
Abstract
Bed sharing increases risk of sleep-related infant deaths. We hypothesized that infant sleep difficulties increase bed sharing, independent of social determinants of health (SDOH). In total, 191 mother-infant dyads in a prospective, longitudinal cohort study completed the Brief Infant Sleep Questionnaire at 1, 4, 6, and 12 months. Sleep characteristics at 1 month (latency, duration, night awakenings) were compared between dyads with/without bed sharing in the first 12 months. Infants who participated in bed sharing slept fewer hours at night (7.1 ± 1.7 hours vs 8.3 ± 1.5 hours, P = .001, d = −0.79), and took longer to fall asleep (0.7 ± 0.6 hours vs 0.5 ± 0.5 hours, P = .021, d = 0.43), even when controlling for SDOH variables that influence bed sharing. Maternal perception of sleep problems did not differ between groups (P = .12). Our findings suggest that infants with quantifiable sleep difficulties at 1 month are more likely to bed share.
Keywords
Introduction
There has been minimal decline in sleep-related infant deaths over the last 20 years. Public health campaigns in the 1990s helped initiate the decrease in sleep-related infant deaths, but according to the American Academy of Pediatrics (AAP), up to 3500 infants still die of sleep-related deaths in the United States each year. 1 Sudden unexplained infant deaths are a leading cause of infant mortality in the United States and many are preventable deaths. 2 The AAP published updated safe sleep guidelines in 2022 to expand upon recommendations to improve infant safety during sleep, with the goal of decreasing the number of preventable infant deaths each year. 1
The new guidelines describe in greater detail recommended sleep surfaces and areas, infant dress for sleep, benefits of feeding with human milk, and avoidance of smoke, alcohol, and drug exposure to decrease infant sleep-related deaths. 1 The AAP remains firm on not recommending bed sharing under any circumstance. 1 Bed sharing occurs when an infant and caregiver sleep together on any surface such as a bed, couch, or chair. The risk for sleep-related deaths associated with bed sharing increases in the presence of risk factors such as prematurity, impairment of caregiver, caregiver smoking, and softness of shared surface. 3 Studies have found that avoidance of bed sharing is one of the most difficult recommendations to consistently follow. 4 Identified barriers include intentional decisions to bed share for ease of breastfeeding and increased maternal sleep as well as unintentional actions such as falling asleep during feedings or consoling of infants. Bed sharing is perceived as helping parents obtain more sleep. 5
Bed sharing risk may increase throughout the night. One study that used videos of infant sleep overnight showed that of infants who changed sleep locations, 67% shared their sleep surface with another person after the transition. 6 Another study also examined the safety of infant second sleep practices which are defined as sleep practices after a nighttime awakening. Approximately 20% of infants who initiated sleep in their own sleep space switched to bed sharing after a nighttime awakening. 7 Previous studies have highlighted that mothers with less education were more likely to participate in unsafe sleep practices. 4 Bryan et al 7 found that parents with a 4-year degree or higher education level had a higher prevalence of unsafe second sleep practices, and as seen in previous studies, second sleep practices tend to be less safe than at initiation of sleep. Parents >30 years old specifically had a higher prevalence of meeting safe sleep criteria at sleep onset, but a lower prevalence after nighttime awakening. 7 These studies suggest that parents with intentions of following safe sleep practices at the start of the night consider changes toward unsafe sleep practices as sleep is disrupted. We were interested to learn if actual or perceived difficulty of infant overnight sleep contributed to bed sharing.
This study used a longitudinal cohort of mother-infant dyads to test the hypothesis that sleep difficulty at 1 month of age would be associated with bed sharing in the first 12 months, irrespective of social determinants of health (SDOH).
Methods
Ethics Statement
This study was approved by the Independent Review Board at Penn State College of Medicine (STUDY00008657). Written informed consent was obtained from all participants at the time of enrollment. The study was registered on clinicaltrials.gov (NCT04017520).
