
Abstract
This study examined primary care provider (PCP) alignment with guideline-based care for adolescent depression screening and identified factors associated with post-screening responses. A retrospective chart review was conducted across 17 primary care clinics. Logistical regressions were estimated across provider specialties, sociodemographic factors, and patient clinical histories. Significant differences in follow-up and identification of depression were found among patients with more severe depression presentation. Follow-up screening was also more likely to be completed among patients with private insurance and less likely to occur among Black patients. Patients with significant mental health history of a mood concern, history of being prescribed psychotropic medication, were currently on medications at the time of the screening, or had a history of an internal mental health referral had a higher predicted probability of being identified as depressed on the patient problem list.
Primary care providers (PCPs) play an important role in the identification and treatment of adolescent depression. At least 80% of adolescents with depressive symptoms will present to their pediatricians for depression management and support.1 -4 Universal screening has the potential to increase identification of these patients and facilitate their contact with evidence-based treatment. 5 Although most pediatric PCPs indicate they should be responsible for referring depressed patients to mental health specialists, 6 referral rates are variable and linkage to services tends to be poor among pediatric patients.6,7 Poor connection to services has been linked to stigma around mental health treatment, poor insurance coverage, and a significant mental health provider shortage, 8 especially among publicly insured patients. 9 The National Center for Quality Assurance (NCQA) and the American Academy of Pediatrics (AAP) recommend that PCPs schedule a follow-up within 60 days of a positive depression screen to monitor the patient’s symptoms and response to treatment. 10 Follow-up care has been identified as an important component of depression management and suicide prevention in the primary care setting;10 -13 however, follow-up care is often poor 7 and providers do not feel they have the necessary tools to monitor and treat patients efficiently. 6
The objectives of our study were to examine alignment with existing quality guidelines for adolescent depression screening, describe how PCPs responded to positive adolescent screens, and identify patient-level and provider-level factors associated with PCP responses to positive depression screens at a large academic medical center. Few published studies have examined universal depression screening programs in the context of real-world primary care practice. Recent studies suggest high levels of variability in follow-up, referral, and medication management practices among PCPs and practices.7,14 -16 Limitations of current studies include small sample size,7,14 restricted data ranges based on appointment type or patient age,14,16 and insufficient data for the impact of mental health history and comorbidities on care.15,17 -19 Although a few studies have looked at screening outcomes and predictors of provider response to positive screens, most were in the context of large-scale integrated mental health support initiatives, 19 which is not reflective of most pediatric primary care practices.20,21 In addition, none of these studies looked at rates of guideline-based rescreening practices among patients with positive screens.17 -19
Method
Study Design
This study consisted of a descriptive analysis of retrospective chart review data for adolescent patients, age 12 through 17 years, who obtained a positive depression screen on the PHQ-9 (Patient Health Questionnaire). These patient care encounters occurred across 17 primary care clinics within a large Mid-Western academic medical center. This study was reviewed by the medical system institutional ethics review board, and it was determined exempt per the federal exemption category 4(iii) at 45 CFR 46.104(d) as secondary research for which consent is not required.
Data Source and Sample
An information analyst retrospectively extracted patient sociodemographic information, clinical history, and encounter specific data from the electronic health records (EHRs) using the Clarity database, a subset of data from the Epic EHR system used to capture all patient health information. The study population consisted of all unique patients aged 12 through 17 years who were seen in primary care and had at least 1 documented and completed PHQ-9 screener between September 2017 and March 2021. The PHQ-9 was administered to patients annually as the standard depression screener during adolescent health maintenance visits or as needed for follow-up or depression management visits. Questionnaires were administered to adolescent patients by check-in staff or medical assistants using tablets or paper and pencil forms during check-in or rooming, depending on clinic-specific workflow. Once the adolescent completed the questionnaire, responses were entered into a structured data entry form within the EHR by medical assistants or by PCPs. The PCP would discuss responses with the adolescent and conduct a risk assessment if suicidal ideation was verbally indicated or endorsed on the PHQ-9. For the purposes of this study and consistent with screening guidelines for this age group, 22 a score ≥10 or an endorsement of suicidal ideation (item #9, “Thoughts that you would be better off dead or of hurting yourself in some way”) was considered a positive screen.
