
Abstract
A retrospective, cross-sectional study of children with bronchiolitis aged 1 to 24 months during an ED visit between 2019 and 2021 was performed. Chi-square or Kruskal-Wallis was used to compare groups. The gamma coefficient was used to measure the association of variables through time. Bronchiolitis cases decreased by 75% from 2019 to 2020 and rose back to prepandemic levels by 2021. Radiographs (gamma −0.443), steroids (gamma −0.298), and bronchodilators (gamma −0.414) decreased during the study period (P < .001). Laboratory studies (gamma 0.032), viral testing (gamma 0.097), antibiotic use (gamma −0.069), and respiratory support (gamma 0.166) were unchanged. The decrease in steroids and bronchodilators was related to a clinical pathway that discouraged their use. Respiratory support remained unchanged. The COVID-19 pandemic (2019-2021) seems to have had little effect on the severity or resource utilization associated with bronchiolitis but may have unraveled a potential bronchiolitis phenotype that may have been more prominent during the pandemic.
Introduction
The SARS-CoV-2 virus (Coronavirus disease 2019 [COVID-19]) has presented challenges to the health care system and the delivery of medical care during the pandemic. Overall, emergency department (ED) visit rates decreased by half during the early stages of the COVID-19 pandemic. 1 The largest decrease occurred among visits for respiratory disorders in the pediatric population, 2 due in part to increased safety measures that were implemented during the pandemic that influenced the transmission of respiratory viruses.2,3 As a result of the COVID-19 pandemic’s influence, there have been drastic changes in the epidemiology of other viral respiratory infections. 4 Respiratory conditions such as bronchiolitis usually follow a strong seasonal variation, with higher volumes beginning in October and extending through March.5,6 However, during the pandemic, there was an average drop of 84% in acute bronchiolitis cases managed in the ED compared with the previous five years. 7
The epidemiology and patient characteristics of bronchiolitis have been described at great length, with bronchiolitis being the leading cause of ED visits and hospitalizations for infants.6,8,9 The extent of resource utilization by diagnostic measures and management of bronchiolitis has also been widely discussed.8,10 However, little is known about how bronchiolitis cases have changed throughout the COVID-19 pandemic and how resource utilization in the ED has affected their diagnosis, management, and patient outcomes. Therefore, the objectives of this study are to (1) describe and compare the clinical characteristics, management, and resource utilization of children with bronchiolitis who visited the ED during the COVID-19 pandemic, and (2) evaluate the temporal distribution of bronchiolitis characteristics during the study period.
Methods
Study Design and Data Source
This is a retrospective, cross-sectional study performed through an electronic medical record (EMR) review of pediatric visits to the ED of a university-affiliated, freestanding pediatric hospital. This study was approved by the Institutional Review Board (IRB).
Identification of Sample
We included children aged 1 to 24 months of age who were evaluated and diagnosed with bronchiolitis from January 1, 2019, to December 31, 2021. Diagnoses included International Classification of Diseases, 10th Edition (ICD-10) codes for the following: acute bronchiolitis unspecified (J21.9), acute bronchiolitis (J21), acute viral bronchiolitis (J21.8), respiratory syncytial virus (RSV) bronchiolitis (J21.0), acute bronchiolitis due to respiratory syncytial virus (J21.0), acute bronchiolitis with bronchospasm (J21), bronchiolitis due to human metapneumovirus (J21.1), history of bronchiolitis (Z87.9), adenoviral bronchiolitis (B97.0), and bronchiolitis caused by influenza virus (J11.1).
Study Variables
Data included patient characteristics (age, date of birth, sex, race/ethnicity, comorbidities, family history), ED visit characteristics (emergency severity index [ESI], 2 chief complaints, history of present illness, symptoms and duration, physical exam), diagnostic workup (radiologic studies, laboratory studies, viral testing by nasopharyngeal polymerase chain reaction), treatment (medication, respiratory support), ED length of stay (minutes), disposition (admission, discharge home), return to the ED in 48 hours, and final diagnosis.
Outcome Measures
The primary outcome measures were (1) the distribution of patient characteristics, management, and resource utilization of bronchiolitis per calendar year, and (2) temporal trend distribution of bronchiolitis characteristics during the COVID-19 pandemic. Secondary outcomes of interest included viral etiology, final diagnosis, and disposition.
