
Abstract

Educational Objectives
Recognize the microbiological differential diagnosis of empyema necessitans, a clinical entity in which an empyema extends out of the pleural space and into the chest wall, producing infection and concomitant swelling in the surrounding soft tissues.
Be aware of the immunomodulatory effects of acute SARS-CoV-2 disease that have been recognized during the COVID pandemic, and the potential role of such virally-induced immune modulation in predisposing children to severe infections with the endemic mycoses.
Case Report
A previously healthy 15-year-old boy presented to the emergency department with a 1-week history of an expanding, tender chest mass near the upper left sternal border and 1 to 2 days of mild, dry cough. He had a recent household exposure to family members with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. He had received his usual childhood vaccines and 2 SARS-CoV-2 mRNA vaccines.
On examination, he was afebrile with normal vital signs. His oral dentition was noted to be poor, with extensive dental caries present, particularly prominent in the posterior mandibular and maxillary molars. His breath sounds were diminished over the left hemithorax. A chest wall mass was noted over the anterior left chest with a raised area of induration that had a diameter of approximately 5 cm. The mass was firm and rubbery in consistency, but without frank fluctuance. In addition to a positive SARS-CoV-2 polymerase chain reaction (PCR) nasal swab, a leukocytosis of 14.3 e3/mL was noted. The differential leukocyte count demonstrated 71% neutrophils; 16% lymphocytes (absolute lymphocyte count, 2.28 e3/mL); 11% monocytes; and 1% eosinophils. His C-reactive protein (CRP) was elevated at a level of 74.9 mg/dL. The erythrocyte sedimentation rate was 64 mm/h (normal range, 0-15 mm/h). Computed tomography (CT) imaging showed a dense consolidation in the left upper lobe extending into the pleural cavity and the chest wall, with 2 well-defined intramuscular pectoralis major abscesses identified both by chest radiograph (Figure 1A) and by chest CT (Figure 1B, C).
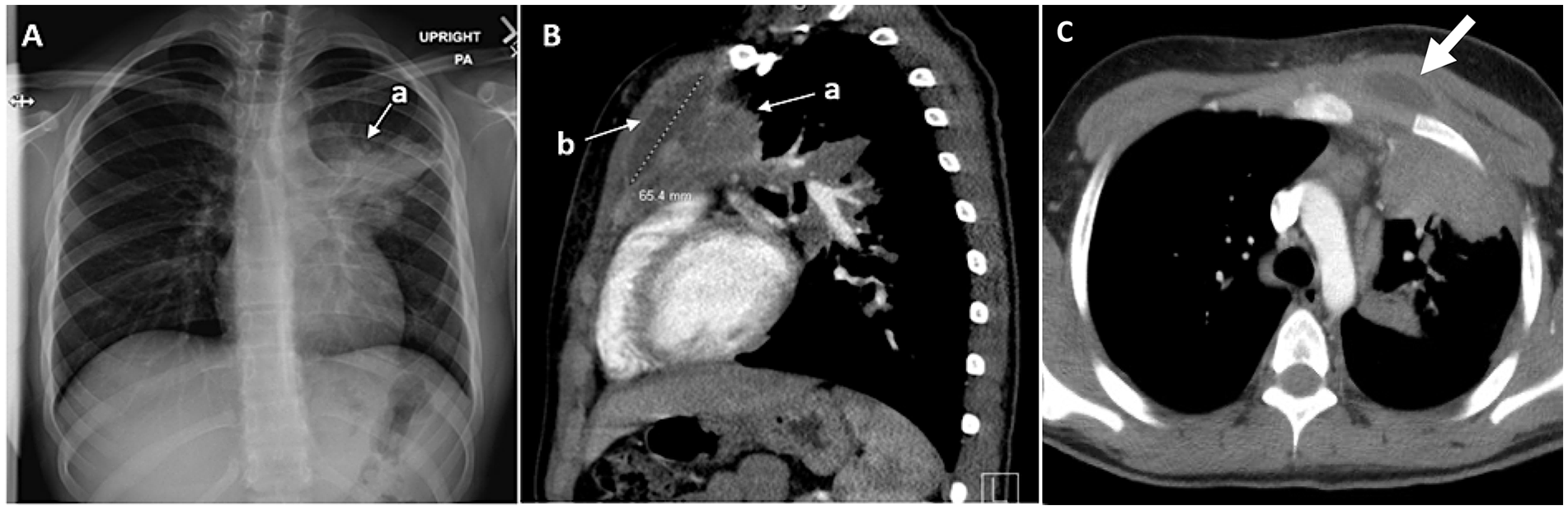
Radiographic findings in patient with empyema necessitans secondary to Blastomyces gilchristii infection. (A) Dense consolidation in the left upper lobe noted on chest radiograph (arrow, a). Right-ward deviation of trachea is noted. (B) Demonstration of transpleural extension of disease (arrow, a) with a well-defined intramuscular pectoralis major abscess noted by CT scan (sagittal view; arrow, b). (C) Transverse CT view similarly demonstrates pectoralis major abscess with extension of infection into chest wall (arrow).
