
Abstract
Since the first case of Severe Acute Respiratory Syndrome Coronavirus-2/Coronavirus Disease 2019 (SARS-COV-2/COVID-19) was discovered in Wuhan, China, it spread to vast limits globally and became a public health disaster, affecting nearly all countries around the globe. Along with mainstream medical treatment, alternative medicine desperately was the need of the hour for youngsters to manage their symptoms while being self-quarantined and ultimately to improve their chances of survival and recovery from COVID-19. Since the beginning of SARS-COV-2, few studies address the clinical-functional presentation of viral infection and management with physiotherapy for children. Major online electronic databases PubMed, PEDro, and Google Scholar were researched to identify, organize and commission the current review. To create a search strategy, Medical Subject Headings and Descriptors of Science and Health were utilized. The authors looked for other studies by screening the references list of the potentially pertinent papers. These computerized searches turned up studies and those studies’ bibliographies with pertinent citations were examined. Personal protective equipment was a crucial component for protection and contact precaution. Following hypoxia, effective oxygen therapy is administered right away. When necessary, under the right circumstances, nasal high-flow oxygen therapy, non-invasive ventilation, lung-protective breathing methods, and prone positioning can be used. Children with SARS-CoV-2/COVID-19 may benefit from physiotherapy interventions with a focus on ventilatory management, airway clearance procedures, early activities, and mobilization.
Introduction
The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-COV-2) outbreak began in late December 2019 in the Chinese city of Wuhan and within a short period it spread to the rest nation. 1 Following the identification of the pathogens using whole-genome sequencing, the WHO classified the SARS-COV-2 as a new beta coronavirus genus and the disease was given the name new coronavirus pneumonia. 2 The coronavirus causing Coronavirus Disease 2019 (COVID-19) affects multiple systems including the cardiovascular system, in addition to the respiratory system. Individuals with a history of heart failure and coronary artery disease became more susceptible to developing decompensation following COVID-19. 3
COVID-19 has capable efficiency of impairing breathing by causing structural deficiencies in the respiratory system. 4 Additionally, depending on the clinical severity displayed, there may be reduced exercise tolerance and respiratory muscle function. 5 Limitations that make it challenging to conduct everyday chores that need the ability to move, including walking and performing self-transfers. 6 According to studies acute myocarditis and severe acute respiratory syndrome (SARS) have also been linked to myocardial infarction and systolic dysfunction. 7
Physiotherapists (PT) walk hand in hand with other specialists involved in the patient’s physical recovery from COVID-19 not because they treat illness but rather because PT prevents and optimizes respiratory inadequacies and reduced functional restrictions following everyday activities. 8 PTs are responsible for providing care for these patients as it is important to comprehend the functional effects of COVID-19 to determine the appropriate course of action. 9 Since, the first pediatric COVID-19 case report was documented in Shenzhen, China, on January 20, 2020, following which several COVID-19 cases have aroused to high limits. 10 The largest review comprised 2143 children, with an average age of 7 who were thought to suffer from COVID-19. Authors noted x731 children (34%) for viral confirmation, 13% for asymptomatic infection, 5% experienced dyspnea or hypoxemia and 0.6% proceeded to acute respiratory syndrome coronavirus 2 (SARS-CoV-2) or multiple organ failure. The symptoms in the remaining minors were modest to moderate. 11
Children who were hospitalized and diagnosed with moderate symptoms did not necessitate admission to the intensive care unit. 12 Children may not have a cough, fever, or shortness of breath. Mild to moderate symptoms are the most commonly reported clinical presentation, although children can also experience severe episodes. 13 Clinical manifestations of SARS-CoV-2 may be more severe in children who have chronic lung diseases such as asthma, cystic fibrosis, congenital heart disease, and immunocompromised (hematological malignancy or solid tumor). 14 It should be noted that while infants with SARS-COVID-2 should be isolated and carefully evaluated, admission to the neonatal intensive care unit is not always necessary. 15 Objective of physiotherapy is health planning promotion among children without COVID-19 clinical symptoms and changes to the chest X-rays. Airway clearance or sputum samples are not appropriate for physiotherapy interventions. The suggested strategies have an educational bent and include telehealth in Physiotherapy and telerehabilitation, which is the delivery of Physiotherapy services over telecommunication networks and the internet. 16 Protection of vulnerable populations, control of infection sources, and blockage of transmission routes: It is advised that isolated children be given their rooms to minimize contact with other residents. 17 There is a significant necessity for cleaning, disinfecting, and ventilation of the rooms where youngsters utilize their personal belongings. 18 We evaluated potential diagnostic and therapeutic strategies for the care of COVID-19 in light of these complications, as well as the solutions suggested by studies to close these gaps. To help public health and policymakers establish strategies to fill the gaps in care for children during the COVID pandemic, we have also attempted to identify research gaps.
