
Abstract

Educational Objectives
In 4 research protocols involving biobanking of clinical samples in pediatric inflammatory bowel disease, participation was not significantly influenced by patient-specific factors (age and sex) or study-related factors (specimen type, clinical setting, recruiter attire, and recruitment method).
29.4% of participants were lost to follow-up in a year-long longitudinal study, with no significant difference in attrition between patient groups and healthy controls, providing real-world data to inform sample size and dropout estimations for future pediatric biobanking-associated research and grant applications.
Introduction
Biobanking, the collection and storage of biological samples for research purposes, has contributed to medical advances and innovations in genetics, molecular medicine, and bioinformatics in recent years. 1 However, only 2% of biobanks in the United States focus exclusively on pediatric patients, despite the recognized need for more research on childhood diseases and the potential benefit of longitudinal sampling. 2 Pediatric inflammatory bowel disease (IBD: Crohn’s disease [CD] and ulcerative colitis [UC]), is multifactorial in nature, influenced by the environment, immune system, gut microbiota, and genetic factors. 3 It is particularly beneficial when studying complex diseases, such as pediatric IBD, to have patient samples for research.
Existing literature has elucidated factors that influence adult recruitment in clinical trials for IBD 4 and indicate overall positive perceptions toward participation in biobanking. 3 However, most studies of children have assessed attitudes toward biobanking rather than actual participation,5,6 resulting in minimal objective data on pediatric biobanking. Pediatric biobanking is further complicated by specific ethical and legal issues surrounding the appropriate role for children in the decision-making process.5,6 In the scientific literature more broadly, the relationship between patient factors such as age, sex, and comorbidity burden on clinical trial participation and attrition has been assessed,7-9 but again there is a lack of pediatric data and very little has been specifically focused on biobanking.
In addition, a novel factor that may influence patient participation is research recruiter attire. Existing literature has described patient perception of health care provider professionalism and competence based on attire in various medical settings.10,11 However, whether these perceptions extend to research recruiters and might affect participation in clinical trials, specifically biobanking, has not yet been investigated.
Here, we prospectively examined factors that may influence patient participation and retention in pediatric IBD research involving biobanking, including age, sex, specimen type, clinical setting, and method of participant recruitment. In addition, we prospectively analyzed the impact of research recruiter attire in 3 of the 4 studies described herein.
Patients and Methods
Four research protocols involving IBD-related biobanking within the Division of Pediatric Gastroenterology at a large, tertiary-care institution were assessed for variables related to patient participation. Each study was approved by the Institutional Review Board and was consistent with the Declaration of Helsinki: H-25818 Risk Stratification and Identification of Immunogenetic and Microbial Markers of Rapid Disease Progression in Children with Crohn’s Disease (“Risk Stratification”; blood and tissue collection during a single diagnostic endoscopy in an outpatient setting, followed by 5 years of longitudinal clinical data recording); H-24295 Hypercoagulable Status and ADAMTS 13 Activity in Pediatric Patients with Inflammatory Bowel Disease (“Hypercoagulable Status”; a single blood collection from hospitalized patients with IBD); H-17654 Digestive Disease Center—Pediatric Inflammatory Bowel Disease Research Tissue Bank (“Tissue Bank”; blood and tissue collection during a single diagnostic endoscopy in an outpatient setting); and H-43759 Microbiome Focused Molecular Investigations in Primary Sclerosing Cholangitis (“Primary Sclerosing Cholangitis [PSC]”; recurring collection of stool and saliva every 3 months for 1 year from patients with UC, patients with UC and PSC, patients with UC and PSC on vancomycin, and healthy controls). All patients were first participants in the IBD-related research trials. Potential subjects who fit study criteria were approached between July 2011 and September 2020, prior to clinically indicated inpatient blood draws or clinically indicated outpatient endoscopies. Assent was obtained from children over 7 years of age.