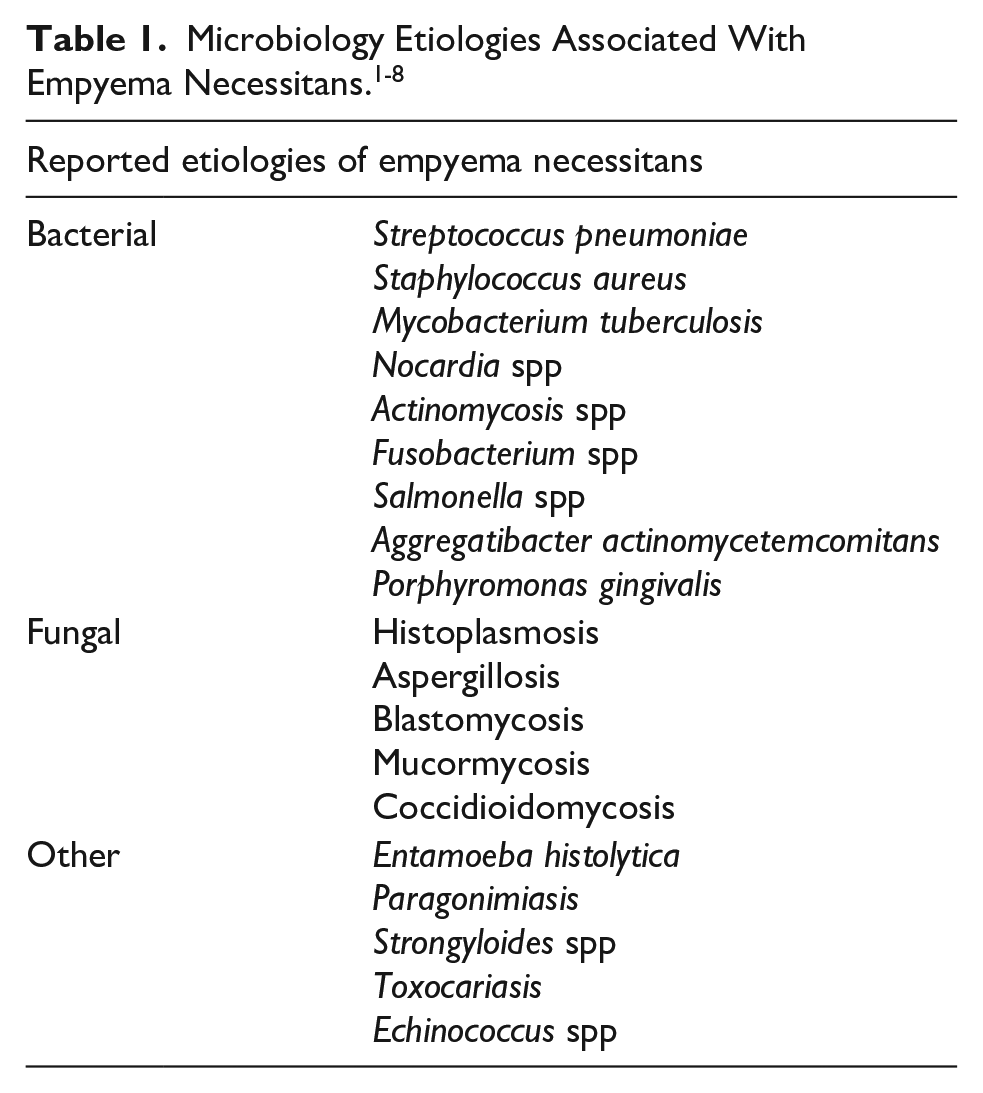
Infectious diseases consultation was obtained. His medical history indicated no previous hospitalizations, no history of unusual infections, and no family history of primary immunodeficiencies. Additional history revealed that breeding colonies of turtles and several snakes were present in the household, although the patient had minimal exposure to these reptiles. There were also 2 fish, 2 dogs and 1 cat in the household. Based on the imaging and physical examination findings, a diagnosis of empyema necessitans was made. In light of his history of household exposure to reptiles and the finding of poor oral dentition on examination, initially a broad differential diagnosis was considered (Table 1).