Materials and Methods
Inclusion and Exclusion Criteria
A systematic search was conducted in PubMed, PEDro, and Google Scholar databases (last accessed August 19, 2022). We included studies performed on SARS-COV-2 among children along with suggesting chest physiotherapy interventions irrespective of any study designs and their publication status from year December 2019 to August 2022. Studies providing information on SARS-COV-2 patients regardless of gender, ethnicity, and variant of COVID-19 were included in the present review. Original studies in English assessing interventions addressing SARS-COV-2 management in children were only included. Even with resource limitations, authors did not include studies published in other languages and excluded book chapters, book reviews, and letters to the editors. The ethical guidelines were followed while conducting the review.
Information Sources and Search Strategy
In August 2022, a search for information regarding SARS-COV-2 and chest physiotherapy interventions among children was completed. PubMed, Scopus, and PEDro were used to search for relevant articles. Throughout the research and reporting procedures, relevant quality assessment scales were used. The search terms were: “Children AND COVID-19,” Chest Physiotherapy AND COVID-19 “SARS-COV-19 AND Pulmonary Rehabilitation AND Children,” “Children AND Chest Physiotherapy.” The authors looked through bibliographies of researched and reviewed papers and found some relevant items related to the current review. We also talked to specialists in the field to see if there were any other relevant information sources and search strategies. Furthermore, we also screened a reference list of potentially relevant studies to seek additional studies.
Reviewing Procedure
The review of studies was scheduled in two phases. In the first phase, three reviewers (AS, NS, and AC) searched for studies from the database. In the second phase, the retrieved studies were reviewed by two reviewers (AS and NS), initially from the titles, abstracts, and available full texts. Other reviewers also reviewed studies to validate the inclusion of studies. Disagreements, during the selection, were resolved through discussion. Articles, titles, and abstracts were obtained from searches for eligibility against the established inclusion criteria on Population, Intervention, Comparison, Outcomes and Study (PICOS). Investigators discussed inclusion and exclusion criteria frequently over the phone to clarify any concerns and inconsistencies that emerged. Full articles were evaluated for all abstracts that met the initial criteria. Results are compiled in tabular form utilizing thematic analysis and narrative synthesis. After articles were retrieved, we purged duplicate records from the various databases. The downloaded citations’ titles, keywords, and abstracts were scrutinized, and paper copies of those that met our selection criteria were retrieved. Using a data extraction sheet, two reviewers (AS and NS) independently extracted the data. The following summary data were used to extract the data: sample characteristics, such as the purpose, setting, design, intervention, results, and conclusion. Topics were arranged in ascending order by the quantity of research in which they were found.
Data Extraction
In the first phase, reviewer’s extracted data from the included papers, while in the second phase, reviewers double-checked the results. All research point estimates of Randomized Controlled Trials (RCT), Systematic Review, Scoping Review, and Case Reports authors were checked all the point estimates thoroughly. The authors only collected the data from the studies which focus on chest physiotherapy interventions in children during the SARS-COV-2 pandemic. To enable an overall estimate of the available evidence, each conclusion of the study on which a generalized conclusion was founded or extracted.
Data Charting
For summarization and data extraction, we followed Consolidated Criteria for Reporting Qualitative Research. 19 Data from included studies were retrieved and evaluated by two independent investigators. Investigators received training preliminary regarding data entry. Data were then entered into a Microsoft Excel data collecting form that had been pre-designed (Microsoft Corp.). Both investigators discussed extraction categories to resolve any concerns and disagreements that occurred. General information in the context of each study including the author, year of publication, study type, specific study population, study or article location, purpose, and main findings were extracted as recommended by best practice guidelines. The present qualitative review included 2 systematic reviews, 1 case report, 1 scoping review, 2 commentaries, 1 RCT, and 6 descriptive reviews.
