
Abstract
Adverse childhood experiences (ACEs) and social determinants of health (SDOH) negatively affect health outcomes. This program was developed to screen for ACEs and SDOH in the primary care setting in families with children 9 months to 5 years of age at well-child checks and provide interventions that support families and build resiliency. Programmatic criteria were identified, referral resources were developed, and a database was implemented, with 246 families enrolled in year 1; 56.9% of caregivers reported 1 or more ACEs for their child, 63% of caregivers reported an SDOH need, and 39.4% of caregivers reported both. The average number of ACEs was 0.94. This program was created to address ACEs and SDOH, to empower families, build resiliency, and provide buffers to mitigate and prevent ACEs. It provides a model that can be implemented in a primary care setting while providing wraparound resources, including integrated mental health resources and referrals, to measure the success of these interventions.
Introduction
Adverse childhood experiences (ACEs), including abuse, neglect, and household dysfunction experienced prior to age 18 years, have been described as the public health emergency of this time. 1 Research shows a wide range of chronic diseases originate with or are exacerbated by exposure to toxic stress, or chronic adversity without sources of resiliency, in childhood. 2 Downstream impacts include learning and cognitive disabilities, asthma, obesity, diabetes, cancer, and behavioral health disorders.2-4 Adverse childhood experiences, when layered with the effects of social determinants of health (SDOH), can combine to exacerbate these exposures and outcomes. Research shows exposure to ACEs and unmet social needs are more common in those living in lower income communities. 5 The American Academy of Pediatrics (AAP) recommends routine screening for ACEs. 6 Early detection and intervention may be able to prevent negative health outcomes. The primary care setting is an ideal place for universal screening, health promotion, and disease prevention. This includes screening for ACEs and SDOH, and providing emerging and evidence-based interventions. The challenge for pediatricians comes in how to address these significant drivers of health outcomes in the clinical setting. While screening and intervention programs are being piloted and validated nationwide, there is currently little information on the practical and logistical steps needed to undertake this type of practice changing action.
Memphis, Tennessee, the county seat of Shelby County, has a metro area population of 1.3 million. 7 It routinely ranks near the top of overall and childhood poverty for a city its size. Recent data show a child poverty rate of 35% and an overall poverty rate of 21.7%. 8 These statistics, combined with poor housing stock, poor public transportation, and high rates of community violence, contribute to numerous SDOH. In 2014, Shelby County conducted a confidential, randomized survey of 1506 residents by telephone. The survey revealed that 52% of individuals reported at least 1 ACE and 12% reported 4 or more ACEs. The most prevalent ACEs were substance abuse, emotional abuse, and violence between adults in the home. Those living in poverty and those with less than a high school education were more likely to report 4 or more ACEs. 9
Memphis is one example of a community with high levels of childhood poverty and attendant accumulation of ACEs, leading to disparities and poor health outcomes. The statistics highlight the challenges that many families and children face in their day-to-day lives and the opportunity for pediatricians and health care providers to address these issues while also taking a strengths-based approach to support families and build resiliency. The Family Resilience Initiative (FRI) was created to address ACEs, SDOH, and infant mental health in the pediatric primary care setting. Programs such as this can equip primary care providers with opportunities to address ACEs in children and change outcomes prior to adulthood. The FRI program provides families with education on ACEs, tools to prevent future ACEs, and the resources to address and mitigate the impact of trauma of previous ACEs, and supports families with health-related social needs (HRSNs) as they navigate these situations. This moves beyond simply screening for ACEs and to implementing proven interventions.
The FRI program is embedded in the University of Tennessee Le Bonheur Pediatric Specialists (ULPS) General Pediatrics Clinic, an academic teaching practice affiliated with the University of Tennessee Health Science Center (UTHSC) that sees more than 14 000 patients per year in the urban core of Memphis. Approximately 95% of the patient population is insured by Medicaid. The FRI program is an integrative, collaborative initiative that employs outreach coordinators embedded in the ULPS clinic to screen for and address ACEs and SDOH. The program partners with families to meet their HRSNs and to provide education, prevention, and intervention for ACEs and their associated health effects.
Methods
Prior to 2018, the ULPS General Pediatrics Clinic routinely screened for food insecurity but not for ACEs or other SDOH. The FRI program was developed as an integrated, multidisciplinary collaborative to screen for and address ACEs and SDOH in the clinical setting using a wraparound approach. The goal is to build resiliency and prevent future ACEs within a trauma-informed setting while utilizing community partner resources to address needs (Supplemental Figure 1).
The FRI Implementation team was established, and the team reviewed existing ACE and SDOH screening tools, programs, and evidence-based or best practice interventions. The primary funder of the program, the Urban Child Institute, was involved in the program from the beginning. A team of clinicians, researchers, and funders visited similar programs in California to learn from existing programs and explore their processes and philosophies. The program learned some aspects of design from other programs in the country with similar aims and was then able to combine best practices from different programs to develop a unique program with an ambitious aim to address ACEs, SDOH, and a robust follow-up and intervention program for each with measurable outcomes. The program was also able to build on a strong, well-established foundation around ACEs and trauma-informed care in the state of Tennessee that was created through the Building Strong Brains program. Tennessee legislators were interested in a way to address ACEs before children become adults, to build resiliency, and to ameliorate the effects of ACEs to build a healthier state. Thus, there was support from the state at the outset as well, a common language, and a strong knowledge base on ACEs.
