
Abstract
In this single-site, retrospective, descriptive chart review and survey, we investigated changes in pediatric behavioral health needs during the COVID-19 pandemic and the relationship between virtual schooling and hospitalized children’s mental health. Subjects included patients aged 6 and 18 years during the 2015 to 2019 and 2020 to 2021 school years who received inpatient mental health care. Parents of patients admitted in 2020 to 2021 were surveyed regarding their child’s schooling. We additionally described and compared subjects using descriptive data, including proxies for illness severity, and assessed how these outcomes changed during the pandemic and correlated with school modality. During the pandemic, the distribution of diagnoses changed, and some markers of severity increased. Patients in exclusively virtual school had higher rates of mood and anxiety disorders and tic disorders, and lower rates of eating and disruptive behavior disorders, than patients with recent in-person school. Further study is needed regarding the impact of virtual schooling on pediatric mental health.
Keywords
Introduction
The COVID-19 pandemic has had a devastating impact on children’s mental health. Since early 2020, studies have noted significant increases in pediatric depression, anxiety, suicide attempts, self-injurious behavior, aggression, and eating disorders.1-8 Numerous professional and governmental agencies have recognized that this situation constitutes an unprecedented emergency in pediatric mental health.9,10
Although the mechanisms driving this crisis are complex, one frequently cited area of concern is school closures.11-15 The abrupt shift to virtual school led to increased psychological distress among students,16,17 and placed increased financial and social stress on families, which has been associated with an elevated risk of abuse and neglect.18-20 Students’ engagement in virtual schooling can be low,21,22 and most working parents cannot provide the level of involvement demanded by such programs. 23 Limitations of virtual schooling are especially pronounced in rural areas, which often lack broadband infrastructure and where children already face increased risk of suicide and other mental illness. 24
The relationship between school modality (in-person vs virtual) and students’ mental health during the pandemic remains unclear. The unfortunate circumstances of the pandemic provide an unusual opportunity to understand the impact of immediate school closure, disruptions in schooling, and changes in school modality on pediatric mental health. We therefore investigated what relationship, if any, exists between school modality and pediatric mental health as measured by inpatient mental health service utilization. In this study, we describe youth who received inpatient mental health care at a single site during the school years between 2015 and 2019 (pre-pandemic period) and 2020 to 2021 (intra-pandemic period), exploring the impact of in-person and virtual learning in the 3 months preceding admission. We hypothesized that patients who attended virtual school immediately prior to admission would display signs of more severe mental illness than patients who attended school in-person. We also postulated that the severity of presentation and overall demand for inpatient mental health services would increase during the 2020 to 2021 academic year compared with pre-pandemic years.
Methods
Setting and Population
The study site is a 234-bed academic, urban, midwestern, tertiary care children’s hospital, with 7800 inpatient discharges and 22 700 emergency department visits annually. The study population included all patients aged 6 to 18 years, inclusive, admitted to the study site during the 2015 to 2019 and 2020 to 2021 school years (September 1-May 31 of each year) who received psychiatry and/or psychology consults, and/or were admitted to the inpatient psychiatry unit. We did not include the 2019 to 2020 school year, as from March to June 2020 up to 20% of study site beds were allocated to adult COVID patients. Furthermore, during that time, psychiatric admissions were contracted due to bed availability and infection control measures per the health system’s COVID surge response. Patients were excluded if they were seen by psychologist within the Department of Physical Medicine and Rehabilitation or the Bone Marrow Transplant service, as these patients are automatically seen by a psychologist for coping with physical illnesses regardless of the presence of psychopathology.
Study Design
This is an institutional review board (IRB)-approved retrospective, descriptive study (HUM00206993) combining chart review and survey components, exploring the prevalence of mental illness, as well as proxies of illness severity, among inpatients at the aforementioned site. Parents of intra-pandemic participants completed a telephone survey to explore engagement in virtual or in-person schooling prior to hospitalization (Supplemental Appendix). The survey was developed by 2 members of the study team, one with expertise in Pediatric Hospital Medicine and another with expertise in Pediatric Consultation-Liaison Psychiatry, with a focus on ensuring face and content validity.