Study Variables
Primary care provider post-screening responses
The research team identified 5 post-screening PCP responses that were available via structured EHR data extraction (ie, did not require manual chart review) and aligned with pediatric depression screening guidelines for PCPs to identify and treat (when appropriate) depression symptoms and to refer and monitor symptoms.10,12 Primary care provider post-screening responses included whether: (1) a follow-up PHQ-9 screen was completed within 56 days of the index screen, per AAP and NCQA guidelines,10,12 (2) a new psychotropic medication was prescribed during or within 1 week of the encounter, (3) an order to a mental health service within the health system was entered during the encounter, (4) a mood disorder diagnosis was made associated with the encounter, and (5) a mood problem was listed as a new problem on the patients problem list in the EHR (ie, enables providers to add and resolve problems over time).
Depression severity
The PHQ-9 is a validated, widely utilized depression screener, highly correlated with diagnostic measures of depression across both adult and adolescent populations. 23 The PHQ-9 scores were categorized into previously validated severity categories based on total score ranges that included mild/no depression (scores 5-9), moderate (scores 10-14), moderate to severe (scores 15-19), and severe (20-27). 24 A score of 10 or higher or the endorsement of question 9 (thoughts of suicide; ≥1) represents the clinically significant cut-off that was used to guide clinical decision-making across primary care sites. Determination of a likely diagnosis of Major Depressive Disorder was identified using item response patterns that reflect the Diagnostic and Statistical Manual of Mental Disorder (5th ed.; DSM-5) diagnostic criteria.
Sociodemographic information
Existing EHR data fields were used to collect data on patient age, sex, race/ethnicity, and insurance status. This information is typically entered at the time of patient registration. Patients were divided into 2 age groups for analyses (12-14 years and 15-17 years). Race and ethnicity categories were based on available data through the EHR and were limited to the following categories as listed verbatim in the patient EHR: “Caucasian,” “Black and African American,” “Asian,” “Hispanic,” “American Indian/Alaskan Native,” and “Other/Unknown.” Insurance status was determined using a patient’s primary insurance listed in the EHR at the time of the screening encounter and included publicly funded insurance plans (ie, Medicaid), private insurance plans, and other (eg, self-pay, automotive insurance).
Primary care specialty
Primary care specialty included 2 categories: (1) patients seen within a general pediatrics clinic and (2) those seen in a family medicine/med-pediatrics clinic. General pediatric providers specialize in only pediatric and young adult patients and providers in family medicine/med-pediatrics see both pediatric and adult patient populations.
History of depression and anxiety
Patient history of depression and/or anxiety problems were identified if the patient had a mood or anxiety problem currently listed as an existing problem in their medical record, had a mood or anxiety concern that was marked as resolved in their medical record prior to their PHQ-9 screening encounter date, or the patient had a mood or anxiety diagnosis made on a previous visit encounter that occurred prior to the screening encounter date. Keywords were used to identify mood or anxiety diagnoses on the patient problem list and visit diagnosis lists.
History of medication prescription
Order start dates for all psychotropic medications were pulled from the medical record, including historic medication prescriptions and existing medication management records. Medications included all categories of antidepressant medication, stimulants, antipsychotics/neuroleptics, and mood stabilizers. A medication inclusion list was created a by child and adolescent psychiatrist on the research team.
History of referral to health system mental health services
Referral orders were those made to in-house mental health services. These were identified by reviewing referral request dates and standardized order text used when referrals are entered into the patients EHR. Referral orders to institutional pediatric psychiatric, psychology, and adolescent-focused mental health providers were identified across screened adolescents. Referrals made to mental health services within the community were not readily available using automated data extraction methods and were not included.
History of emergency department visits
Emergency Department (ED) visits within the health system (Children’s Emergency Services and Psychiatric Emergency Services) were examined and identified for each patient if the chief complaint for the ED encounter was related to a mood concern. Keywords were used to filter chief complaint encounters to ensure the inclusion of the wide range of mood problems that could be assigned by ED providers.