Assessment of Risk of Bias and Sensitivity Analysis
Two reviewers (AS and AC) independently evaluated the risk of bias for each trial included in the synthesis using the core risk of bias items from the Cochrane Collaboration. We reached consensus between these authors to settle disagreements. Incomplete outcome data (attrition bias), random sequence generation (selection bias), allocation concealment (selection bias), blinding of outcome assessment (detection bias), and selective reporting were the domains that we evaluated using this instrument (reporting bias). Based on the recommended descriptive judgments, we categorized studies as having a high, uncertain, or low risk of bias for each item. We used sensitivity analyses to test the robustness of the findings in relation to the analysis and design decisions we took in order to get our results. The effects of including or eliminating trials were examined.
Quality Assessment of Studies Included in the Review
Data were extracted from studies meeting inclusion criteria. Methodological quality assessment for Systemic Review was done using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The quality of RCT was estimated by determining adherence to Consolidated Standards Of Reporting Trials (CONSORT) guidelines. The Consensus-based Clinical Case Reporting Guideline (CARE) Checklist was used to determine the relevance of the case report included in the review. All reviewers noted the justification for inclusion or exclusion, and disagreements were discussed and settled by consensus in order to enable comparison of the appraisal processes. We used the assessment to provide comments about the overall quality of the studies that were included for each of these areas. Two reviewers (NA and AS) independently evaluated the papers in two steps, first reading the abstracts and subsequently the entire texts and extracted data, to determine the quality of each study.
Results
Selection of Studies
A total of 1993 potential studies were found in the initial search (1988 from particular databases and 5 from manual searches). A total of 229 identical records were eliminated. We reviewed 1745 titles and abstracts, and 1679 records were excluded because they didn’t fit our inclusion criteria. Of these, 66 were evaluated as full texts. Thirty-three of these studies were eliminated due to incorrect publication type, 13 owing to incorrect study design, 2 because of a wrong outcome, 4 due to incorrect protocol, and 1 because of wrong demographics. Finally, 13 articles ultimately passed the eligibility requirements and were counted in the review. Figure 1 depicts the flowchart of the study selection procedure.
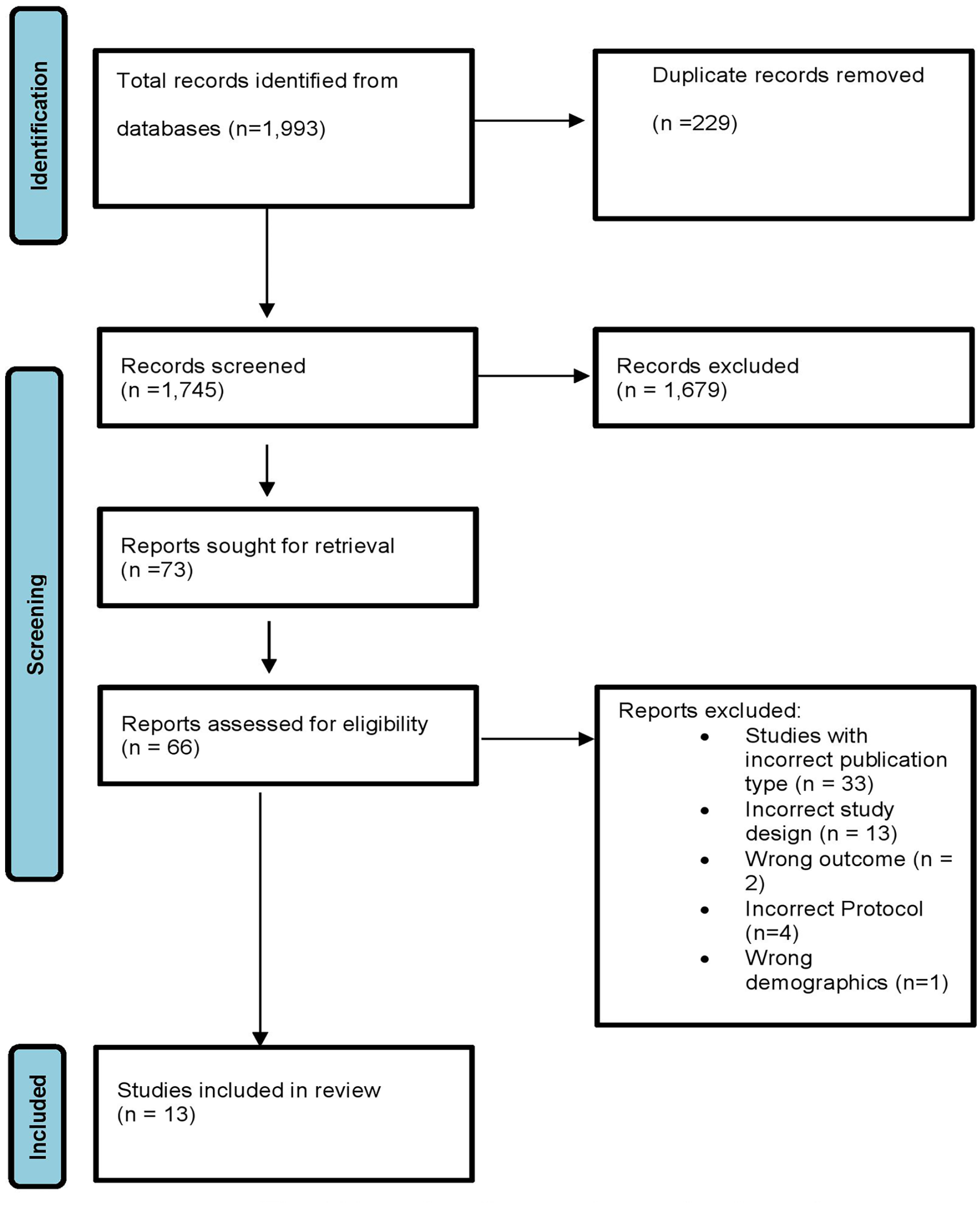
Flowchart for selecting studies for review.
Reporting Risk of Bias