The same research recruiter approached potential subjects to enroll in the Risk Stratification, Hypercoagulable Status, and Tissue Bank studies. She alternated weekly between wearing scrubs or professional attire without a white coat. An independent observer did not appreciate any noticeable changes in the recruiter’s behavior based on attire. Participant age (in years) at study enrollment, participant sex, biobanked sample type (blood vs blood and tissue), clinical setting (inpatient vs outpatient), patient/family decision to participate, and recruiter attire (scrubs vs professional attire) were noted at each encounter.
For the PSC study, an additional variable of recruitment method was included. Some patients were approached in person for consent and others by telephone. Rates of consent were noted in the context of recruitment method. Rates of withdrawal and loss to follow-up over the study’s 1-year duration were also documented. Recruiter attire was not tracked in the PSC study.
For the Risk Stratification, Hypercoagulable Status, and Tissue Bank studies, group comparisons were performed via Fisher exact test for participant sex, age, biobanked sample type, clinical setting, and recruiter attire. For the PSC trial, rates of study completion among participant groups and participation rates by recruitment method were analyzed via Fisher exact test. These analyses were performed after the studies concluded. Statistical significance was drawn at P < .05.
Results
A total of 200 patients were approached to participate in the 4 clinical trials, of which 147 (73.5%) legal guardians gave consent. There was no significant difference in consent rates among the 4 studies, which varied in clinical setting and biobanked tissue type as described in the “Methods” (P = .4221, Table 1).
Rates of Patient Participation.

In 4 clinical studies related to biobanking in pediatric inflammatory bowel disease, no significant difference in consent rates was found among the studies (P = .4221). These studies varied in their biobanked sample type and clinical setting.
For the Risk Stratification, Hypercoagulable Status, and Tissue Bank studies, the average age was 12.6 years and 50 out of 101 participants (49.5%) were female. There were not statistically significant differences across participation rates with age (P = .82), sex (P = .47), biobanked specimen type (blood vs blood and tissue, P = .35), or clinical setting (inpatient vs outpatient, P = 1). For these 3 studies in which recruiter attire was alternated, 37 out of 47 patients (78.7%) consented to participate when the recruiter wore scrubs, and 42 out of 54 (77.8%) consented when she wore professional attire (P = 1).
For the 1-year longitudinal PSC study, 20 out of 68 (29.4%) patients withdrew or were lost to follow up. By participant group, the dropout rate was 34.8% in the UC group, 23.1% in the PSC group, 28.6% in the PSC on vancomycin group, and 28.0% among the healthy controls, with no significant difference in dropout rates among these groups (P = .939, Table 2). When analyzed by recruitment method, 13 out of 16 patients (81.3%) consented to study participation by phone; in-person, 10 out of 12 consented (83.3%). There was no significant difference between recruitment methods (telephone vs in-person, P = .376). Overall, we found no significant difference in any of the variables assessed in relation to study participation or retention.
Rates of Study Completion and Withdrawal by Patient Group.
