
Abstract
Children with medical complexity (CMC) receive care from many clinicians. Our objective is to describe caregivers’ experiences about telehealth for CMC. This qualitative study conducted in North Carolina involves semistructured interviews with 23 caregivers of CMC (15 English; 8 Spanish). Data were analyzed using thematic content analysis. Five themes were identified: (1) telehealth allayed caregivers’ fears about their children’s exposure to COVID-19 and mitigated the challenges with in-person visits during the pandemic. (2) Telehealth reduced the logistical challenges of in-person visits for CMC, enabled providers to see children in their home environment, and prevented appointment cancelations. (3) System inaccessibility, technical problems, and providers’ inability to deliver telehealth were challenges. (4) Inadequate evaluation of the child and caregiver-provider communication were limitations. (5) Caregivers were satisfied with telehealth, found variability in telehealth offering, and wished telehealth continued to remain an option. Telehealth is a viable option for outpatient care delivery for CMC.
Introduction
Children with medical complexity (CMC) account for about 0.5% of all children in the United States and have health conditions that involve multiple organ systems.1,2 Children with medical complexity need long-term services from multiple providers. 1 Access to health care services is important for the well-being of CMC; however, these needs are often unmet.3,4 Access to primary and specialty care is particularly problematic for CMC of minority race/ethnicity, and those living in rural areas.5,6
Telehealth has long been considered a potential solution to address barriers in access to care for children.7,8 An integrative review reported the benefits of telehealth in clinical outcomes and family satisfaction. 9 Telehealth improved clinical outcomes of CMC including reduction in hospitalizations, serious illnesses, and adverse outcomes. 10 Telehealth contributed to reductions in travel time, cost, and appointment delays for children 11 and enhanced child engagement in care. 12 Telehealth helped reduce unplanned health visits and increased planned clinic visits for CMC. 13 Although models of telehealth exist, telehealth services have not been widely available until the COVID-19 pandemic. Also, parents’/caregivers’ (henceforth referred to as caregivers) perspectives on telehealth experiences for CMC have not been evaluated.
In response to the COVID-19 pandemic, for the first time in the United States, telehealth has become available as an option for outpatient pediatric care.14,15 This provides an unprecedented opportunity to examine the usefulness of telehealth in the health care delivery of CMC. At present, health insurance programs are evaluating whether telehealth flexibilities need to be continued. 16 Understanding caregivers’ perspectives is important when making policy decisions about telehealth in the health care delivery for children. The objectives of our study are to understand the benefits and challenges of telehealth from the perspectives of caregivers of CMC.
Methods
This study was conducted at Brenner Children’s Hospital (BCH), the tertiary care children’s hospital within the Atrium Health Wake Forest Baptist system in northwestern North Carolina. This qualitative study involved interviews of parents/caregivers of CMC about their experiences with telehealth for their children during the COVID-19 pandemic. We used the Consolidated Reporting of Qualitative Studies (COREQ) Checklist 17 (Appendix A) as a guide in reporting the study. The Institutional Review Board (IRB) of Wake Forest University School of Medicine approved the study.
Participants
Children with medical complexity were identified from a referral database maintained by the institution’s pediatric palliative/complex care program (called the Pediatric Enhanced Care Program [PECP]). Children are eligible for the program if they have a long-term condition that lasted or is expected to last ≥12 months, need care from ≥5 specialists/services, or use ≥2 types of medical technology (eg, gastrostomy tube, tracheostomy, etc). Using electronic health record (EHR) data, we identified a list of children who met the following criteria: age < 18 years as of March 10, 2019, referred to PECP before March 10, 2020, and had at least one pediatric neurology subspecialty visit between March 10, 2019 and March 9, 2020. We chose attendance at neurology outpatient visit as an inclusion criterion because we had detailed information about telehealth use for these children from the EHR as part of another study from this project. Of the 319 children on the preliminary list, we excluded 28 children who turned 18 years old before the recruitment and 12 children who died in order to not to interfere with caregivers’ grief process. Of the remaining 279 children, the primary languages of caregivers were English (n = 239) and Spanish (n = 40).
English-speaking caregivers of eligible children were recruited by one of the authors (HD), and Spanish-speaking caregivers were recruited by the care coordinator of PECP. Caregivers had to be aged ≥18 years at the time of the interview and the primary caregiver of the child. With EHR data, we used purposive sampling to recruit at least 8 children in each of 6 subgroups of interest: (1) Spanish as primary language, (2) black race, (3) rural residence, (4) age >10 years, (5) not used telehealth at BCH between March 10, 2020 and March 9, 2021 (“pandemic period”), and (6) had ≥10 clinic appointments/year.
Eleven caregivers declined participation. Seven agreed to participate, but either did not return consent or schedule interviews. We recruited 8 caregivers in each subgroup of interest, except race. We were able to recruit only 6 caregivers of black children and could not continue recruitment further because of time and resource limitations.
Qualitative Data
Twenty-three interviews (15 English and 8 Spanish) were conducted from February to March 2022 via Webex (a video conferencing platform), telephone, or in-person encounters according to participants’ preferences. All English interviews, except one, were conducted via Webex. One English interview was attempted through Webex but could not be conducted due to technical difficulty on the part of the participant and was changed to a telephone interview. Of the Spanish interviews, 5 were conducted by Webex, 2 in-person, and 1 via telephone. Based on a conceptual model (Figure 1), an interview guide was developed in English (Appendix B) and translated into Spanish. The interview guide was revised once as interview progressed. English interviews were conducted by one of the authors (SG), and Spanish interviews were conducted by the care coordinator of PECP. Informed consent was obtained from participants, either in-person, by mail, or electronically. Each participant was given a $30 gift card as an incentive.
