
Abstract
The purpose of this study is to determine the frequency of irritable bowel syndrome (IBS) and the influencing factors in children aged 4 to 9. The cross-sectional descriptive study included 1176 children between the ages of 4 and 9 who applied for Family Medicine Centers between March 1, 2017 and April 30, 2017 for various reasons. Pediatric Gastrointestinal Symptoms Questionnaire, Roma III Version (QPGS-RIII) was applied to the volunteers (children’s parents or caregivers), and Beck Anxiety Scale was applied to the mothers accompanying their children. A total of 603 (51.9%) of the children included in the study were female and 559 (48.1%) were male. When the applied QPGS-RIII was evaluated with IBS diagnostic criteria, IBS was found in 137 children and IBS frequency was found to be 11.8% (95% confidence interval [CI]). Significant differences were found in socioeconomic level, eating habits, TV-watching habits, and IBS status (P < .05).
Introduction
Irritable bowel syndrome (IBS) is a common syndrome that is seen more frequently in girls than boys in most studies, 1 and it is seen in various studies with a frequency of approximately 6% to 14% in childhood, although it is not yet possible to obtain precise data. 2 Irritable bowel syndrome is not life-threatening but deteriorates the quality of life; presents with long-term and recurrent abdominal pain in the absence of an organic or metabolic disease, often with constipation and diarrhea, followed by a change in bowel habits with abdominal complaints. It is known as the most common cause of recurrent abdominal pain.3,4 There is no specific biochemical, histopathological, and radiological diagnostic test to diagnose IBS; the diagnosis is based on well-defined anamnesis and symptoms but organic gastrointestinal diseases should be excluded. 5 Although it is a very common syndrome in primary and gastroenterology clinics, it is often difficult to diagnose if no abnormality is found in the examinations. 6 As IBS is a functional disease, there is no specific examination, laboratory or imaging method for its diagnosis in primary care. Diagnosis is based on symptoms; however, these are not sufficiently specific to IBS either. In view of the lack of underlying organic cause, a symptom-based approach, namely the Rome criteria, has been proposed for better diagnosis without the need for exclusionary testing. Therefore, diagnostic criteria based on Manning, Rome I, Rome II, and Rome III symptoms became the basis for epidemiological studies. 7 Finally, in June 2016, the Rome IV Criteria began to be used. 8 In our country, there is no standardized primary-care approach or comprehensive research performed in primary care in children with abdominal pain and defecation disorders. The aim of this study was to determine the frequency of IBS in children aged between 4 and 9 years in central Izmir, and the factors that affect IBS, and to determine the relationship between mother anxiety and child IBS by applying Beck Anxiety Scale to mothers.
Materials and Methods
This is a cross-sectional descriptive study. In this study, 1176 children aged between 4 and 9 years were included via random sampling method from each of the 11 central districts of Izmir, from 15 family health centers, some in rural areas, and some in urban areas.
Izmir is the third-most populous city of Turkey and is located in the Aegean Region This city receives an increasing number of immigrants from all over the country, and in terms of demographic characteristics, it has a good socio-economic level and a high literacy rate. The population aged 4-9 and registered in the Family Health Centers in the central districts of Izmir was determined as 181.317 at the time of the study. Sampling size was found by stratifying according to age with a known sample formula. The number of children stratified by age was distributed proportionally to the number of children in each district within each age group.
Data were collected face-to-face. After obtaining the necessary permissions, parents who volunteered and signed consent to participate in the study were asked to complete a questionnaire including demographic features, the Pediatric Gastrointestinal Symptoms Questionnaire Rome III Version (QPGS-RIII) (Table 1), and Beck Anxiety Inventory. Mental retardation and alarm symptoms in the child are exclusion criteria. Potential alarm features in children with IBS are as follows: family history of inflammatory bowel disease, celiac disease or peptic ulcer disease, persistent right upper or lower abdominal pain, dysphagia, odynophagia, persistent vomiting, gastrointestinal blood loss, nocturnal diarrhea, arthritis, perirectal disease, involuntary weight loss, deceleration of linear growth, delayed puberty, and unexplained fever. The families of the children who were thought to have IBS as a result of the questionnaire analysis were informed and directed about further investigations.
