
Abstract
Children are vulnerable to medical errors. Adverse events are leveraged as educational tools in Morbidity and Mortality (M&M) Conference. Traditionally, M&M has brought angst when discussing adverse events. Our goal was to transition M&M to an educational environment highlighting system failures. A survey was created to capture data on satisfaction, education, and system process improvement. Feedback from the surveys led to several changes, including fostering a multidisciplinary forum, prioritizing educational topics, and emphasizing process improvement. In 5 years, satisfaction with M&M Conference has increased by 29%, with an increase by 50% when asked if process improvement issues were addressed adequately, and 100% of faculty incorporate what they learn from M&M into their practice. By developing a hands-on approach to M&M, we have improved satisfaction and focused on education and system process improvement. This design could be used throughout the medical community to improve discussion of adverse events which should improve patient safety.
Introduction
Critically ill children are vulnerable to medical errors and adverse events.1-3 About 50% of adverse events are preventable and are rarely due to individual mistakes but may be due to a series of errors resulting from system breakdowns.4-8
Since the early 20th century, the Morbidity and Mortality (M&M) Conference has been the traditional forum to examine medical errors and adverse outcomes in an attempt to improve surgical practice. In 1983, the Accreditation Council for Graduate Medical Education (ACGME) mandated M&M as a required component of all resident training. 9 This conference has become a key learning forum for both medical and, in particular, surgical specialties over the years; however, the M&M Conference format and the goals are widely varied, from division to division within the same hospital practice. Often, discussion of error focuses on an unexpected adverse outcome instead of events related to processes of care that may have contributed to the error in review.
The traditional M&M forum had a judgmental and punitive environment such that “name/blame/shame/train” was the mantra used for training newly minted physicians.10-13 In the historic model of our M&M Conference at UT Southwestern, for example, we would have the Attending or Fellow involved in the case to present directly to the ICU division. Not only did this process frequently lead to a biased review of the case, it was often perceived as a less-than-constructive discussion and more of a finger-pointing opportunity for the senior faculty.
As a result, our goal was to restructure the Pediatric Critical Care M&M Conference at UT Southwestern Medical Center from a closed, single-discipline discussion of patient deaths (mortalities) to an integrative, multidisciplinary, collaborative, and patient safety-centered forum. Our vision was to develop a conference that would be learner-friendly and have the focus remain on system lapses, which, historically, has contributed to medical errors.14-17
Conference Design and Format
The pediatric intensive care unit (PICU) at UT Southwestern is a 44-bed unit that offers quaternary-level care for children in the Dallas-Fort Worth metropolitan area with approximately 2500 admissions per year. Our daytime staffing model is made up of 3 provider teams, consisting of 1 Attending, 1 Fellow, and 3-4 frontline providers being a mixture of second- and third-year residents and APPs (advanced practice providers.) Our nighttime staffing model is 1 Attending, 1 Fellow, and 3 frontline providers to cover the 3 teams. The PICU is part of a Level 1 trauma center and an Extra Corporeal Membrane Oxygenation (ECMO) Center of Excellence. The M&M Committee discusses all mortalities that occur in this PICU.
The M&M Committee, made up of 7 Attendings with varying levels of experience, 2 senior fellows, and 1 PICU APP, performed gap analysis through several brainstorming sessions to evaluate the existing M&M Conference. Through annual PDSA (Plan Do Study Act) cycles, interventions were implemented to restructure the M&M Conference. Our goal was to create a safe and nonjudgmental environment and to prioritize interventions accordingly.
The first task for the Committee was to solidify a mission statement for the Conference. The Committee adopted the following mission statement: “A monthly, inter-disciplinary forum to engage in objective, non-judgmental review of adverse outcomes and seek opportunities for systematic process change. We seek to identify areas for improvement and promote professionalism, ethical integrity, and transparency in the inquiry process.”
The Committee now focuses on instituting an efficient, but effective process, which is transparent and will ensure ongoing feedback to the Division. Described below are some of the initiatives that the Committee has already instituted to streamline the process.
Case selection
Figure 1 illustrates the process that is followed beginning with data generation and ending with the case presentation in the Conference.