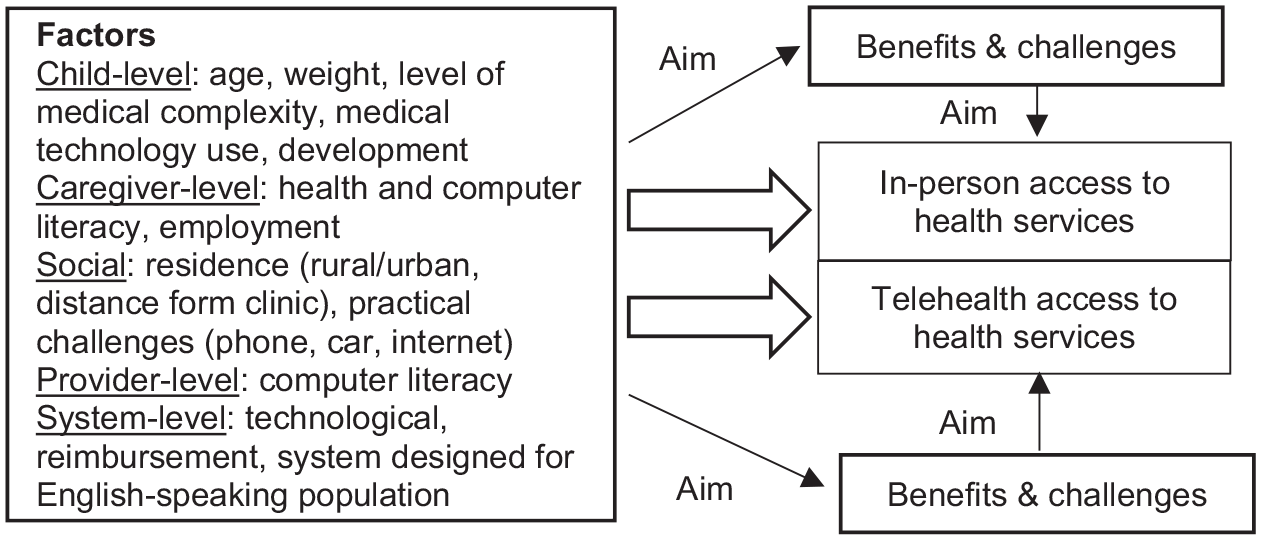
Conceptual framework of telehealth and in-person access to outpatient specialty care for children with medical complexity.
Interviews were audio-recorded and transcribed by professional transcriptionists. Spanish transcripts were translated into English by a professional translator. Transcripts were reviewed by the interviewers for accuracy and uploaded into ATLAS.ti version 7.5. 18 One of the authors (SN) listened to all English interviews and reviewed all Spanish transcripts. Based on initial reviews and the conceptual framework, a codebook was developed. Two authors (SN and SG) coded the first 2 transcripts separately, and compared code applications, resolving differences and revising the codebook. For the remaining transcripts, one author coded the transcript, and a second author reviewed the coded segments and reconciled any differences in coding with the primary author. The codebook was revised thrice as coding progressed. The final version of the codebook was applied to all transcripts.
One author summarized text within each code or group of codes. A second author reviewed the summaries of the coded text and reconciled any differences with the summarizing author. After all summaries and reviews were complete, themes were identified by their prevalence and salience in the data. The principles of thematic analysis were applied. 19 No new themes were identified after the 12th interview.
Quantitative Data
Child-level data (age, race, ethnicity, health insurance status and address) and encounter-level data (number of clinic and telehealth appointments) were obtained from the EHR through Wake Forest Center for Biomedical Informatics (WFBMI). We used children’s addresses and data from the American Community Survey 20 to calculate the rurality score (range: 0-1). A rurality score of >0.5 was defined as urban, and a score of ≤0.5 as rural. Distance to BCH was calculated using coordinates for BCH and the child’s address, using a function developed by WFBMI. Children’s medical conditions were obtained from chart reviews.
A brief survey was administered to caregivers prior to the interview that included caregiver-level information and household income. The survey also elicited information about the number of appointments (in-person, video, or audio) the child had in the 6 months prior to the interview; and preferences for appointment type, access to and preference for devices for telehealth (smartphone vs. computer), and comfort level for using different devices and the EHR patient portal. Comfort level was measured on a scale of 1 to 5, with 1 being “not at all comfortable” and 5 being “extremely comfortable.” The 21-item Telehealth Usability Questionnaire (TUQ), 21 a reliable and valid measure of users’ assessment of telehealth was adapted for pediatrics and our institution’s patient portal and administered. Responses for each item on TUQ are on a scale of 1 to 7, with higher scores indicating greater usability of or satisfaction with telehealth.
Quantitative data were analyzed in Microsoft Excel. The median and range for continuous variables, and number and proportion for categorical variables were calculated.
Results
Quantitative Results
Characteristics of children and caregivers are presented in Table 1. The median age of children was 11 years; 61% were non-white; 35% were Hispanic; and 43% had rural residences. The median distance to BCH was 22 miles. The median number of clinic appointments in the pre-pandemic (March 10, 2019 to March 9, 2020) and pandemic (March 10, 2020 to March 9, 2021) years were 8 and 7 respectively, and telehealth appointments/year (March 10, 2020 to March 9, 2021) were 2.
Participant Characteristics.
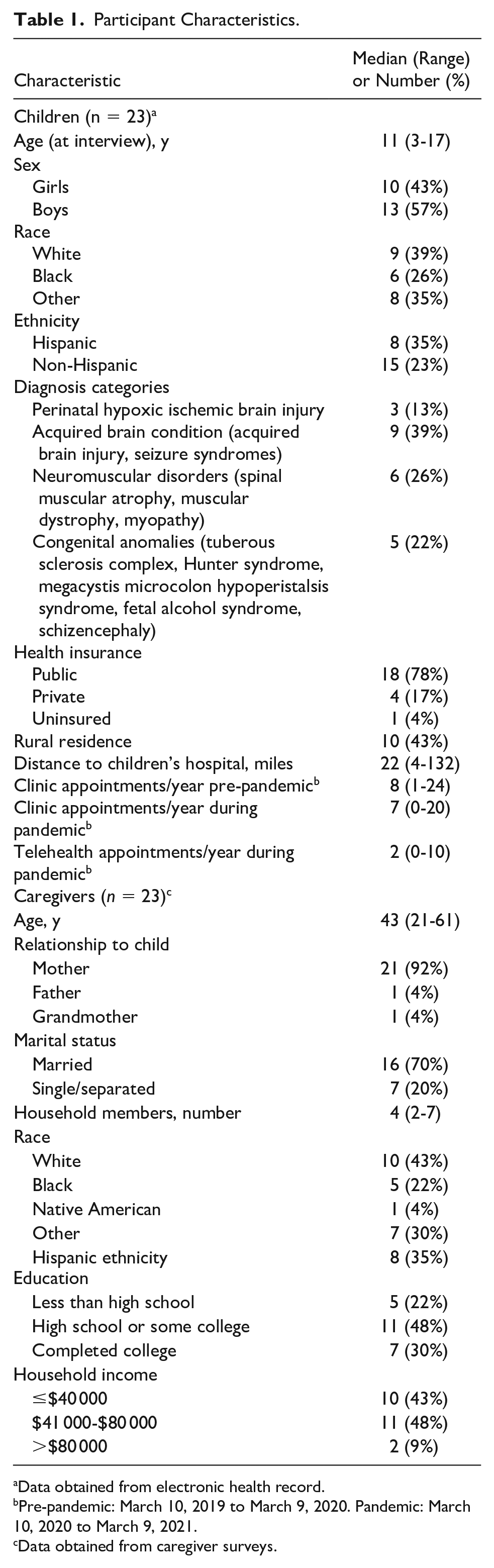
Data obtained from electronic health record.