Irritable Bowel Syndrome. 8
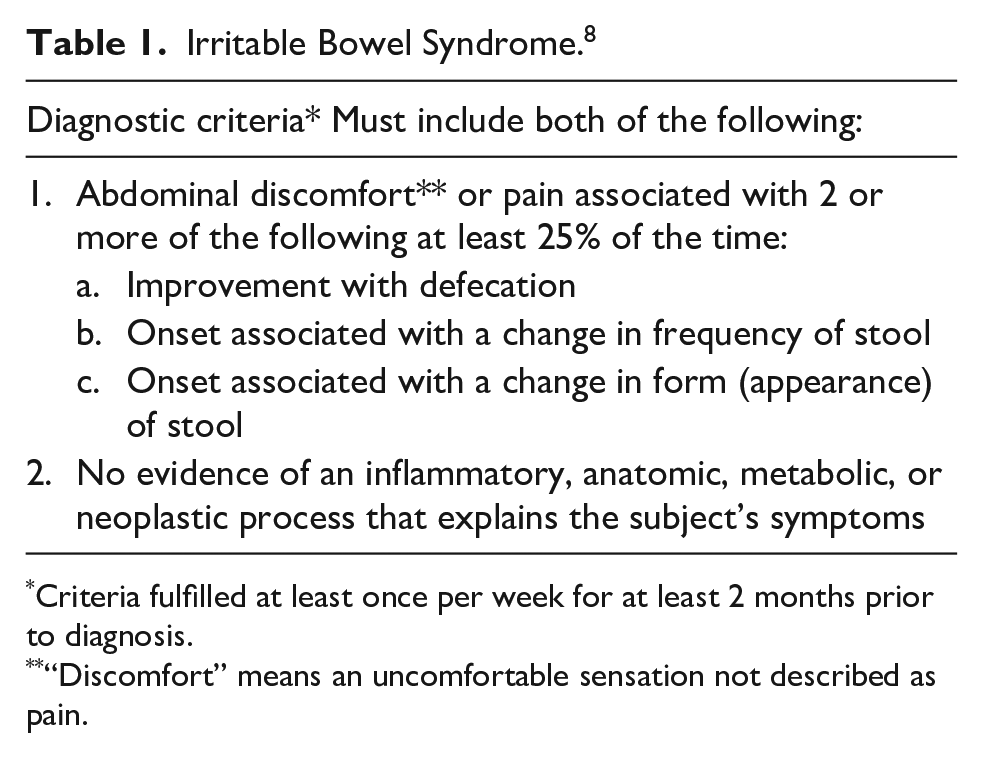
Criteria fulfilled at least once per week for at least 2 months prior to diagnosis.
“Discomfort” means an uncomfortable sensation not described as pain.
Pediatric Gastrointestinal Symptoms Questionnaire Rome III Version
Rome III criteria include 2 separate questionnaires for ages 4 to 9 and 10 to 18. According to the criteria, children in these age ranges can be diagnosed with functional dyspepsia, IBS, abdominal migraine, functional abdominal pain, functional abdominal pain syndrome, functional constipation, nonretensive fecal incontinence, aerophagia, and cyclic vomiting syndrome.
Pediatric Gastrointestinal Symptoms Questionnaire Rome III IBS criteria are in Table 1. For IBS diagnosis, the patient must meet all criteria.
*These criteria must be fulfilled at least once a week in the 2 months preceding the diagnosis.
A validity and reliability study was conducted by Özgenç et al. 9
Beck Anxiety Inventory
The scale was developed by Beck et al., which measures the severity of anxiety experienced by individuals; it was designed to investigate subjective anxiety and somatic symptoms. Consisting of 21 items which are scored Likert type between 0 and 3, it is completed by the patient alone. The score range is 0 to 63. Higher total scores on the scale indicate greater severity of anxiety. Around 8 to 15 points are considered mild anxiety, 16 to 25 points, moderate anxiety, and 26 to 63 points, severe anxiety. Validity and reliability studies for Türkiye were performed by Ulusoy et al. 10
Statistical analyzes were performed using the SPSS 15.0 package program. Frequency distributions were calculated, chi-square and Fisher’s exact tests were used for categorical variables, t-test, and analysis of variance (ANOVA) were used for continuous variables in comparative analyses. Statistical significance was set at P < .05 for all analyses.
Ethics clearance was required from Dokuz Eylül University Ethical Board (2016/08-46).
Results
The participants of the study are 1176 children who applied to 15 Family Health Centers in Izmir city center for any reason. According to the predetermined exclusion criteria, 11 with alarm symptoms and 3 with digestive system disease were excluded and analyzes were performed on 1162 people.
