did not attend kindergarten or lacked family members in such groups. In addition, parents of children without comorbidities or who feared infection displayed higher willingness to vaccinate their children compared to parents of children with comorbidities or who were not afraid of infection. Moreover, parents or children’s close contacts infected with SARS-CoV-2 demonstrated greater willingness to vaccinate their children compared to those not infected or with uninfected close contacts, respectively. Furthermore, parents with fully vaccinated family members or children’s close contacts exhibited higher willingness to vaccinate their children compared to those without fully vaccinated family members or children’s close contacts, respectively.
Figure 5 reveals that parents with sufficient knowledge of COVID-19 symptoms, vaccine side effects, transmission, spread speed, fatality, immunity longevity, herd immunity, and prevention displayed higher willingness to vaccinate their children compared to those with insufficient knowledge.
Reasons That Parents Hesitated or Refused to Vaccinate Their Children
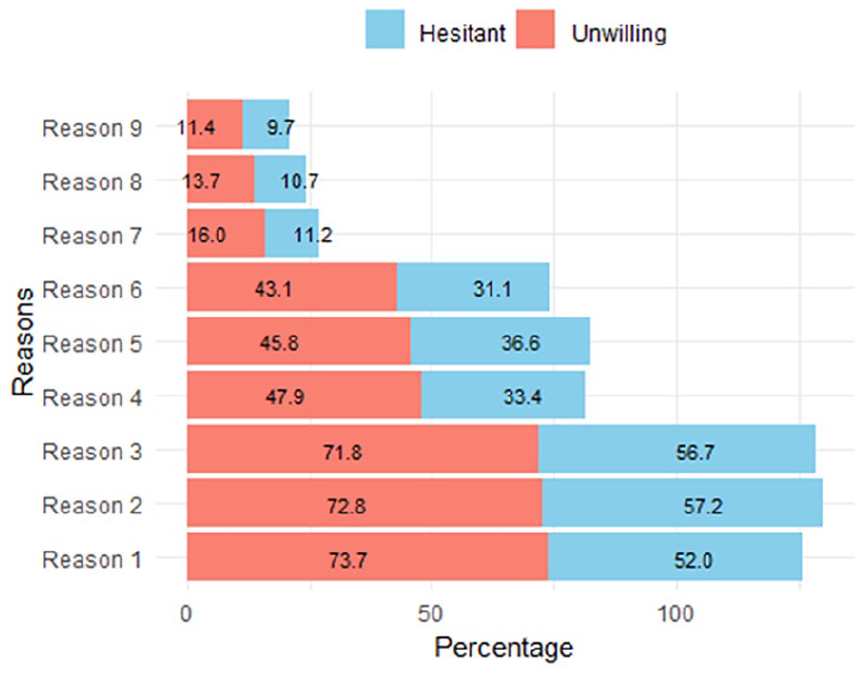
An analysis to investigate parents’ reasons for hesitance or unwillingness to vaccinate their children with current COVID-19 vaccines was conducted (Question Z1, Supplemental Material). The 9 most common reasons were incorporated into the options for parents to choose from, with results depicted in Figure 6.
Reasons that parents hesitated or refused to vaccinate their children aged from 6 months to under 5 years (measured in percentage).
Figure 6 highlights the top 3 reasons for parental refusal/hesitancy to vaccinate their children: concerns about vaccine side effects (reason 1), risk of myocarditis and pericarditis (reason 2), and long-term impact on fertility (reason 3). Among parents concerned about vaccine side effects, 73.7% were unwilling and 52% were hesitant to vaccinate their children due to fears of severe reactions or death. Similarly, among those worried about myocarditis and pericarditis, 72.8% were unwilling and 57.2% were hesitant to vaccinate their children. Concerning long-term impact on fertility, 71.8% were unwilling and 65.7% were hesitant to vaccinate their children.
The next 3 prevalent reasons deterring parents from vaccinating their children included concerns about vaccine inefficacy (reason 4). This encompassed worries that current COVID-19 vaccines might not safeguard children against new variants/subvariants or that fully vaccinated children could still contract or re-contract the virus. Furthermore, parents expressed concerns that present vaccines were not specifically developed for children (Reason 5). In addition, they perceived a low likelihood of their children contracting the virus, given high vaccination rates among other age groups (reason 6).
The remaining concerns hindering parents from vaccinating their children included the decreasing number of cases (reason 7) or deaths (reason 8) in the community and their children’s comorbidities. Specifically, 16% of unwilling parents and 11.2% of hesitant parents believed that decreasing community cases posed lower risks to their children. Similarly, 13.7% of unwilling parents and 10.7% of hesitant parents perceived decreased community deaths, indicating a less severe pandemic. In addition, 11.4% of unwilling parents and 9.7% of hesitant parents cited their children’s comorbidities as a reason for reluctance to vaccinate.