The FRI program utilizes a modified version of the Pediatric ACEs and Related Life-Events Screener (PEARLS) developed by the Bay Area Research Consortium on Toxic Stress and Health (BARC) that includes the 10 original ACE questions regarding abuse, neglect, and household dysfunction, and 7 additional questions related to community violence, discrimination, housing insecurity, food insecurity, separation from a caregiver, physical illness or disability of a caregiver, and death of a caregiver. 10 This tool was chosen due to the experience of the research team and the validation of this tool. The Accountable Health Communities (AHC) HRSN Screening tool developed by the Centers for Medicare and Medicaid Services (CMS) was chosen as the SDOH screening tool. It is a 10-item, standardized questionnaire covering housing instability, food insecurity, transportation problems, utility help needs, and interpersonal safety. This tool was chosen for its length, the ability to provide timely intervention for issues identified, and the anticipation for potential reimbursement for administration of the tool in the clinical setting. 11
The FRI program is funded through the State of Tennessee and a grant from the Urban Child Institute, a nonprofit organization focused on early childhood development. Funding provided employment for 2 outreach coordinators, a program manager, and partial support of a psychologist and program evaluator. The program utilized affiliations within a large health care system and university to provide medical-legal services, social services, and connections to a large database of community resources.
The FRI program has been integrated as a part of the ULPS General Pediatrics Clinic since May 2018. The program began with 2 outreach coordinators embedded in morning clinics Monday through Thursday, screening patients ages 9 months to less than 5 years of age as part of their well-childcare visits. The outreach coordinators introduce themselves to the family and assist with developmental screenings or other paperwork to build rapport and assist with clinic flow in an effort to minimize the impact on the total time of the clinic visit (Supplemental Figures 2 and 3). The outreach coordinators take advantage of the time between patient triage and a provider entering the room to do the bulk of their work. After an introduction, they ask the caregiver about participating in the FRI program and obtain consent. The AHC HRSN screening tool is administered first to build rapport and trust, and then the ACE screening tool.
If the family identifies any SDOH, the outreach coordinator works with the family to identify the most pressing need and works to meet that need directly through clinic resources, Methodist Le Bonheur Community Outreach services, or a network of community partners. A warm handoff is provided at each step and the outreach coordinator re-contacts the family to ensure they were able to access these resources and the need was met. This includes the outreach coordinator connecting with the various resources to ensure that they can provide the service required, their access information, and any other pertinent information for the family, as well as providing an introduction and sense of safety for the family as they reach out to a new service.
If any ACEs are identified, the outreach coordinator offers the family a free consultation and counseling through an embedded UTHSC child psychologist. If the family accepts, the outreach coordinator provides a warm handoff to the psychologist. The warm handoff ensures an introduction to the psychologist which the client is aware of and a part of, allowing a sense of safety and the beginning of rapport. The warm handoff includes information on the ACEs and SDOH the family has reported and any other pertinent medical or social information gained as part of the intake process. Subsequently, the psychologist performs an intake assessment and provides evidence-based treatment and infant mental health services to address the identified needs.
Education on adverse childhood experiences and strategies for prevention are provided to all families, as are general counseling to promote healthy living and well-being. The outreach coordinators may also provide, directly or through referral, other evidence-based programs that promote resiliency, nurturing relationships, developmental skills, and other practices. The outreach coordinators are very flexible throughout this process. They may step out of the room during the medical encounter or may stay at the request of the family. They may continue to collect information and provide resources both before and after the medical portion of the visit as needed.
After the intake process, the outreach coordinator provides a summary of the referral information, and the caregiver completes a brief satisfaction survey. If the client has an appointment with the psychologist, the outreach coordinator provides the appointment information and plans to meet the client at the appointment for the warm handoff. The outreach coordinator also communicates the findings and proposed interventions to the medical team, closing the loop for the entire care team. This process also includes a warm handoff model if all parties are available so that the new information can be incorporated into the ongoing medical care, which serves to inform the medical team of any ACEs or SDOH reported and their nature. The outreach coordinator then documents a summary of the findings and interventions in the medical record and client database. The documentation in the medical database also closes the loop for the medical team and serves as a backup process in the event that a warm handoff was not performed in real time during the visit.
The outreach coordinators perform a variety of follow-up activities with the families enrolled. Through a tiered triage system based on intensity of the needs, outreach coordinators follow up with families via text, phone call, home visits, and at future visits to provide ongoing assessments, interventions, and other resiliency resources. Additional interventions offered to all FRI families include the Triple P—Positive Parenting Program, the LENA (Language Environment Analysis) Start Program, Tennessee Building Strong Brains initiative ACE education, and other community-based programs. Family Resilience Initiative also provides free transportation to families for psychology appointments.
