
Abstract
Children who identify as Black or multiracial report significantly higher exposure to adverse childhood experiences, which places them at greater risk for poor mental and physical health outcomes. These disparities and increasing awareness of racism as an adverse childhood experience has resulted in the American Academy of Pediatrics, American Psychological Association, and other groups declaring racism a public health crisis. To provide high-quality care, providers who engage with patients and families impacted by systemic racism must be aware of its role in health disparities. This requires clinicians to have the knowledge and skills to discuss racism with colleagues, patients, and families. To promote clinicians’ competence to engage in these discussions, this article 1) sensitizes providers to historical and contextual factors that inform experiences with anti-Black racism and health disparities and 2) offers strategies to address anti-Black racism in clinical care.Embracing the process of brave, informed conversations about race represents a pathway for building trust between providers and patients, a key component of various health outcomes. Additionally, these foundational skills of reflection, cultural humility, and bias recognition will be needed to engage in allyship and advocacy both within and beyond the exam room.
Introduction
Adverse childhood experiences (ACEs) provide a model to more fully understand and intervene on well-documented disparities in health care. Children identifying as black or multiracial report significantly higher exposure to ACEs compared with whites.1,2 This results in a significantly greater risk of poor mental and physical health outcomes and care. 3 Given its invocation of a stress response, often chronic in nature, racism is often considered an ACE, although it was not included in the initial ACE study.4-6 More recent studies have included experiences with racism and discrimination as an ACE.7,8 Racism’s harsh impact on health and society has been reified by the recent murders of black Americans by police officers and the COVID-19 pandemic, with black people contracting the virus and dying at disproportionate rates. 9 This has resulted in the American Academy of Pediatrics, American Psychological Association, and other groups declaring racism a public health crisis.10-12
Health care providers who engage with patients and families affected by systemic racism must be aware of its role in health disparities. Moreover, clinicians need a working knowledge base by which they can discuss racism with colleagues, patients, and families. This article seeks to (1) sensitize providers to historical and contextual factors that inform experiences with antiblack racism and health disparities and (2) offer strategies to address antiblack racism in clinical care. We have chosen to focus on racism that impacts people who identify as black given the unique health disparities this group faces; similar approaches may be useful for those working with other racially minoritized groups. Understanding the history and context of this specific group can provide a framework for understanding the history and context of other racial and ethnic groups.
Contextual Factors
Within the United States, systemic racism is a pervasive system of racial inequity that advantages white people and disadvantages black people. Systemic racism was built into legislation, policies, and practices across all areas of American life and persists today. For example, the 1930s practice known as “redlining” led to segregated neighborhoods, limited the ability of black individuals to create generational wealth through real estate, and led to disparities in school funding across neighborhoods. Today, schools are often funded through taxes on property and locally assessed taxes; therefore, less funding is provided for schools in neighborhoods deemed “less desirable,” contributing to lower performance among schools serving predominately black students. These structural disparities lead to lower educational attainment, which can decrease life expectancy and lifetime earnings. 13
The recently well-publicized murders of black people by police officers have heightened awareness of the pervasive inequities built into incarceration and policing systems today and since their inception. 14 Currently, black people are 3 times more likely to be killed by a police officer than their white counterparts, and black people are incarcerated at 5 times the rates of white people. 15
In parallel with other institutions in our country, the roots of modern medicine in the United States are rich with exploitive practices and racism. The stories of Henrietta Lacks and the Tuskegee Syphilis Study are among the most widely known unethical studies in medical history. However, in numerous lesser-known stories exists the legacy of this harmful relationship reverberating today in the health disparities seen in chronic and acute conditions, premature death, and infant mortality. 16
Practices to Respond
As our brief and limited review of historical and contextual factors intimates, providers must first understand the root causes of racism to provide transformative, equitable care. Concurrently mitigating the impact of racism is equally important, given increasing rates of racial stress (from direct and/or vicarious discriminatory racial encounters) and racial trauma (post-traumatic stress disorder–like symptoms that emerge because of exposure and re-exposure to racial stressors).16,17 Strategies at the provider level to address both knowledge gaps and bias/interpersonal racism can indirectly impact broader systems, as changes in provider behavior influence workplace culture and impact systems such as academic health centers. Therefore, this section illustrates how the impact of racism can be explored first individually through reflective practice and cultural humility, and then how providers may dialogue about race both inside and outside the examination room. These strategies aid in building trust and promoting culturally informed care.
Reflective Practice and Identity
Reflective practice is a crucial step to promote racial equity. This requires recognition that one’s attributes, values, views, and context influence how they understand the world. 18 Reflecting on identity provides a framework to understand one’s own power, privilege, and potential sources of bias. This practice also provides an opportunity for providers to understand how they may be viewed by patients and families and gives insight into the assumptions that may surface during patient-provider interactions.