Participants
This study used a prospective, longitudinal cohort design to assess sleep practices among breastfeeding mother-infant dyads from birth through 12 months of age. Singleton infants delivered at term (37-42 weeks gestation) were eligible. Dyads with maternal or infant factors that could impact feeding (eg, maternal drug use or HIV, infant metabolic disease, or neonatal intensive care unit admission), factors affecting long-term follow-up (eg, plan for primary pediatric care outside our medical center, plan for infant adoption), or inability to complete surveys in English were excluded. A convenience sample of infants was enrolled within 7 days of delivery. Enrollment occurred between April 20, 2018 and October 5, 2020 at the newborn nursery or the outpatient pediatrics clinics affiliated with our academic medical center. There were 2487 infants screened for eligibility and 359 met inclusion criteria. There were 221 dyads who consented to participate, and 191 completed sleep surveys. The primary medical outcome was bed sharing at any time during the first 12 months after birth. Dyads who completed the study were dichotomized into 2 groups (bed sharing or no bed sharing) through administration of the Brief Infant Sleep Questionnaire (BISQ) at 1, 4, 6, and 12 months. Parents who endorsed bed sharing (at any timepoint) when asked, “What is your child’s sleeping arrangement” were assigned to the bed sharing group (n = 38).
Measures
Electronic surveys administered by research staff were used to assess demographic factors and SDOH for all dyads. The following characteristics were assessed: maternal age, maternal race, maternal education level, family income, medical insurance status, marital status, maternal depression (present/absent), number of individuals living in the household, infant sex, infant gestational age, and infant birth weight. The following elements of the BISQ were used to measure difficulties with infant sleep at 1 month of age: total time asleep at night (hours), total time awake at night (hours), and time required to put infant to sleep (hours). At 1 month of age, mothers also subjectively reported “Do you consider your child’s sleep to be a problem?” (Yes/No). We chose the 1-month timepoint because this is the earliest well-child check when concerns about sleep patterns typically arise.