Statistical Analysis
Sociodemographic variables and clinical characteristics were summarized for the target subsample of patients who presented with at least 1 positive PHQ-9 screen during the study period. One-way and 2-way frequency tables were obtained to study post-screening responses to positive screens. Logistic regressions were estimated to determine the odds of each post-screening response across provider specialty, patient sociodemographic factors, and patient clinical history. Predicted probabilities were obtained as well as average marginal effects for each predictor variable using the margins command. All analyses were conducted using Stata/SE release 15. 25 Patient records were excluded if they had an incomplete screener, preventing the calculation of a total score or if the patient was ≥18 years of age at date of the PHQ-9 visit encounter.
Results
From September 2017 to March 2021, 14, 194 unique patients with an associated completed PHQ-9 screener were identified (see Figure 1). Patients who were 18 years or older at the time of their first screen were removed, resulting in a total of 12, 227 unique adolescents with a completed PHQ-9 questionnaire during a primary care visit. We identified 2925 patients with at least 1 positive screen (ie, PHQ-9 total score ≥10 or endorsement of suicidal ideation on question 9), 223 of whom were removed due to patient age at first positive screen date (≥18 years), resulting in a final subsample of 2702 unique patients 12–17 years of age, with at least 1 positive PHQ-9 score recorded in their medical record.
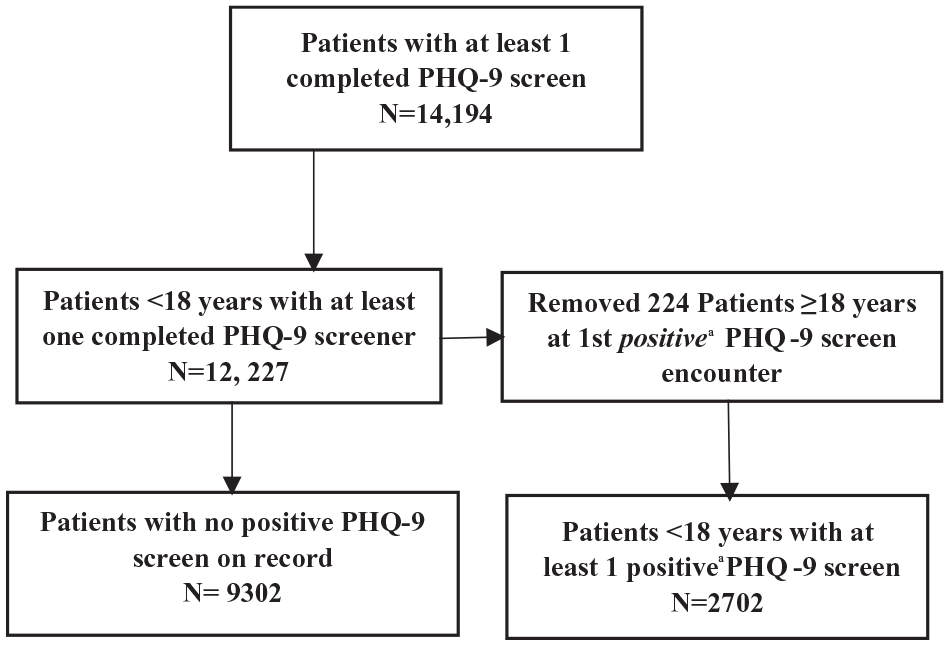
Sampling flowchart.
Sociodemographic and clinical history data are presented in Table 1 for 2702 patients with at least 1 positive PHQ-9 encounter during the study period. Approximately three quarters of the above patients were ages 15 to 17 years, and they were mostly white (70%) and identified as female in their EHR (67%). Seventy percent were privately insured, and most patients were seen in a pediatric specialty clinic (72%) vs a family medicine clinic (28%). About one quarter of this subsample of patients had a history of a mood or anxiety concern listed in their medical record prior to the screening encounter, with 12% having a documented emergency room visit related to a mood concern. About one-third of patients either had a history of psychotropic medication prescription at the time of their screen or were actively prescribed a medication treatment regimen. Finally, 3% of patients had prior history of a documented mental health referral made to a program housed within the health system (eg, Child and Adolescent Psychiatry).
Patient Sociodemographic Characteristics and Clinical History Information (N = 2702).