To explore their identity, providers may consider how they describe themselves in the following categories (among many, many others):
Race
Ethnicity
Gender identity
Sexual orientation
Primary language(s)
Ability status
Age
Exploring these questions provides a picture of the multiple aspects of identity for everyone. Each aspect has associated resources and restrictions. 18 Resources may aid opportunity, and restrictions may make conventional success more challenging. This reflection enables us to appreciate the nuanced nature of identity and the saliency of various identities in different contexts.
For example, in a clinic that provides care to a predominantly black population, the racial identity of the health care providers is predominant. In a discussion with a new mother about her experiences breastfeeding, the authors’ identity as women may be more salient. Furthermore, reflection on our multiple identities provides opportunities to recognize nuance. In talking with a black mother about disciplining her 5-year-old black son, one author’s identity as a white woman will likely feel different to the mother (and to the provider) than the experience of authors who identify as black women.
Table 1 provides an example of one of the author’s identities and how this aligns with their resources and restrictions.
Example of Identities and Associated Resources and Restrictions.
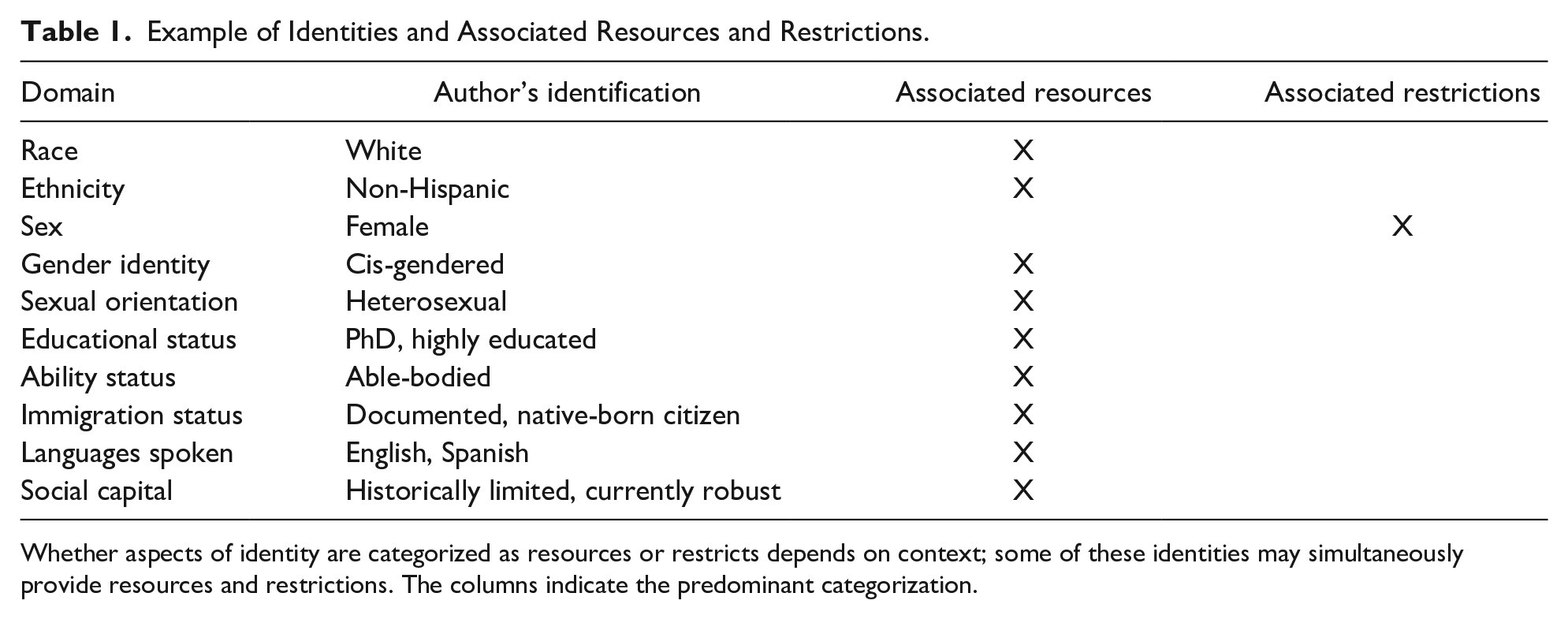
Whether aspects of identity are categorized as resources or restricts depends on context; some of these identities may simultaneously provide resources and restrictions. The columns indicate the predominant categorization.