Statistical Analysis
Univariate statistics were used to describe the sample. Chi-square and Fisher’s exact tests were used to test for differences in prevalence measures between groups (pre-pandemic vs intra-pandemic, or survey respondents vs non-respondents). Continuous variables (median income, age, and length of stay) were compared using independent sample t-tests or Wilcoxon-Mann-Whitney tests. All analyses were completed using R version 4.2.1.
We report descriptive demographic data (Table 1), admission counts, mental health diagnoses, and proxies of mental illness severity. We included analysis of race and ethnicity due to the presence of well-documented racial and ethnic disparities, both in direct effects of COVID-19 infection and in access to virtual schooling resources.25,26 Diagnoses were determined by International Classification of Diseases, Tenth Revision (ICD-10) codes with all mental health diagnoses being described for each patient. Admissions were classified as scheduled (planned > 1 day in advance), urgent (same-day admissions from the outpatient setting or transfers from an outside hospital), or emergent (admissions from the emergency department). Proxy measures of severity of mental illness included use of as-needed antipsychotic (haloperidol, chlorpromazine, quetiapine, risperidone, aripiprazole, olanzapine, and ziprasidone) or benzodiazepine (midazolam, lorazepam, clonazepam, diazepam, and alprazolam), length of stay, admission type, discharge disposition, and readmission rate within the same school year. These proxy measures have been used in prior studies of pediatric mental health during the pandemic. 27
Comparison of Pre-pandemic (2015-2019) and Intra-pandemic (2020-2021) Groups With Respect to Demographic and Clinical Outcome Measures.
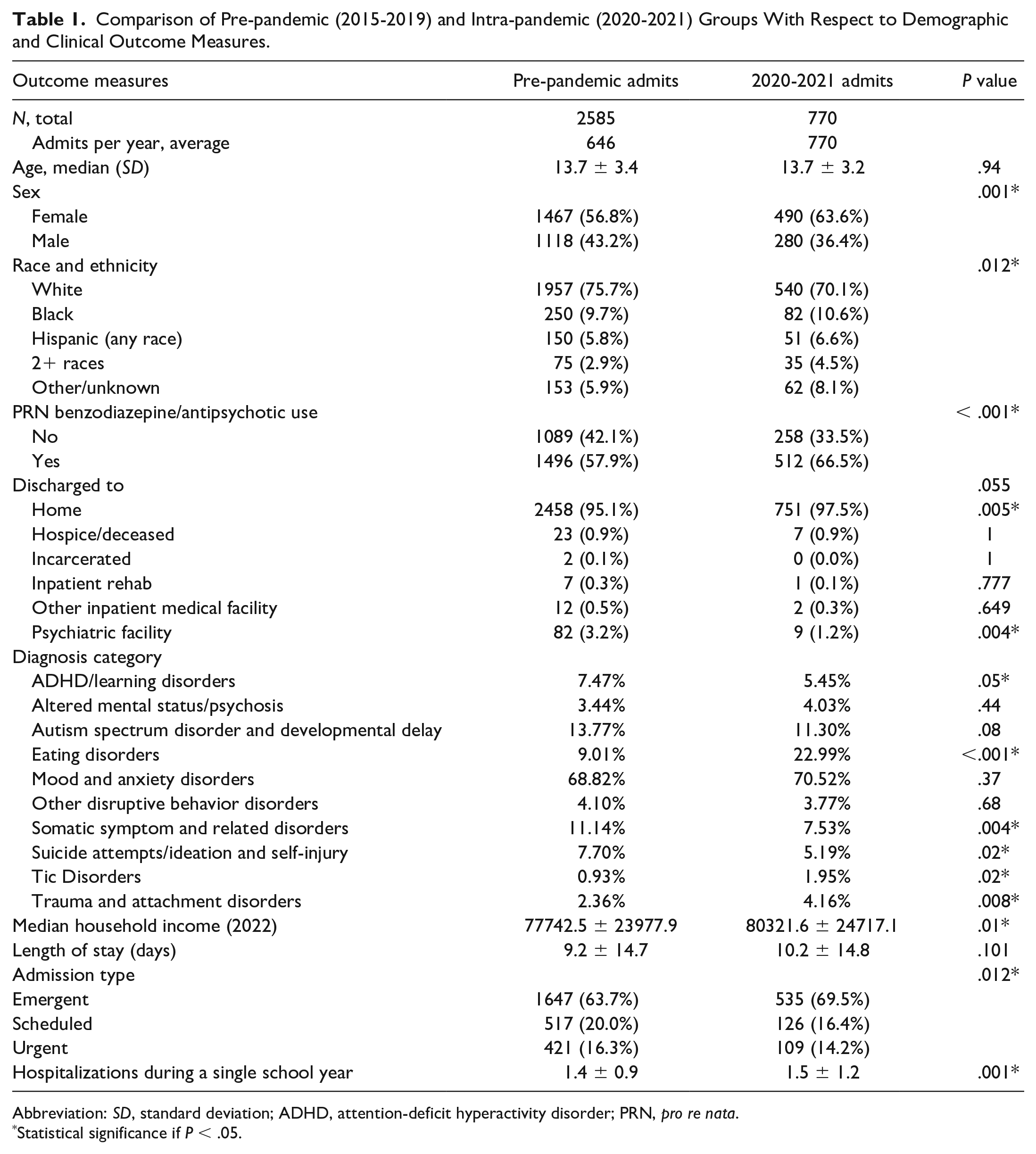
Abbreviation: SD, standard deviation; ADHD, attention-deficit hyperactivity disorder; PRN, pro re nata.
Statistical significance if P < .05.
Associations between these measures and school modality were assessed by comparing intra-pandemic patients who exclusively attended virtual school for the 3 months prior to admission with those who attended at least 1 day of in-person school in that time. Outcome measures were additionally compared between survey respondents and non-respondents to help ensure that children of respondents were representative of the intra-pandemic sample as a whole.