Parents’ Preferences for Vaccine Origin to Vaccinate Their Children Aged From 6 Months to Under 5 Years
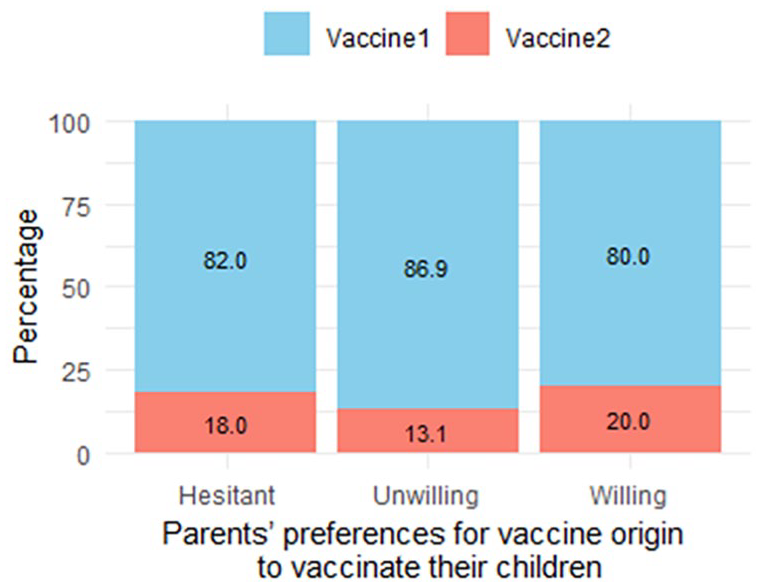
Parents were surveyed regarding their preference for vaccine origins to immunize their children (Question Z2, Supplemental Material). Given current approvals, only vaccines originating from the United States and China were recommended for this age group.5-7 Consequently, parents were presented with these 2 options. Results are detailed in Figure 7.
Parents’ preferences for vaccine origin to vaccinate their children aged from 6 months to under 5 years (measured in percentage).
Figure 7 reveals that 80% of surveyed parents favored US-origin vaccines for their children’s immunization. Conversely, Chinese-origin vaccines, although approved in 5 countries, were less favored. Notably, even hesitant or refusing parents expressed preferences for vaccine origins. These data holds significance for vaccine campaign planning.
The Association Between Parents’ Willingness to Vaccinate Their Children Aged From 6 Months to Under 5 Years and the Selected Influential Factors
To enhance the study’s reliability, it is crucial to identify and acknowledge potential sources of bias and methods to address them. Endogeneity commonly challenges parametric studies. Although instrumental variables (IVs) or 2-stage least squares (2SLS) methodologies ideally mitigate endogeneity, real-world availability of IVs or information to construct them is exceedingly rare.54-56 Similarly, the requisite variables for producing IVs in 2SLS are often lacking.57-59 Consequently, the study selected relevant independent variables in alignment with previous research to address this challenge.