Discussion
Hospital Course
The infectious diseases consultative service offered the opinion that the patient had pneumonia and accompanying parapneumonic effusion that had progressed to frank empyema necessitans. Surgical intervention was recommended. After consultation with the pediatric surgery service, the decision was made to drain the chest wall abscess under the guidance of the interventional radiology service. A 10F left upper anterior chest wall subcutaneous drain was placed, concomitant with drainage of ~20 mL of thick, purulent, white fluid. No organisms were identified by the gram stain, and he was treated empirically with ceftriaxone. Flow cytometry analysis of the fluid revealed a preponderance of T cells, with no evidence of aberrant immunophenotype. Cytology demonstrated no evidence for malignant cells, with Grocott methenamine silver and Periodic acid-Schiff stains positive for budding yeast forms. Fungal antigen and antibody tests recommended by the infectious disease consultation service were positive for Blastomycosis dermatitidis. The urine antigen was positive at a level of 1.44 ng/mL, and the serum antigen was positive at a value of 0.22 ng/mL. Serum antibody studies demonstrated a positive enzyme immunoassay (EIA) test, with an index value of 8.1. Immunodiffusion and serum precipitin antibodies for B dermatitidis were also positive. Upon further questioning, the patient was noted to have gone camping in the woods in the Detroit Lakes region of Minnesota during the summer months. Approximately 2 weeks after collection, a fungal culture of abscess fluid was reported positive for a Blastomyces species. Subsequent DNA sequence analysis of this isolate, performed at the Centers for Disease Control and Prevention, demonstrated that his infection was due to an organism highly related to B dermatitidis, specifically, Blastomyces gilchristii. 9
After commencement of antifungal therapy, the patient’s symptoms improved. Additionally, immunological studies were recommended by the infectious diseases consultative service but were declined by the primary care hospitalist team. Although amphotericin B therapy is recommended by the Infectious Diseases Society of America for “severe or moderately severe disease” due to blastomycosis, 10 with his limited symptoms, the primary care team elected, after consultation with the family, to discharge the patient on oral itraconazole therapy. A therapeutic level of itraconazole (trough level, 1.4 mg/mL) was documented on outpatient follow-up. Following 6 months of therapy, the patient was asymptomatic, and there was no evidence on physical examination of chest wall swelling.