Results
Participant Characteristics
The study sample included 3355 patients (Table 1), including 2585 admitted pre-pandemic and 770 intra-pandemic. The mean age was 14.0 years. The majority of patients were female (58.3%) and white (74.4%). Approximately, one third of invited families (255 of 770, 33.1%) responded to the survey. No significant differences were seen with respect to any outcome measures between the children of survey respondents and those of non-respondents. Lifetime prevalence of virtual schooling was 98.0% among survey respondents. Of those attending virtual school, 77.9% were in virtual school for the majority (greater than 50%) of the 3 months leading up to their first hospital admission, and 60.8% exclusively attended virtual school during those 3 months.
Changes During the Pandemic
Comparisons between all outcome measures before and during the pandemic are shown in Table 1. Patients in the intra-pandemic group were significantly more likely to be female than pre-pandemic (63.6% vs 56.8%, P = .001). The distribution of race and ethnicity also changed significantly during the pandemic, with the proportion of white patients decreasing and the proportion of patients whose race was unspecified increasing. In addition, patients admitted during the pandemic lived in ZIP codes with a median income roughly $3000 higher (in inflation-adjusted 2021 dollars) than pre-pandemic. The distribution of mental health diagnoses changed significantly during the pandemic, relative to pre-pandemic, as well. The proportion of patients with eating disorders more than doubled during the pandemic, from 9.0% to 23.0% of all mental health-related admissions. Smaller but still significant increases were seen in the proportions of patients with tic disorders, as well as trauma and attachment disorders, while the proportions of patients with attention-deficit hyperactivity disorder (ADHD) and learning disorders, somatic symptom and related disorders, and suicidal ideation and/or self-injury decreased. The number of admissions in the study sample rose from 646 per year pre-pandemic to 770 during the intra-pandemic period.