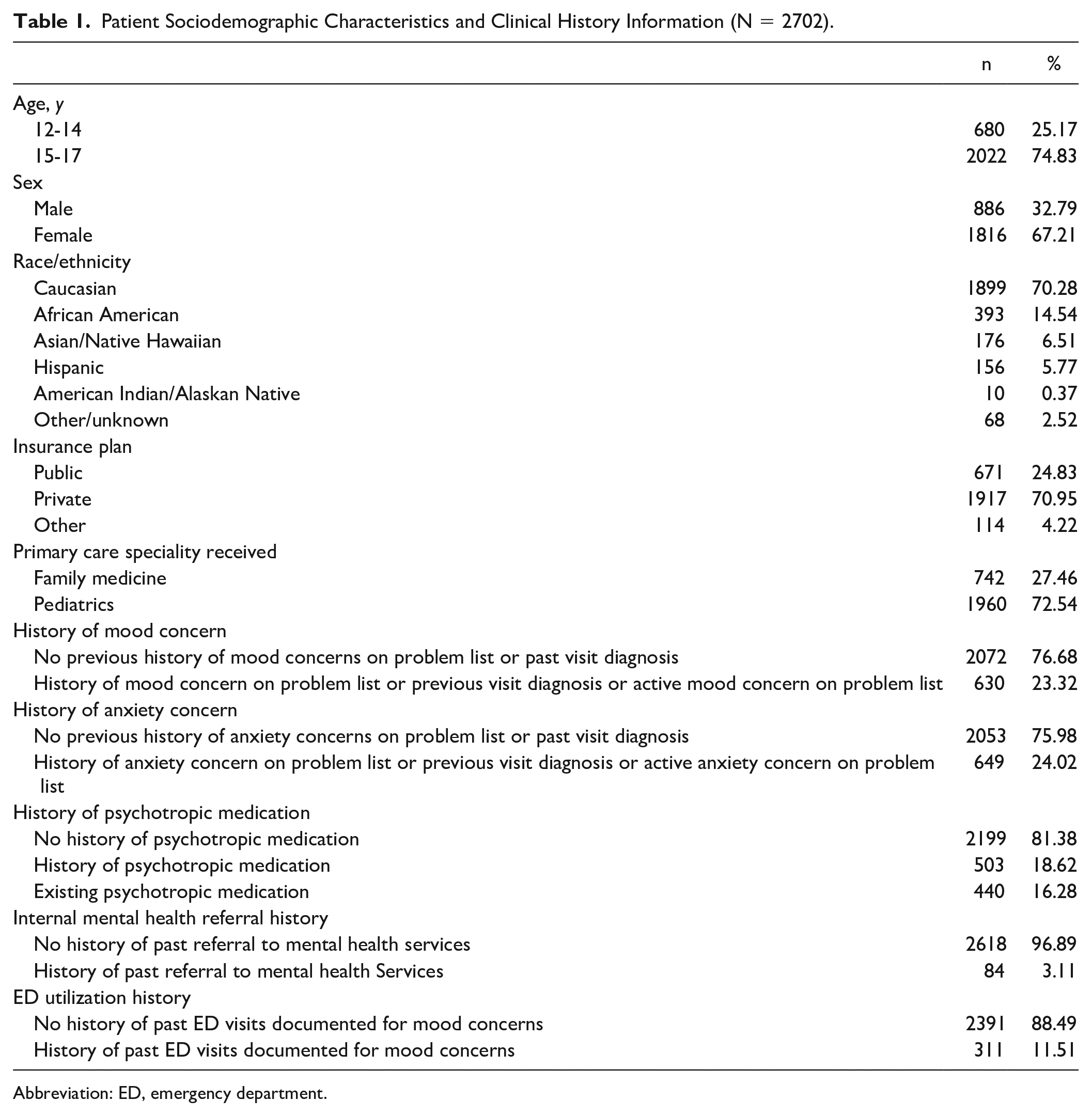
Abbreviation: ED, emergency department.
The percent occurrence of each post-screening response is summarized in Table 2 across all sociodemographic and clinical history variables. Among the 2702 patients, EHR documentation indicated 21% were provided a repeat follow-up screener within the recommended 8-week timeframe, 12 5% were prescribed a new psychotropic medication, 5% were referred to mental health services within the health system, 14% were given a visit diagnosis that included a mood concern, and 24% had a mood problem listed on their problem list at the time of the encounter. Approximately 49% of patients received at least one of the above post-screening responses.