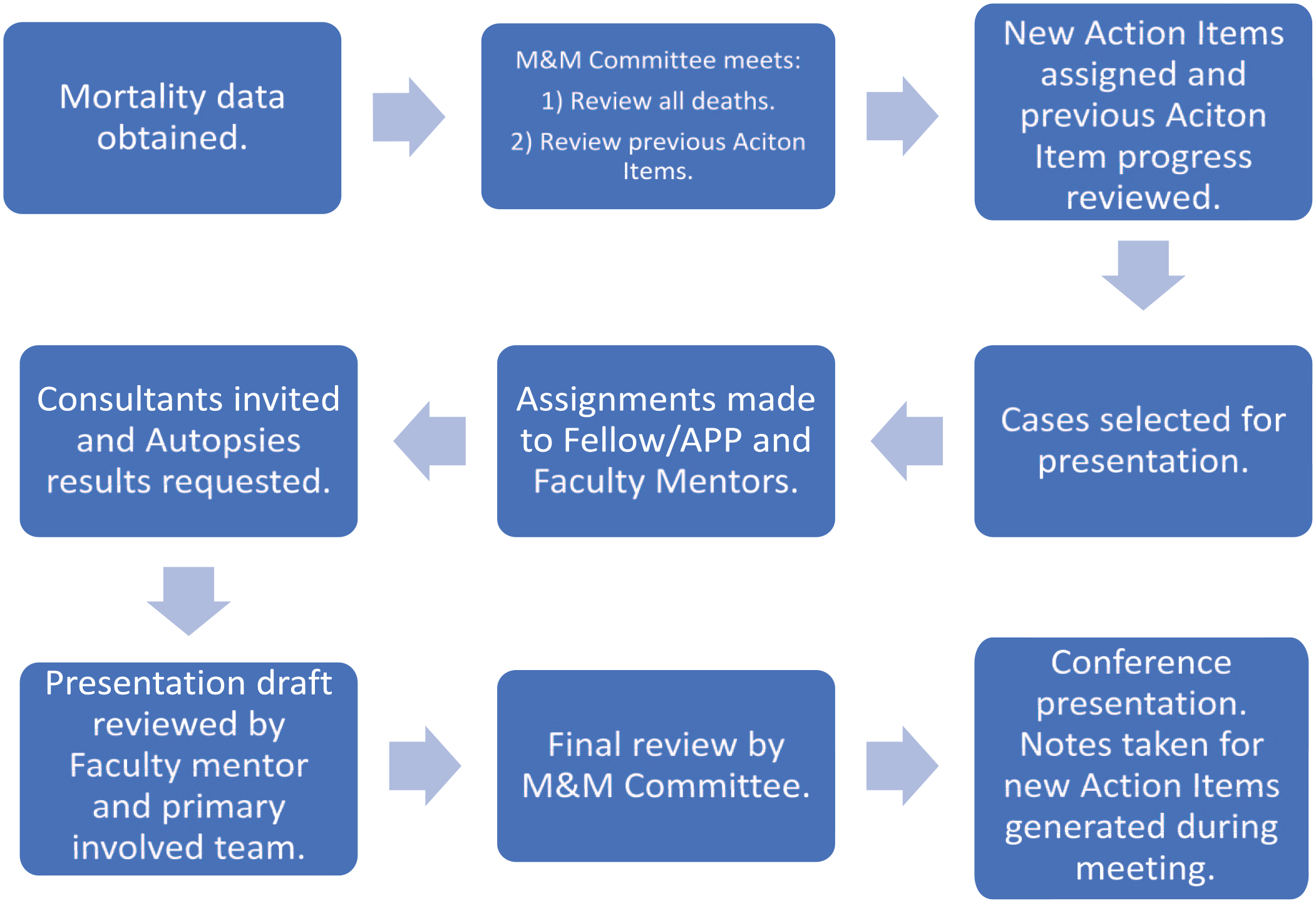
M&M: from idea to conference.