Statistical Analysis
Student t- tests, Mann-Whitney U tests, or chi square tests were used to compare demographic factors and SDOH between bed sharing and non-bed sharing groups. Variables that differed between groups were assessed in a binomial regression analysis, where bed sharing was the dependent variable, sleep difficulty (total night sleep) was the independent variable, and demographic and SDOH factors that had displayed between group differences were selected as covariates. Omnibus likelihood ratio tests were performed for each variable. Model fit (McFadden R2) and accuracy for predicting bed sharing (sensitivity, specificity, area under the curve [AUC]) were reported.
Results
Participants
Participating mothers had an average age of 30 years (±5) and were predominantly white (141/191, 74%) (Table 1). Approximately half of infants were women (104/191, 54%). They had an average gestational age of 38.9 (±1) weeks, and an average birth weight of 3351 (±448) g. Most mothers were married (143/191, 75%), had private health insurance (154/191, 81%), and had a college or postgraduate degree (133/191, 70%). Few mothers reported depression (29/191, 15%). Most families (99/191, 52%) reported a household income above $75 000 per year, and the median household size was 4 individuals (range 2-9). Sixteen of the 38 mother-infant dyads who admitted to bed sharing were doing so at 1 month. Mother-infant dyads who participated in bed sharing during the first 12 months were less likely to have a college or postgraduate degree (P = .029, X2 = 10.8) and less likely to report an income above $50 000 (P = .019, X2 = 5.4). They did not differ in other demographic factors or SDOH.
Participant Characteristics.
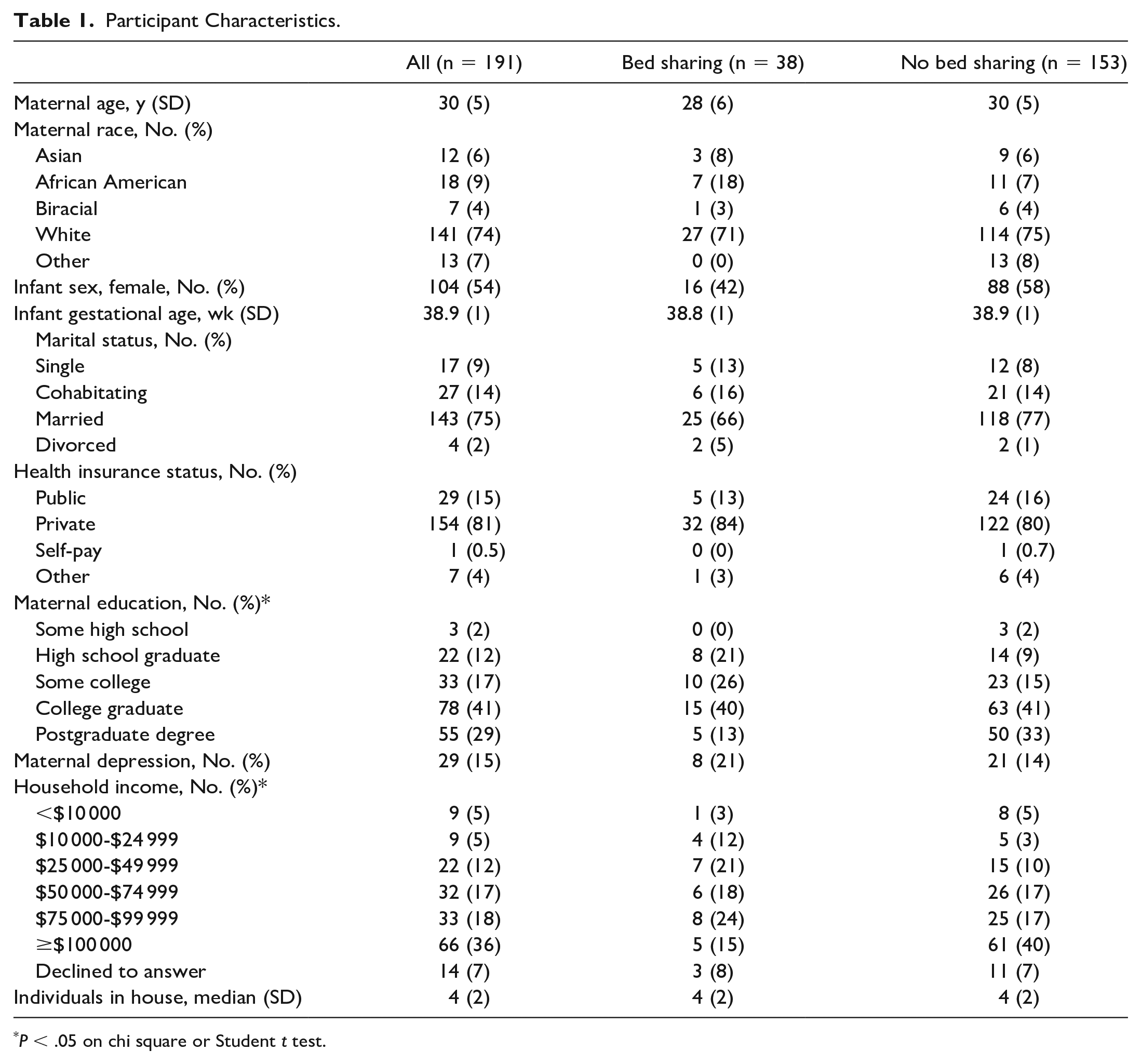
P < .05 on chi square or Student t test.
Sleep Characteristics
At 1 month of age, infants who went on to bed share slept fewer hours at night (7.1 ± 1.7 hours, P = .001, d = −0.79) and took longer to fall asleep (0.7 ± 0.6 hours, P = .021, d = 0.43) than infants who did not bed share (8.3 ± 1.5 hours and 0.5 ± 0.5 hours, respectively) (Figure 1). At 1 month of age, there was no difference between groups in the total time awake at night (P = .46) and the number of parents reporting their child’s sleep to be a problem (P = .12).