Discussion of Case and Relevant Literature
The patient described in this report presented with empyema necessitans (also known as empyema necessitatis), a rare complication of pulmonary/pleural space infections in which infected fluid dissects spontaneously from the pleural cavity into the contiguous chest wall soft tissue space. Although first described in the mid-nineteenth century, 11 it has been less commonly encountered in the post-antibiotic era. Empyema necessitans usually presents as a chest wall mass, although infection may extend into the flank, groin, or thigh. 1 The infectious etiology most classically associated with this diagnosis is Mycobacterium tuberculosis, 2 although many pathogens have been described (Table 1).3-7 These etiologies include the endemic mycoses histoplasmosis, blastomycosis, and coccidioidomycosis. 4 Less common etiologies can include parasitic infections such as Paragonimus westermani. 5 Empyema necessitans can also be a complication of poor dental health, including periodontitis. 6 Cases may also be polymicrobial in nature. 7 Patients may manifest disease with fever and severe systemic toxicity, although the evolution and presentation can also be indolent in nature. 7 Surgical debridement and appropriate antimicrobial therapy represent the key elements in the management of empyema necessitans. 8
Of note, the patient described in this report tested positive for COVID-19 at the time of his hospital admission with blastomycosis. We hypothesize that the patient’s serious Blastomyces infection was potentially causally related to his antecedent SARS-CoV-2 infection. 12 It is clear that immunodeficient hosts, including individuals with primary immune deficiency, are also predisposed to fungal infections. Impaired cell-mediated immunity, neutrophil dysfunction, and C3 deficiency are typical inborn errors of immunity (IEI) that can predispose patients to such infections. The patient described in this report had a normal leukocyte count and differential. Other studies, such as quantitative serum immunoglobulin levels, lymphocyte phenotype analyses, evaluation of lymphocyte proliferative responses to phytohemagglutinin, neutrophil functional tests, and C3 levels should be considered in the evaluation of a patient with an invasive mycotic infection. Additional immunological studies were suggested in this case, but were deferred by the primary care (hospitalist) team, given the patient’s negative medical history for other serious infections.
In support of the hypothesis that COVID-19 disease may have predisposed this patient to a serious Blastomyces infection, it has become increasingly clear that SARS-CoV-2 infection has a substantial impact on the human immune response. Type 1 interferons have been shown to play a critical role in innate immune responses to COVID-19 disease.13,14 SARS-CoV-2 also directly affects the host immune response, including induction of dysregulation of genes involved in B-cell and T-cell responses15,16 and results in changes in innate immunity, including perturbation of natural killer (NK) cell-mediated activity. 17 There is evidence that, for patients with COVID-19 disease, there is an increased risk of latent tuberculous infection progressing to active tuberculosis (TB). 18 COVID-19 disease is also associated with reactivation of latent cytomegalovirus infection. 19 A striking example of the impact of SARS-CoV-2 on the emergence of secondary fungal infection is the association with severe mucormycosis that was observed in India, during the height of the COVID pandemic. Over 30 000 cases have been reported to date, 20 with approximately 15% attributable mortality due specifically to Mucor infection. Although the intercurrent presence of diabetes and the concomitant use of steroids both contributed substantially to the mucormycosis disease burden, 21 COVID-19-induced T-cell exhaustion was also observed, 22 and this immunomodulatory effect of the SARS-CoV-2 virus likely increased the susceptibility of these patients to experience severe fungal disease with Mucor. A similar enhancement of risk for other fungal infections, triggered by intercurrent SARS-CoV-2 infection, has been noted for histoplasmosis, 23 cryptococcosis, 24 coccidioidomycosis, 25 and, as for the patient described in the current report, blastomycosis. 26
When considering a potential fungal superinfection in a patient with COVID-19 disease, the endemicity of fungal pathogens where the patient lives or has traveled is an important historical clue. In this instance, blastomycosis was an unsurprising finding when the etiology for our patient’s infection was determined. Blastomycosis is a relatively common diagnosis in Minnesota when compared with other states; in fact, Minnesota and Wisconsin account for 75% of all blastomycosis cases reported annually in the United States. 27 Outdoor activities and soil exposure are associated with infection throughout Minnesota, and at least one-third of Minnesotans engaged in in-state recreational activities that acquire this infection are exposed to the pathogen in a location other than their home county. 28 Our patient’s history of a summer camping trip, where he explored wooded areas and engaged in outdoor recreation, was compatible with these known features of blastomycosis epidemiology. We hypothesize that this patient’s Blastomyces infection, which was indolent and subclinical in nature, transformed into an aggressive and invasive infection, with spread to the chest wall, driven by the immunomodulatory effects of his acute COVID-19 infection. It was of interest to note that, upon molecular testing, the causative agent for the patient’s illness was B gilchristii, and not B dermatitidis. The use of whole-genome sequencing and single-nucleotide polymorphism (SNP) analyses to evaluate blastomycosis molecular epidemiology in Minnesota identified B gilchristii as the causative agent in 2 recent outbreak investigations. 29 B gilchristii has a smaller geographic range, encompassing Canada and the northern United States, than does B dermatitidis, which is found throughout the Great Lakes, the Ohio and Mississippi River valleys, and the St. Lawrence River. 29
Final Diagnoses
COVID-19 infection.