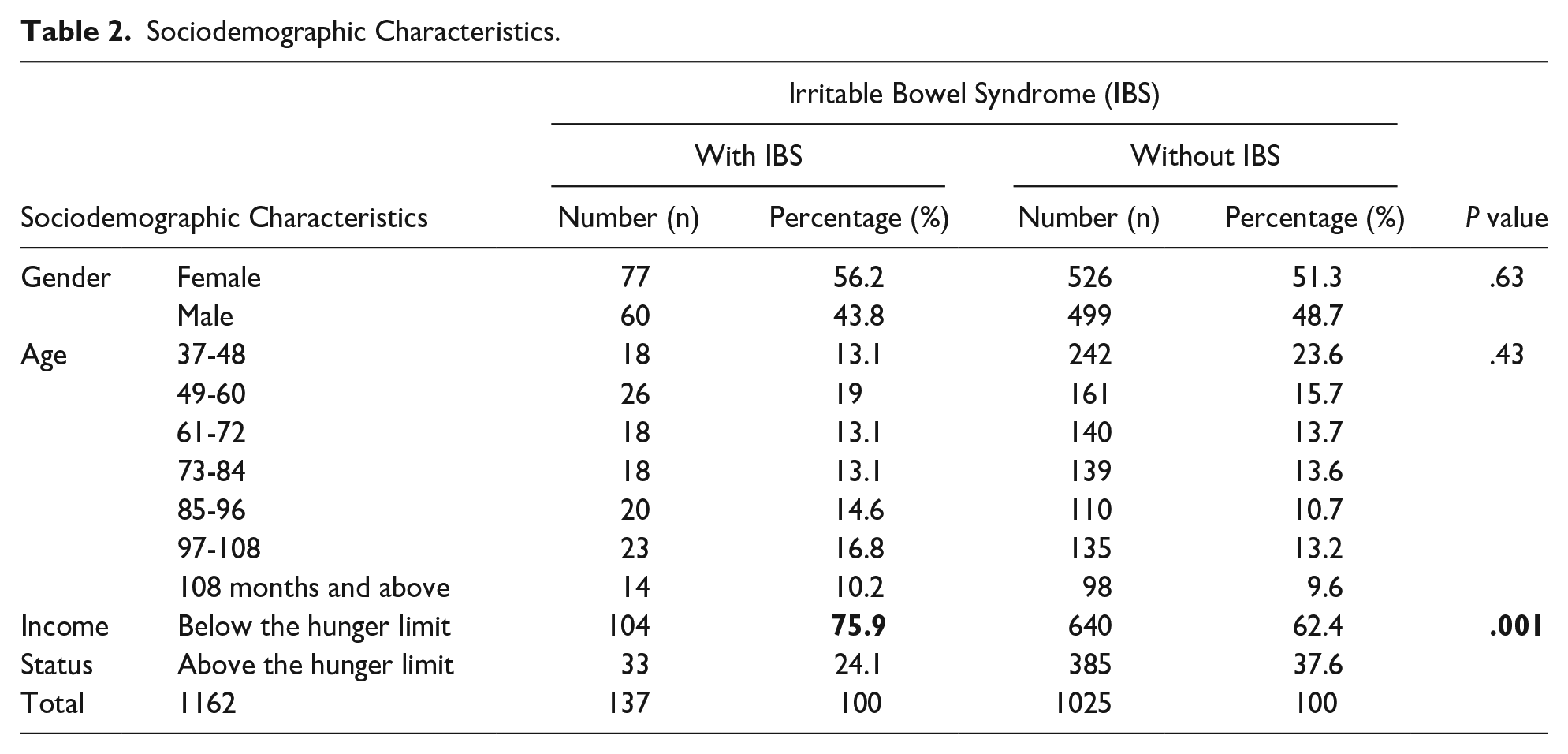
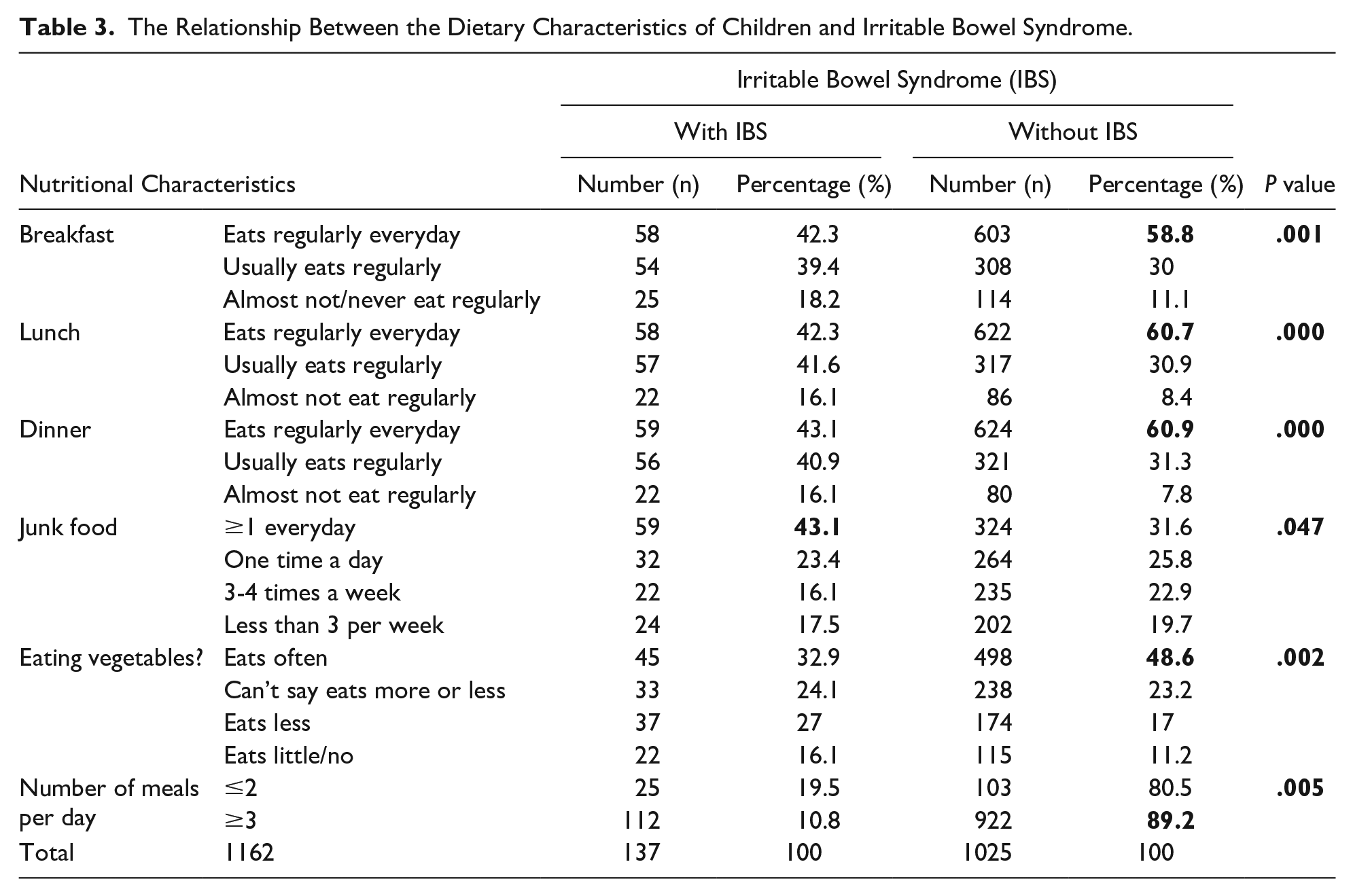
When 1162 children were evaluated with the QPGS-RIII scale IBS Diagnostic Criteria, IBS was determined in 137, and the incidence of IBS was found to be 11.8%. According to our findings, 56.2% (n = 77) of those with IBS were girls; 19% (n = 26) were between 49 and 60 months; 51.8% were between 11 and 20 kg. When the income level of the families was examined, it was determined that 75.9% of these were from low monthly income families (Table 2). No IBS was observed among 91.8% (n = 603) of those who regularly had breakfast, 91.5% (n = 622) of those who regularly had lunch, and 91.4% (n = 624) of those who regularly had dinner. A significant difference was found between the children’s number of daily meals and IBS (P = .005). Irritable bowel syndrome was found in 19.5% of those who ate only 1 or 2 meals a day, but only 10.8% of those who ate at least 3 meals a day. There was a significant relation between the regularity of children’s and IBS. It was observed that 58.8% (n = 58) of the children without IBS ate breakfast regularly (P = .001), 60.7% (n = 58) had regular lunch (P = .000) and 60.9% (n = 59) had regular dinner (P = .000).