Percentage of Post-Screening Provider Responses Across Patient Sociodemographic Characteristics and Clinical History Information.
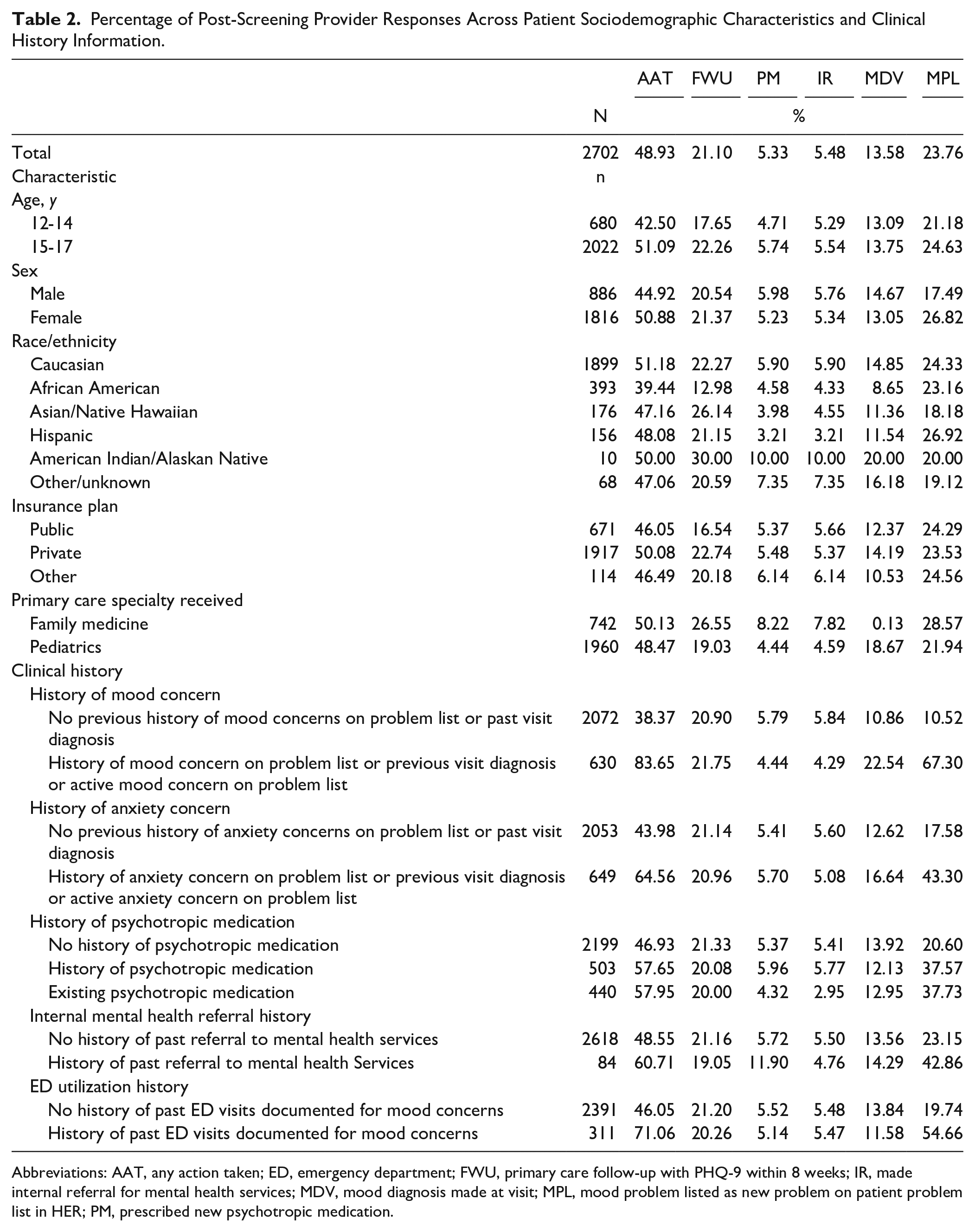
Abbreviations: AAT, any action taken; ED, emergency department; FWU, primary care follow-up with PHQ-9 within 8 weeks; IR, made internal referral for mental health services; MDV, mood diagnosis made at visit; MPL, mood problem listed as new problem on patient problem list in HER; PM, prescribed new psychotropic medication.