In an Online Resource 2, the risk of bias evaluation is described in depth. We deemed selection bias (selection bias) and random sequence creation to be high risk and ambiguous, respectively. Yet, it may be said that the results measured are objective, which lowers the chance of detection bias. Finally, we thought that reporting bias and attrition represented an unclear risk.
Main Findings of the Articles Included in the Review
Changes in lung function including a decrease in pulmonary compliance and cardiovascular repercussions were seen post-COVID-19. Physiotherapy intervention in managing children was found to be effective in managing chest complications associated with COVID-19. Early physiotherapy and the management of oxygen therapy and ventilatory support (invasive and non-invasive) for these patients were effective in managing symptoms. 20
Early management of children with physiotherapy hospitalized during COVID-19 served as effective and was essential to maintain and recover the functional status of the patients. Manual techniques, aiming at maintaining pulmonary expandability and promoting bronchial hygiene including compression/decompression, prolonged slow expiration (PSE), manual hyperinflation (MH) with self-inflating bag and bag squeezing enhanced recovery time post-COVID-19. 21
Benefits of Early Physiotherapy
Articles report difficulty in access to rehabilitation facilities due to COVID-19 having a deleterious impact on the respiratory condition of medically complex children. In reciprocation, early mobilization, postural drainage, and breathing exercises conducted in the presence of skilled respiratory PT should be included at an early phase and must be adjusted according to the patient’s unique underlying pathophysiology. 22 The potential for including respiratory exercises in home-based rehabilitation programs for 2.5–24-year-old male DMD patients with various disease stages. Asynchronous telerehabilitation techniques, such as the video showing patients with DMD how to perform breathing exercises considering the recent SARS-CoV-2 virus epidemic, this approach has been suggested. 23
The COVID-19 pandemic, which is caused by the SARS-CoV-2, caused a global pandemic that fundamentally changed how long-term care facilities handle infections. Hundreds of people have been infected by COVID-19, whereas other common viral respiratory viruses mostly stopped spreading during their usual seasons. All forms of rehabilitation services saw a considerable decline. Physiotherapy hours per month on average dropped from 134 before COVID to 84 after COVID (p = 0.0027). After COVID, the monthly average for occupational therapy hours dropped from 112 to 64 (p = 0.0016). Despite increased infection control measures and declining rates of viral illnesses, there is a paradoxical rise in the use of respiratory care across several domains in medically complex children residing in pediatric long-term care facilities. This rise may be attributed to increased sedentary behavior brought on by the drop in rehabilitation therapies during the post-COVID period.