Some markers of mental illness severity also changed significantly during the pandemic. Intra-pandemic admissions were more likely to be emergent and more likely to be readmitted within the same school year. In addition, the intra-pandemic period saw a significantly higher rate of as-needed benzodiazepine and antipsychotic use. More patients were discharged home during the pandemic compared with the pre-pandemic period. There was no significant difference in length of stay between the pre-pandemic and intra-pandemic groups.
Relation to Type of Schooling
Comparisons of all outcome measures between survey respondents (n = 255) in 100% virtual school and respondents with at least some recent in-person school are shown in Table 2. Significant differences were noted between those who attended school 100% virtually versus those who attended at least 1 day of in-person school with respect to the prevalence of certain diagnoses. Mood and anxiety disorders and tic disorders were significantly more prevalent among patients in exclusively virtual school, while eating and disruptive behavior disorders were significantly more prevalent among patients who recently attended in-person school. No significant differences were observed between the 2 groups with respect to any demographic variables or markers of mental illness severity.
Comparison of In-Person and Virtual Schooling Groups With Respect to Demographic and Clinical Outcome Measures.
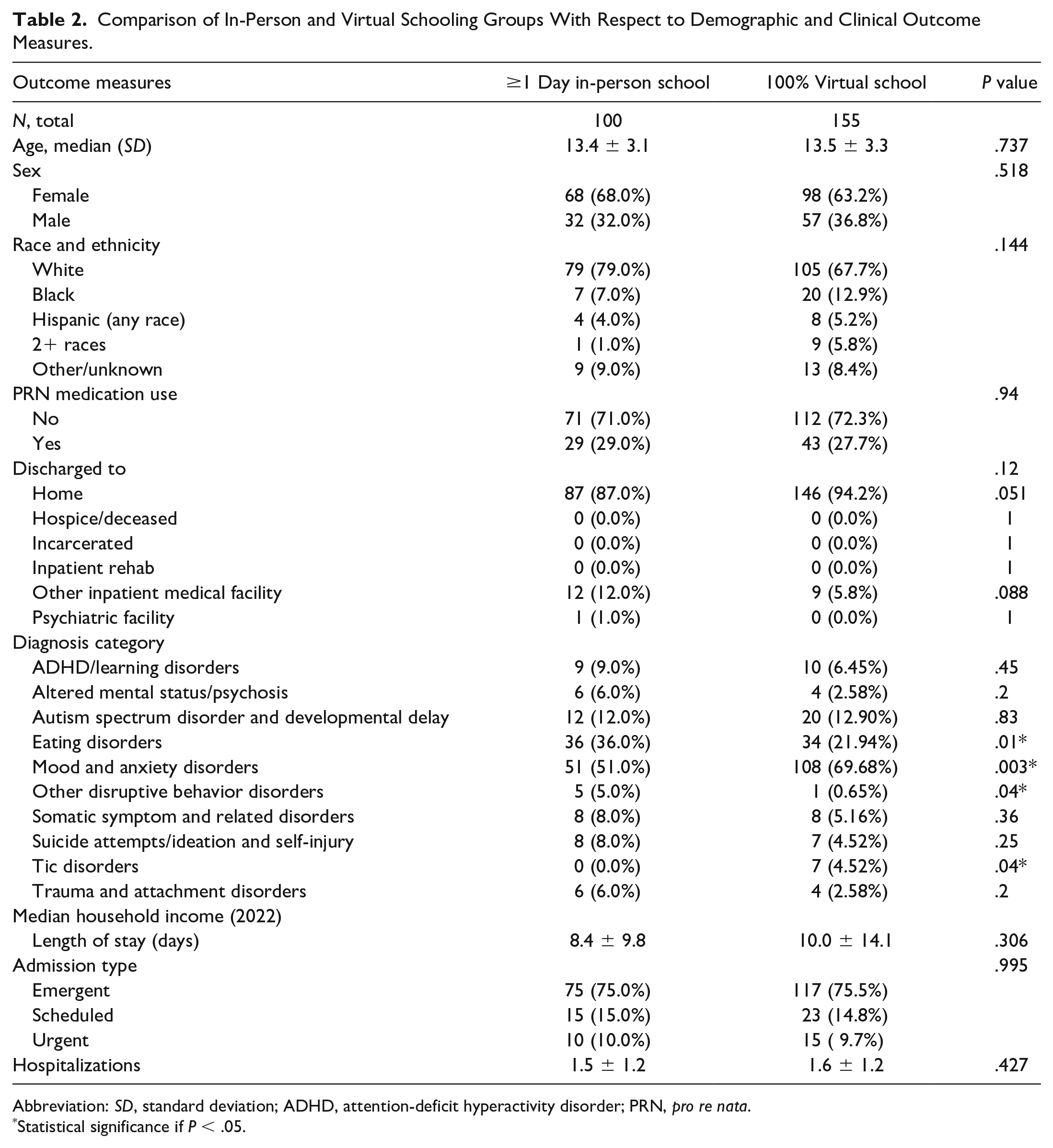
Abbreviation: SD, standard deviation; ADHD, attention-deficit hyperactivity disorder; PRN, pro re nata.
Statistical significance if P < .05.
Discussion
In this retrospective study, we examined trends in inpatient mental health service utilization among pediatric patients before and during the COVID-19 pandemic as well as the relationship between mental health symptoms and school modality (in-person vs virtual) during the pandemic. We observed significant changes in the demographics of patients admitted to the study site with mental health diagnoses before and after the onset of the pandemic. We also observed significant changes in the frequencies of certain mental health diagnoses among patients admitted before and during the pandemic. We did not observe a relationship between recent school modality and the severity of mental health symptoms, as measured by several proxy measures, among patients admitted during the pandemic as hypothesized. However, we did observe significant differences in the distribution of diagnoses between the virtual and in-person schooling groups. We did not note any change in overall demand for mental health services at the study site.