Pulmonary and pleural space infection due to blastomycosis, with associated empyema necessitans.
Conclusion
Empyema necessitans was a common complication of pneumonia in the pre-antibiotic era, but the diagnosis is rarely encountered today. This case report highlights a unique presentation of a minimally symptomatic patient with an indolent B gilchristii infection who had an acute and significant clinical deterioration after acquiring COVID-19 infection, with evolution of a fungal pneumonia that extended into his chest wall. We hypothesize that the acute SARS-CoV-2 infection, through dysregulation of host immunity (most likely due to suppression of T-cell responses), contributed to acceleration of his underlying Blastomyces infection. Invasive fungal infections are reported complications of COVID-19 disease, and clinicians should be mindful to consider this association for patients who live in endemic regions.
This case illustrates how the immunomodulatory effects of COVID-19 may facilitate emergence of invasive disease for what would otherwise be a subclinical, endemic infection such as blastomycosis. In addition to the potential contributory effect of intercurrent COVID-19 in this patient, the classic IEI should be considered in such a situation. These usually present in early childhood, but in exceptional cases these do not appear until adolescence or adulthood. The patient with late-onset IEI presents with a mostly healthy childhood and often receives little medical attention. Such atypical cases may be diagnosed by using the European Society for Immunodeficiency criteria. 30 Detailed immunological examination should be considered in such settings, to avoid overlooking underlying immunodeficiency. However, immune deficiency need not be invoked in all instances of blastomycosis, since the ubiquitous and endemic nature of blastomycosis in Minnesota results in many clinically symptomatic cases that occur in immunocompetent individuals. The complication of this endemic mycosis that we describe in this case, empyema necessitans, indicates that blastomycosis should be considered in a child presenting with unexplained chest wall swelling, particularly if an underlying pulmonary/pleural infectious process is present. Diverse etiologies are described, but among the endemic mycoses, blastomycosis is a particularly important causal agent for empyema necessitans to consider in the upper Midwestern United States. Due to climate change, the geographic range of endemic mycoses is expanding in the United States, making it likely that increased numbers of cases of infection with these pathogens will be encountered in the future. 31
Author Contributions
NK and MRS: Conceived of the paper and wrote the first draft of the manuscript. MI: Contributed data and performed data analyses and participated in critical review and editing of the manuscript.
Footnotes
Acknowledgements
We thank the UMN Infectious Diseases Diagnostic Laboratory (Dr Patricia Ferrieri) and the Minnesota Department of Health Public Health Laboratory for assistance in identification of the Blastomyces isolate.
Authors’ Note
This case was originally presented as a poster (unpublished) at the University of Minnesota Department of Pediatrics annual Pediatric Research, Education and Scholarship (“PRESS”) symposium, April 1, 2022 (“First Place” award, resident category).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MDH’s work was supported in part by a cooperative agreement with the Centers for Disease Control and Prevention as part of the Epidemiology and Laboratory Capacity for Infectious Diseases Program (U50/CK000371).
Ethics Statement
The authors gratefully acknowledge the permission of this patient’s family to share the information contained in this case report. Written informed consent for publication of this patient’s information and consent for publication of corresponding images was provided by the patient’s mother. Written assent was also directly provided by the patient described in this case report.
Non-Anonymized Ethical Statement With Ethics Clearance
In addition to written consent provided by the parent and written assent from the patient, who is the subject of this case report, after review with the University of Minnesota Institutional Review Board (IRB), the determination was made that the content of this manuscript did not constitute research and with the documented signed permissions, the determination was further made that this case report submission could be considered successfully endorsed for ethics clearance.