Sociodemographic Characteristics.
A significant difference was observed between children’s consumption of junk food and IBS (P = .047). It was determined that 43.1% (n = 59) of those with IBS consumed more than one portion of junk food per day. There was a significant difference between children’s food choices and IBS development (P = .006). It was observed that 27% (n = 37) of the children with IBS had a limited range of food preferences. No significant relation was found between the children’s meat-eating habits and the development of IBS (P = .051). However, a significant difference was observed between vegetable consumption and IBS development (0.002); it was determined that 43.1% (n = 59) of those with IBS ate few or no vegetables.
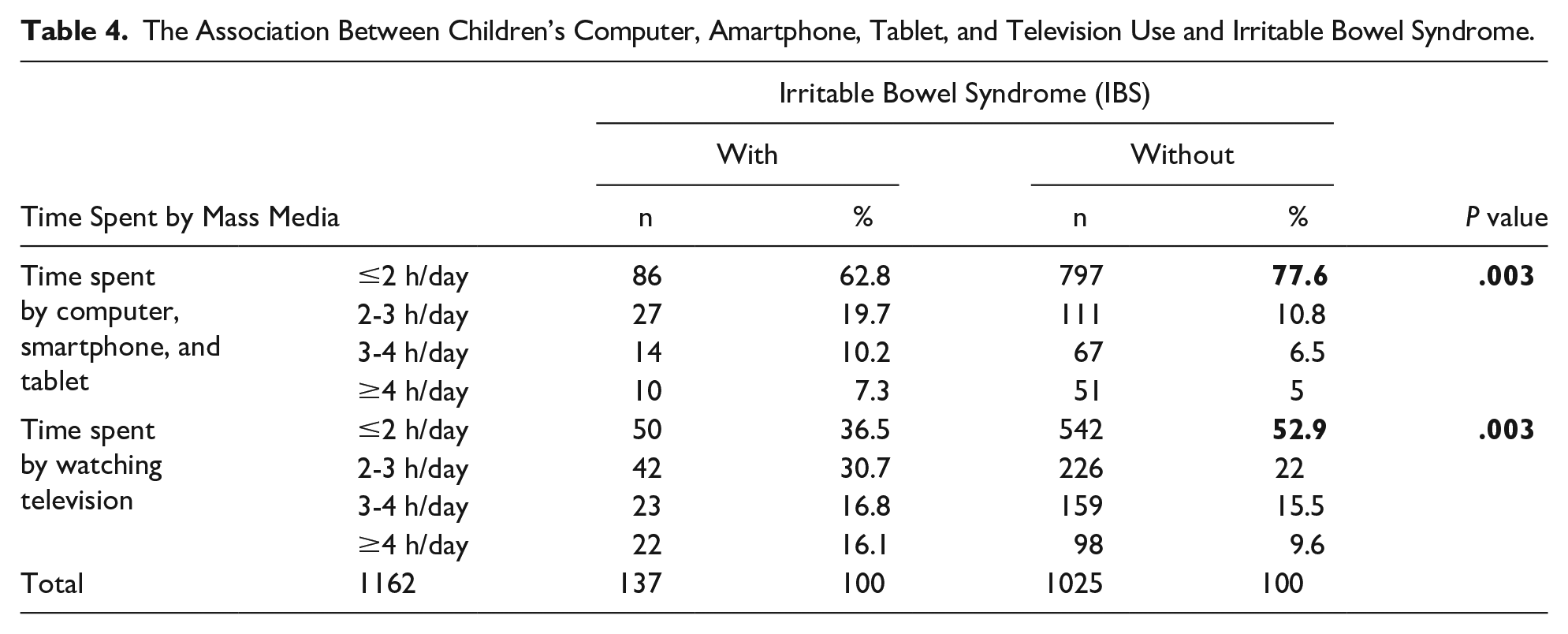
The relationship between IBS and the time children spend with mass media was examined, and a significant relation was found. Considering the time spent with devices such as computers, smartphones, and tablets, it was found that 55% of those without IBS spent less than 1 hour a day (P = .003). Regarding the time they spent watching television, 81% of those with IBS watched television more than 1 hour a day (P = .003).