The outreach coordinators also perform annual screenings on patients and families as part of the FRI renewal process. These are ideally conducted in the clinic as part of a future visit but may be conducted via phone. This process consists of an annual screening for SDOH needs and the ACE screening, just as in the initial intake process. If any new needs are identified, the process described above begins anew to address current or ongoing issues. This information is entered into the database and communicated to the medical team.
The FRI team utilizes a robust, health insurance portability and accountability act of 1996 (HIPAA)-compliant database through iCarol (Ottawa, Ontario, Canada) to track all patients and families enrolled, and to map the interventions provided, follow-up frequency, and follow-up activities. For the results, raw data from the client intake forms were exported into SPSS (Version 27), and descriptive statistics were generated.
Results
The FRI program was implemented in the ULPS General Pediatrics Clinic in May 2018. For the first year of intake through May 2019, FRI evaluated 334 families, with 246 agreeing to participate in the FRI program (73.6%; Table 1). Children served during FRI’s first year (n = 246) were predominantly black (92.3%) and non-Hispanic/Latino (96.7%). Family Resilience Initiative saw a nearly equal split of male and female children (51.6% male). Families were predominantly low income, with 58.8% reporting an annual income of $15 000 (US$) or less. At enrollment, 39.4% of families reported having both ACEs and SDOH, and 56.9% reported at least 1 or more ACEs. Sixty-three percent of families reported at least 1 SDOH-related need. The FRI program also enrolls families who have no ACE or SDOH issues reported to allow the team to notify these families for future education or resiliency opportunities. This applied to 19.5% of families enrolled in the first year (n = 246).
FRI Client Demographics.
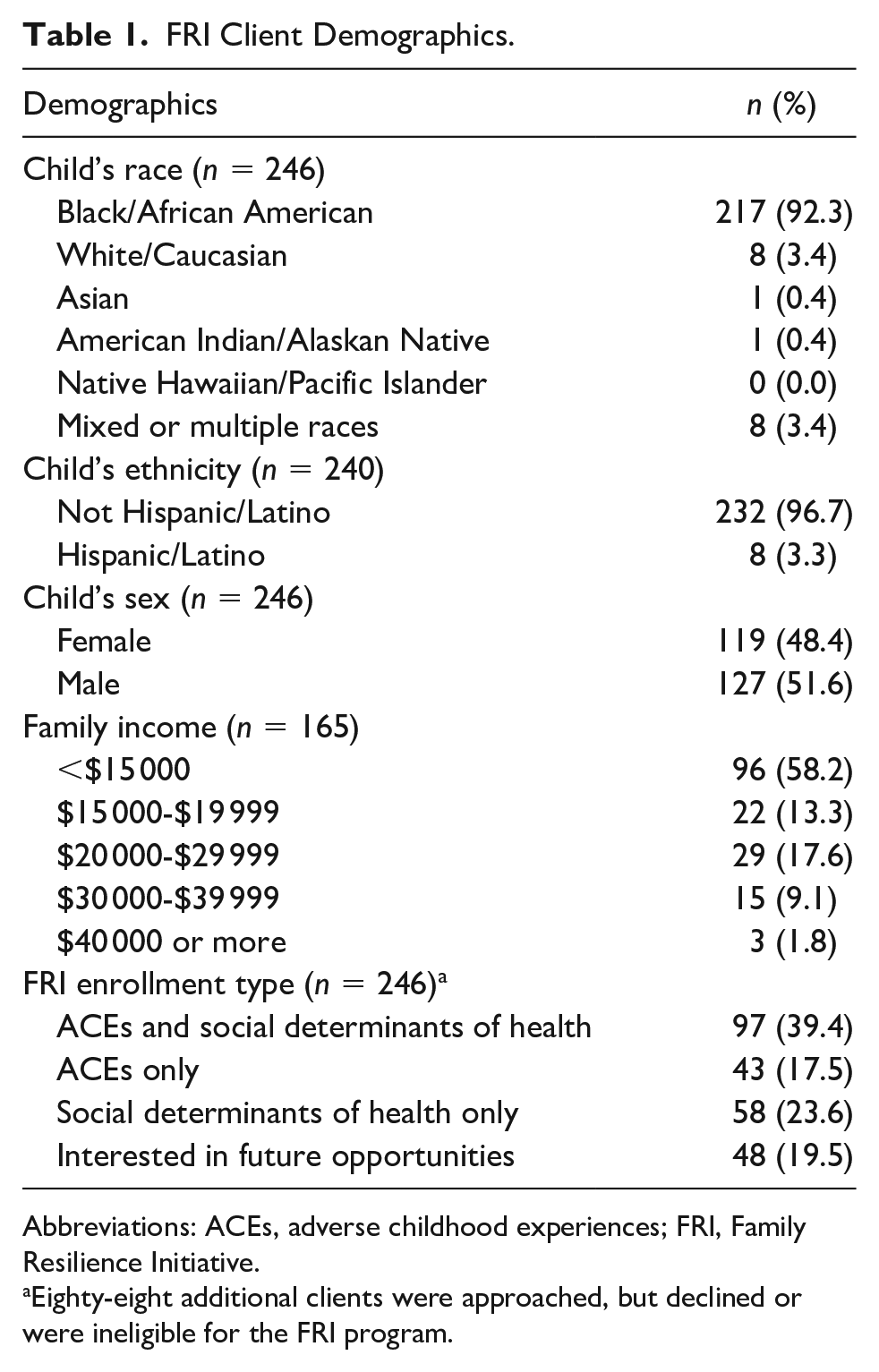
Abbreviations: ACEs, adverse childhood experiences; FRI, Family Resilience Initiative.