The average marginal effects were calculated to determine the predicted probability of each response across patient sociodemographic variables and mental health history characteristics (see Supplemental Appendix A for Average Marginal Effects Tables). Patients in the older age category and patients with private insurance coverage had a higher predicted probability of receiving an 8-week follow-up screener. Follow-up screeners were predicted to be completed less often among those seen by a pediatric specialty provider. A lower percentage of Black patients were predicted to have a documented follow-up screener and to receive a diagnosis of depression. Patients who saw a pediatric primary care specialty provider had a lower predicted probability of being prescribed medication, a higher probability of being identified as having depression during the screening encounter visit diagnosis, and a lower probability of receiving an internal mental health referral and of having a mood concern listed on their problem list.
Patients who endorsed more severe depression presentation had a higher predicted probability of a documented follow-up screener within 8 weeks of their initial screen and were found to be more likely to be identified as “depressed.” A significant mental health history of a mood concern resulted in higher predicted probability of identification of a mood problem during the visit encounter and listed on the patient’s problem list. A history of anxiety predicted a diagnosis of a mood concern during the visit encounter. Finally, patients who had a history of a prescribed psychotropic medication, were currently on medication at the time of the screening encounter, or had a history of an internal mental health referral had a higher predicted probability of being identified as depressed on the patient problem list.
Using the model-based predicted values, the predicted probabilities of post-screening responses for each of the above factors are presented in Figure 2. Predicted probabilities for family medicine providers were higher than pediatric providers across all post-screening responses, except documentation of a mood problem within the visit diagnosis. White patients were observed to have higher predicted percentages for the provision of follow-up care and for mood disorder diagnosis at the visit compared to Black patients. Similar findings were observed among the older age group (15-17 years), who had higher predicted probability of receiving a follow-up screen than the younger age group.
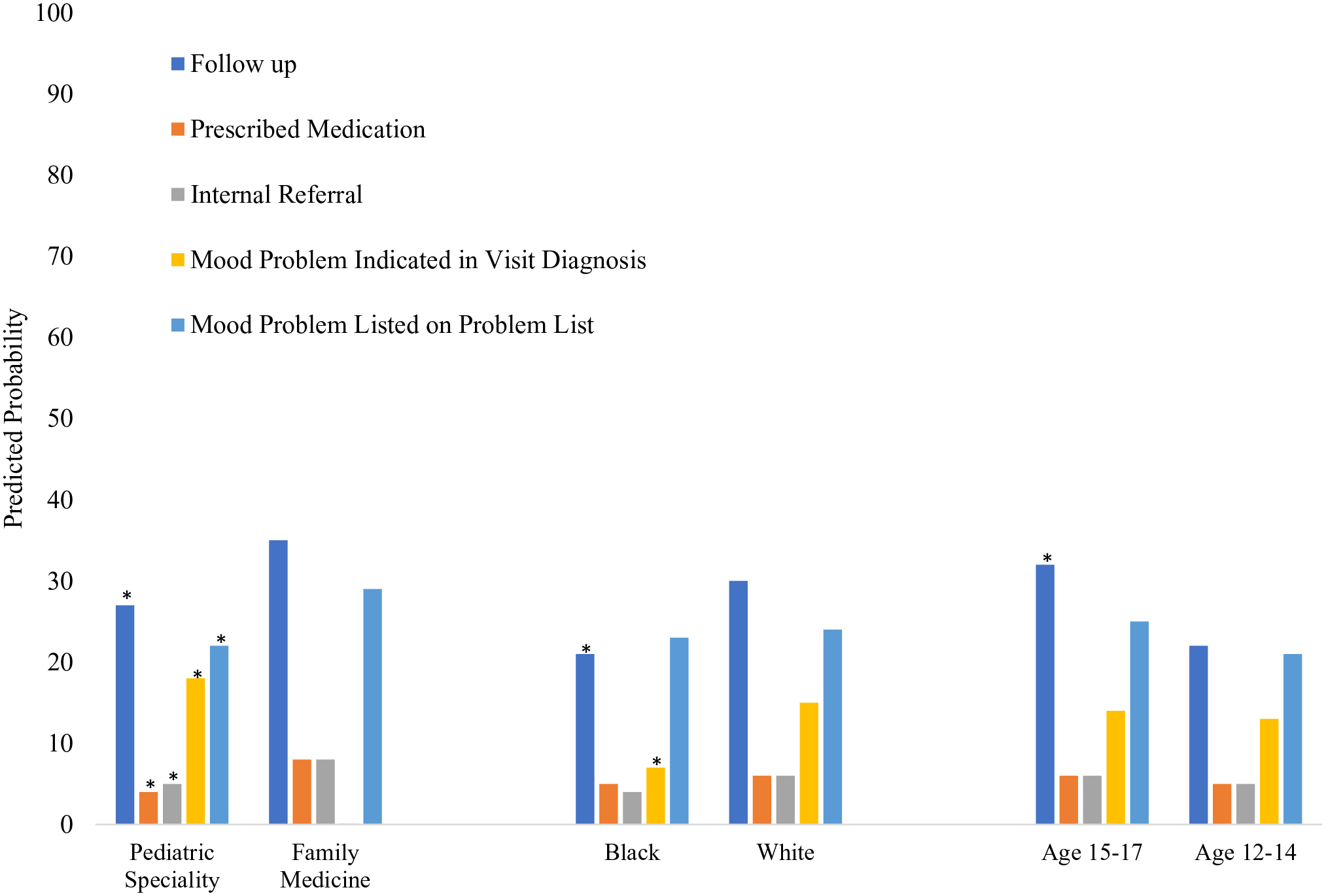
Predicted probabilities of post-screening responses to positive depression screeners across provider specialty, patient race, and patient age.
Discussion
This is the first study to our knowledge that has examined post-screening responses in the context of guidance-driven depression management in primary care. We included a large patient sample across 17 pediatric and family medicine clinics. We were inclusive of all patient screening encounters regardless of visit type and measured mental health and medication history as predictors of interest. Findings were not measured in the context of quality improvement or practice change initiatives.