Cultural Humility
Once providers have engaged in reflective practice to understand their identities, cultural humility can guide their process of approaching conversations about race with patients. Cultural humility is “a lifelong commitment to self-evaluation and critique, to redressing power imbalances . . . and to developing mutually beneficial and non-paternalistic partnerships with communities on behalf of individuals and defined populations.” 19 Cultural humility requires providers to recognize feelings of shame, guilt, and fear associated with having conversations about race, especially when the provider’s identities afford them more privileges than their patients. Engaging in this work alongside someone else (eg, another provider or staff) can strengthen the commitment to this work and support recognition of one’s affect and need to engage in emotional regulation during conversations about race. This collaboration can also support providers’ understanding of implicit biases—unconscious and involuntary attitudes that can influence affect, behavior, and cognitive processes—impacting provider-patient interactions and creating challenges to engaging in cultural humility. 20 Examples of these biases include perceiving black families as demanding, minimizing black patients’ experiences of pain, and having less confidence in black families’ ability to follow recommendations. 20 The motivation to engage in the internal work of self-reflection and distress tolerance is to reify providers’ equity values and desire to evolve as a provider.
Cultural humility, reflection on identities, and recognitions of one’s own biases promote providers’ capacity to (1) identify racial trauma in clinical encounters and (2) inform their ability to respond in a culturally responsive manner. 21 For example, families may be hesitant to trust providers, especially those from a different racial or ethnic background or those using a different communication style. 16 Families may use defensive language (eg, “Why are you asking me whether I have enough food?”), which can be adaptive or protective in various environments where they need to advocate for themselves and do not trust others’ intentions. 16 However, in an encounter where a provider’s inquiry represents the intent to support the family (eg, providing information on local food banks), this may result inadvertently in perpetuating disparities. Other families may be easily emotionally dysregulated in an unpredictable clinical environment (eg, “Why are you taking so long to see my child?!”), which can be related to neurobiological changes associated with ACEs.16,22 This can make the development of rapport more challenging and divert the focus of the clinical encounter. When reflecting on patient encounters, be mindful not to rely on unconscious biases; families and patients are unique as are their lived experiences. The goal is to heighten awareness of how historical and contextual factors may present in common clinical experiences. Engagement in difficult dialogues about race is crucial for connecting with families and placing their concerns in context.
Engaging in Dialogues About Race
In the Examination Room
Aligning with cultural humility practices, a provider’s role during clinical encounters is neither to fix families’ experience of racism nor to try to reframe the family’s narrative. Instead, we offer a model that is an extension of the medical home principles of family-centered, culturally responsive care and appreciates the role of racial stress and trauma in clinical work with families. The PEARLS (Partnership, Empathy, Apology, Respect, Legitimize, Support) framework is taught in many nursing and medical schools as an effective communication approach. 23 The authors developed Figure 1 as a guide for addressing common concerns providers may have in initiating conversations about race. Therein are examples of how to apply PEARLS to conversations with patients and families about experiences of racism.
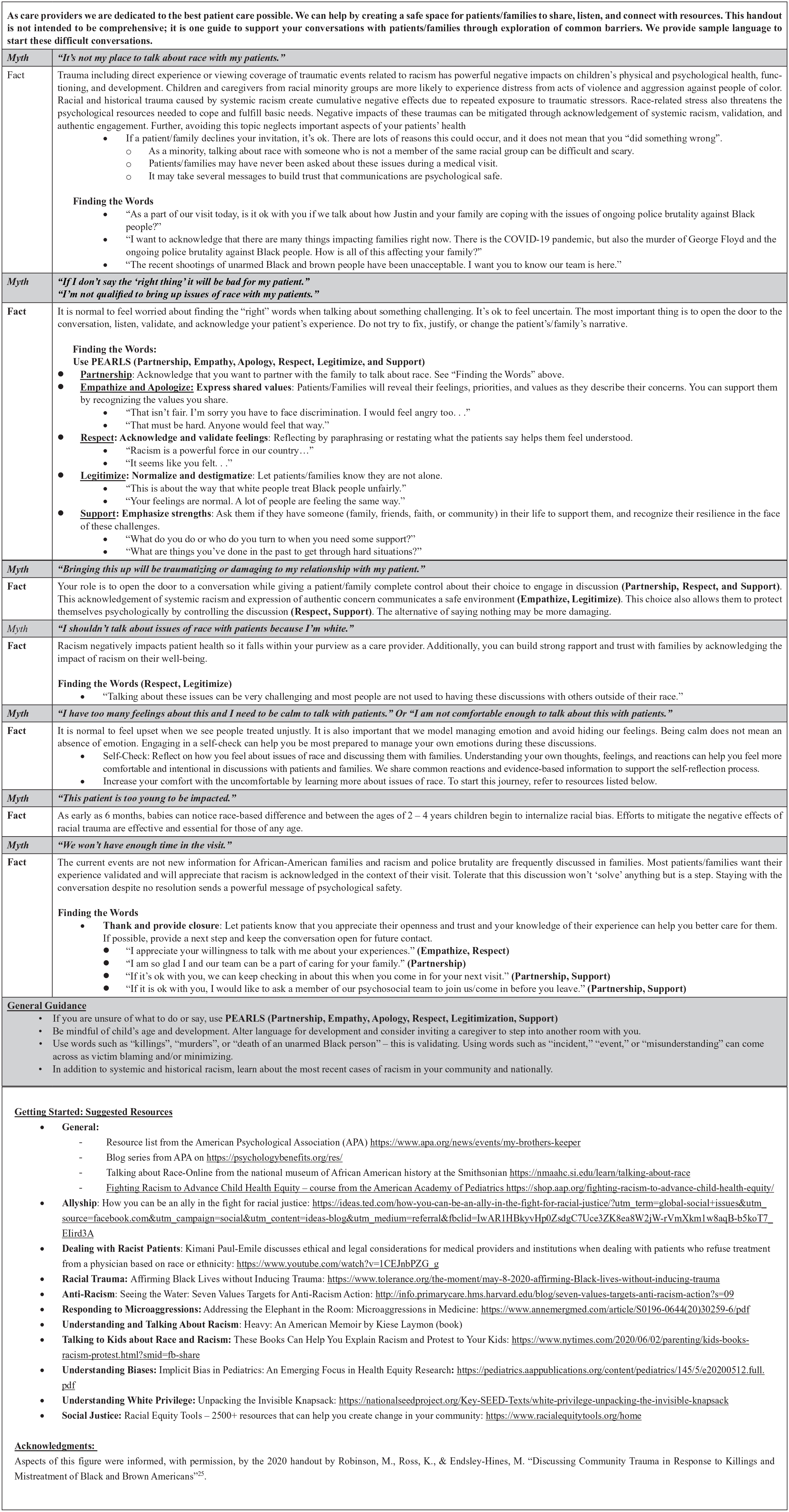
Guidance for providers related to patient and family experiences of racism.