The M&M Committee reviews all mortalities from the previous month and decides which cases should be formally discussed in the Conference. Cases are chosen for discussion if they are found to be educational, concerns about clinical management arise, a system problem is identified, and/or if the family has elected to have an autopsy performed. Cases are then assigned to a Fellow or APP and an Attending who did not participate in the care of that child, to review and present at the Conference. The Fellow or APP prepares and presents the case, and the Attending serves as the faculty mentor to aid in preparing for the presentation. Assigning an uninvolved party helps to limit bias in case review and presentation. The case assignments are tasked 1 month in advance to ensure the presenting team of the Fellow and Attending has ample time for a thorough review. The reviewing team is expected to interview the involved primary Attending and Fellow with the goal of understanding the sequence of events and gaining perspective on the care plan and the mortality. The interviews have a goal to enhance the representation of the terminal events that may not be captured in the medical record. Once the case is prepared, the presentation is sent back to the primary team and the M&M Committee for final review prior to presentation at the Conference.
Case designation
Cases are stratified to be presented into 3 categories: (1) Expedited, (2) Standard, and (3) Case-of-the-month, depending on the complexity or identification of system breakdown issues or an opportunity for learning. To ensure consistency in the presentations, we encourage the use of custom-templated slide decks which are provided to the presenting Fellow or APP at the time of the assignment. Expedited cases are short and presented in 1 to 2 slides highlighting a minor educational opportunity with discussion limited to 5 to 10 minutes. Standard cases highlight a more significant educational topic or process issue and have a longer discussion time ranging from 10 to 15 minutes. Standard cases frequently involve patients who have had a more complicated course/longer ICU stay. Complex cases wherein the Committee identifies either system-wide lapses, need for significant process improvement, or major education lapses, are designated as the Case(s) of the Month. These presentations include a fishbone diagram and a process map to better dissect the case and highlight opportunities. Cases are allotted 30 minutes for discussion.
Case preparation: meeting the educational objective
Reviewing mortalities during the Committee meeting, we identify educational topics to be highlighted and discussed. Topics are chosen based on whether new literature exists, a recent update in practice or policy change has been made, treatment of a rare disease is captured, or performance of a high-risk/low-frequency procedure occurred. The presenting team is asked to review the literature, contact outside institutions when relevant, and invite guest speakers for certain topics. During the prior months, sample educational points reviewed in the forum were as follows:
Risk of venous thromboembolism in patients with sickle cell trait and hyperosmolar hyperglycemic syndrome.
Ventricular tachycardia in the setting of Acetaminophen overdose.
Bleeding risk and management of bleeding while on ECMO.
Conference participation
In cases with multispecialty involvement, the involved subspecialists are invited to the Conference to provide insight into the case. For example, the General Surgery team, which works closely with us in cannulating and managing ECMO patients, is invited to the M&M forum when there is presentation of such a patient. We also encourage the Fellow and Attending reviewing the case to contact the subspecialists for feedback or input when assembling the case presentation. The invitees are asked to contribute to the formal slide presentation with educational literature and/or practice guidelines in addition to the discussion during the conference.
Moderator for M&M conference
We incorporate a facilitator/moderator for each M&M conference. This person engages and encourages the audience to participate in a blame-free constructive discussion. The moderator is provided case reviews and reviews each case prior to the conference. The moderator helps reframe clinical questions when needed and redirects the discussion when necessary to ensure that the time limit allotted for each case is respected.
Postconference review
During the monthly M&M Conference, any system-based issues identified are generated into Action Items. These items are then assigned to different Committee members to follow up and address outstanding concerns. We review the Action Items with the Pediatric Critical Care Division quarterly, meeting our goal of transparency and maintaining division-wide engagement in the quality improvement initiatives. The following are examples of the process improvements that have been identified and implemented over the past 5 years:
Establishment of an antibiotic task force, led by an intensivist, to improve the timeliness of administration of antibiotics in the PICU in patients with severe sepsis (goal to decrease the amount of time between ordering and administering antibiotics.)
Formalized NICU-PICU workgroup to streamline the transfer of patients from the NICU to the PICU.
Provided access to the restricted drug, K-Centra (Human Prothrombin Complex Concentrate), for intensivists and trauma surgeons in patients requiring the massive transfusion protocol. Previously, this drug was restricted to ordering solely by hematologists and such protocol caused a delay in procuring it for patients in the PICU needing it emergently.
Insight from pediatric critical care division
In addition to restructuring the conference, our goal was to improve engagement and participation from the Division. To create a safe and respectful environment, we needed input from all stakeholders. We actively sought insight from the entire Critical Care Division on strategies to improve our M&M Conference.