CPT Techniques
Findings of a study suggested that physiotherapy had a major role in slowing the progression and assisting in recovery by enhancing the functional status of the pediatric population admitted neonatal intensive care setup post-SARS-COV-2 infection. Supplemental oxygen therapy (1 L/min), when administered along with regular physical therapy sessions (techniques included: compression/decompression, PSE, MH with a self-inflating bag, and bag squeezing), helped maintain sufficient pulmonary expandability, promote bronchial hygiene, and maintain blood gases levels within normal limits. Addition of general mobility exercises apart from chest physiotherapy interventions assisted in early weaning off the ventilator. Also, early incorporation of chest physiotherapy interventions has contributed to an overall decrease in the duration of intensive care unit (ICU) stay among obese children diagnosed with SARS-Cov-2 infection and requiring intensive care and invasive mechanical ventilation. Techniques involving airway clearance, pulmonary expansion, and activities to enhance mobilization (sessions involved passive to resistive exercises during hospitalization) have known to decrease dependency on ventilator and assist patients to walk unsupported at discharge, thereby augmenting recovery and enhancing their functional status.24,25
In a study involving pediatric patients admitted to critical care setup, it was observed that despite vigorous medical treatment using protective pulmonary ventilation, sedation, and neuromuscular blockers, patients admitted to ICU are at high risk of developing muscle weakness, consequently worsening their morbidity and mortality.25,26 The role of physiotherapy interventions with exercises, mobilization, and early rehabilitation is extremely important to promote the recovery of survivors of critical illness associated with COVID-19. Along with chest physiotherapy interventions involving airway clearance and cardio-respiratory maneuvers, it is essential to simultaneously monitor and control drive pressure at values ≤15 cm H2O with plateau pressure limited to 28 cm H2O to avoid new damage to the lung.27-29
The summary of the included studies in the review is shown in Table 1.
Summary of Identified Studies for the Present Qualitative Review.
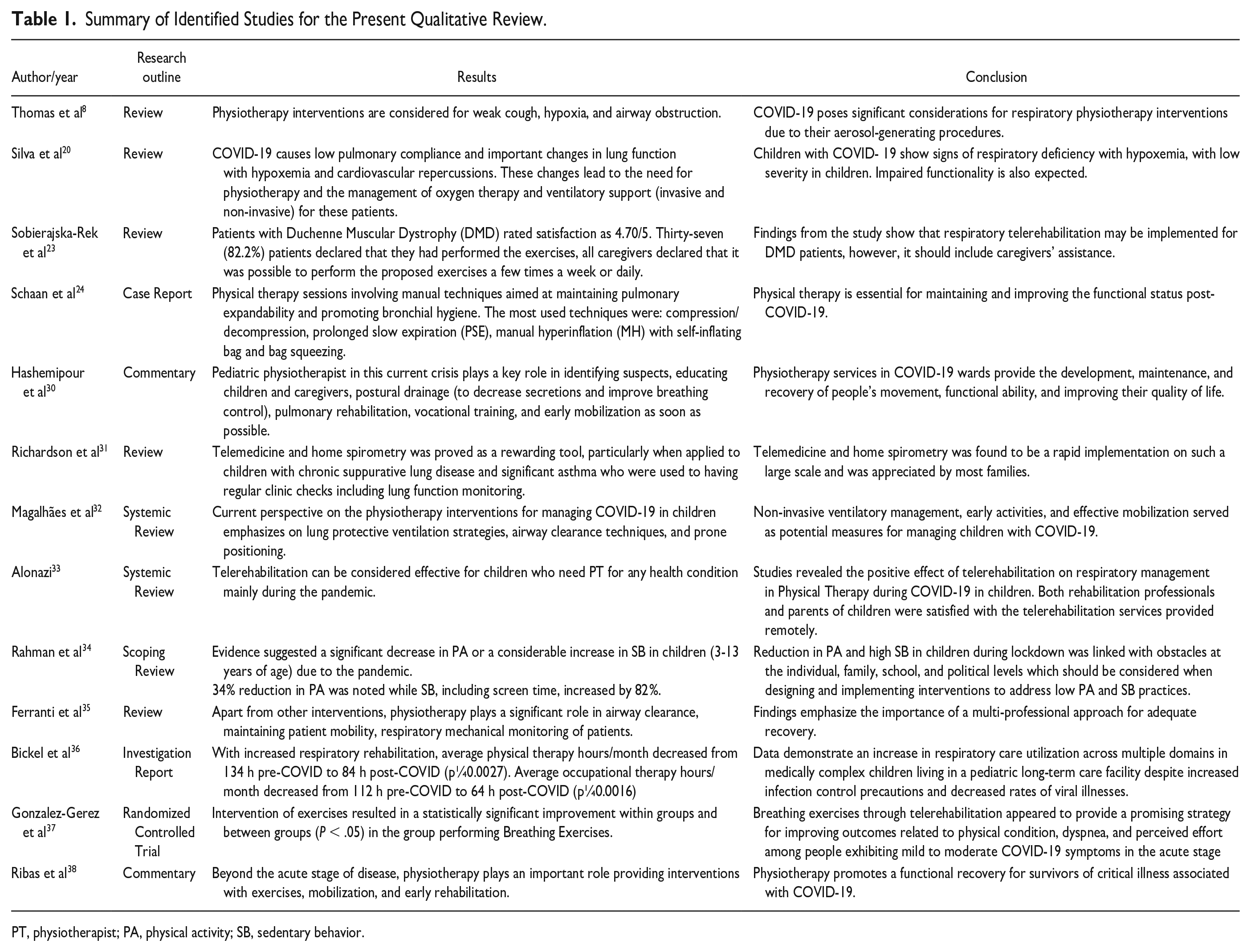
PT, physiotherapist; PA, physical activity; SB, sedentary behavior.
Discussion
Risk of Infection in Children
Children tend not to protect their faces when coughing and sneezing, despite the decreased incidence and severity of the disease in this age group. In addition, they frequently touch their faces and interact physically with their teams and peers. All these factors label children as minimally cautious about healthy behavior. Furthermore, the reopening of schools may potentially serve as a breeding environment for illness. Commonly seen clinical symptoms were myalgia/fatigue (18.7%), cough (55.9%), rhinorrhoea (20%), and fever (59.1%). In contrast to adults, children hardly ever developed severe upper respiratory issues necessitating admission to an intensive care unit. 39 According to studies, variations in path immunological mediators required for viral entry and immune system-mediated responses are likely to cause low-grade lung injury. 40
Assessment and Management of Respiratory Distress in ICU Setup
The Oxygenation Metric (OI) [(OI= MAP × FiO2 × 100/ PaO2)] is an optimum index for classifying the severity of juvenile ARDS in patients receiving invasive mechanical ventilation. The mean airway pressure (MAP), oxygen fraction (FiO2), and partial oxygen pressure in arterial blood are used to calculate the oxygenation index (PaO2). Mild acute respiratory distress syndrome (ARDS), moderate ARDS, and severe ARDS (OI> 16) are the three categories used to describe the severity of lung injury. 41 Aerosol-generating physiological therapeutic techniques such as aspiration of the airways, collection of secretions from the upper airways, assistance during tracheal intubation, and cardiorespiratory arrest maneuvers might be categorized as high risk. It’s crucial to keep in mind that even simple procedures like handling a patient directly for positioning, choosing to extubate, replacing the barrier filters, and adjusting or fixing the tracheal tube carry some danger. 42