Outside of the Examination Room
The work to dismantle racism and the white supremacist ideology that entrenches everyone is not limited to patient care roles but extends to all aspects of the professional role. Notably, we have been socialized to maintain this ideology through our words and behaviors. For example, what is the best response when race or racism is present in daily interactions with colleagues? Despite many academic institutions’ verbal allegiance to anti-racism, day-to-day, many avoid active acts of anti-racism with colleagues. Finders and Kwame-Ross describe speech acts common to academia that fortifies the structures of racism directed toward black people and other racially minoritized groups. 24 Specifically, these are behaviors made by white people, such as the following:
Not hearing a speech act as privileging white people or as racist
Despite recognizing a speech act as racist, remaining silent publicly and providing support privately
Pivoting conversations away from race
Perception of talk from or between black or other racially minoritized colleagues to be angry or emotionally charged
Becoming visibly upset during discussions about race or racism, or considering such as a personal attack, resulting in a shift from the issue at hand
Talking over colleagues from racially marginalized backgrounds. 24
Disruption of racist processes requires naming and addressing these behaviors the moment they occur. Health care providers should take note of behaviors during meetings, in the workroom, on rounds, and in leadership circles and should consider how they might respond when they have the opportunity to do so. For example, during a staff meeting, one might encourage team members to consider the racial make-up of the physician and nonphysician staff, and the implications of those dynamics on families. In addition to this reflection and pre-planning, providers can discuss their efforts with a trusted colleague. It is normal to be fearful and nervous to respond in the moment. In fact, systemic racism and white supremacist ideology rely on individual discomfort to fortify itself. It is only by refusing to accommodate fear and anxiety that health care providers can help dismantle these systems.
Call to Action
Embracing the uncomfortable process of being vulnerable in conversations about race with patients and families represents an opportunity for a small but impactful corrective experience. Most people have never had these conversations in a health care setting or with someone outside of their intimate support network. It is uncommon for these hard discussions to happen across racial lines. Over time, brave, informed conversations will be a pathway for building trust between providers and patients, a key component of various health outcomes. 22
Change is required beyond the examination room. Providers seeking to expand their sphere of influence can use their resources (eg, education level, background, racial/ethnic status) to amplify the voices of patients of color and advocate for systemic practices or policies within their clinical setting, institution, community, and government. Although beyond the scope of this commentary, these broader efforts, which need to be anchored in allyship with black people and other racially marginalized groups, will require the foundational reflection skills, cultural humility, and bias recognition used in patient-provider interactions. 25
Author Contributions
RH: Conceptualized this project; completed the analyses; drafted and revised the manuscript; approved the final manuscript as submitted.
AMSC: Conceptualized this project; completed the analyses; drafted and revised the manuscript; approved the final manuscript as submitted.
EM: Conceptualized this project; completed the analyses; drafted and revised the manuscript; approved the final manuscript as submitted.
Footnotes
Acknowledgements
The authors acknowledge the pivotal role of patients with whom they work in shaping this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval/Patient Consent
This work was exempt from external/IRB review and did not require patient consent.