Study participants who attended school entirely virtually for the 3 months prior to admission were more likely to be diagnosed with a mood or anxiety disorder, compared with those who attended at least 1 day of in-person school. Though our study design precludes drawing causative conclusions, this relationship may suggest the social isolation, disruption in routines, and loss of protective factors provided by the school environment associated with school closures may be associated with the development or worsening of such disorders, a phenomenon that has been observed in other pandemic-era studies of the pediatric population.28-31 However, there was no significant difference in the prevalence of mood and anxiety disorders between the pre-pandemic and intra-pandemic study populations. Disruptions in schooling may have acted as a risk factor for the development of such disorders, and it is also possible that patients already at high risk for such disorders may have elected to attend school virtually when both in-person and virtual options were available. Such decisions may have subsequently limited access to school-based counseling and mental health resources for students with greater needs. School districts considering future virtual instruction should be mindful of this finding, and consider providing mental health checks, counseling resources, and/or opportunities for in-person socialization and support, where possible.
Our findings are consistent with prior studies demonstrating significant increases in health care utilization related to eating disorders during the pandemic.32,33 It is unclear what factors contributed to the inverse association between virtual schooling and eating disorders seen in this study; however, school-related social and academic stressors may have been reduced among students in virtual school, who may have also experienced closer parental engagement and supervision. If this finding is replicated in future studies, it warrants further investigation into the possible therapeutic role of virtual instruction for children with eating disorders and at high suicide risk, particularly during periods of intense psychosocial strain, such as the COVID-19 pandemic.