Eighty-eight additional clients were approached, but declined or were ineligible for the FRI program.
Family Resilience Initiative clients answer a total of 17 ACE questions (Figure 1). The most common ACE reported in section 1 (Questions 1-10) was separation or divorce of parents/guardians (40.7%). The second most common ACE reported in this section was the child living or having lived with a household member who was depressed, mentally ill, or attempted suicide (13.4%). In section 2 (Questions 11-17), the most common ACE was children experiencing or who have experienced a serious medical procedure or life-threatening illness (10.2%), while exposure to violence in the neighborhood was also reported frequently (6.1%). The number of reported ACEs in children seen by FRI ranged from 0 to 8, with an average of 1 ACE per child. Forty families (33.1%) received a referral for psychology services (n = 246).
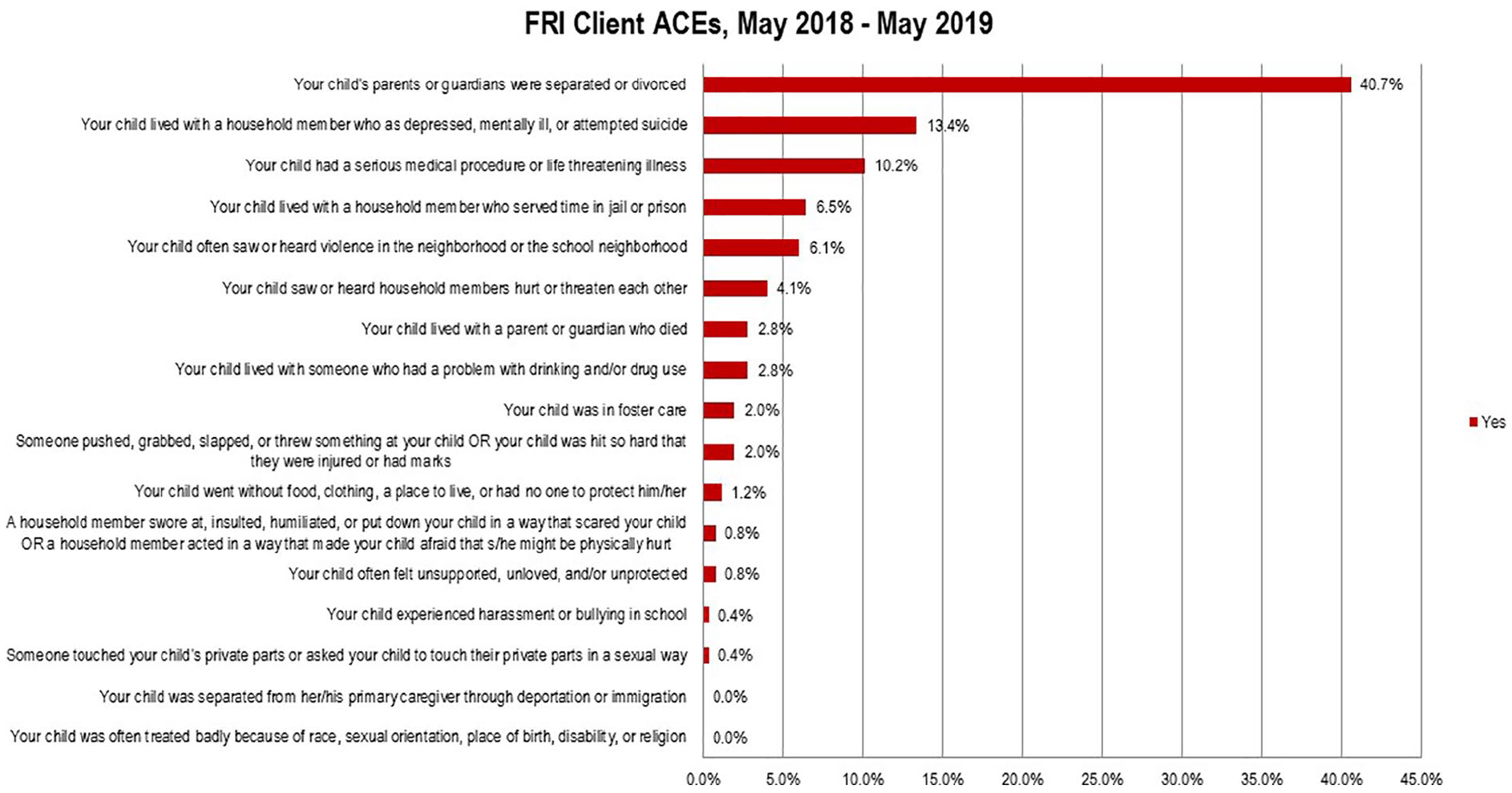
FRI client ACEs. Section 1: Questions 1-10; Section 2: Questions 11-17.