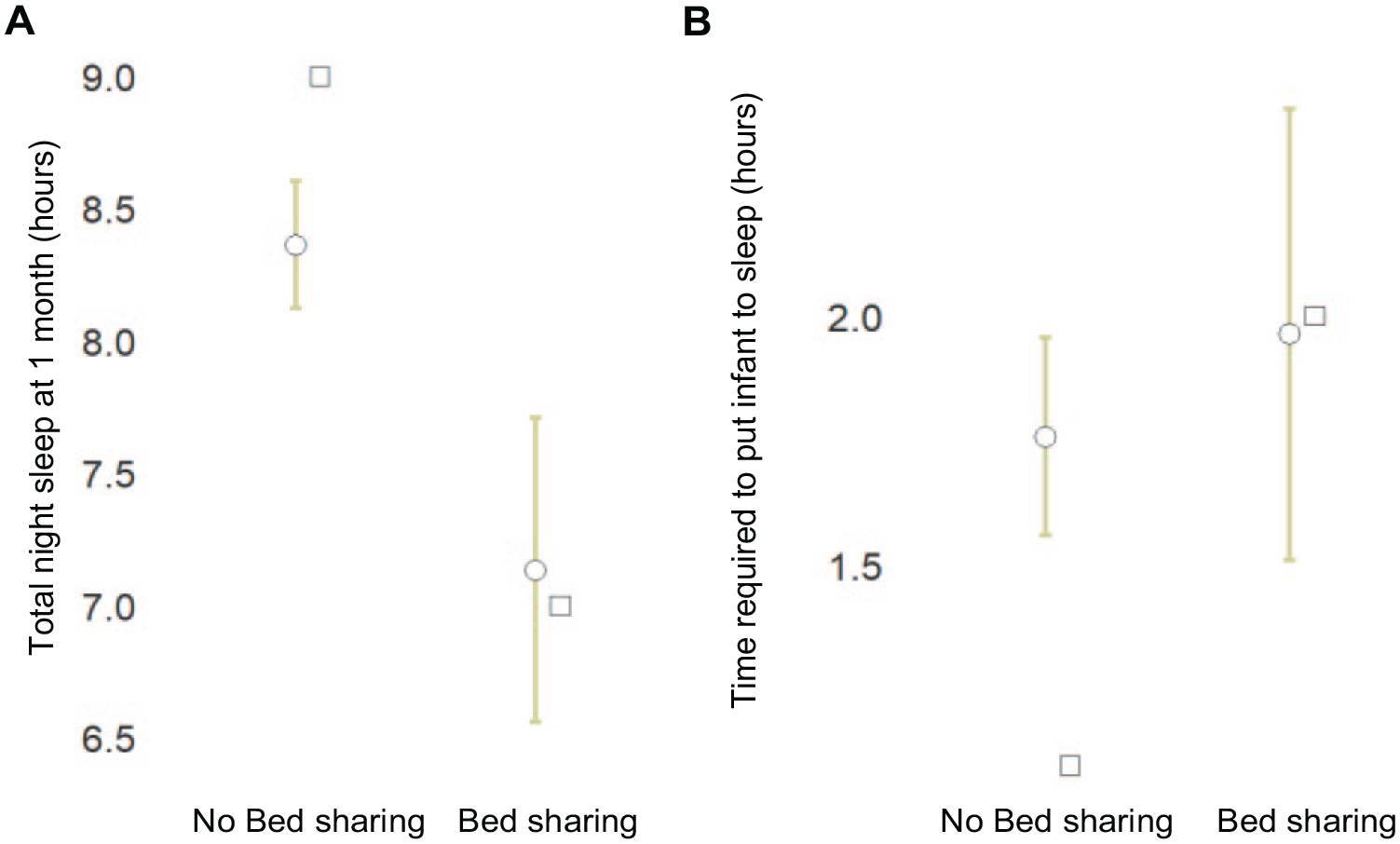
Infants who bed share in the first year take longer to fall asleep and sleep less at 1 month of age. Whisker plots display the
Risk Factors for Bed Sharing
A binomial regression analysis determined that total hours of night sleep (X2 = 10.71, P = .001) and total time required to put infant to sleep (X2 = 3.95, P = .047) influenced bed sharing, while controlling for family income (X2 = 9.08, P = .247) and maternal education level (X2 = 5.81, P = .214). The model accounted for 20.8% of the variance between groups (P = .0001, X2 = 36.8), differentiating infants who went on to bed share with 91% sensitivity, 52% specificity, and an AUC of 0.82.
Discussion
This study shows that infants with increased sleep latency and decreased sleep duration at 1 month are more likely to bed share in the first 12 months. These quantifiable risk factors are associated with bed sharing regardless of SDOH. Interestingly, very few mothers reported their infant’s sleep to be a subjective problem, and there was no association of perceived sleep problems with bed sharing. This specific information that (1) trouble falling asleep and (2) fewer hours spent asleep at night are associated with increased bed sharing, regardless of mother’s perceived sleep problems, can help to guide conversations and interventions to decrease rates of bed sharing.