The reasons for the decrease seen in suicide attempts and self-injury, which does not align with prior studies showing increased suicidality among youth during the pandemic, are not clear. 4 Reduced school-related stressors and/or increased opportunity for parental supervision among patients in virtual school may have contributed to this finding, though no difference was seen in these diagnoses between the in-person and virtual schooling groups. As our study population was limited to inpatients, cases of completed suicide were also necessarily not included in our sample, making it difficult to draw conclusions relating to this topic.
Significant differences were additionally noted in the frequencies of tic and disruptive behavior disorders among participants in the intra-pandemic group, with tic disorders more common, and disruptive behavior disorders less common, among patients in exclusively virtual school. Previous studies have identified an increase in functional tic disorders during the pandemic and suggested many of these newly diagnosed tic or tic-like disorders may be related to social media trends.34-36 It is possible that virtual school was associated with greater social media exposure than those in-person school, which may have contributed to this finding. However, the very small numbers of patients with these conditions in our sample (7 and 6 for tic and disruptive behavior disorders, respectively) makes it difficult to draw meaningful conclusions in this regard.
Study participants admitted during the pandemic were less likely to be white compared with pre-pandemic. The commensurate rise in patients of unknown race may be the result of reduced inpatient staffing and/or increased reluctance of patients to disclose their race in the setting of social injustice. These findings may also be related to well-established racial and ethnic disparities in COVID-19-related morbidity and mortality;37,38 however, we did not specifically observe increases in the share of patients who identified as black, Hispanic, or more than 1 race. The proportion of female participants also increased during the pandemic. This effect is likely related to the disproportionate increase in admissions for eating disorders and mood and anxiety disorders in 2020 to 2021, as both categories of illness affect females at higher rates than males.39,40
Lower-income families have been disproportionately burdened by the COVID-19 pandemic and its downstream effects, including reduced access to childcare, employment and related benefits, and public transportation. 41 It is surprising, then, that the median income of our study sample rose between the pre-pandemic and intra-pandemic periods. This is likely the product of widespread challenges to mental health care access during the pandemic and may suggest even higher-income families lacked alternatives to inpatient hospitalization.42-45 However, this result may also have been skewed by geography, with more families presenting from the immediate vicinity of the study site and fewer from outlying communities with lower average income.
Some measures of mental illness severity, as measured by the proxies in this study, increased significantly during the pandemic, compared with the pre-pandemic period. These findings align with prior studies exploring mental illness severity during the pandemic.27,29,46-48 The proportion of patients admitted in crisis from the emergency department, rather than as scheduled or urgent admissions, increased significantly during the pandemic. Utilization of as-needed psychotropic medications, which are typically given to acutely behaviorally dysregulated or distressed patients when less invasive measures, such as verbal de-escalation have failed, also increased significantly during the pandemic. This finding may suggest more severe illness during the pandemic; it may also be related to reduced staffing and/or differences in prescribing patterns between individual providers. Notably, patients admitted during the pandemic were more likely than those admitted pre-pandemic to be discharged home, rather than to inpatient psychiatric facilities. Although this finding may suggest milder illness during the pandemic, it may also reflect worsening shortages of local inpatient psychiatric beds during the pandemic—a phenomenon that may itself have contributed to greater severity of illness and higher rates of rehospitalization. Our results do not support any correlation between recent virtual schooling and severity of mental illness.