Family Resilience Initiative families reported a variety of SDOH issues as part of their enrollment screenings (Table 2). The most common issues were around food insecurity, with utility needs and transportation needs reported as the second and third most common issues, respectively. Reports of food insecurity were common, with 33.5% reporting worry about running out of food before they had money to buy more and 25.8% reporting that their food did not last and not having money to buy more. Overall, 5.6% of families responding reported that they did not have housing or that they were worried about losing their housing in the near future. Many families reported concerns related to housing outside of housing instability, such as problems with mold, smoke detectors not working, water leaks, or pest infestation. Utility needs were reported in 19.6% of respondents, while transportation needs encompassing both medical and nonmedical needs were reported by 18.4%. Families also reported issues around personal safety, most commonly that someone insults or talks down to them (16.3%) or screams or curses at them (17.1%), while rates of reporting physical harm (4.5%) or threats of harm (6.1%) were lower. Families reported their most pressing concerns were food (36.1%), followed by housing (21.5%) and the child’s development (18.8%). Outreach coordinators made referrals for 62.9% of all clients, and 70.2% of those reporting at least 1 ACE or SDOH (n = 246).
Social Determinants of Health.
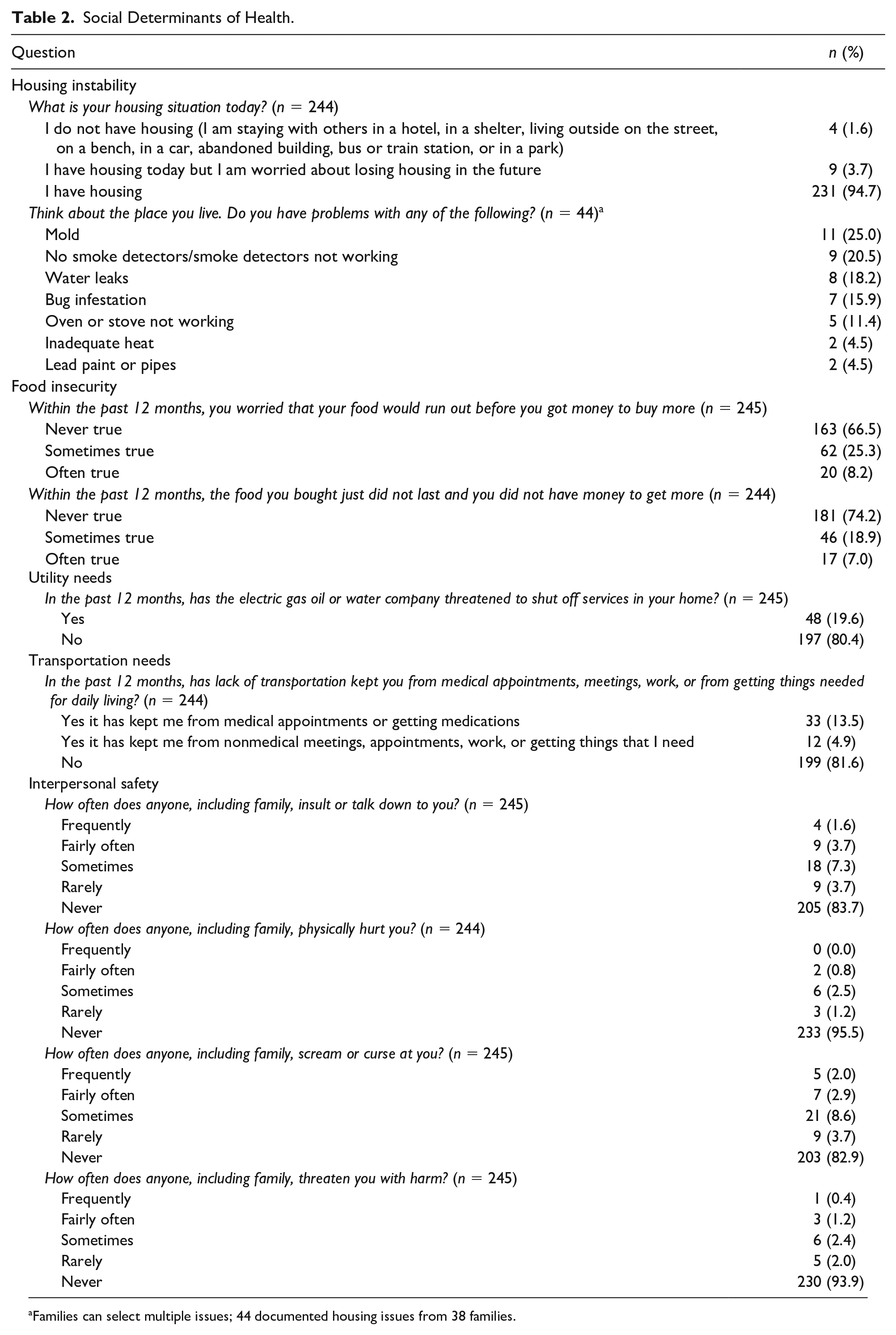
Families can select multiple issues; 44 documented housing issues from 38 families.