In addition, a thorough evaluation of the child’s respiratory condition, and evaluation of physiotherapy for children with COVID-19 should assess the child’s general physical health, including muscle strength, thoracic mobility, overall body mobility, endurance, and general physical activity. Additionally, it is important to thoroughly evaluate the strength and endurance of respiratory muscles, mobility of the musculoskeletal system, state of the bronchi, and breathing pattern. It is emphasized, physiotherapy is not only used to treat a child’s current condition but also for conditions such as malignancies, cardiac conditions, and kidney problems. 43
Children confined to intensive care units are prone to acquired muscular weakness enabling the child’s typically functional limitations to promote physical falls. Herein, the major action of physiotherapy with children is to improve joint range of motion, strength, breathing capacity, and cardiovascular tolerance leading to positive pulmonary functions. 44 Aerosol-generating operations are not only restricted to intubation and suction, in regards, PT should be aware that close contact with a child during activities like positioning, play therapy, and ambulation might also be hazardous. 45
Chest Physiotherapy Measures
Respiratory morphology and function of children and adults change greatly with time, necessitating the administration of respiratory physiotherapy procedures in accordance with one’s age. 46 Techniques like forced expiration, slow and prolonged expiration, increased expiratory flow, total slow expiration with the glottis open in a lateral posture, postural drainage, percussion and vibrations (manual techniques), MH, active cycle of breathing, oscillatory positive expiratory pressure (PEP), autogenic drainage, assisted autogenic drainage, forced drainage, slow and prolonged expiration, oscillatory PEP, instrumental techniques and incentive spirometer are brought to use. 47 Children require specialized physiotherapy intervention strategies based on assessment and reassessment. 48
Insights of CPT Interventions in PICU
In pediatric respiratory diseases, the main goals of Chest Physiotherapy (CPT) are to help in the removal of obstructive tracheobronchial secretions, which reduces airway resistance and improves work of breathing and gaseous exchange; to enable early weaning from the ventilator; to prevent or resolve respiratory complications; to expand collapsed lobes; and to speed up recovery. 49 In order to avoid or reduce the effects of critical sickness and immobility (such as postural abnormalities and muscle deconditioning) and to maximize functional results following Pediatric Intensive Care Unit (PICU), it is crucial to consider the long-term effects of critical pediatric illness or injury. 50
Children who are on a ventilator are at risk of oxygen toxicity, hyperinflation, positional atelectasis and/or consolidation, poor mucociliary clearance, and lower functional residual capacity as a result of laryngeal braking. 51 Airway blockage, infection, atelectasis, and finally chronic lung disease may result from increasing the amount and viscosity of secretions as a result of the ET tubes (foreign body), poor humidification of ventilator gases, and disease processes themselves. Considering the known health consequences of CPT, children who are critically ill, hemodynamically unstable, have pulmonary hemorrhage (either spontaneously or as a result of surfactant therapy), pulmonary edema, coagulation defects, elevated or uncertain intracranial pressure, pulmonary hypertension, and/or a history of hypertensive crises, as well as very premature or small gestational age infants, should all be relative contraindications and precautions to CPT. 52
Breathing Exercises