Bed sharing is a known risk for infant sleep-related deaths. This is particularly true when additional risks are present, including infant age less than 12 weeks, presence of bulky bedding, maternal smoking, and maternal alcohol use.8,9 Bed sharing remains a common practice despite its association with accidental suffocation or strangulation from entrapment, wedging, overlay, or other mechanisms of asphyxia. Adherence to strict avoidance of bed sharing is challenging for many reasons and is a controversial topic in the literature. 5 Parents may intentionally choose to bed share when no alternate safe sleeping space such as a bassinet or crib is available, for cultural reasons, for breastfeeding purposes, or for safety of the infant.10-13 Unintentional bed sharing may occur as parents and infants fall asleep with feedings or comforting and settling.10,11,13 Transitions from separate sleep surface to bed sharing may occur as an attempt to improve parent and infant sleep.6,7 In addition, there is a positive correlation between sleep loss and risk-taking behaviors with people more likely to choose short-term gains over long-term consequences. 14
Results from this study demonstrating sleep difficulties as a risk for bed sharing are consistent with other studies’ findings. 5 Our study expands this knowledge to show specific sleep difficulties that increase the risk of bed sharing. Conversations related to sleep difficulties for infants at early well visits at the primary care office, such as the newborn, 1-month, and 2-month visits, can prepare parents for sleep difficulties and bed sharing risks. Information can be learned from parents regarding intentional and unintentional bed sharing behaviors that develop in response to sleep difficulties. Parent and patient-centered strategies can be discussed to reduce bed sharing when infant sleep is a challenge. Strategies can include small process changes to reduce maladaptive behaviors and may differ from patient to patient. In some situations, advice related to bedtime routines and other improved sleep hygiene practices could also have effects on reduced bed sharing. 15
Our findings suggest that infants with quantifiable sleep difficulties may not be perceived as problematic by the mother; therefore, sleep concerns may not be routinely shared at office visits. It is common to ask parents about sleep at early infant visits. The results of this study suggest that bed sharing has similar impacts on sleep latency (12 minutes) as nighttime video games 16 and cell phone use in adolescents, 17 both of which are frequent topics of clinical counseling at well visits. In addition, the study shows that bed sharing may reduce total nighttime sleep by 72 minutes per night, a significant reduction (15%) in the total nighttime sleep for healthy infants. 18 Asking more targeted questions related to time spent getting the infant to sleep and total amount of overnight sleep could better inform practitioners how to approach conversations related to safe sleep. These questions may also reveal details related to second sleep practices which have been shown to change from safe to unsafe. 7
Strengths of our study include a moderate-to-large sample size and longitudinal data collection, which reduces recall bias. Information related to sleep was obtained using the BISQ, a standardized tool, improving the validity and reliability of our results. Our study also collected a variety of important SDOH, allowing us to control for these important factors.
Limitations of our study include cohort characteristics. Most of our participants identified as white, had a college or postgraduate degree, were married, and had private health insurance, potentially decreasing the generalizability of our results. Only term infants whose mothers intended to breastfeed for at least 4 months were included in the study. A commonly cited reason for bed sharing is ease of breastfeeding; therefore, it is unclear how bed sharing results could have differed if mother-infant dyads who did not breastfeed were included. Our primary outcome of bed sharing relies on subjective parent reports instead of video-recorded sleep patterns possibly leading to reporting bias. In addition, some infants in our study (16/191) were already bed sharing at 1 month, so sleep patterns at 1 month may not be early enough to predict future unsafe sleep in all infants.
Conclusion
Despite efforts over the last 20 years, only a minimal decline in sleep-related infant deaths has occurred. Sleep difficulties related to increased sleep latency and decreased sleep duration are associated with increased rates of bed sharing, a known risk factor for sleep-related infant deaths, regardless of whether mothers perceive sleep to be a problem. With this information, primary care clinicians can make a difference. Implementing more specific questions about sleep parameters may help clinicians identify bed sharing and provide an opportunity to discuss safe sleep practices.
Author Contributions
BAM, CNI, and SDH all contributed to conception and design, interpretation, drafting and critically revising the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy. SDH contributed to acquisition and analysis of the data.
Footnotes
Acknowledgements
We thank Alle Confair for assistance with recruitment and data collection. We thank Desirae Chandran for assistance with data organization. We thank the mothers and infants who participated in this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SDH is a clinical advisory board member for Spectrum Solutions and Chief Medical Officer for Quadrant Biosciences, neither of which played a role in this research. The other authors declare no relevant conflicts of interest related to this research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Gerber Foundation to SDH (#5295).
Ethical Approval
This study was approved by the Independent Review Board at the Penn State College of Medicine (STUDY00008657). Written informed consent was obtained from all participants at the time of enrollment. The study was registered on clinicaltrials.gov (NCT04017520).