
Abstract

Educational Objectives
Treatment of aHUS is blockade of the AC pathway with eculizumab, while acutely, appropriate supportive treatment is crucial.
Mutations of complement regulatory proteins should be sought in patients with aHUS.
Introduction
Atypical hemolytic uremic syndrome (aHUS) is a rare disorder characterized by dysregulation of the alternate complement pathway. 1 Most patients have their initial episode of aHUS before the age of 2.2-4 Episodes may be triggered by a variety of factors such as drugs, rheumatologic disease, malignancy, and immunization, but the most common trigger is infection (responsible for 50%-60% of episodes), including viruses. The trigger remains undetermined in one third of episodes.1,4 Coronavirus disease 2019 (COVID-19) should be kept in mind as a possible trigger for aHUS. In such patients, genetic studies of the complement regulatory proteins should be undertaken. We hereby present a critically ill patient who needed respiratory support and dialysis due to aHUS triggered by severe acute respiratory syndrome coronavirus 2 (SARS-CoV 2) infection to emphasize the fact that patients with preexisting renal disease may be predisposed to aHUS and a severe clinical course that may be triggered by intercurrent infections such as COVID-19.
Case Presentation
Fourteen-year-old girl presented with fatigue, anorexia, and cough during the preceding 3 days. Her medical history was significant for nephrotic syndrome (NS), which was steroid resistant. The patient was diagnosed with focal segmental glomerulosclerosis (FSGS) at the age of 7, when she presented with proteinuria, diagnosed incidentally, with no symptoms suggestive of renal disease. Kidney biopsy performed at that time had revealed no immune complexes and histology was consistent with FSGS. She was started on cyclosporine. Genetic testing revealed a heterozygous LMX1B mutation (c.737G>A, de novo) at the age of 7, which is expected to be resistant to immunosuppression. Cyclosporine was stopped, and she was started on enalapril for proteinuria and atorvastatin for hypercholesterolemia. The patient did have FSGS but remained clinically stable on ACE inhibitors on 7 years follow-up. She had good renal function, with a urea level of 58 mg/dL and creatinine level of 0.8 mg/dL 1 month prior to this presentation. The total protein/creatinine ratio was 1.64 in the values of this patient before the admission. She never had any previous hospital presentations due to attacks of acute kidney injury or edema and fluid overload prior to this hospitalization.
On physical examination at admission, she had bilateral pretibial edema, hypertension (152/100 mm Hg), tachycardia (150 beats per minute) and tachypnea (30-40 breaths per minute). Her breath sounds were decreased bilaterally, particularly at lung basis, indicating loss of aeration. Her physical examination was otherwise unremarkable. Because she had a cough and respiratory distress, COVID-19 was considered, and SARS-COV-2 PCR result was positive. Laboratory values at the patient’s admission were as indicated in Table 1. Schistocytes were noted on peripheral smear (Figure 1). Direct antiglobulin test was negative. Coagulation studies were within normal range. She was anuric. She was diagnosed with aHUS based on the constellation of acute kidney injury (AKI), microangiopathic hemolytic anemia (MAHA), thrombocytopenia and normal C3 levels. Considering typical clinical and laboratory findings, repeat kidney biopsy, which was unlikely to alter management, was not performed. Evidence of a current respiratory infection rather than an infection in the preceding weeks, lack of fever, gastrointestinal involvement, mucocutaneous involvement, thrombocytopenia, lymphopenia and shock precluded a diagnosis of multisystem inflammatory syndrome in childhood, another COVID-19 associated disease with endothelial damage, according to the current criteria. 5
Laboratory Values at Presentation.

Abbreviations: g/dL, grams per deciliter; mg/dL, milligrams per deciliter; mmol/L, millimoles per liter; µg/L, microgram per liter.