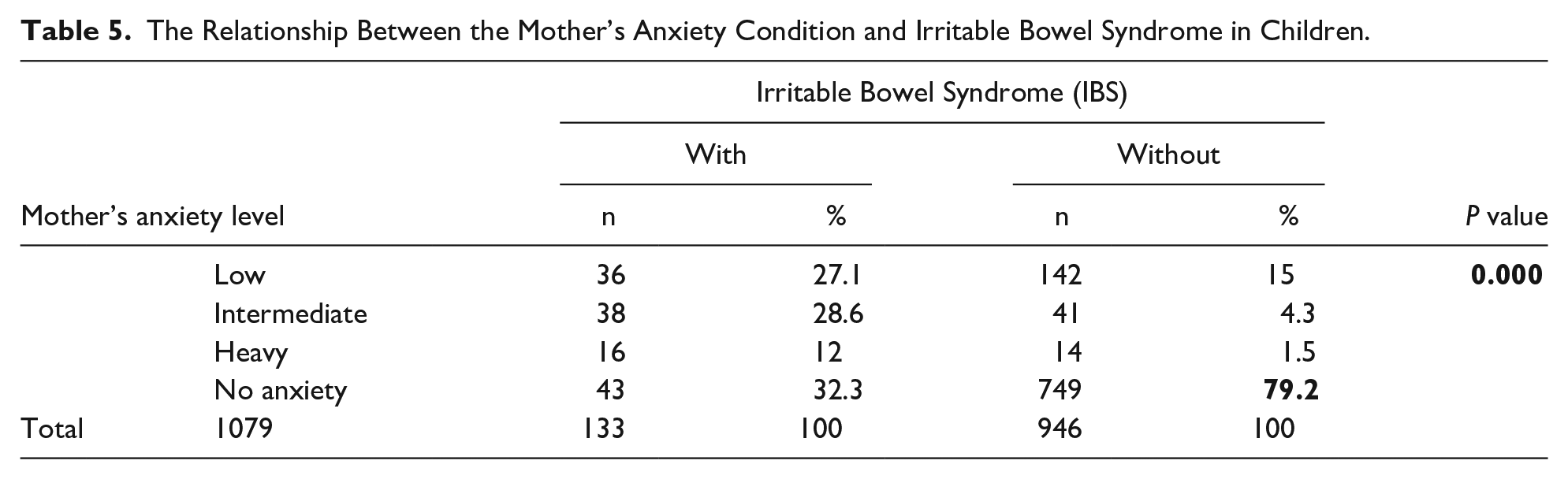
There was a significant relation between the presence of anxiety in the mother and the development of IBS in the child (P = .000).
When the relationship with IBS was examined, there was a significant difference between the child’s nutritional habits (except meat consumption), the number of meals, computer and television habits, the presence of anxiety in mother, and the development of IBS (P < .05) (Tables 3, 4, and 5). No significant relationship was found between IBS and the following variables: sex, age, weight, regularity of physical activity, amount of sleep, and breast milk intake (P > .05).
The Relationship Between the Dietary Characteristics of Children and Irritable Bowel Syndrome.
The Association Between Children’s Computer, Amartphone, Tablet, and Television Use and Irritable Bowel Syndrome.
The Relationship Between the Mother’s Anxiety Condition and Irritable Bowel Syndrome in Children.
Discussion
Recurrent abdominal pain (RAP) is a condition in children that is costly and difficult to diagnose and treat, frustrating for the family and child, deteriorates the quality of life, and can be accompanied by psychiatric problems. 11 Irritable bowel syndrome is a common cause of recurrent abdominal pain in childhood. 3
Reports in Turkey and worldwide on IBS in childhood report different prevalence percentages. In a study in China, the prevalence of the disease was found to be 13%, and this varies between regions. In a meta-analysis of 58 articles, the incidence of IBS was 8.8%. 10
In our country, no studies were conducted to determine the incidence of IBS in childhood in primary care, and the only application of Rome II Criteria was to 2217 students freshman students at Abant İzzet Baysal University, and the prevalence of IBS was found to be 10.8%. 11 However, there are studies conducted in the second and third levels of care.