Pre-pandemic: March 10, 2019 to March 9, 2020. Pandemic: March 10, 2020 to March 9, 2021.
Data obtained from caregiver surveys.
Caregivers’ experiences with telehealth are in Table 2. Almost all (96%) caregivers had access to a smartphone. All 6 caregivers who did not have a computer were Spanish-speaking. A majority (57%) preferred smartphones for telehealth. Caregivers’ comfort levels for using computers, smartphones, or the EHR portal was high. The median overall score for TUQ was 6.3. Of the subscales, the score for reliability was the lowest (5.6).
Telehealth Experiences of Children With Medical Complexity Based on Caregiver Surveys.
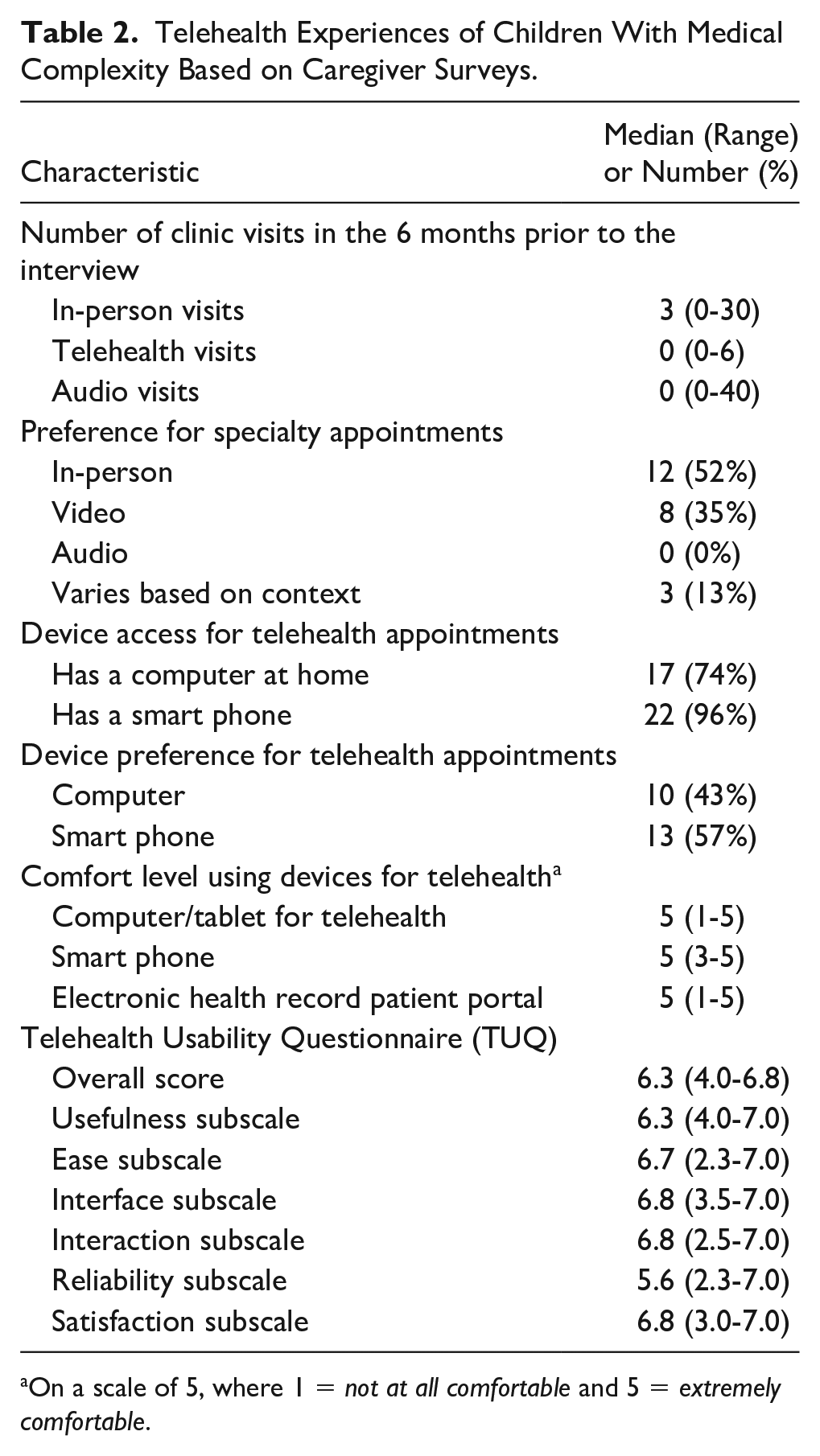
On a scale of 5, where 1 = not at all comfortable and 5 = extremely comfortable.
Qualitative Results
The median duration of the interviews, excluding the administration of the surveys, was 36 (range: 16-49) minutes. Qualitative themes are presented below and illustrative quotes in Tables 3 to 5.
Benefits of Telehealth for Children With Medical Complexity: Themes With Illustrative Caregiver Quotes a .