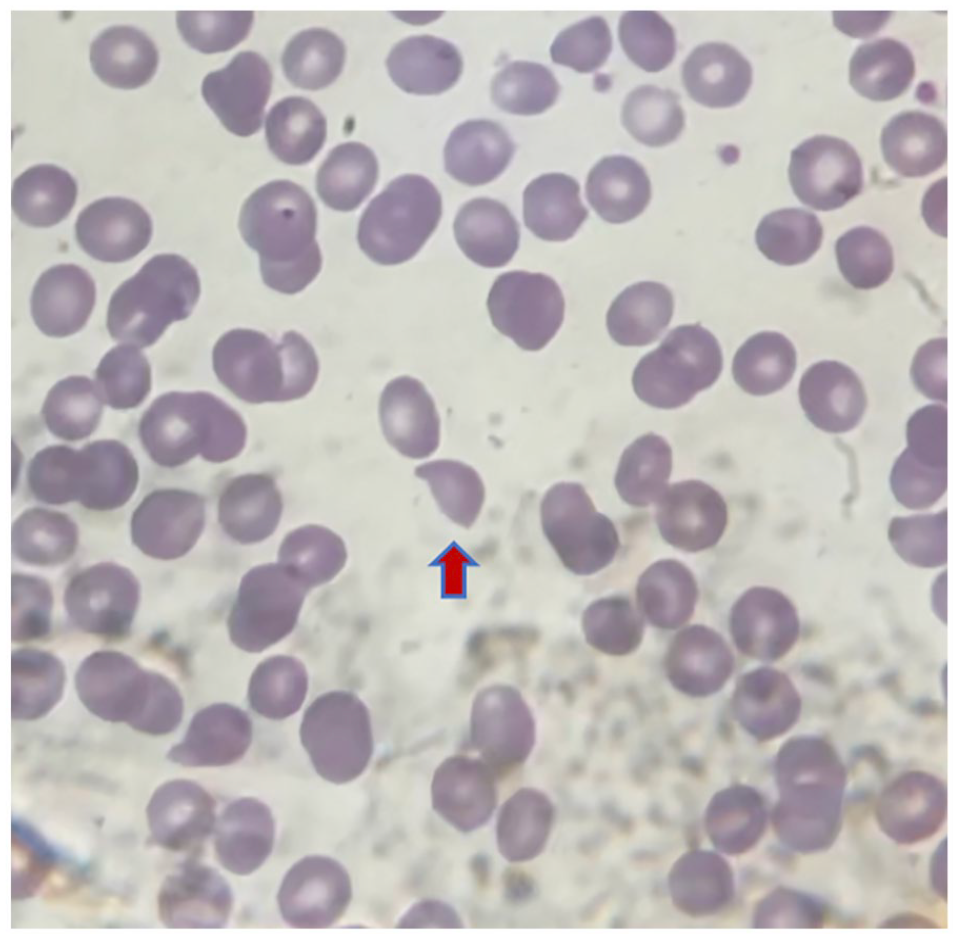
Schistocytes were noted on peripheral smear (red arrows).
She was admitted to the pediatric intensive care unit and intubated due to worsening respiratory distress. Baseline saturation was 91%, breath sounds were decreased on auscultation and diffuse infiltrates were noted on X-ray, consistent with acute respiratory distress syndrome (ARDS). With the literature on the efficacy of IV remdesivir being uncertain and the ARDS being attributed to the aHUS, intravenous remdesivir and steroids were not initiated. 6 She underwent 3 daily sessions of therapeutic plasma exchange (TPE) (1.5 × plasma volume on day 1 and 1 plasma volume on subsequent days) (Prismaflex, Baxter International Inc., Illinois, USA) for aHUS. Fresh frozen plasma was used as replacement fluid to restore possibly depleted ADAMTS-13. A blood sample was drawn to check for ADAMTS-13 levels before TPE. The result was obtained on day 3 and was normal, confirming aHUS (0.61 IU/mL). Thereafter, the patient was started on eculizumab. Appropriate immunizations for encapsulated bacteria were provided, and lifelong penicillin prophylaxis was initiated after discontinuation of antibiotics.
The patient also needed a variety of supportive measures. Her ARDS required invasive ventilation with a lung protective strategy using high positive end expiratory pressure (PEEP) and low tidal volume (<6 mL/kg). She was started on a PEEP of 15 cm H2O, which was gradually weaned down. She was extubated on day 11, after which she was supported with noninvasive ventilation. Her cardiac dysfunction with an ejection fraction of 50% necessitated milrinone infusion for 9 days. She needed continuous renal replacement therapy for renal support and maintenance of fluid balance until she reached cardiorespiratory stability and could tolerate intermittent dialysis (Figure 2). She had hypertension, which persisted despite amlodipine, atenolol, and doxazosin, required glyceryl trinitrate infusion and ultimately responded to minoxidil. She was transferred to the pediatric ward on day 28. Throughout the first 2 weeks, she required 10 packed red blood cell transfusions. Thrombocytopenia improved at the end of week 1. However, she needed transfusions for up to 4 months. She remained anuric throughout her PICU stay. Unfortunately, although she started producing urine, amounts remained below the threshold of anuria. Therefore, she remains on a chronic hemodialysis program. Her genetic aHUS panel revealed a heterozygous, pathogenic nonsense mutation on the complement factor H gene (c.877C>T). She was discharged from the hospital after 2 months.

This chart summarizes certain aspects of our patient’s clinical course including laboratory values and treatment modalities.
Discussion
Mutations or autoantibodies may disrupt the function of regulatory proteins of the alternative complement (AC) pathway, which may cause uncontrolled AC activation and aHUS, characterized by MAHA, thrombocytopenia and AKI. Mortality rates are around 25% and about half of the patients ultimately have dialysis-dependent end-stage renal disease. 1 Renal involvement frequently causes hypertension.