Deep breathing exercises, PEP therapy, regionalized breathing exercises, the active cycle of breathing technique, rhythmic PEP, and autogenic drainage are a few of the breathing techniques that are occasionally employed in the PICU. Deep breathing exercises have been touted as the most secure, affordable, and efficient approach to keep the lungs enlarged and secretions circulating. 53 Breathing exercises are rarely used in the PICU setting because ventilated children find them challenging to complete, but they might be helpful for older, nonventilated children who are compliant. 54
Mobility Exercises
The stability, age, developmental stage, and general health of the patient should all be taken into consideration while choosing a mobility exercise. The broad term “mobilization” encompasses a variety of actions, including active limb exercises, rolling or turning in bed, sitting in or out of bed on a chair, standing, and walking (with or without assistance). 55 The objectives of mobilization include enhancing thoracic mobility, boosting lung volume, assisting secretion clearance, enhancing exercise capacity, muscular strength, and cardiovascular fitness, preventing postural deformities, enhancing bone ossification, and improving bladder and bowel function, in addition to offering psychological advantages. 56 According to a study, <10% of critically sick children received mobilization treatment, It is obvious that there is an immediate need for thorough, prospective studies on the security and effectiveness of mobility in the PICU in particular. 57
Mild to Moderate Symptoms
For children with upper respiratory tract infections, airway clearance techniques served as a beneficial method to prevent complications arising because of SARS-COV-2. Home therapy involving mobilization and early functional activities in children presenting with mild symptoms during the acute phase of the disease help alleviate the adverse impact of sedentary activities and postures. However, children presenting with mild pneumonia-like features needed close contact Physiotherapy sessions involving chest expansion exercises to clear out the sputum. Active cycle of breathing technique and autogenic drainage patterns were beneficial for adolescents who were able to follow commands. 8
Techniques to facilitate secretion clearance include assisted or stimulated cough maneuvers. Children with severe pneumonia required continuous monitoring for desaturation assisted with vigorous physiotherapy sessions. Supplemental oxygen therapy is required if oxygen saturation levels dropped to <94% at rest.58,59
Physiotherapy in Respiratory Support
For children presenting with critical illness, interventions involving lung recruitment maneuvers were incorporated to generate an increase in transpulmonary pressure and improve the oxygenation index for early rescue in severe ARDS. 1 to 2 h of prone positioning, 3 to 4 times a day is suggested for children with spontaneous breathing. For severe respiratory distress, due to SARS-COV-2, 12 h of prone positioning is indicated. 60
In the treatment of SARS-COV-2 patients, postoperative changes, mobilization, and respiratory physiotherapy play a significant role in recovering from hypoxia and weaning off the patient from a mechanical ventilator. 61 Pediatric patients affected by SARS-COV-2 presented different forms of disease manifestation, and physiotherapy was found to be essential for maintaining and improving the functional status along with other treatment interventions. Play therapy in children is one of the main roles of physiotherapy for children admitted to intensive care units. Prolonged immobility makes children prone to muscle weakness. Activities aimed to increase the range of motions in the joints, strength, breathing capacity, and cardiovascular tolerance during work out resulted in favorable pulmonary function. 30 Home-based spirometry had a positive impact on the respiratory function following the acute phase of the SARS-COV-2 in children presenting with mild dysfunction. 31