Although all 32 factors/independent variables in the complete model could impact parents’ willingness to vaccinate their children, Akaike information criterion (AIC) tests identified 17 factors/variables as most explanatory,60-62 as detailed in the Supplemental Material. Thus, this study used the following reduced multinomial logistic regression model:

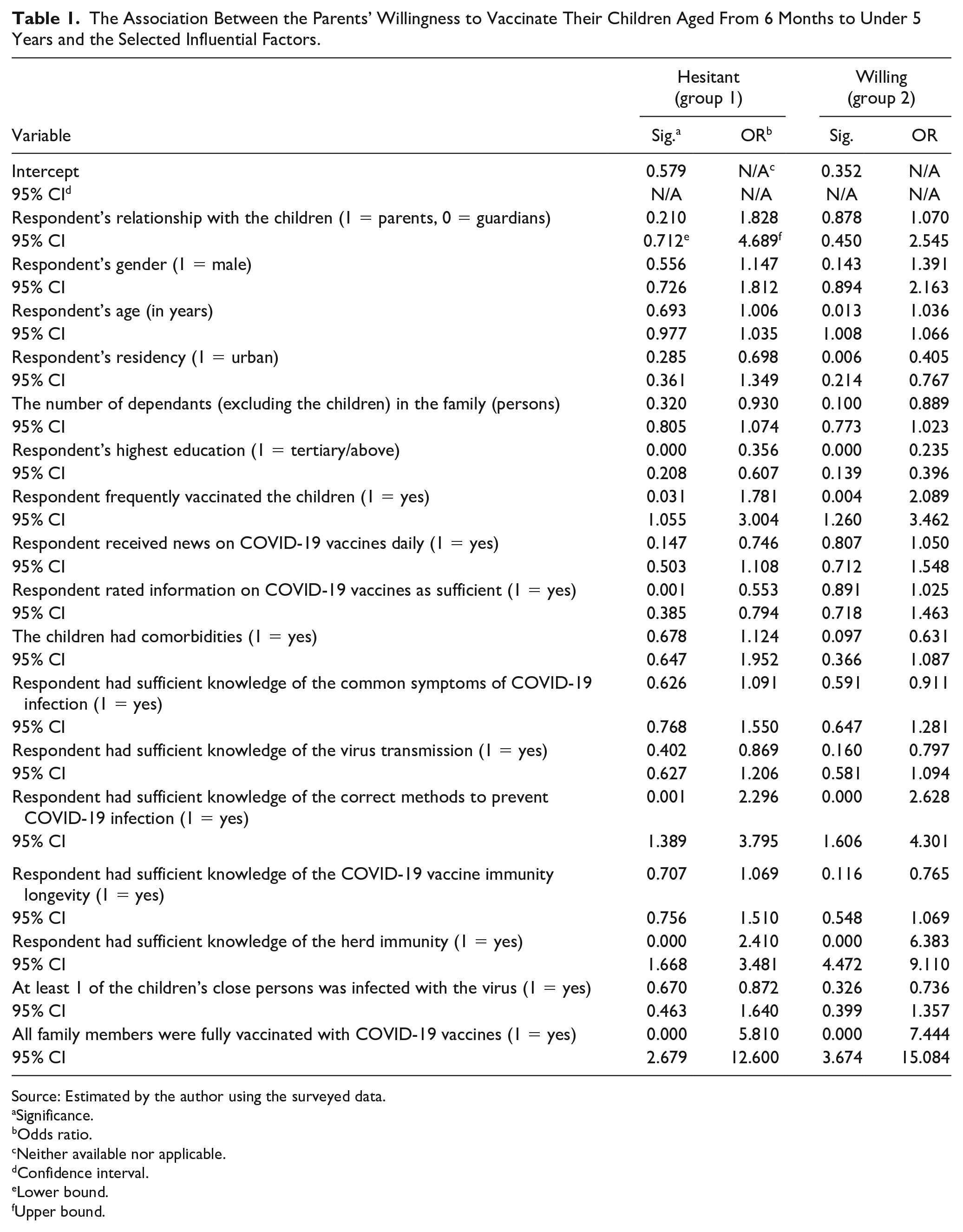
in which Yi and Xi were previously defined in Equation 2, and the recommended Xi identified by the AIC tests are detailed in the Supplemental Material. As mentioned earlier, regression results for group 0 are excluded. Furthermore, the willingness of groups 1 and 2 (representing parents who hesitated and refused to vaccinate their children, respectively) was compared to that of group 0. The regression results for groups 1 and 2 are presented in Table 1.
The Association Between the Parents’ Willingness to Vaccinate Their Children Aged From 6 Months to Under 5 Years and the Selected Influential Factors.
Source: Estimated by the author using the surveyed data.
Significance.
Odds ratio.
Neither available nor applicable.
Confidence interval.
Lower bound.
Upper bound.
Table 1 reveals that older parents were more likely to vaccinate their children (odds ratio [OR] = 1.036, 95% confidence interval [CI] = 1.008-1.066, P = .013), with significance observed for group 2. Conversely, urban-dwelling parents were less likely to vaccinate (OR = 0.405, 95% CI = 0.214-0.767, P = .006), significant for group 2. Surprisingly, those with tertiary education were less likely to vaccinate (group 1: OR = 0.356, 95% CI = 0.208-0.607, P = .000; group 2: OR = 0.235, 95% CI = 0.139-0.396, P = .000), significant at the 1% level for both groups. In addition, group 1 parents rating vaccine information as “sufficient” were less likely to vaccinate (OR = 0.553, 95% CI = 0.385-0.794, P = .001), significant at the 1% level for group 1.