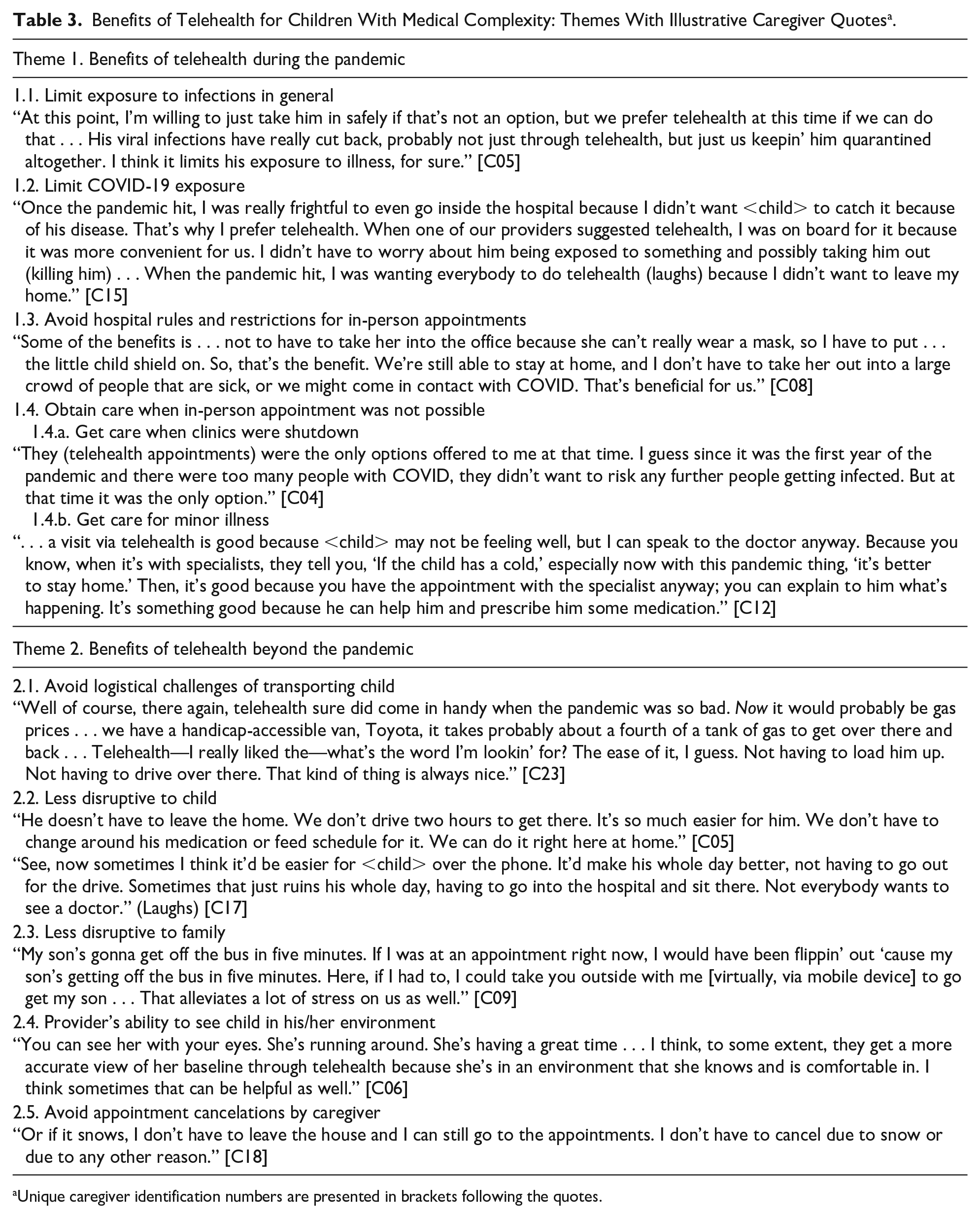
Unique caregiver identification numbers are presented in brackets following the quotes.
Challenges With or Limitations of Telehealth for Children With Medical Complexity: Themes With Illustrative Caregiver Quotes a .
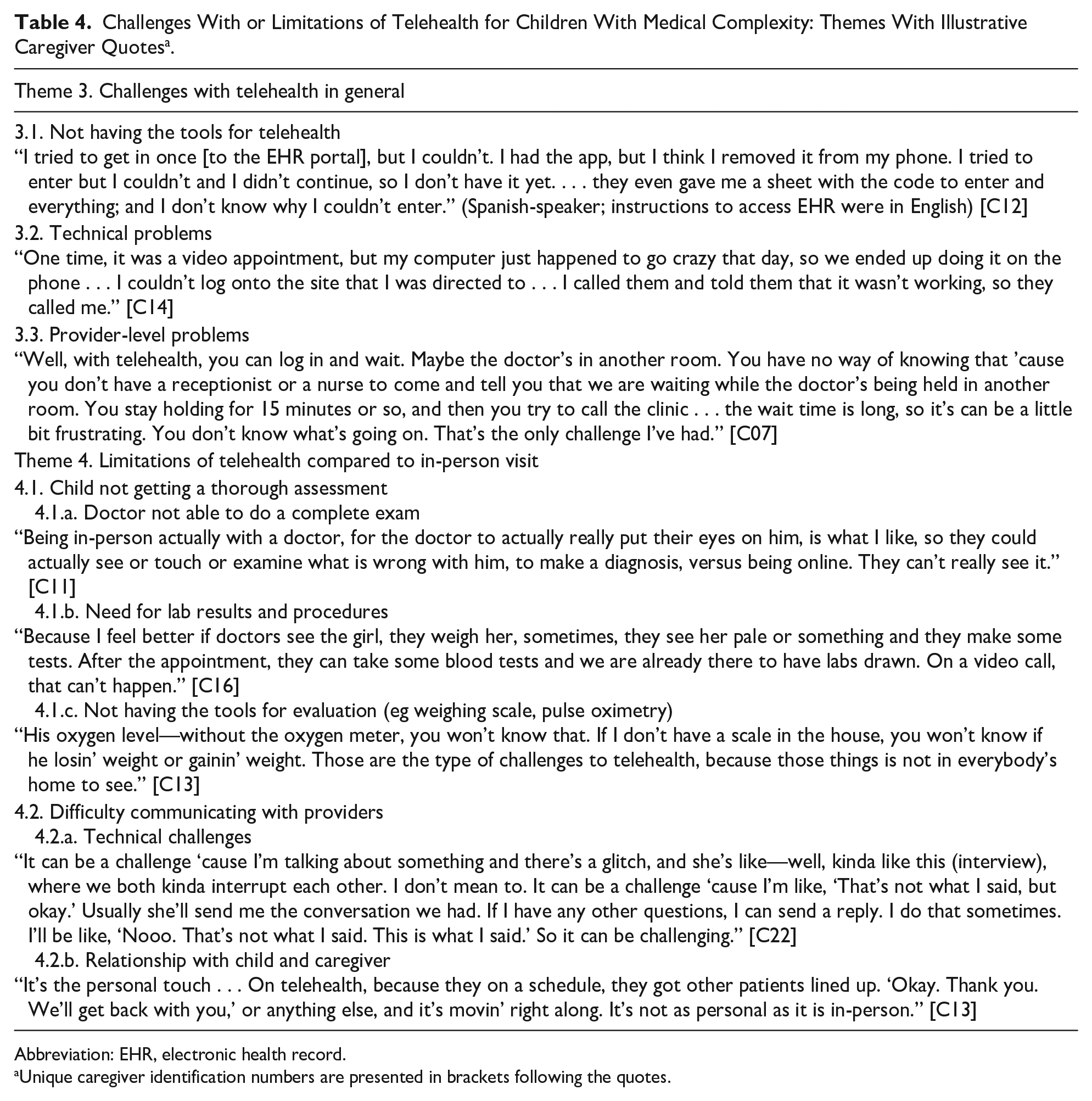
Abbreviation: EHR, electronic health record.