Statistical Analysis
Data exploration was performed for continuous variables with standard metrics (means and standard deviations, ranges, medians, and quartiles as well as normality testing) and nominal variables with frequency analysis (highest frequency to lowest frequency for each variable). Chi-square was used to evaluate the differences between the distributions per calendar year. Temporal trend distribution per calendar year was evaluated using the gamma coefficient test. The gamma coefficient test was used to measure the strength and direction of the association between variables across the years. A gamma of 1.0 was used to reflect a positive perfect relationship across the years, while a gamma of −1.0 was used to reflect a negative perfect relationship between the variables across the years. A gamma of 0.00 reflected no association. All statistical analyses were conducted in IBM SPSS Statistics 28 (IBM Corp., Armonk, NY, USA) with P-values less than .05 considered statistically significant.
Results
We identified 1057 EMRs that met inclusion criteria and comprised 932 unique patients, of which 64% were male, 61% were of Hispanic or Latino origin, and 68% had public health insurance. The median patient age was 7 months (IQR 4-13 months). Bronchiolitis cases decreased by 75% from 2019 (471) to 2020 (122) and increased to prepandemic levels by 2021 (464). Emergency severity index levels 2 and 3 decreased, while ESI levels 4 and 5 increased during the study period (gamma −0.254, P < .001). Eighty-five percent of patients had no comorbidities during the study period (gamma 0.131, P < .05). Medical history was remarkable for previous episodes of bronchiolitis (13.2%), followed by reactive airway disease (6.1%). Medical history for allergies (ie, seasonal, food, milk protein) (gamma −0.810, P < .001) and previous bronchiolitis episodes showed a decreasing trend (gamma −0.656, P < .001). Family history of atopy (including asthma, hay fever, and atopic dermatitis) showed a decreasing trend during the study period (gamma −0.678, P < .001). An age-stratified analysis by age group (0 to 3 months, 4 to 12 months, and 13 to 24 months) was performed (Table 1). The 0- to 3-month and 4- to 12-month age groups decreased from 2019 to 2021, while the 13- to 24-month age group increased (gamma 0.194, P < .001). We found no significance in the history of present illness for fever, sore throat, cough, shortness of breath, vomiting, or decrease in urine output during the study period. The use of medications reported during the illness showed an increase in bronchodilators (gamma 0.281, P < .001) and a decrease in antipyretics (gamma −0.329, P < .001) and intranasal normal saline and suction (gamma −0.362, P < .001). However, from 2019 to 2021, we noted a decreasing trend of prior use of bronchodilators (gamma −0.294, P < .001) and steroids (gamma −0.346, P = .004). Physical examination was remarkable for an increase in the presence of retractions (gamma 0.131, P = .020), a decrease in the presence of prolonged expiratory phase (gamma −0.879, P < .001), and a decrease in nasal congestion (gamma −0.445, P < .001).
Distribution of Clinical Characteristics of Children With Bronchiolitis Who Visited the Emergency Department, 2019-2021 (N = 1057).
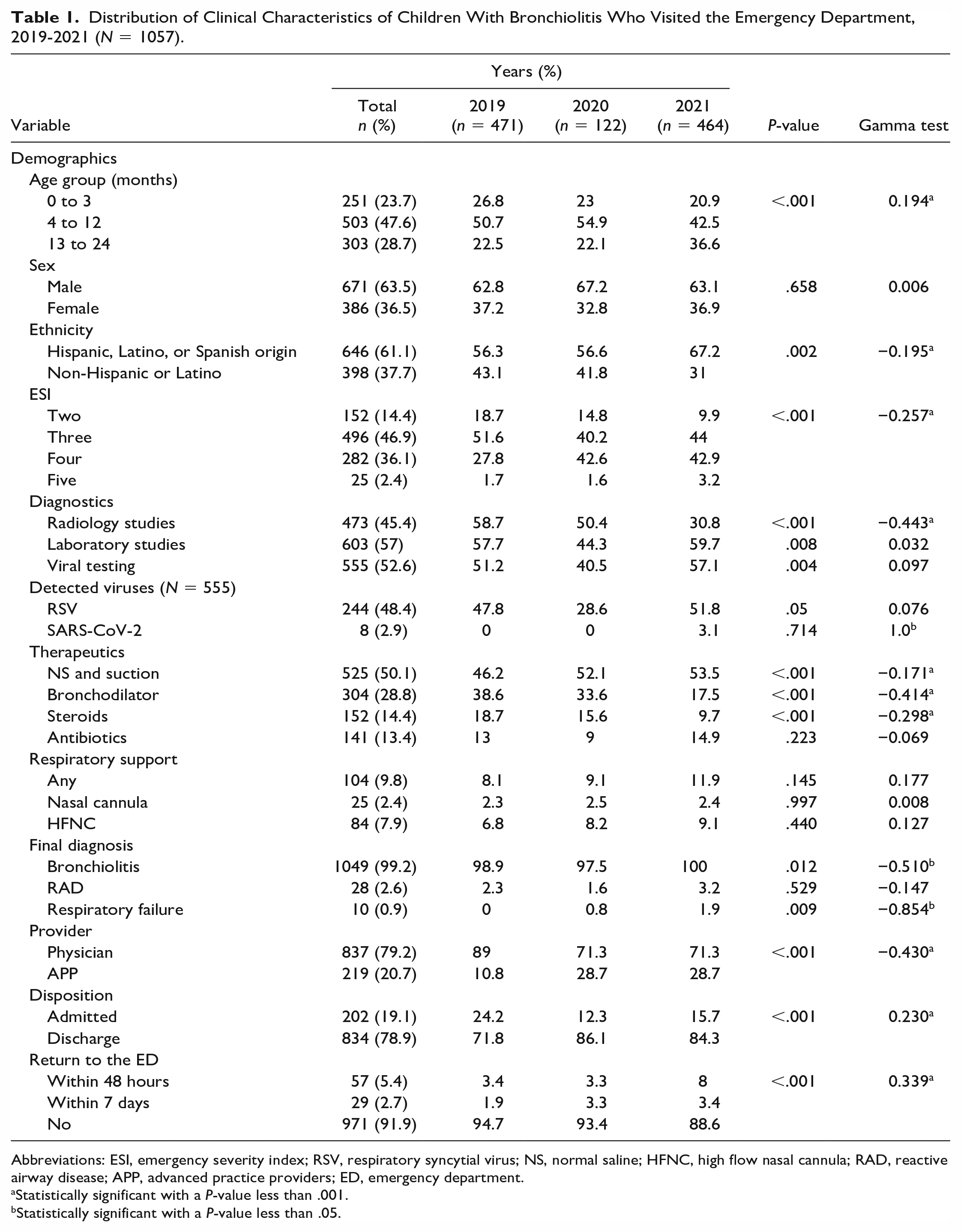
Abbreviations: ESI, emergency severity index; RSV, respiratory syncytial virus; NS, normal saline; HFNC, high flow nasal cannula; RAD, reactive airway disease; APP, advanced practice providers; ED, emergency department.
Statistically significant with a P-value less than .001.
Statistically significant with a P-value less than .05.
The only diagnostic resource associated with a decreasing trend during the study period was the use of radiographs (gamma −0.443, P < .001). Therapeutic resources exemplified by intranasal normal saline and suction (gamma −0.171), bronchodilators (gamma −0.414), and steroids (gamma −0.298) decreased during the study period (P < .001). There was an increase in laboratory studies (gamma 0.032) and viral testing (gamma 0.097), albeit not significantly (P > .05). Viral testing was performed in 52% of patients, with 61% of cases tested having at least 1 virus detected. The most frequent organism detected was respiratory syncytial virus (244, gamma −0.076, P = .351), followed by human rhinovirus/enterovirus (70, gamma −0.188, P = .205) and human metapneumovirus (16, gamma −0.029, P = .917). Only eight patients had bronchiolitis due to COVID-19. Subgroup analyses showed that the 13- to 24-month age group was associated with a higher frequency of radiologic studies (adj resid = 4, Bonferroni adjusted P < .001), RSV diagnosis (adj resid = 2.5, Bonferroni adj P = .07), intranasal normal saline and suction (adj resid = 5.5, Bonferroni adj P < .001) and bronchodilator use (adj resid = 4.8, Bonferroni adj P < .001). There is a significance (gamma 0.233, P < .001) associated with age and negative RSV test result. Antibiotic administration in the ED was similar for the 4- to 12-month and 13- to 24-month age groups but significantly lower for the 0- to 3-month age group (adj resid −4.4, Bonferroni adj P < .001). The age group was not significantly related to ESI, use of laboratory studies, viral testing, COVID-19 diagnosis, nasal cannula use, or return to the ED.