Complement-mediated hemolytic anemias have been reported to flare with COVID-19. To date, 9 adults have been reported to have HUS in the setting of COVID-19, 8 of which were found to have COVID-19 and aHUS concomitantly, while in 1 patient, there were 2 days between the onset of COVID-19 and hemolysis. 7 Pediatric reports are much scarcer. One 3-year-old Turkish child with consanguineous parents and a history of 2 siblings succumbing to unknown cause at the ages of 7 months and 1.5 years, 8 and two Roman Bulgarian infants with mutations in the EXOSC3 gene, which encodes a multiprotein ribonuclease complex crucial for RNA processing 9 were reported. One 14-year-old adolescent girl was reported to have TMA triggered by COVID-19, which required intubation. That patient also had extreme hyperferritinemia (>100 000 ng/mL and rhabdomyolysis with creatine kinase levels of 55 695 U/L). However, her renal function recovered, while our patient remains on dialysis. Furthermore, unlike those patients, who needed no more respiratory support than oxygen by mask, our patient had severe ARDS requiring high PEEP and cardiac dysfunction requiring milrinone.
Extrarenal involvement is common in aHUS. Central nervous system (altered level of consciousness, drowsiness, seizures, encephalopathy, cortical blindness), lungs (pulmonary hemorrhage), circulatory system (cardiomyopathy, myocardial infarction, heart failure), and muscles (rhabdomyolysis) can be involved.1,3 Our patient had severe ARDS, which required invasive mechanical ventilation with high PEEP and cardiac dysfunction. Such involvement is rare in aHUS. 10 We think that possible culprits for this particularly severe disease course in our patient may be COVID-19, baseline endothelial dysfunction (ED) due to NS or both.
Most patients who had aHUS flare triggered by COVID-19 are renal transplant recipients, who have a variety of risk factors including tacrolimus use and ischemia-reperfusion injury. NPHS2, WT1, and NPHS1 stand out as the most frequently observed mutations in steroid-resistant NSs. Although the LMX1B mutation is not as frequent as those mentioned above, it can cause FSGS without extrarenal involvement. 11 Our patient had isolated NS due to LMX1B mutation and was stable on ACE inhibitor monotherapy for proteinuria. No reports exist yet of aHUS triggered in the setting of an LMX1B mutation. Endothelial dysfunction has been shown in adults and children with NS due to a variety of causes.12,13 However, we believe that ED due to the underlying renal disease may have predisposed the patient to further ED and TMA or led to a more severe disease course. One cause of TMA is uncontrolled malignant hypertension. However, our patient was clinically stable before this HUS episode and had normal blood pressure recorded during outpatient follow-up. 14
Genetic predisposition, namely, mutations in AC regulation, is common in patients with aHUS. Determining the underlying mutation with genetic testing is warranted, if possible, even if there are known triggers. Finding the mutation may help guide management and estimate recurrence risk after renal transplantation (Table 2). Our patient’s genetic atypical HUS panel revealed a heterozygous, pathogenic nonsense mutation on the complement factor H (CFH) gene (c.877C>T). Disruption of the CFH function is associated with a particularly severe phenotype, which may also explain our patient’s renal nonrecovery. 15 Scarce reports in the literature mention coexistence of FSGS and HUS. Unfortunately, these reports are not recent and do not report complement protein levels. 16
Commonly Seen Mutations Associated aHUS.

Abbreviation: aHUS, atypical hemolytic uremic syndrome.
Treatment of aHUS has 2 main components, namely, acute supportive treatment, and blockade of AC dysregulation. Acutely injured kidneys and lungs may further damage each other in critical illness. Therefore, conservative fluid management with judicious fluid administration, avoidance of positive fluid balance, timely initiation of diuretics and CRRT may prevent further worsening of lung function while lung-protective ventilation with low tidal volume and optimal PEEP may prevent propagation of AKI.17,18 Therapeutic plasma exchange is beneficial through removal of autoantibodies and proteins mediating endothelial injury and restoration of normal ADAMTS-13 levels. However, it does not address the underlying complement dysregulation. Eculizumab, currently the principal chronic treatment option in aHUS, prevents cleavage of C5 into C5a and C5b, thereby blocking formation of the membrane attack complex, thus preventing ED. 1 It seems to be effective in treating the initial episode, as well as preventing recurrence and renal recurrence after transplantation. Earlier initiation may lead to improved renal outcome.1,19,20 Our patient had hematologic remission, but unfortunately, due to a combination of the effects of COVID-19, chronic ED due to NS and her mutation, she remains on dialysis.
Conclusion
Microangiopathic hemolytic anemia, acute kidney injury, and thrombocytopenia in the absence of a diarrheal illness should prompt consideration of aHUS. It should be remembered that in addition to this triad, acutely, aHUS may involve all body systems. Mechanism of illness involves disruption of AC pathway regulation due to genetic causes or autoantibodies. Determination of the particular mutation may help in prognostication. Chronic treatment is AC blockade, while acute treatment is supportive. Patients with underlying baseline ED may experience a more severe disease course or more adverse ultimate outcome. 1
Author Contributions
AGG, SI: Treated the patient, collected data, drafted the manuscipt.
DD, ZYY: Treated the patient, provided critical oversight during writing and revised the manuscript.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval/Patient Consent
Our study did not require an ethical board approval because this was a case report and not a study, so informed consent was waived.