As anticipated, parents with regular child vaccination habits were more inclined to immunize their children (group 1: OR = 1.781, 95% CI = 1.055-3.004, P = .031; group 2: OR = 2.089, 95% CI = 1.260-3.462, P = .004), significant at the 5% and 1% levels for groups 1 and 2, respectively. Conversely, in group 2, parents of children with comorbidities were less likely to vaccinate (OR = 0.631, 95% CI = 0.366-1.087, P = .097), with a modest impact. Parents with adequate knowledge of COVID-19 prevention were more likely to vaccinate (group 1: OR = 2.296, 95% CI = 1.389-3.795, P = .001; group 2: OR = 2.628, 95% CI = 1.606-4.301, P = .000), significant at the 1% level for both groups. Similarly, parents believing in herd immunity with 70% full vaccination were more inclined to vaccinate (group 1: OR = 2.410, 95% CI = 1.668-3.481, P = .000; group 2: OR = 6.383, 95% CI = 4.472-9.101, P = .000), significant at the 1% level for both groups. Likewise, parents with fully vaccinated family members were more likely to vaccinate (group 1: OR = 5.810, 95% CI = 2.679-12.600, P = .000; group 2: OR = 7.444, 95% CI = 3.674-15.084, P = .000), significant at the 1% level for both groups.
Discussion
The percentage of parents who were willing, hesitant, and unwilling to vaccinate their children in this study differs slightly from the 59.3%, 28.75%, and 23.1% medians reported in a review of 44 papers by Galanis et al. 64 This discrepancy may be due to differences in pandemic severity, children’s ages, parents’ or guardians’ demographic characteristics, cultural factors, COVID-19 vaccine availability, the sufficiency of pandemic and vaccine information in the study locations, the level of trust in health care systems, public health policies, and previous experiences with vaccination campaigns. However, Vietnam’s success in achieving high COVID-19 vaccination rates (89%) overall can be attributed to strong government leadership and clear communication, which fostered public trust through consistent and transparent public health messages. Effective community engagement and mobilization through local leaders and organizations ensured accurate information reached diverse population groups. The country’s well-organized health care infrastructure, utilizing mobile vaccination units and local health care centers, facilitated efficient vaccine distribution, particularly to remote areas. Intensive public health campaigns, tailored to address specific concerns and vaccine hesitancy in different communities, also played a crucial role. In addition, Vietnam’s proactive international cooperation and timely procurement of vaccine supplies ensured a steady supply, maintaining the momentum of the vaccination campaign.
The findings presented in Table 1 highlight several noteworthy trends in parental willingness to vaccinate children against COVID-19. Older parents, typically possessing greater knowledge and experience, demonstrated a higher inclination to vaccinate their children, corroborating previous studies,26-28,43,45,49 whereas younger parents may require additional information to make informed decisions, as indicated by contrasting research.33,34,64 However, urban parents in this older demographic showed a lower likelihood of immunizing their children, contrary to expectations.31,32,49 Similarly, parents with higher education levels exhibited lower vaccination rates, challenging previous findings,42,43,65,66 but aligning with Yigit et al, 67 necessitating further investigation. Conversely, parents in both age groups who regularly vaccinated their children demonstrated a higher inclination to immunize them, reflecting positive prior experiences.44,45 Surprisingly, parents in group 1 who deemed COVID-19 vaccine information sufficient were less inclined to vaccinate their children, suggesting potential concerns outweighing perceived benefits. 68 Furthermore, parents of children with comorbidities showed reduced vaccination inclination, contrary to expectations,45,48 possibly due to heightened health concerns. The study also highlights the importance of parental knowledge of COVID-19 preventive measures and herd immunity in influencing vaccination decisions, aligning with existing literature.29,38,49 To enhance parents’ understanding of COVID-19 preventive measures, including recommended vaccines, information should be disseminated through multiple channels, such as health care workers, doctors, and other reliable sources. 69 According to the World Health Organization (WHO), 70 herd immunity can be achieved through vaccination or prior infection, with the latter waning within months. Furthermore, vaccine immunity does not fully guard against new variants, as evidenced by Omicron’s breakthrough infections. 71 These insights are critical for informing vaccination consultations and campaigns, especially in light of evolving variants and the need for bivalent COVID-19 vaccines,72,73 underscoring the importance of ongoing research in this area to guide future interventions and policy decisions. In addition, the influence of peer vaccination behavior on parental decisions warrants further exploration. 74
The findings suggest that in this study, there were no significant differences in willingness to vaccinate between parents and guardians, nor did parental gender or the number of family dependants (excluding children) significantly impact willingness. This contradicts previous research,45,75 indicating a potential shift in parental attitudes and knowledge over the course of the pandemic. Similarly, the lack of significant difference in willingness between parents receiving daily COVID-19 vaccine news and those who did not was unexpected, warranting further investigation. Surprisingly, parents’ willingness, regardless of sufficient knowledge of common COVID-19 infection or vaccine immunity longevity, did not significantly differ from those with insufficient knowledge, contrary to Duong and Antriyandarti, 49 suggesting a potential saturation of information dissemination. Moreover, the willingness of parents whose children had at least 1 close contact infected with the virus did not significantly differ from those whose children’s close contacts remained uninfected, contrary to findings from numerous other studies.26,28,38,45,48,49 One possible explanation for this difference could be the high prevalence of virus infections, with approximately 11% of Vietnamese infected as of August 1, 2022.76,77 These results highlight the dynamic nature of parental attitudes and knowledge in response to the evolving pandemic landscape and underscore the need for ongoing research to explore the nuances of vaccine decision-making in diverse contexts. Future studies should delve deeper into these unexpected findings to elucidate their implications for public health interventions and vaccination campaigns.