Irritable bowel syndrome is a long-term and recurrent functional syndrome that negatively affects the quality of life and negatively affects education. There is no specific test to diagnose IBS; rather, diagnosis is made by excluding organic gastrointestinal diseases. 5 Although it is a very common syndrome in primary-care clinics, pediatric and pediatric gastroenterology clinics, it often presents with no abnormalities on the physical exam. 6 Recurrent abdominal pain is often called functional abdominal pain during clinical practice, and if patients 4 to 18 years of age meet Rome criteria, can be diagnosed as IBS. 12
Irritable bowel syndrome is a disease that can be effectively managed by primary-care physicians, but it is often referred to pediatric gastroenterologists, leading to high costs. 13 In our country, there is no widespread standardized screening method for the diagnosis of IBS, and the data on the frequency of IBS in childhood is insufficient. Therefore, in this study, we aimed to determine the frequency of IBS and the factors affecting in children 4 to 9 years of age in Izmir; we propose an easy-to-implement, cost-effective, and noninvasive diagnostic method to raise awareness of the Rome Criteria. In the study, the QPGS-RIII scale was applied to a sample of children aged 4 to 9 years in central Izmir, and the incidence of IBS was found to be 11.8%.
In the literature, there is no variation according to age, but in terms of gender, IBS is seen more frequently in girls than boys. 14 As a matter of fact, this latter trend is found in most of the studies conducted in the world.1,2,15 In this study, similar to the literature, no significant difference was found according to age, but in contrast to most studies, no significant gender difference was found in terms of IBS.
Determining the health level of the society in relations to the economic level is very important in health studies. In this study, it was aimed to identify any potential relationship between IBS and economic level by determining the families’ total monthly income. Based on data from the Turkish Statistical Institute in March 2016, when the survey was conducted, the poverty line was set at around 1500 TL, which was the estimated monthly income required for a family of 4. 16 In this study, the rate of families with monthly income below this established limit was 64%. A significant difference was found between the economic level and IBS. Around 75.9% of the children with IBS were from families with incomes below the hunger limit (Table 2). This finding is supported by a study conducted in Europe showing that the decrease in health services, decreased quality of life, and increased life stressors were associated with IBS in people with low socioeconomic status. 17 Therefore, the reason for the high numbers of children with IBS in families with income below the hunger limit may be their greater exposure to life stressors, as well as the lack of access to eat fiber-rich foods, fewer daily meals and the lack of a balanced diet. Although a lower family income and lower level of education appeared to result in a higher percentage of children experiencing functional abdominal pain disorders, in most studies, this trend was not statistically significant. 18
Concerning the relationship between childhood IBS and nutrition, there is not enough data in this area. A 2009 Cochrane review concluded that the regulation of diet to treat IBS in children and adolescents does not have a high level of evidence, but probiotic supplementation with lactobacilli is beneficial. 19 However, the knowledge that the diet exacerbates the symptoms of IBS provides a valid justification for our suspicion of diet.
Most of the dietary recommendations made so far consist of recommendations for healthy nutrition for IBS patients. Several studies have shown the effect of skipping meals on IBS. In these studies, irregular feeding and skipping meals have been shown to affect colonic motility and exacerbate IBS symptoms. However, there is currently no high-level study showing that irregular feeding has an effect on IBS. 20
In some studies, the relationship habits are investigated between the prevalence of IBS with regular eating, and the prevalence of IBS was found to be high in patients with irregular meals per day in studies in Turkey, Japan, and Korea. 21 In our research, we discovered that most children suffering from IBS maintain a regular eating schedule with breakfast, lunch, and dinner. In addition, we observed that 89.2% of those who do not have IBS also consume at least 3 meals regularly (Table 3). It is worth considering that the relatively low occurrence of IBS might be attributed to the frequent and consistent meal consumption, as IBS patients are commonly advised to eat smaller, more frequent meals. 20
In this study, the consumption of unhealthy snacks (junk food) and IBS were significantly different (P = .047). It was found that 43.1% of the patients with IBS consumed more than one portion of junk food per day (Table 3). Unfortunately, there is no study in the literature on this subject. However, the unhealthy snacks contain additives, preservatives, colorants, and these may be related to the development of hypersensitivity reaction and intolerance in IBS patients whose digestive system is more sensitive than average. 22