To gather feedback, annual surveys were distributed over 5 academic years with 4 specific aims:
Measure participant satisfaction.
Measure the perception of M&M as a safe environment.
Measure the perception of M&M as a learning environment.
Assess opportunity for new process changes.
Survey-monkey platform was used for the distribution of the surveys to preserve anonymity and to facilitate honest feedback.
Annual Survey Results and Implementations
We deployed a web-based annual survey questionnaire, created using a modified Delphi technique, where multiple members of the Committee served as the surveyed experts. The questionnaire was not tested for reliability or generalizability, but content validity was derived from the method of creation using the modified Delphi technique. 18
Over 5 years, our survey response rate was between 72% and 91%. Figure 2A-C illustrates the improvement seen in the Conference over the past several years.
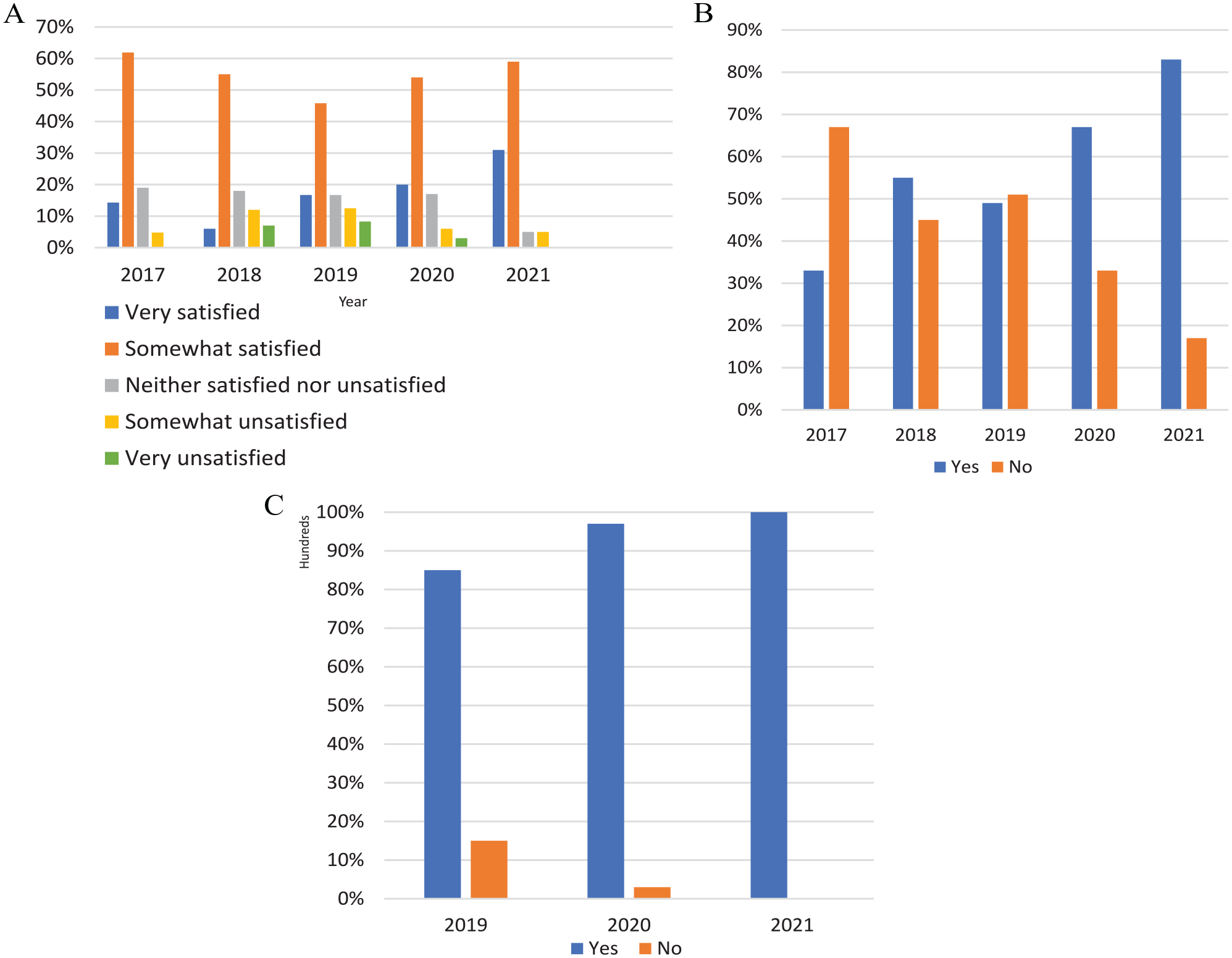
(A) Satisfaction with M&M Conference 2017-2021. (B) Process improvement has been adequately addressed through this forum 2017-2021. (C) Incorporation of what is learned in M&M into clinical practice 2019-2021.