A crucial component of the FRI program is the follow-up activities that the outreach coordinators perform with families (Table 3). This includes reaching out to resources on their behalf, following up to ensure that a connection with the referral resource was established, that the referral met the reported need, assisting with paperwork or other items, scheduling and confirming appointments, and more. Outreach coordinators conducted a total of 2240 follow-up activities. Of the follow-ups, the most common activity was following up on a referral (29.4%), followed by confirming appointments (18.3%) and well-being check-ins (13%).
Referrals and Follow-Ups.
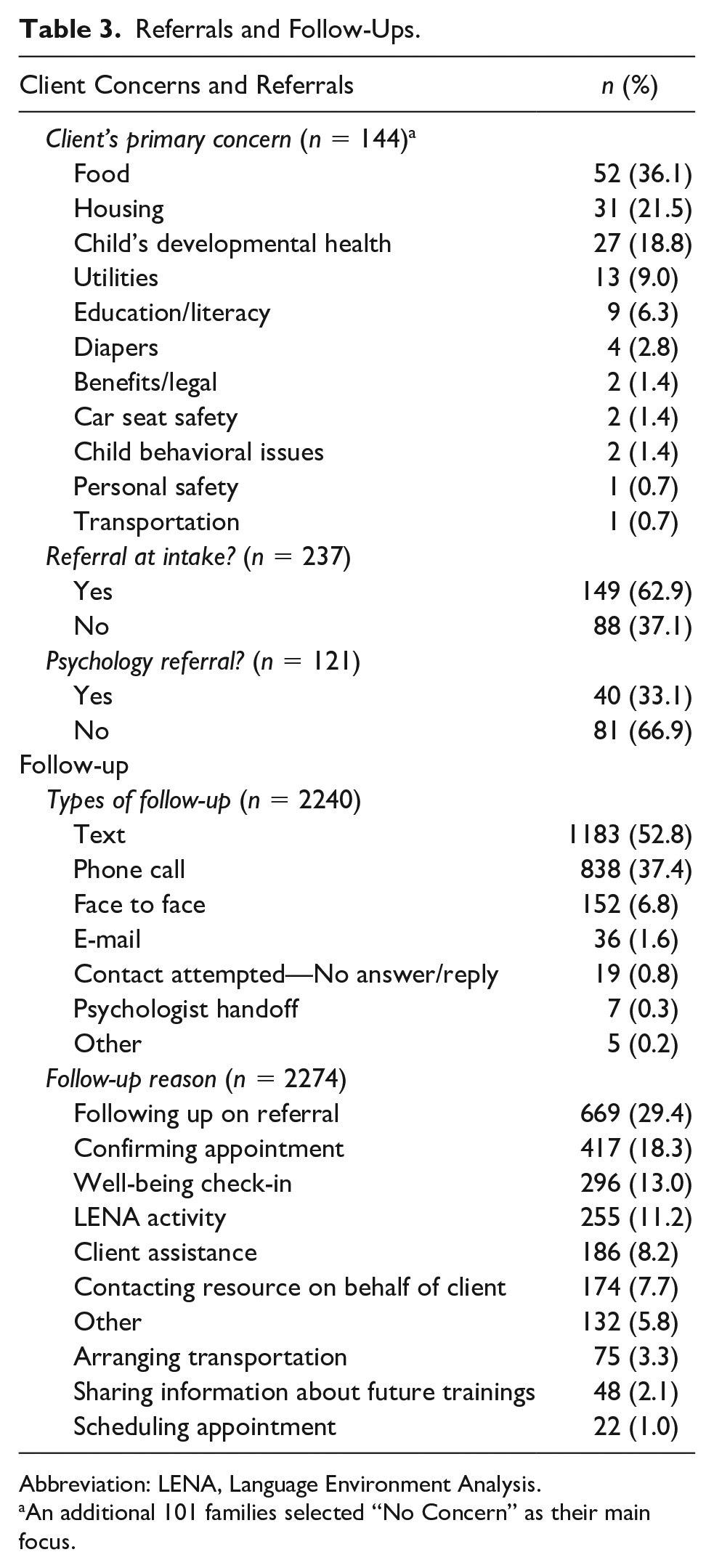
Abbreviation: LENA, Language Environment Analysis.
An additional 101 families selected “No Concern” as their main focus.