This study has several important limitations, particularly with regard to the investigation of school modality. We were only able to survey one third of families whose children were admitted at a single site, creating the possibility of significant response bias. Parental recollection of their children’s school modality immediately prior to admission was likely imperfect, particularly since the survey was completed 8 months after the end of the 2020 to 2021 school year. Our analysis also involved a large number of individual comparisons. While these comparisons involved were not independent of one another, and thus do not necessitate the use of a Bonferroni or other similar correction, it is possible that the effects seen in this study could be the result of a type I error. Furthermore, we did not attempt to capture longer-term data about virtual schooling, and patients who had been in virtual school for periods greater than 3 months may have experienced different mental health effects compared with patients who switched school modality more recently. Including only hospitalized patients also necessarily captures a small subset of patients with mental illnesses. In addition, patients in the study population often received multiple diagnoses, including non-mental health diagnoses, associated with each individual hospitalization; as such, not all were hospitalized for reasons relating to mental illness alone. The vast majority of patients with mental illnesses are treated as outpatients, and thus were not represented in our sample. Though we chose to include only inpatients to focus on patients with the most severe illness, this excluded most children and adolescents who were affected by school closures and may have led to results that were skewed by outside factors, such as bed availability and parental hesitance to bring a child to the hospital in the midst of a pandemic. Changes in outpatient mental health care access may also have played a role in the increased share of pandemic-era patients presenting to the emergency department, potentially confounding the use of this metric as an indicator of illness severity. Finally, our study population included some patients who required mental health care during admissions for reasons other than mental illness, and thus we cannot draw conclusions regarding the population of patients admitted for mental illness alone.
The relationship between school modality, mental health symptoms, and inpatient care is nuanced and complex, and many possible confounders could not be directly addressed in this study. This study provides a broad look at a complex phenomenon and should be viewed as a starting point for future investigation. Subsequent studies should expand to include larger and/or multiple geographic regions, include patients seen in emergency and/or outpatient settings, and describe changes, if any, in the community prevalence of mental illness during periods of school closure. In addition, further study is needed to validate and explicate the changes seen in this study regarding specific mental health diagnoses as they relate to virtual school, including the specific predisposing and alleviating factors among youth at risk for tic, disruptive behavior, eating, and mood and anxiety disorders. Such studies should attempt to account for the ways in which local COVID-19 prevalence, bed availability, and socioeconomic factors influenced pediatric mental health utilization. Future interruptions of in-person schooling should also be studied in real-time to obtain prospective data on the effects of virtual schooling on students’ mental health.
Conclusion
This study demonstrates increased utilization of inpatient psychiatry and psychology services for certain mental health diagnoses, including eating, tic, and trauma and attachment disorders, among pediatric patients during the pandemic. Several markers of mental illness severity increased during the pandemic, including as-needed medication use, readmission rate, and the rate of emergent admissions. In addition, we found that mood and anxiety disorders were more prevalent, and eating disorders less prevalent, among patients attending exclusively virtual school during the 3 months prior to hospitalization. No correlation was seen between recent virtual schooling and severity of mental illness. Future study is needed to elucidate the impact of virtual school on pediatric mental health, while investigating how best to respond to the current pediatric mental health crisis.
Author Contributions
TBL: Contributed to conception and design, contributed to acquisition, analysis, and interpretation, and drafted the manuscript.
RF: Contributed to acquisition and analysis.
LR and NM: Contributed to conception and design and to interpretation.
HM and JS: Contributed to analysis and interpretation.
KK and AO: Contributed to design and to interpretation.
KM: Contributed to conception and design, and to acquisition, analysis, and interpretation.
All authors critically revised the manuscript and gave final approval.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228231209671 – Supplemental material for Virtual Schooling and Pediatric Mental Health During the COVID-19 Pandemic
Supplemental material, sj-docx-1-cpj-10.1177_00099228231209671 for Virtual Schooling and Pediatric Mental Health During the COVID-19 Pandemic by Thomas B. Leith, Reni Forer, Leah Rappaport, Nasuh Malas, Harlan McCaffery, Julie Sturza, Kristin Kullgren, Alana Otto and Kimberly Monroe in Clinical Pediatrics
Footnotes
Acknowledgements
The authors wish to acknowledge the UM-hosted Capstone for Impact Grant and NIH T35 Short Term Biomedical Training Program for providing financial support for this project, Benjamin Margolis MD for his oversight of the latter program, and Bethany Freeland for assisting with data extraction.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIH T35 Short-term Biomedical Training Program and the Capstone for Impact Grant, both hosted by the University of Michigan Medical School. The sponsor did not participate in the work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.