National quality standards for adolescent depression management in primary care highlight the importance of conducting a follow-up screener within 2 months of the initial positive screen.10,12 Moreover, studies have found that elevated scores on repeat screeners was a strong predictor of depression persistence 6 months later. 26 Although the efficacy of repeated measurement is well understood, 27 studies reporting real-world depression screening outcomes have found follow-up screening rates to be low among pediatric patients. 7 Our findings add to the literature by suggesting the possible influence of specific patient or provider-level factors on post-screening follow-up care practices.
Significant differences in the predicted probabilities of provider actions were found across sociodemographic variables, symptom severity, and clinical history among the 2702 patients who had a positive screen during a primary care encounter. Older adolescents had higher predicted probability for repeat screening in reference to the younger age category. This finding aligns with epidemiological research pointing to increasing depression prevalence with age among adolescents. 28 It is also possible that PCPs perceive younger patients to be more likely to initiate a follow-up visit if symptoms become worse because of increased parental monitoring and involvement in the medical care of younger teens. Lower average marginal effects among Black patients and those who are publicly insured may be attributed to under-identification of mood problems due to known mental health disparities faced by Black youth and children from low socioeconomic status (SES) households. 9 It is also possible that differences in care are due to actual inequities in the delivery of depression follow-up care. For example, unconscious bias may exist among providers surrounding interpretation of depression severity and need for repeat screening. System-level factors could also be contributing to inequity in the management of depression among Black and low SES youth (eg, clinics in more racially diverse or low-income neighborhoods are provided fewer resources compared to clinics in White or affluent neighborhoods). Future research should attempt to evaluate whether such inequities exist so that meaningful systems-level solutions can be identified.
Average marginal effects for post-screening provider responses were lower among pediatric specialty providers in reference to family medicine providers. These differences may be due to differences in clinical decision-making practices related to provider specialty training, 29 clinic-specific practice norms, 30 or comfort with selective serotonin reuptake inhibitor (SSRI) management. 31 It is also possible that pediatric specialty providers relied more on narrative documentation of clinical decision-making, which is not captured by structured data extraction. For example, pediatric providers may have documented their treatment decisions differently than family medicine providers. Such documentation differences are important to investigate further, particularly for identifying outcomes for the purposes of quality improvement. A manual review of narrative progress notes would aid a comparison of provider practices, documentation patterns, and help us to better understand the contexts in which decisions were made. In addition, patient-level data are important, as existing studies suggest that patients and families often do not feel repeated screening is necessary and therefore decline follow-up appointments. 7 Future examinations of post-screening provider responses should include information on parent and patient perceptions, if possible, in addition to the provider’s recommendations.