Discussion
The feasibility of the FRI model has been demonstrated through the successful design, implementation, and experience through 1 year of screening and enrollments. In the first year of the project, 246 clients were enrolled, 310 total referrals were made for 121 clients, and 2240 follow-up activities were conducted. The adoption of best practices using a standardized instrument and a database system led to successful implementation and allows for seamless replication of the project. Health care systems may use this approach to implement trauma-informed care.
The FRI program aims to provide holistic, trauma-informed care while addressing social and mental wellness. Many studies have been conducted on the health outcomes and the intergenerational effects of maternal ACEs on the child,2,12,13 but few studies have examined protective factors beyond the parent-child dyad. These protective factors are what the FRI program seeks to employ and study through the interventions provided by a multidisciplinary team. Addressing ACEs and SDOH is the future of pediatrics. The AAP supports screening in the primary care setting. While screening tools are being developed and validated, it is important to integrate these services into standard medical care and in alignment with the medical team.
The FRI program serves a young population aged 9 months to 5 years at the time of enrollment; data show that ACEs are common at these ages, with an average of 1 ACE reported per child. In addition, 56.9% of children had at least 1 ACE reported. This supports evidence that ACEs are universal from a young age. Adding to the knowledge that ACEs affect brain structure, stress hormone levels, and a multitude of health and educational outcomes indicates an urgent call to action. In pediatrics, SDOH affects the whole family, including the child. Many of these issues are inextricably linked to childhood ACEs. Combining the experience of commonly reported ACEs with the most commonly reported SDOH demonstrates what these families face in their lived experience. This further explains the overlay of ACEs and SDOH in pediatric medicine and the need to address both with a focus on intervention to mitigate the effects of previous exposures, while providing resiliency building, empowerment, and education to prevent future ACEs.
The experience of FRI describes 1 method to select appropriate screening tools, develop clinical protocols, and to integrate programs addressing SDOH and ACEs into the primary care setting. Tools that can be administered efficiently while also providing information that can be addressed in the clinical setting are essential for success. The outreach coordinators provide a bridge between the patient, family, and medical team by developing rapport and discussing sensitive information in a trauma-informed manner. While many programs focus solely on either ACEs and SDOH, the FRI program is unique and ambitious in its attempt to address both ACEs and SDOH, recognizing that these issues are often intertwined for families. By meeting SDOH needs and building trust, the team can then address ACEs to provide evidence-based intervention, education, and prevention strategies.
One unique component of the FRI program is the seamless access to psychology services. For families who meet the criteria, the first appointment for services can be made at the clinic visit, with the potential for same-day services. In addition to contacting the client with appointment reminders, on the appointment day, the outreach coordinator is there to greet the client, provide support, and provide a warm handoff to the psychologist. Family Resilience Initiative is also able to offer no-cost transportation to these appointments, further assisting the clients in accessing psychological services.
Another critical and unique component of the FRI program is the intensity and frequency of the follow-up activities to maintain contact and build relationships with families. This type of continued contact builds trust and allows the FRI program to ensure that resources were accessed, and needs were met. This part of the program will continue to be studied for effectiveness and client satisfaction over the course of the program. Based on other relational programs, such as the Nurse-Family Partnership, 14 the FRI team theorizes that this will be a key component to building resiliency and well-being in clients and in empowering families in the future. This level of follow-up and rapport is unique for a clinic-based program and has been seen as one of the keys to success.
The strengths of this study include the robust referral systems in place, the repeated follow-up and contact with the families through the outreach coordinators, and embedded mental health services provided by a psychologist. The limitations include the fact that this is just 1 year of data and is the reported experience of 1 clinic. As FRI is a new program and the relationship between the families and the coordinators is still developing, families may underreport ACE and SDOH needs. A further limitation is that families are asked to respond yes or no to individual ACEs rather than simply report a total number of ACEs (a common practice in many ACE screeners). While this may lead to an underreporting of ACEs, the FRI team found it essential to gather individual ACE data to offer the most comprehensive assistance for families. Last, this program was conducted in a resident teaching practice, which allows more time per visit than a typical private practice setting, which may affect the application of this program in different settings. However, data collected demonstrate that the average visit length was not significantly affected by the program. This may be attributed to the outreach coordinators assisting families with developmental screening questionnaires. In addition, providers have recognized that a small increase in the visit length can result in great benefits to the patients and families. It is also recognized that crises such as homelessness, a significant loss of resources due to a fire, acute food insecurity, or other issues may necessitate a longer visit time as the outreach coordinators and medical team work to create a plan and support for these families. Last, children and families were enrolled only at well-child visits, so that some needs may be missed, and families were only enrolled in morning clinics to allow for the enrollment of controls in the afternoon for the FRI research program.
Several key lessons were identified over the first year of the program. Although the FRI team recognized the importance of the outreach coordinators building rapport and trust with the family, this was initially underestimated. Initially, outreach coordinators asked about ACEs before SDOH but found low rates of disclosure. Therefore, FRI rearranged the questions to ask about SDOH first, prior to asking about ACEs. This resulted in improved rapport and disclosure between the families and outreach coordinators. Another lesson was the number of ACEs required to initiate a psychology referral. Initially, the threshold was 4 ACEs, based on the strong relationship to adverse health outcomes with those having 4 or more ACEs. 9 However, the FRI team recognized that few children met the threshold for referral. The threshold for referral was lowered to 1 to account for the young age of the population, which allowed more children to receive needed mental health services.