The results demonstrate improvements in satisfaction, process improvement, and education. The degree of satisfaction with the Conference within the Division has improved from 61% to 90% as measured on a 5-point Likert-type scale. On the same Likert-type scale, those within the Division who are very satisfied with the Conference have increased from 14% to 31% over the past 5 years (Figure 2a). A noteworthy trend was seen to the inquiry regarding process improvement initiatives being addressed in this Conference, increasing from 33% to 83% (Figure 2b). In the last 3 years of survey responses, some questions were altered to address new concerning issues. When asked whether Faculty and Fellows incorporate what they have learned in M&M into their clinical practice, there has been an increase from 81% to 100% (Figure 2c).
Each survey had a space for the Divisional members to put any additional comments and provide suggestions for improvement. These comments were used as tools to put into place initiatives to enhance and restructure the Conference. Based on the annual survey feedback received thus far, the following initiatives have been incorporated into our M&M process.
Stringent Case Selection
Historically, every death was reviewed in the Conference. Survey comments revealed that cases were being presented when there was no opportunity for improvement creating less time to devote to cases where there was opportunity for improvement or education. To provide more time for discussion of complex cases of the month and truly elucidate the Action Items that would facilitate process improvement, the Committee identified certain exclusion criteria for case presentation. Specifically, if any mortality meets 2 of the 4 criteria, it was excluded from presentation in the Conference. The criteria include the following:
Admitted to ICU moribund with very low chance of survival.
Death within 48 hours (or first brain death exam within this period) of ICU admission.
Limited teaching or educational opportunities.
No nursing/ethical issues regarding the patient’s care.
Although these cases are excluded from being presented to the Division, the cases still receive M&M Committee review. An email is sent to the providers involved in the case to ensure there were no concerns from the case that provider(s) felt warranted discussion in the Division-wide meeting.
Ethical approval/patient consent
Our study did not require ethical board approval as this did not involve direct patient care.
Multidisciplinary Forum—Efforts to Increase Organizational Collaboration and Unit Teamwork
The involved subspecialists are notified that one of their patients will be discussed in M&M, and they are provided timely notification of the date, time, and location of the M&M Conference. To encourage attendance, the Conference provides Continuing Medical Education (CME) credits. Also, the Conference is held between 12:00 pm and 1:30 pm which coincides with mid-day breaks to facilitate subspecialists’ attendance between clinics and rounds. In addition, the presentation order is adjusted to accommodate subspecialist schedules. Attendance records indicate that an average of 3 to 5 subspecialists were present in each of the monthly Conferences in 2021, while most of the Conferences in 2018 had no subspecialist.
Based on the feedback received, we restructured the conference to include input from other division M&M meetings and institution committees. We collaborate with the hospital ECMO team leadership to share key discussion points from ECMO Team case reviews as part of M&M presentations. We also invite representation from other hospital committees such as the Quality Department to share pertinent information from event reviews such as RCAs and FMEAs (Failure Mode and Effects Analysis). We also incorporate pertinent information from mortality reviews done by other divisions.
We chose to expand attendance to increase teamwork within the unit. The Conference was opened to representation from our bedside providers. The nursing managers act as the liaisons and seek information from the bedside staff prior to the Conference. During the presentation, the nursing managers are provided dedicated time to express any nursing, respiratory therapist, and/or ancillary staff concerns specific to that case.
Enhance Learning Opportunities
At times, clinical duties preclude Attendings, Fellows, and APPs from attending the Conference and the surveys revealed that these providers were missing out on the educational offerings presented during the meetings. To improve access to educational opportunities, at the end of each month, a compilation of all educational topics and pearls is generated and distributed in a monthly newsletter to the Division. The newsletter is entitled “Lessons Learned” to highlight that the content focuses on educational opportunities (Figure 3). The emphasis is on disseminating and reinforcing high yield educational points and summarizing the case-specific discussions and comments that are shared during the Conference.