The top reasons for parental refusal or hesitancy to vaccinate their children include concerns about vaccine side effects and efficacy. These concerns are consistent with findings reported by investigators and authors who examined similar issues in different geographic locations.63,78 This alignment suggests that apprehensions about vaccine safety and effectiveness are common among parents worldwide, highlighting the need for targeted education and communication strategies to address these fears.
Conclusion and Research Limitations
Despite significant strides in COVID-19 vaccination efforts targeting priority groups in Vietnam, there persists a notable deficiency in immunizing young children aged 6 months to under 5 years. This gap presents considerable risks, as unvaccinated children may act as potential vectors for transmitting the virus. This study investigated parental willingness to vaccinate young children against COVID-19 in Vietnam, surveying 5960 respondents, representing approximately 0.07% of children aged 6 months to under 5 years, between May 20 and June 24, 2022. Employing multinomial logistic regression, the research analyzed factors influencing parental willingness, identified concerns, and preferences for vaccine origins. Results showed 50.5% of parents willing to vaccinate, 30.2% hesitant, and 19.3% unwilling. Concerns included vaccine side effects, myocarditis risks, and perceived vaccine efficacy. A strong preference for US vaccines was noted, with over 80% favoring them, indicating higher parental trust. Regression analysis revealed older parents more inclined to vaccinate, whereas urban residents and those with tertiary education were less likely. Regular vaccination behavior and belief in achieving herd immunity positively influenced decisions. Further investigation is needed to understand nuanced dynamics and address remaining limitations, offering valuable insights for targeted interventions to promote vaccination acceptance and broader coverage. This study employed a web-based survey, potentially introducing bias due to self-reporting, which may lead to discrepancies between reported behaviors and actual actions. In addition, recall bias may affect the accuracy of parents’ recollections of their past behaviors and attitudes toward vaccinations. Social desirability bias could also influence responses, as parents might provide answers, they perceive to be more socially acceptable rather than their true beliefs or behaviors. Moreover, the anticipated impact of parental residency, education, and information sufficiency on vaccination willingness did not align with expectations, highlighting the need for further investigation in future studies. These limitations should be considered when interpreting the findings and underscore the necessity for employing complementary methods in future research to mitigate these biases.
Author Contributions
Conceptualization, methodology, software, validation, formal analysis, investigation, resources, data curation, writing - Original draft; writing - review & editing, visualization, project administration.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228241281126 – Supplemental material for Parents’ Willingness to Vaccinate Their Children Aged From 6 Months to Under 5 Years With COVID-19 Vaccines
Supplemental material, sj-docx-1-cpj-10.1177_00099228241281126 for Parents’ Willingness to Vaccinate Their Children Aged From 6 Months to Under 5 Years With COVID-19 Vaccines by An Hoai Duong in Clinical Pediatrics
Footnotes
Acknowledgements
I extend my heartfelt gratitude to the respondents who generously devoted their valuable time and actively participated in the surveys. Their invaluable contributions made this research possible and enriched its outcomes in meaningful ways. I would also like to express my sincere appreciation to the esteemed researchers at Griffith University. Their insightful comments and guidance throughout the course of this study played an instrumental role in shaping the direction and quality of the research. The collective support from both the respondents and the research colleagues has been instrumental in making this endeavor a success, and I am truly grateful for their unwavering commitment and cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical clearance for the present study has been formally approved and issued by the Department of Preventive Medicine, Vietnamese Ministry of Health, under the reference number 192/QĐ-ĐĐNC/YTDP/2022 and the protocol/ID: 192/04/22, research title “Parents’ Willingness to Vaccinate their Children Aged from 6 Months to under 5 Years with COVID-19 Vaccines.”
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Availability of Data and Materials
The data sets produced and analyzed in this study are not publicly accessible due to the sensitive nature of the content, including demographic information and personal opinions. However, detailed data, variable codes, and analytical scripts for STATA, SPSS, and R can be obtained from the corresponding author upon a justified request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.