The median length of stay in the ED was 168 minutes (IQR 120-236). We found no significance in the prescription of bronchodilators, steroids, antibiotics, or intranasal normal saline and suction during the study period. Eighty percent of patients were discharged home (gamma 0.230, P < .001). There was a significant increase in the rates of return to the ED within 7 days (gamma 0.339, P < .001) from 2019 to 2021. Overall, the readmission rate more than doubled between 2019 (5.3%) and 2021 (11.4%).
Discussion
The COVID-19 pandemic drastically changed the epidemiology of respiratory viruses that cause bronchiolitis, 7 and, in doing so, it changed the utilization of pediatric ED resources. 2 Children with bronchiolitis in the 4- to 12-month age group during the study period continued to be the most frequently seen in the ED.2,8 There was an inversion between the 0- to 3-month and 13- to 24-month age groups, making the latter age group the second most frequent in 2021, unlike prior years. This could be due to the higher rate of respiratory infections in the older age group upon the decrease in social distancing, return to school, and lifting of mask-wearing mandates in 2021. 2 Patient demographics such as sex and ethnicity remained steady during the study period, reflecting the pathophysiology of the disease2,6,8 and the demographic population of the community. 2 The prevalence of comorbidities among our patient population was similar to the ones described in the literature, 11 showing a significant decreasing trend during the pandemic. 12 This is associated with retained social distancing in this high-risk population. 2 Disease severity exemplified by the ESI based on acuity and resource needs 13 showed that there was a decrease in higher acuity (ESI 2/3) with a corresponding increase in lower acuity (ESI 4/5). This may be due to decreased access to primary care during the pandemic2,14 or fear surrounding COVID-19 symptoms in children.15,16 This is further exemplified by the increase in return rate to the ED at 48 hours, which was not related to an increase in disease severity or admission after return to the ED. Another reason may be the increasing need to rule out COVID-19 in these patients with respiratory viruses and the increased caution surrounding respiratory illnesses in the pediatric population, but this has yet to be studied. Our study demonstrated that 1% of patients were diagnosed with respiratory failure, with a statistically significant difference in the distribution across the years but with a decreasing trend. The negative gamma in this case was likely driven by the non-mutually exclusive nature of the final diagnoses, as it was not supported by an increase in respiratory support.
The temporal distribution analysis on the use of resources in children with bronchiolitis showed a significant decrease in radiology studies, intranasal normal saline and suction, bronchodilator, and steroid use. These significant trends may have been driven by the implementation of an updated ED clinical pathway on the diagnosis and management of bronchiolitis that aligned with the national recommendations made by the American Academy of Pediatrics on the diagnosis and management of bronchiolitis which discouraged their use. 8 The use of respiratory support increased during the pandemic, albeit not significantly, which further promotes the inference that there was no increase in disease severity. In contrast, Bermúdez Barrezueta et al 11 assessed the effect of the COVID-19 pandemic in Spain and reported a significant decrease in low-flow and high-flow oxygen therapy, with an increase in noninvasive ventilation during the pandemic. However, at baseline, their prevalence of respiratory support was twice as high as the one in our institution. This could be related to the higher severity of disease and increase in intensive care admissions associated with their younger patient population. This may also be explained by our older patient population who did not require an increase in respiratory support, as they used more resources, including bronchodilators. Furthermore, although we noted a decrease in the prior use of bronchodilators and steroids, we saw an increase in bronchodilator administration during the illness. This could be due to the presentation of a bronchiolitis phenotype that seemed to be responsive to bronchodilator therapy during the pandemic. A recent systematic review proposed that the following clinical characteristics support a patient profile that may benefit from bronchodilator therapy, at least on a therapeutic trial basis. 17 These include (1) older age (> 6-12 months),18-22 (2) wheezing,23,24 (3) atopic dermatitis/eczema,25,26 and (4) history of asthma in a first-degree family.23,25 Our patient population showed a significant increase in two of the four criteria during the COVID-19 pandemic, which may be a reflection of the ED use, the patient population in general, or epidemiological changes associated with a specific bronchiolitis phenotype, which merits further investigation. The increase in advanced practice providers (APPs) in the later part of the study period was related to patient volume and a decrease in ESI. 2