Unique caregiver identification numbers are presented in brackets following the quotes.
Caregiver Satisfaction With Telehealth for Children With Medical Complexity: Themes With Illustrative Caregiver Quotesa.
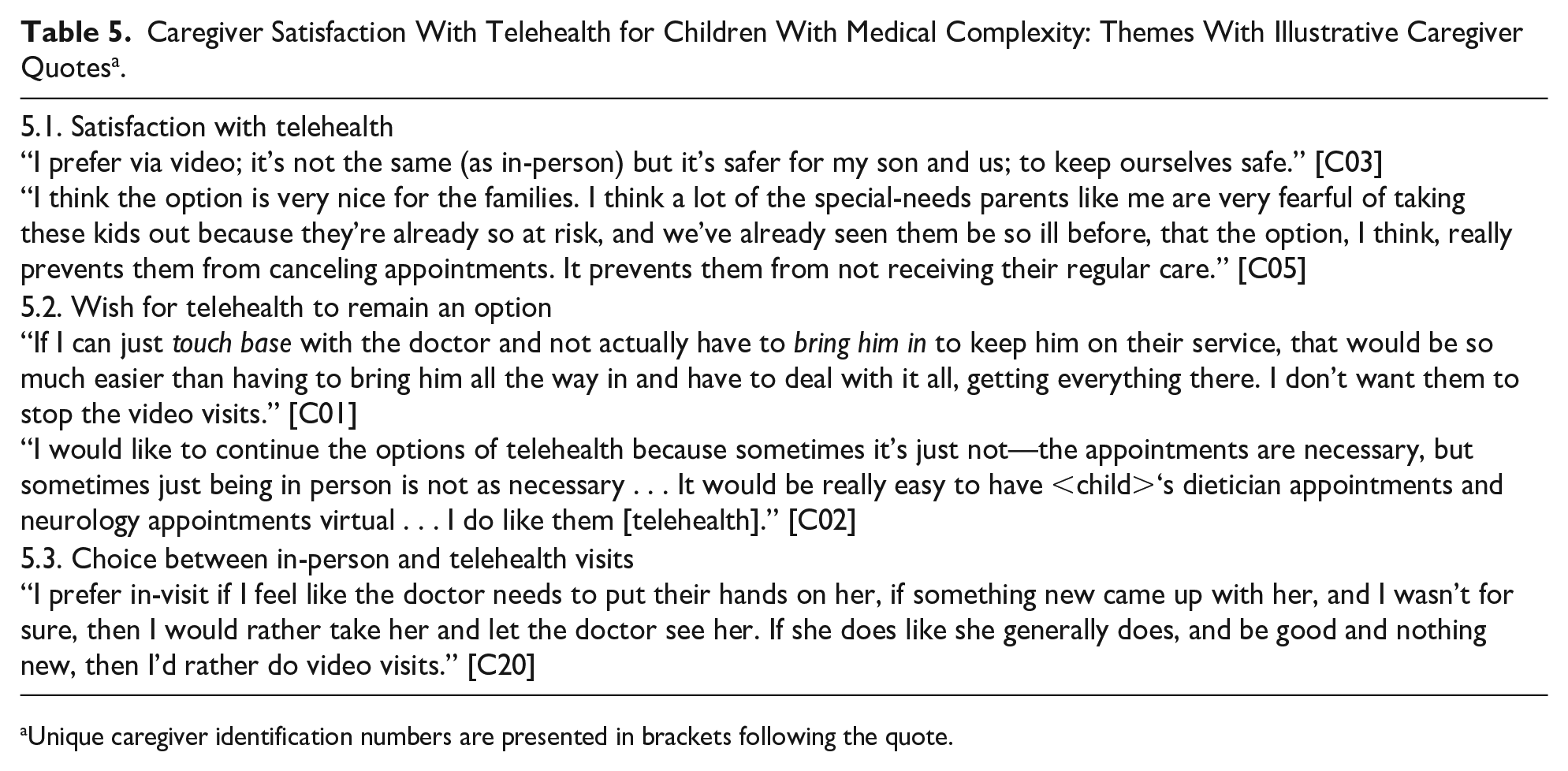
Unique caregiver identification numbers are presented in brackets following the quote.
Theme 1: Telehealth allayed caregiver fears about exposing their vulnerable children to COVID-19 and mitigated the challenges with in-person visits during the pandemic
Owing to their children’s medical fragility, even without a pandemic, caregivers wished to minimize their children’s exposure to germs. Telehealth appointments helped avoid exposing their children—and themselves—to a myriad of illnesses. Almost all caregivers said they were fearful of exposing their children to COVID-19. Caregivers considered their children to have poor immunity because of their underlying medical conditions and fragility. Hence, they were fearful of a serious illness if their children were to contract COVID-19. Some recalled prior experiences where children became seriously ill after a minor infection. As a result, caregivers avoided taking their children out of their homes during the pandemic. Caregivers especially tried to avoid taking their children to the hospital. For these reasons, they canceled their children’s in-person appointments, or changed them to telehealth appointments. Limiting children’s exposure during the pandemic was the singular most important benefit of telehealth. Only 2 caregivers (both Spanish-speaking) said they were not concerned about COVID-19 and preferred to take their children to in-person appointments. Another caregiver said that going to in-person appointments was an important exception to keeping her child at home during the pandemic.
Telehealth mitigated challenges children faced related to hospital policies and requirements for in-person visits during the pandemic. These included hospitals’ COVID-19 safety protocols, such as mask requirements and social distancing. Several caregivers reported difficulties with their children using masks—they could not keep the masks on, or masks caused anxiety and breathing difficulty. Hospital rules restricted the number of people accompanying each child during the pandemic for in-person appointments. This was problematic for CMC who needed additional people to provide medical care during clinic appointments. Telehealth helped circumvent these problems.
During the pandemic, hospitals shut down clinics and canceled appointments. Some caregivers said that early in the pandemic, providers offered telehealth as the only option for clinic appointments. Telehealth provided an opportunity for children to receive necessary care that otherwise would not have been possible. In addition, when children had respiratory illnesses, clinics’ pandemic rules restricted the caregivers from taking children to in-person appointments. Telehealth enabled CMC to get care for minor illnesses that would not have been possible otherwise.