In children with SARS-COV-2 infection, especially after discharge, chest physiotherapy is a significant adjuvant therapy for enhancing respiratory functioning and quality of life. Apart from a few expert suggestions based on anecdotal evidence, there is still a paucity of evidence about its efficacy during the acute stage. Chest physiotherapy, on the other hand, is an individual treatment based on the patient’s unique presentations. As a result, when patients have symptoms that can be helped by chest physiotherapy, it may be administered while the patients are being constantly monitored for potential negative side effects. Additionally, precautions including the use of surgical masks, if available, should be followed when providing chest physiotherapy to patients who are in the acute stage to prevent cross-infection.
Strength and Limitations
The main strength of this present review is that the search process was carried out through major databases. However, interpretations of the findings were made considering several limitations. First, there was a lack of evidence present that directly deals with children with SARS-COV-2 and chest physiotherapy. The information regarding the settings is substantially different among them. So, this fact hampers the generalization and comparisons of the current situation from that examined in the study. Second, the review was conducted using the available evidence to date. Thus, further studies published in this duration are excluded from the review process. The studies included did not support sufficient data to enable conclusions on the wider aspect. Perhaps the quality and quantity of chest physiotherapy interventions during the SARS-COV-2 pandemic are effective in improving health-related Quality of Life (QoL). Future recommendations should be considered on doing large sample randomized controlled/clinical trials to estimate mediating relationships between changes in physical activity, sleep, and wake time with the functional status of children. Assessing the methodological quality of the studies reviewed was difficult because different study designs were identified.
Clinical Application
Physiotherapy has been utilized to treat a variety of respiratory issues. When administered early, it has been claimed to enhance gaseous exchange, reverse pathological progression and reduce or eliminate the requirement for artificial ventilation. Patients who are on mechanical ventilation may struggle to breathe. This puts the patients at risk for pneumonia brought on using a ventilator and lung collapse. Chest physiotherapy can be utilized in certain situations to shorten hospital stays on a mechanical ventilator and in the ICU and to avoid ventilator-associated pneumonia. Techniques including airway clearance, lung maneuver recruitment, endotracheal suctioning, and a change in posture are advised for patients who are on a ventilator. Positioning, an active breathing cycle, manual or ventilator hyperinflation, percussion, and vibration, with PEP, are among the recommended airway clearance techniques.
Conclusion
Majorly all healthcare personnel have gone through a face-to-face encounter with SARS-CoV-2 infection and critically ill pediatric patients have been reported at all ages. Chest physiotherapy interventions, when included in acute stage, have known to be a promising therapeutic strategy in improving physical competence and decrease adverse effects related to pulmonary complications. Furthermore, a decrease in the overall duration of stay was observed in the intensive care setup. As respiratory assistance is crucial thus, integrative strategies should be considered. Thus, the authors emphasize the significance of multidisciplinary approach involving chest physiotherapy and musculo-skeletal rehabilitation to reduce complications, facilitate recovery and ensure effective healing in children.
Author Contributions
Study conception and design: AS, NS; data collection: AS, AC; analysis and interpretation of results: NS; draft manuscript preparation: AS, NS, AC. All authors reviewed the results and approved the final version of the manuscript.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval/Patients Consent
Not applicable as it does not involve human and animal participants.