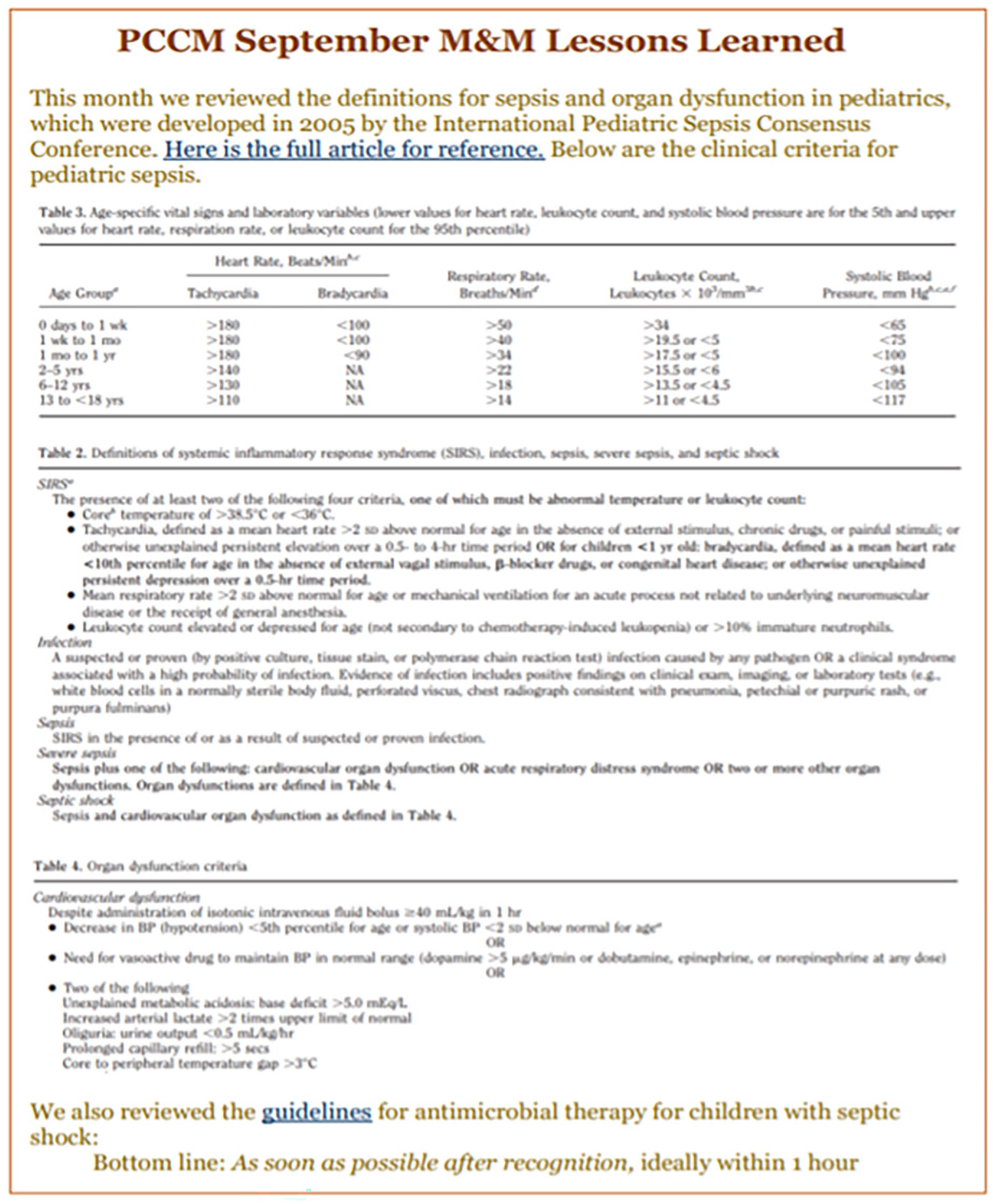
September 2021 “lessons learned” monthly newsletter.