Before 2021, COVID-19 was seldom found in children with bronchiolitis. 27 Our study identified eight children with COVID-19 bronchiolitis in 2021, of which one had co-infection with RSV. These findings refute Berdah et al 12 who assessed the effect of the COVID-19 pandemic in France and suggested that SARS-CoV-2 alone does not cause bronchiolitis. Our findings are likely due to the advent of the COVID-19 Delta variant in March 2021 in the state of Florida, rather than the COVID-19 Alpha variant that was predominant at the time. 28 A recent study showed that children were 2.5 times more likely to become infected with Delta,29,30 which coincides with the instances of COVID-19 bronchiolitis in 2021 compared with the initial Alpha variant. Furthermore, our study showed half of the children with bronchiolitis underwent viral testing, of which the most common organism was RSV followed by human rhinovirus/enterovirus. 11 Overall, we saw a significant decrease in trends for most respiratory viruses except RSV, which decreased from 2019 to 2020 but went back to its epidemiologic baseline in 2021. Public health measures imposed to prevent the spread of the COVID-19 pandemic (eg, social distancing, masking mandate, and nonpharmaceutical interventions) were effective at mitigating the diffusion of all respiratory infections. 31 However, much has changed since the advent of COVID-19, and it has significantly affected the epidemiology of respiratory illnesses. Ultimately, studies have been able to report on the epidemiological changes of bronchiolitis associated with their severity, resource use, and hospitalization during the COVID-19 pandemic. However, this is the first study to our knowledge that aims to describe patient characteristics associated with bronchiolitis during the COVID-19 pandemic and sheds light on potential bronchiolitis phenotypes that may have become more prominent during the pandemic. Whether the changes are due to natural competition between respiratory viruses, the introduction of vaccines, safety measures such as quarantine or masking, herd immunity, provider practice, or inherent patient characteristics and epidemiological responses remains to be seen.
Limitations
This study sought to describe and compare the clinical characteristics of children with bronchiolitis during their visit to a single pediatric ED during the COVID-19 pandemic, which may affect the generalizability of the study. Because of this study’s retrospective nature, we cannot determine causality and can only make observations and inferences. We performed EMR extraction, which is limited by the extent of documentation by the medical provider. Final diagnoses might have been used inconsistently across providers, which could result in misclassification. Because this analysis is limited to the pediatric ED, we lack information on children who may be seen elsewhere. Availability of viral analysis may have been provider-dependent or resource-dependent, as during the pandemic, viral testing was limited for cohorting purposes and the presence of comorbidities or was dependent on the type of testing kit. The implementation of a clinical pathway in the ED that discouraged the use of radiologic studies, laboratories, viral testing, bronchodilator use, and steroids may have helped curb the use of resources in the ED and may not have been directly related to natural provider behavior or disease process.
Conclusions
Safety measures implemented during the COVID-19 pandemic helped curb the transmission of respiratory viruses that cause bronchiolitis. The decreased use of diagnostic and therapeutic resources was related to the implementation of a clinical pathway that discouraged their use. The use of respiratory support increased throughout the study period but did not reach significance. The COVID-19 pandemic (2019-2021) seems to have had little effect on the severity or resource utilization associated with bronchiolitis but may have unraveled a potential bronchiolitis phenotype that may have been more prominent during the pandemic.
Author Contributions
AJ designed the study, designed the data collection instrument, coordinated and performed data collection, drafted the initial manuscript, and reviewed the manuscript. Dr. Maul performed comprehensive data analysis, drafted the initial manuscript, and reviewed and revised the manuscript. PH, MS, and SG coordinated and performed data collection and assisted in drafting the initial manuscript. Drs. Sarandria, Glass, Blake and Alexander designed the study, and critically reviewed and revised the manuscript for important intellectual content. Dr. Rivera-Sepulveda conceptualized and designed the study, designed the data collection instrument, performed data analysis, drafted the initial manuscript, and critically reviewed and revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the (AHRQ-PCORI-funded) PEDSnet Scholars Training Program (5K12HS026393-03), which is a national faculty development program that trains individuals in the competencies of learning health systems science.
Ethical Approval
This study was approved by the Institutional Review Board (IRB).