Next steps include continued evaluation and research of the FRI program, including further data collection for subsequent enrollees and renewals, and research to evaluate the FRI interventions and impact on child development, health outcomes, health care utilization, and more. Layered on top of the FRI clinical program is a research program that will track a subset of families in a more intensive, Institutional Review Board (IRB)–approved, quasi-randomized research method to further evaluate the effectiveness of these intervention programs. The FRI program can be scaled up and replicated in different clinical practice settings. The team is interested in securing funding to allow for enrollment of adolescents and to expand to a nonacademic practice setting. The FRI program is interested in seeking other funding streams, with an ultimate goal that policy makers, payors, and others would see the clinical, medical, and monetary value in programs such as this and provide adequate funding and resources for all patients and families. Last, a longitudinal study following families for an extended amount of time to further develop long-term outcomes would be of interest to determine the success of programs such as this.
Conclusions
The process for development, implementation, and the FRI first-year experience provides a model for screening for ACEs and SDOH, and providing a wraparound approach to services in the medical home. The mitigation of the effects of ACEs and prevention of future ACEs can alter the physical, mental, and behavioral health, as well as the educational and vocational outcomes of the child through building support and resiliency. It is urgent that clinicians providing care for children do so in a trauma-informed manner and provide connections to resources that can address both ACEs and SDOH in real time.
Author Contributions
JAY: Contributed to the conceptualization and design, methodology, investigation, supervision and data curation, drafting the initial manuscript, and the review and editing of the manuscript.
LWR: Contributed to the methodology, supervision, data curation, drafting the initial manuscript, and the review and editing of the manuscript.
AM: Contributed to the methodology, data curation, formal analysis, drafting the initial manuscript, and the review and editing of the manuscript.
JAM: Contributed to the conceptualization, design, supervision, funding acquisition, data curation, and the review and editing of the manuscript.
SM: Contributed to the conceptualization, design, methodology, supervision, data curation, drafting the initial manuscript, and the review and editing of the manuscript.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228221093279 – Supplemental material for Whole Child Well-Child Visits: Implementing ACEs and SDOH Screenings in Primary Care
Supplemental material, sj-docx-1-cpj-10.1177_00099228221093279 for Whole Child Well-Child Visits: Implementing ACEs and SDOH Screenings in Primary Care by Jason A. Yaun, Lisa W. Rogers, August Marshall, Jonathan A. McCullers and Sandra Madubuonwu in Clinical Pediatrics
Supplemental Material
sj-pdf-2-cpj-10.1177_00099228221093279 – Supplemental material for Whole Child Well-Child Visits: Implementing ACEs and SDOH Screenings in Primary Care
Supplemental material, sj-pdf-2-cpj-10.1177_00099228221093279 for Whole Child Well-Child Visits: Implementing ACEs and SDOH Screenings in Primary Care by Jason A. Yaun, Lisa W. Rogers, August Marshall, Jonathan A. McCullers and Sandra Madubuonwu in Clinical Pediatrics
Supplemental Material
sj-pdf-3-cpj-10.1177_00099228221093279 – Supplemental material for Whole Child Well-Child Visits: Implementing ACEs and SDOH Screenings in Primary Care
Supplemental material, sj-pdf-3-cpj-10.1177_00099228221093279 for Whole Child Well-Child Visits: Implementing ACEs and SDOH Screenings in Primary Care by Jason A. Yaun, Lisa W. Rogers, August Marshall, Jonathan A. McCullers and Sandra Madubuonwu in Clinical Pediatrics
Supplemental Material
sj-pdf-4-cpj-10.1177_00099228221093279 – Supplemental material for Whole Child Well-Child Visits: Implementing ACEs and SDOH Screenings in Primary Care
Supplemental material, sj-pdf-4-cpj-10.1177_00099228221093279 for Whole Child Well-Child Visits: Implementing ACEs and SDOH Screenings in Primary Care by Jason A. Yaun, Lisa W. Rogers, August Marshall, Jonathan A. McCullers and Sandra Madubuonwu in Clinical Pediatrics
Footnotes
Acknowledgements
The authors would like to thank the entire Family Resilience Initiative (FRI) Implementation and Quality Improvement teams, the outreach coordinators, and the entire University of Tennessee Le Bonheur Pediatric Specialists (ULPS) General Pediatrics Clinic staff. We appreciate guidance from Dr. Dayna Long (University of California-San Francisco) and the Bay Area Research Consortium on Toxic Stress and Health (BARC) in designing the program.
Authors’ Note
There are no prior publications or submissions with any overlapping information, including studies and patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Urban Child Institute, Memphis, Tennessee; State of Tennessee, Nashville, Tennessee; Children’s Foundation Research Institute, Memphis, Tennessee; and Memphis Research Consortium, Memphis, Tennessee.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.