Promote Culture Change by Creating a Safe, Blame-Free Environment
Although it is difficult to change an ingrained culture, we have made a conscious effort to move from a finger-pointing and blame-assigning environment to a safe environment, free from retaliation where the focus is on learning and improving outcomes. Using the survey comments and lessons learned from discussions with colleagues who had been successful in transforming their respective M&M Conferences into open and safe discussion forums, the Committee put into place new practices to adjust conference norms. These adjustments encouraged an open venue for discussion of events. We focused on shifting the culpability from the individual to the system in reviewing and presenting the cases.
The Conference now begins with a slide to remind attendees to “Be Kind, Be Nice and Be Respectful.” We emphasize the confidential and secure nature of the discussion at every Conference to promote a safe learning environment. We promote anonymity by not calling upon the involved team during the Conference. However, if the primary team chooses to voluntarily speak and provide input, they are welcome to do so. One slide in the presentation deck is titled “Primary Team Perspective” and provides the involved team’s thoughts about the terminal events if they are unable to be present or choose not to speak during the presentation. We find that over time, when this slide is presented with increased frequency it prompts more primary team members to speak and share their view of the events contributing to the death in the Conference forum; the feedback is that an avenue for such discussion is cathartic.
The atmosphere of the conference was greatly altered by focusing each case presentation on education. There is great opportunity to learn from medical errors, complications, and unanticipated outcomes if the focus is on educating and not liability or culpability. In fact, the initial surveys revealed there was room for improvement in providing feedback. The Committee responded by soliciting senior faculty to have direct discussions with the medical staff responsible for medical errors. These discussions were candid, yet respectful. Acknowledging that such conversations require practice and finesse, we organized a mandatory communications workshop for providers to improve our ability to provide constructive criticism.
The Committee also believes that culture change starts with buy-in, support, and role modeling from leadership. The Pediatric Critical Care Leadership has embraced these initiatives and is supportive of the Committee’s efforts to transition M&M Conference into an educational and beneficial learning environment for all attendees. The positive response from the Division is demonstrated in the Conference attendance. Our attendance records indicate that in 2018, the average percent of divisional Attendings present was 50%, and in 2021, the average has gone up to 73%.
Action Items and Closing the Feedback Loop
Over the last 5 years, 46 Action Items have been completed. Such Action item categories include, but are not limited to process improvement, education, system-wide change, and practice change. The goal is to continue to incorporate new initiatives each year. As the Division continues to adapt and become more comfortable with the new format of M&M, participants will be willing to offer more suggestions for change.
Morbidity Taskforce
Like many institutions, the M&M Conference has primarily focused efforts on mortalities with little to no attention given to morbidities. With this awareness, the M&M Committee created a subgroup to focus solely on morbidities. To improve recognition of morbidities, our team created a QR code. When scanned, the QR code links to a reporting system to record morbidities. The morbidity taskforce reviews these events and presents themes and relevant events in a quarterly quality conference.
Future Directions
Although, we have seen improvements in our results, we continue to strive for excellence and plan to incorporate the below initiatives in the near future:
Invite a representative from the PICU pharmacists to participate in our committee and open the Conference to attendance by all the PICU pharmacists. This will further enhance the multidisciplinary and collaborative milieu of the Conference forum.
Incorporate input from previous graduated fellows by surveying ex-fellows to ask if they saw improvement or change of their core pediatric critical care knowledge with this change of M&M format throughout the years of their fellowship. We would also like to know if they have incorporated these changes to their current institution if applicable.
Allocate time during the Conference to focus on “Awesome and Amazing” cases. This time would be used to highlight processes and/or outcomes that were successful and excellent. We recognize that there are many opportunities to learn from success and not all learning comes solely from adverse outcomes.
Conclusions
By developing a more hands-on, collaborative, and transparent approach to the M&M process, we have improved overall satisfaction with the M&M Conference and leveraged it as a tool for quality improvement and education at UT Southwestern in the Pediatric Critical Care Department. This newly implemented design could be used throughout the medical community to improve lessons learned through M&M and discussion of adverse events with the goal of improving patient safety.
Author Contributions
All authors have contributed equally.
Footnotes
Acknowledgements
The authors thank the Pediatric Critical Care Division at UT Southwestern and Children’s Medical Center Dallas.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval/Patient Consent
Our study did not require ethical board approval as this did not involve direct patient care.