In our study, it was seen that approximately half of the children without IBS consumed vegetable meals quite or very frequently (Table 3). However, while there was a significant difference between vegetable consumption and IBS (.002), this significance was not found for meat consumption (.051). In the literature, we found no studies with substantial evidence to explain the relationship between IBS and diet; no relationship was found in several randomized controlled trials. 19 Hence, this finding holds significance as it is among the initial evidence pointing to a potential inverse connection between a diet rich in vegetables and IBS. Nevertheless, it is premature to definitively determine the influence of nutrition on IBS at this stage. Nonetheless, it is crucial to monitor the patient’s dietary intake and tailor the treatment accordingly. 23 It is clear that more research is needed in this area. This study focused on the effect of a sedentary lifestyle and its relationship with IBS. For this reason, questions focused on the use of electronic communication devices such as television, tablets, computer, smart phone, and the amount of regular physical activity. There was a significant difference between the time spent on IBS and television (P = .003) and the time spent on computers, tablets, and smartphones (P = .003). There was, however, no significant difference between regular physical activity and IBS (P = .211). It was seen that 77.6% of those without IBS spent less than 2 hours a day with computers, smartphones, tablets, and 52.9% of those without IBS spent less than 2 hours watching TV (Table 4). When we look at the literature, many studies investigated whether sedentary life increases symptoms in patients with IBS, but most of these evaluated this in terms of amount of physical activity. However, in a study conducted on children, it was emphasized that spending much time with electronic communication devices may lead to a sedentary life in the long term, disrupt sleep patterns, and increase IBS symptoms. 24 Therefore, the relationship between IBS and a sedentary lifestyle is not limited to physical exercise. Further research is needed to evaluate the time spent with electronic communication tools.
To investigate the factors affecting IBS in children, Beck Anxiety Scale was applied to the mothers accompanying the children attending Family Health Centers to examine the effect of mothers’ anxiety status on child IBS. A significant difference was found between anxiety status of 1079 mothers and IBS in children (P = .000). According to this, of the children without IBS, 79.2% had mothers who did not have anxiety. When the relationship between IBS and anxiety is considered, some studies show that parents’ anxiety is reflected in children’s temperament from the age of 1 year and that anxiety in later life is associated with recurrent abdominal pain. 19 In addition, studies on children and adolescents have shown that anxiety and depression are common symptoms in addition to intestinal symptoms in functional gastrointestinal system diseases. 25 In this study, a significant difference was similarly found between mother’s anxiety and child IBS, and it was concluded that this study supports the studies in the literature.
Implication for Practice
In our country, there is no standard primary-care approach and comprehensive research performed in primary care in pediatric patients with abdominal pain and defecation disorders. This leads to unnecessary examinations, serious financial burden, and deterioration in the quality of life of the child. With the increase and awareness of the use of the Rome Criteria, as used in this study, more children can be screened in the first step, reducing unnecessary costs and improving the quality of life of the child and the family. This disease has a negative effect on the child’s biopsychosocial development. In this study, we aimed to raise awareness about the diagnostic and treatment methods like QPGS-Roma III criteria and determined the incidence of IBS in children aged 4 to 9 years in family health centers in Izmir province to be 11.8%. Contrary to popular belief, IBS is not only an adult disease; we have demonstrated that it is a childhood common disease with negative effects.
There were some limitations of our study. While we inquired about alarm symptoms to caregivers to rule out organic diseases, we did not conduct any laboratory or imaging tests. Consequently, it is possible that a child with IBS was excluded from the study solely because they exhibited an alarming symptom. In addition, IBS is a disease that is thought to have familial transmission. However, we could not determine the existence of IBS in to all of the family because this would have involved reaching out to both the mother and father, and to siblings, if any, and to applying the age-appropriate Roman criteria. However, the time and resource limitations mean that this focus was not appropriate for our study. We did not investigate in detail about this disease and the underlying factors, or the negative impact on the child’s biopsychosocial development.
Given that our study was carried out in primary-care settings and focused on children, we acknowledge a limitation in reaching a lower number of affluent and educated families compared to the broader population. This is because socioeconomically disadvantaged families often tend to have more children. More recently, family physicians have begun to care for the child starting from birth and providing follow-up and health protection; bringing an opportunity to recognize this disease with a simple screening test. They can provide guidance that can prevent harm to the physical and mental health integrity of the child; thus, they can increase in the quality of life of the child.
Authors’ Contribution
LAD: Design, Data collection, Material, Analysis, Draft writing, Review.
OG: Material, Analysis, Draft writing, Review
NÖ: Data Collection, Analysis, Draft writing, Review, Critical review
Footnotes
Acknowledgements
All the authors would like to thank to Simon Mumford for English language editing and also would like to thank all the Family Physicians who were participated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.