Certain aspects of a patients’ clinical history were also found to result in higher predicted probability of post-screening responses. Patients in higher depression severity categories were more likely to receive follow-up and be identified as having a mood disorder diagnosis. Patient medication history was also predictive of identification of a mood disorder diagnosis, but was not predictive of the other post-screening responses. Although documentation of a past mood or anxiety concern was predictive of provider identification of a mood concern post-screening, these patients did not have a greater predicted probability of receiving follow-up care, medication, or a referral. Primary care providers may have been more likely to monitor or intervene if a patient’s symptoms were ongoing. However, these patients may be more likely to be engaged in services or therapy at the time of screening and therefore may not have required ongoing support. Manual chart review would be required to determine whether this group of patients was more likely to be engaged in services at the time of the screening encounter. Few studies have examined mental health history in relation to screening practices, yet this may be an important predictor of how depression screeners are interpreted and lead to treatment recommendations.
There are several limitations of this study. First, patient outcomes were sampled from a single medical system. Although data were collected across multiple clinics, demographic variability was limited to mostly suburban geographic regions covered by the health system. Second, the information gathered was limited to what could be extracted systematically from the EHR. Therefore, nuanced information regarding provider actions was not accessible, including whether community referrals were made or if medication or follow-up was attempted but declined by the patient. A follow-up study that includes in-depth chart review of visit notes would provide more detailed information on provider recommendations, patient response, and rationale for decisions regarding need for follow-up, referral, or treatment. More sophisticated analysis methods such as hierarchical linear modeling (HLM) may have provided stronger insights into issues of care inequity, particularly around differences found between subspecialists, and should be considered in future research. Finally, this study was descriptive in nature and only identifies associations between patient variables and provider actions at the time a specific screener was given, limiting our interpretation of causal relationships between variables and the influence of events that occurred prior to administration. This is especially true when evaluating risk of bias in patient care.
Our observations of post-screening provider responses to elevated depression screeners offer important directions for future research and quality improvement efforts. Identification and symptom monitoring are critical components of quality standards for depression screening in pediatric primary care settings.10,12 Understanding the patient-level and provider-level factors related to provider referral and treatment practices provides important directions for further investigation of mental health treatment disparities, inequities, and barriers to care. Future research should further investigate how patient age, race, and provider specialty impact depression care among youth seen in primary care.
Author Contributions
All authors contributed to the conception/design of the of the study or contributed to the acquisition, analysis, or interpretation of data presented in this manuscript. All authors contributed to drafting the manuscript or critically revised it for important intellectual content. All authors gave final approval of the manuscript as it is currently written and agree to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228231223782 – Supplemental material for Real-World Depression Screening Practices Among Primary Care Providers Across Patient-Level and Provider-Level Characteristics
Supplemental material, sj-docx-1-cpj-10.1177_00099228231223782 for Real-World Depression Screening Practices Among Primary Care Providers Across Patient-Level and Provider-Level Characteristics by Teryn Bruni, Shawna Smith, Joanna Quigley, Elizabeth Koval, Leah LaLonde, Alexandros Maragakis, Amy M. Kilbourne, Cheryl King, Kelly Orringer and Joyce M. Lee in Clinical Pediatrics
Footnotes
Acknowledgements
The authors thank Jessica Good, MS (Eastern Michigan University) for assisting with data management efforts.
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Institutes of Health (NIH) grant numbers P30DK089503 (MNORC), P30DK020572 (MDRC), and P30DK092926 (MCDTR) from the National Institute of Diabetes and Digestive and Kidney Diseases and the Elizabeth Weiser Caswell Diabetes Institute at the University of Michigan. The study sponsor(s) had no involvement in the study design, collection, analysis, or interpretation of data, manuscript preparation, or the decision to submit this manuscript for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.