Theme 2: The benefits of telehealth extended beyond caregivers’ fear of exposure to infection and pandemic challenges
For the most part, telehealth appointments were convenient, easy, and straightforward. Telehealth reduced the logistical challenges of in-person appointments such as disruption to the child’s routine or medical care and the difficulty of transporting a medically fragile child. Thus, telehealth was less taxing and anxiety provoking to the child. Telehealth appointments were easier to schedule around caregivers’ work and activities of the family. This allowed for greater flexibility in scheduling clinic appointments. In addition, telehealth saved caregiver time, effort, and money on travel and avoided missed work. For these reasons, telehealth was less tiring or stressful for the caregiver than in-person visits. In general, telehealth minimally disrupted everyday life for the entire household and greatly reduced caregiver burden associated with clinic appointments.
Telehealth allowed clinicians to see children in their home environments and provided a glimpse of the child’s daily life. Four mentioned that telehealth availability enabled timely assessment and treatment of their children’s symptoms. Many caregivers said that telehealth helped them keep appointments during the pandemic, rather than cancel due to minor illness or other complexities. They voiced that availability of telehealth beyond the pandemic would help avoid appointment cancelations and enable children to get the care that they need.
Theme 3: Telehealth presented technological and logistical challenges to caregivers and providers
Many caregivers reported challenges with telehealth. Two caregivers (both Spanish-speaking) said that they did not have access to the institution’s EHR patient portal and, as a result, did not use telehealth at all. A few found it difficult to keep telehealth appointments organized, including 2 mentioning that it was harder to remember telehealth more so than in-person appointments.
Several experienced technical problems prevented, delayed, or complicated telehealth appointments. For some, background noise was distracting. Most technical problems were related to internet connectivity. One caregiver said that her internet service “clogged up” due to her children attending virtual school. Although only a few mentioned that audio calls were used, several said that providers changed video visits to audio calls when there were connectivity issues. Some said audio calls were inferior to video visits because there was no opportunity for the provider to observe the child.
Many mentioned provider-level challenges—providers not being able to use telehealth effectively, technology challenges (eg, not being able to add another provider to the visit), and not joining on time for the appointment. Some caregivers became frustrated waiting for providers to join the telehealth visit. They suggested that clinicians offering telehealth should have a system to notify caregivers when they are running late. One recommended a standardized platform for telehealth since her child attends specialty clinics in several institutions and each hospital uses a different telehealth platform. Another recommended a live chat option for troubleshooting during the visit. A few said that providers need more education about telehealth because there is a lot of variability in providers’ abilities to use/provide telehealth.
Theme 4. There were clinical limitations to telehealth compared to in-person visits
One of the limitations of telehealth was providers not being able to perform a thorough evaluation of the child. Many caregivers perceived it highly important for doctors to evaluate their children’s symptoms accurately, given their complex health conditions. Caregivers feared that lack of thorough evaluation could lead to misdiagnosis or administering wrong treatments. Some mentioned specific limitations with telehealth, such as doctors not being able to listen to the heart and lungs, check muscle tone, assess hip mobility, and so on. In addition, certain assessments—weight, vital signs, and so on—were only feasible with in-person appointments. Certain specialty visits were associated with the need for laboratory testing and procedures (eg, blood gas for pulmonologist or ultrasound for nephrologist) and had to be in-person rather than telehealth. Caregivers whose children did not receive home health nursing lacked or had to acquire medical equipment at home (eg, weighing scale) to facilitate telehealth. All participants acknowledged the benefits of hands-on evaluation, which they equated to better quality of care. For this reason, many said in-person appointments were better, even though they liked the convenience and safety of telehealth.
Another limitation with telehealth was maintaining good communication with the provider about their child’s health. In-person appointments yielded higher quality communication than virtual appointments (ie, doctors understood them better), and video visits were better than audio appointments. Some felt telehealth resulted in miscommunication. Technical disruptions further inhibited clear communication. However, for others, telehealth was comparable to in-person visits in terms of communication. In-person interactions were more personable/enjoyable for caregivers and/or children than electronic ones; telehealth was impersonal. Interestingly, 3 caregivers said they preferred in-person appointments because they were a “people person.” One mentioned that with in-person visits, they could get printed documentation about the visit; this was not possible with telehealth visits.
Theme 5: Caregivers were satisfied with telehealth and wished telehealth to remain an option beyond the pandemic
Overall, caregivers felt that telehealth was a “good option,” “fantastic,” “great benefit,” especially for CMC. Many caregivers preferred telehealth appointments. Some said they requested telehealth when scheduling appointments. For some children, all visits during the pandemic were telehealth visits.
There was variability in whether telehealth was offered—telehealth was not offered at all or not offered frequently enough. There was marked variability in which specialty departments offered telehealth, and telehealth was not an option for some specialties. Some mentioned that telehealth was offered early in the pandemic but was not continuing to be offered. Caregivers wished that more providers/specialties would offer telehealth and more frequently. When asked what policy makers should know about telehealth, most caregivers said that they wanted telehealth to continue beyond the pandemic years.
Caregivers prefer to have a choice between telehealth versus in-person when scheduling appointments. Given the choice, they would select the mode of appointment according to the current needs of their children—sick or well, level of complexity. Therefore, their preference for telehealth varied by specialty and that preference shifted based on the child’s changing needs. Some preferred telehealth for certain types of visits—follow-up rather than initial visits with specialists, regular visits with primary care physicians rather than specialist visits, and visits to discuss symptoms and treatment plan changes. When the caregivers thought their children were stable, or did not require hands-on assessment, they preferred telehealth. Specialty visits that did not require checking oxygen levels, weight, lab tests, or procedures were often preferred as telehealth.
Subgroup Differences
We did not discern differences in qualitative themes based on the 6 subgroups of interest, participant characteristics, or caregiver survey responses about telehealth experiences. The only exception was that the 2 caregivers who reported on the survey that they did not use EHR portal and another who rated very low comfort level with EHR portal were Spanish-speaking interview participants. Two of these 3 participants described in interviews that they did not use EHR portal.
Discussion
Since CMC are the highest users of clinical services of all children, their caregivers likely have the most experience with telehealth. To our knowledge, there are no prior reports of caregiver experiences about telehealth for primary or specialty care appointments of CMC. Caregivers in our study found telehealth to be a valuable option for CMC to receive care during the pandemic and strongly felt that telehealth should remain an option beyond the pandemic. Telehealth flexibilities have now been made permanent by NC Medicaid. 22 Commercial insurance companies are evaluating whether to continue telehealth services for their beneficiaries after the end of the public health emergency. 16 Results of our study could guide policymakers in making decisions about keeping telehealth as an option for pediatric care.