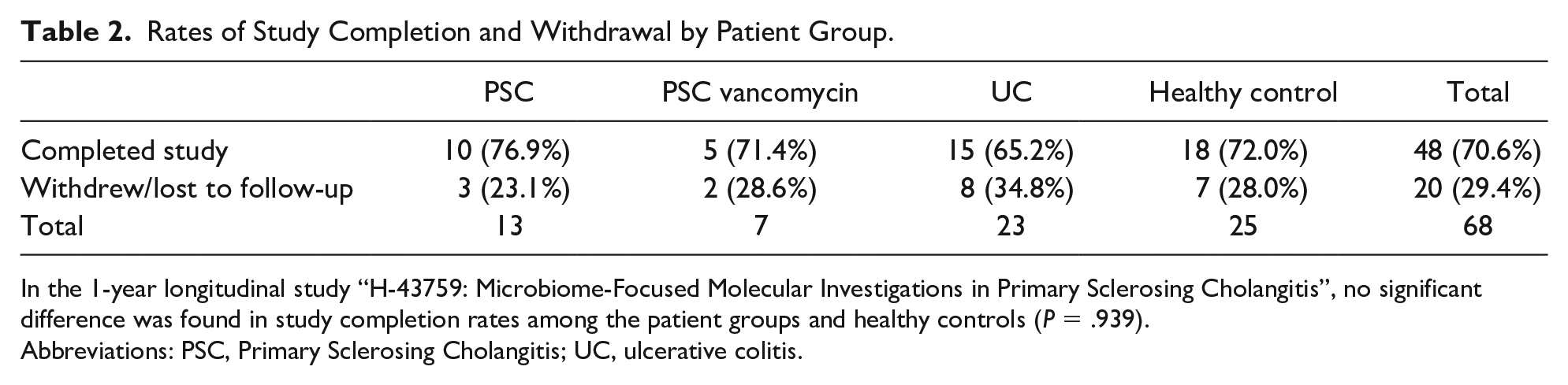
In the 1-year longitudinal study “H-43759: Microbiome-Focused Molecular Investigations in Primary Sclerosing Cholangitis”, no significant difference was found in study completion rates among the patient groups and healthy controls (P = .939).
Abbreviations: PSC, Primary Sclerosing Cholangitis; UC, ulcerative colitis.
Discussion
This study provides one of the first prospective investigations into pediatric participation in biobanking of clinical samples. Our overall high rate of participation (73.5%) is consistent with existing literature on positive patient perceptions toward biobanking.3,5,6 Importantly, rates of withdrawal or loss to follow-up in the 1-year longitudinal study were consistent across patient groups, including healthy controls, which contrasts with literature in the adult population in which patients with chronic illness 12 or a higher number of comorbidities 7 have higher rates of attrition. Our rates of recruitment and retention in these studies provide real-world data to inform planning and sample size estimations for future biobanking-associated research studies in pediatrics.
The lack of significance of recruiter attire is consistent with prior studies in which provider attire did not affect patient perception of professionalism or competence.10,11 However, our method of using the same research recruiter who alternated attire each week was novel as it provided prospectively collected data to address this question for the first time in the pediatric literature.
While none of the factors examined in our study had a statistically significant impact on patient participation, further research is warranted to investigate if any other variables or interventions might increase recruitment or retention in pediatric research studies, particularly those related to biobanking. For example, patient-specific factors that we did not assess in this study, such as ethnicity, insurance status, religious beliefs, trust in the medical system, and distance from the clinic, may play a role in study participation. We postulate that novel and creative approaches that anticipate and address hesitations to research participation, perhaps through multidisciplinary communication frameworks 13 or the use of social media 14 could be avenues toward increased public awareness of the importance of biobanking and ultimately increased pediatric participation.
While we aim to increase pediatric participation in biobanking, it is important to remain mindful of the ethical and legal ramifications specific to the pediatric population. While we obtained assent from children above age 7, there is ongoing debate in the biobanking literature regarding the appropriateness of involving children in the decision to participate in biobanking and at what age they may be able to provide assent.5,6 In addition, collecting specimens from children raises the question of re-contacting these participants for their consent once they reach legal adulthood and how and when to disclose incidental findings.5,6 In biobanking in any population, participants may have concerns related to loss of confidentiality and the potential for discrimination in purchasing life or health insurance. 3 Our involvement of pediatric patients in biobanking aims to advance the medical field, specifically inflammatory bowel disease diagnosis and management, yet these ethical and legal considerations must be carefully weighed in this field of investigation.
Author Contributions
Footnotes
Acknowledgements
We would like to acknowledge the Gutsy Kids Fund including philanthropic donations from the Brock Wagner, Klaasmeyer and Frugoni families, and numerous other generous philanthropists.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Public Health Service grant DK56338 funding the Texas Medical Center Digestive Diseases Center. RK was supported by the Gutsy Kids Fund (see Acknowledgement).