Caregivers in our study reported that providers did not offer telehealth consistently, and there was a lot of variability based on specialty. This is consistent with studies based on EHR data and provider reports.15,23 Such interspecialty or intraspecialty variability in telehealth offering is problematic for CMC because they receive care from many different specialists. Pediatric practices should be organized in such a way that telehealth is integrated into providers’ workflow. Providers should offer telehealth as an option to caregivers when scheduling appointments. Another challenge with offering telehealth is the lack of consensus in what conditions or aspects of care are amenable to telehealth.23,24 Interestingly, caregivers had clarity about what visits are suitable for telehealth and felt that they should have a choice about when to use telehealth versus in-person visit for an appointment.
One of the main challenges with telehealth was the problem with internet connectivity. In fact, 13 caregivers had some form of challenge with video interviews for this study. Good-quality internet connection is imperative for telehealth to be useful. Internet access should be considered a social determinant of health and be made universally available. 25 In our study, 2 Spanish-speaking caregivers did not have access to EHR portal, and consequently could not access telehealth for their children. Systems created for English-speaking families could create inequities in health care delivery. 26 Children of minority race are more likely to miss specialty appointments. 27 Future research is needed to evaluate whether telehealth can be a solution to reducing disparities in access to care for CMC. 24
There are limitations to our study. The study is limited to a single institution and focused on specialty care. Experiences about telehealth may be different for other institutions. However, caregivers discussed their experiences with primary care and specialty care outside BCH as well. As this is a qualitative study, the extent of benefits and challenges could not be quantified. Although we purposively recruited children of 6 priority populations, we could not achieve this goal for black CMC. Studies focused specifically on minority CMC are needed to better understand inequities in telehealth delivery.
Caregivers of CMC are satisfied with telehealth and find it to be a viable option for outpatient care delivery for their children, even outside of the COVID-19 pandemic. There are many challenges with telehealth, especially not being offered consistently by providers. Our study results can be used by policymakers to make decisions about continuation of telehealth flexibilities, and by providers to implement changes in their practice.
Author Contributions
SN contributed to conception and design; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; critically revised manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
HDF contributed to acquisition and analysis of data; critically revised manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SLG contributed to design; contributed to acquisition, analysis, and interpretation of data; critically revised manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Appendix A
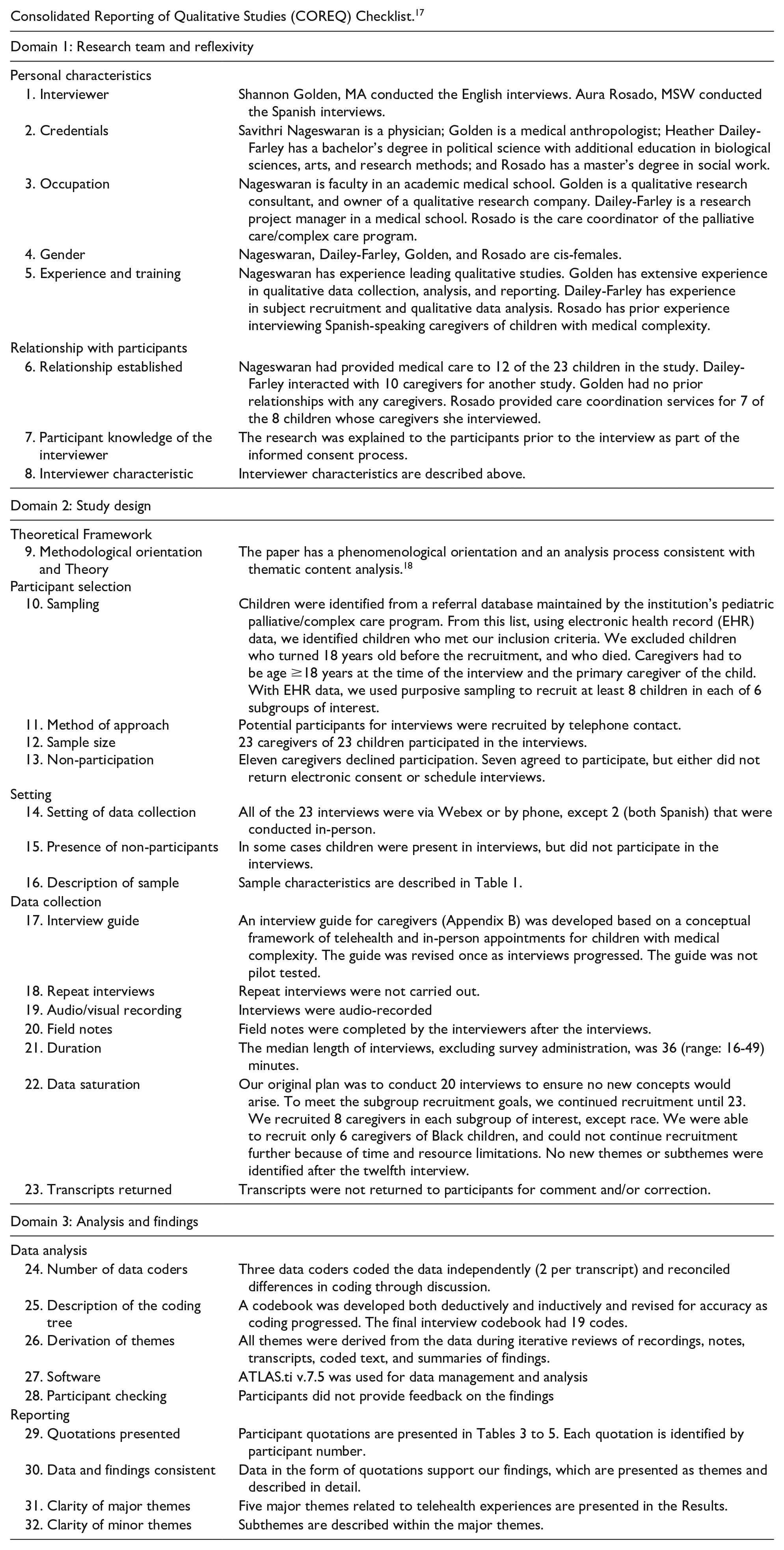
Consolidated Reporting of Qualitative Studies (COREQ) Checklist. 17
| Domain 1: Research team and reflexivity | |
| Personal characteristics | |
| 1. Interviewer | Shannon Golden, MA conducted the English interviews. Aura Rosado, MSW conducted the Spanish interviews. |
| 2. Credentials | Savithri Nageswaran is a physician; Golden is a medical anthropologist; Heather Dailey-Farley has a bachelor’s degree in political science with additional education in biological sciences, arts, and research methods; and Rosado has a master’s degree in social work. |
| 3. Occupation | Nageswaran is faculty in an academic medical school. Golden is a qualitative research consultant, and owner of a qualitative research company. Dailey-Farley is a research project manager in a medical school. Rosado is the care coordinator of the palliative care/complex care program. |
| 4. Gender | Nageswaran, Dailey-Farley, Golden, and Rosado are cis-females. |
| 5. Experience and training | Nageswaran has experience leading qualitative studies. Golden has extensive experience in qualitative data collection, analysis, and reporting. Dailey-Farley has experience in subject recruitment and qualitative data analysis. Rosado has prior experience interviewing Spanish-speaking caregivers of children with medical complexity. |
| Domain 1: Research team and reflexivity | |
| Relationship with participants | |
| 6. Relationship established | Nageswaran had provided medical care to 12 of the 23 children in the study. Dailey-Farley interacted with 10 caregivers for another study. Golden had no prior relationships with any caregivers. Rosado provided care coordination services for 7 of the 8 children whose caregivers she interviewed. |
| 7. Participant knowledge of the interviewer | The research was explained to the participants prior to the interview as part of the informed consent process. |
| 8. Interviewer characteristic | Interviewer characteristics are described above. |
| Domain 2: Study design | |
| Theoretical Framework | |
| 9. Methodological orientation and Theory | The paper has a phenomenological orientation and an analysis process consistent with thematic content analysis. 18 |
| Participant selection | |
| 10. Sampling | Children were identified from a referral database maintained by the institution’s pediatric palliative/complex care program. From this list, using electronic health record (EHR) data, we identified children who met our inclusion criteria. We excluded children who turned 18 years old before the recruitment, and who died. Caregivers had to be age ≥18 years at the time of the interview and the primary caregiver of the child. With EHR data, we used purposive sampling to recruit at least 8 children in each of 6 subgroups of interest. |
| 11. Method of approach | Potential participants for interviews were recruited by telephone contact. |
| 12. Sample size | 23 caregivers of 23 children participated in the interviews. |
| 13. Non-participation | Eleven caregivers declined participation. Seven agreed to participate, but either did not return electronic consent or schedule interviews. |
| Setting | |
| 14. Setting of data collection | All of the 23 interviews were via Webex or by phone, except 2 (both Spanish) that were conducted in-person. |
| 15. Presence of non-participants | In some cases children were present in interviews, but did not participate in the interviews. |
| 16. Description of sample | Sample characteristics are described in Table 1. |
| Data collection | |
| 17. Interview guide | An interview guide for caregivers (Appendix B) was developed based on a conceptual framework of telehealth and in-person appointments for children with medical complexity. The guide was revised once as interviews progressed. The guide was not pilot tested. |
| 18. Repeat interviews | Repeat interviews were not carried out. |
| 19. Audio/visual recording | Interviews were audio-recorded |
| 20. Field notes | Field notes were completed by the interviewers after the interviews. |
| 21. Duration | The median length of interviews, excluding survey administration, was 36 (range: 16-49) minutes. |
| 22. Data saturation | Our original plan was to conduct 20 interviews to ensure no new concepts would arise. To meet the subgroup recruitment goals, we continued recruitment until 23. We recruited 8 caregivers in each subgroup of interest, except race. We were able to recruit only 6 caregivers of Black children, and could not continue recruitment further because of time and resource limitations. No new themes or subthemes were identified after the twelfth interview. |
| 23. Transcripts returned | Transcripts were not returned to participants for comment and/or correction. |
| Domain 3: Analysis and findings | |
| Data analysis | |
| 24. Number of data coders | Three data coders coded the data independently (2 per transcript) and reconciled differences in coding through discussion. |
| 25. Description of the coding tree | A codebook was developed both deductively and inductively and revised for accuracy as coding progressed. The final interview codebook had 19 codes. |
| Domain 3: Analysis and findings | |
| 26. Derivation of themes | All themes were derived from the data during iterative reviews of recordings, notes, transcripts, coded text, and summaries of findings. |
| 27. Software | ATLAS.ti v.7.5 was used for data management and analysis |
| 28. Participant checking | Participants did not provide feedback on the findings |
| Reporting | |
| 29. Quotations presented | Participant quotations are presented in Tables 3 to 5. Each quotation is identified by participant number. |
| 30. Data and findings consistent | Data in the form of quotations support our findings, which are presented as themes and described in detail. |
| 31. Clarity of major themes | Five major themes related to telehealth experiences are presented in the Results. |
| 32. Clarity of minor themes | Subthemes are described within the major themes. |
Appendix B. Caregiver Interview Questions
As a reminder, the purpose of today’s discussion is for us to learn from you about what your child’s health care experiences have been like during the pandemic. For most of the questions, we are going to focus on March 2020 through March 2021. I know that is a while ago, but please do the best you can. This time period includes the year prior to pandemic initial shutdowns and the year after.
~ In what ways, if any, did this differ between specialists?
~ In what ways, if any, did this differ between specialists?
I would like to have a thorough understanding of the benefits and challenges of telehealth versus in-person clinic visits. You’ve told me some already, but let’s go deeper.
ASK Q6 ONLY TO CAREGIVERS WHO EXPERIENCED TELEHEALTH
Probe: tell me about audio/phone visits.
Probe: tell me about video visits.
Probe: how about benefits of telehealth for child’s therapies (PT, OT, speech etc)?
Probe: tell me about audio/phone visits.
Probe: tell me about video visits.
Probe: how about challenges of telehealth for child’s therapies (PT, OT, speech etc)?
Probe: How often do you experience these challenges?
Acknowledgements
The authors thank Ms. Aura Rosado MSW (Care Coordinator of the Pediatric Enhanced Care Program in the Department of Pediatrics at Wake Forest University School of Medicine) for recruiting and interviewing Spanish-speaking caregivers for this study.
Authors’ Note
This paper was presented at the 2023 Pediatric Academic Societies Annual Meeting as a poster presentation.
No content in this manuscript was AI-generated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by the Wake Forest Clinical and Translational Science Institute (WF CTSI) Pilot Grant (PI: Nageswaran) as part of the CTSI Pilot Grant Program and the Wake Forest Center for Biomedical Informatics (WFBMI) funded by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR001420. The content is solely the responsibility of the authors and does not represent the official views of the NIH.
Ethical Statement
The Institutional Review Board of Wake Forest University School of Medicine approved the study (IRB00072712). All participants gave written informed consent.
Data Availability Statement
While we are unable to share the actual interview transcripts (interview data) to protect the identity of study subjects, we can share summarized textual data upon reasonable request directly to the corresponding author.