
Abstract
This study assessed the impact of respiratory syncytial virus–confirmed hospitalizations (RSVH) on caregivers of high-risk preterm infants. Caregivers for infants born at 29 to 35 weeks’ gestational age and hospitalized for confirmed RSV disease responded to measures of self-rated and perceived infant stress (1-7; 7 = very stressful), perceived infant health (0-100; 100 = best imaginable health), and productivity impairment. Data were collected at hospital discharge through 1 month post-discharge. Caregiver responses indicated high stress levels, poor health, and productivity loss were reported at discharge; however, steady improvements were seen through 1 month post-discharge: caregiver-rated stress (from 6 to 2), infant stress (5 to 1), caregiver-perceived infant health (64 to 84), and productivity loss (mothers: 91% to 31%; fathers: 81% to 18%). Qualitative results indicated emotional impact, family routine disruption, financial concerns, and medical concerns persisted at 1 month post-discharge. This study found the caregiver burden of RSVH persists at least 1 month beyond discharge.
Background
Respiratory syncytial virus (RSV) is the leading cause of infant hospitalizations in the United States. 1 Children at greatest risk for severe RSV disease include preterm infants ≤35 weeks’ gestational age (wGA) as well as children ≤24 months of age with chronic lung disease of prematurity (CLDP) and hemodynamically significant congenital heart disease (HS-CHD).2,3 The preterm infant ≤35 wGA population constitutes the largest of these high-risk populations.
No vaccine is currently available to prevent RSV disease and there is no treatment to cure the disease. The only available option for prevention is seasonal RSV immunoprophylaxis (IP) with palivizumab, a humanized monoclonal antibody targeting the RSV F-protein. RSV IP has been shown to effectively reduce hospitalizations in high-risk preterm infants ≤35 wGA and children ≤24 months of age with CLDP and HS-CHD compared with placebo in randomized controlled trials.4-6
The American Academy of Pediatrics Committee on Infectious Diseases (COID) provides guidance on the use of RSV IP. In the 2014 update to this guidance, the COID no longer recommended the use of RSV IP in US preterm infants 29 to 35 wGA, except for those with other qualifying medical conditions, such as CLDP or HS-CHD. 7 Previously, the COID recommendations included all preterm infants born at <32 wGA and a subset of high-risk infants born at 32 to 35 wGA.8,9
The SENTINEL1 observational study provided insight into the impact of the guidance change by characterizing RSV-confirmed hospitalizations (RSVH) in US preterm infants born at 29 to 35 wGA who were not receiving RSV IP during the 2014-2015 RSV season. 10 RSVH, which among high-risk infants can frequently result in intensive care unit (ICU) admissions, 10 creates significant distress for the infants (eg, need for supplemental oxygen, impacts on functional status, and pain). Although there are studies that document the impact of hospitalization for any reason on caregivers and families, there is limited information on the experience of caregivers of infants hospitalized specifically for RSV disease.11-16 The aim of this research was to understand the impact of RSVH on high-risk preterm infants born at 29 to 35 wGA and their caregivers.
Materials, Subjects, and Methods
Study Design
This study was a secondary analysis of data collected during the SENTINEL1 study, a multicenter, noninterventional, observational cohort study of preterm infants 29 to 35 wGA and aged <12 months who were hospitalized for laboratory-confirmed RSV disease and who did not receive RSV IP (ClinicalTrials.gov identifier: NCT02273882). 10 Data were collected from October 1, 2014, through April 30, 2015, across 43 sites in the United States. Among the 702 infants with community-acquired RSVH identified in the SENTINEL1 study, a subset of 212 infants were enrolled for in-depth characterization of their RSV illness and to gain an understanding of infant and caregiver stress and infant health. An independent ethics committee/institutional review board approved the final study protocol, including the final version of the informed consent form and other written information and materials provided to the caregivers. Written informed consent was obtained for all enrolled participants in the study.
Measures
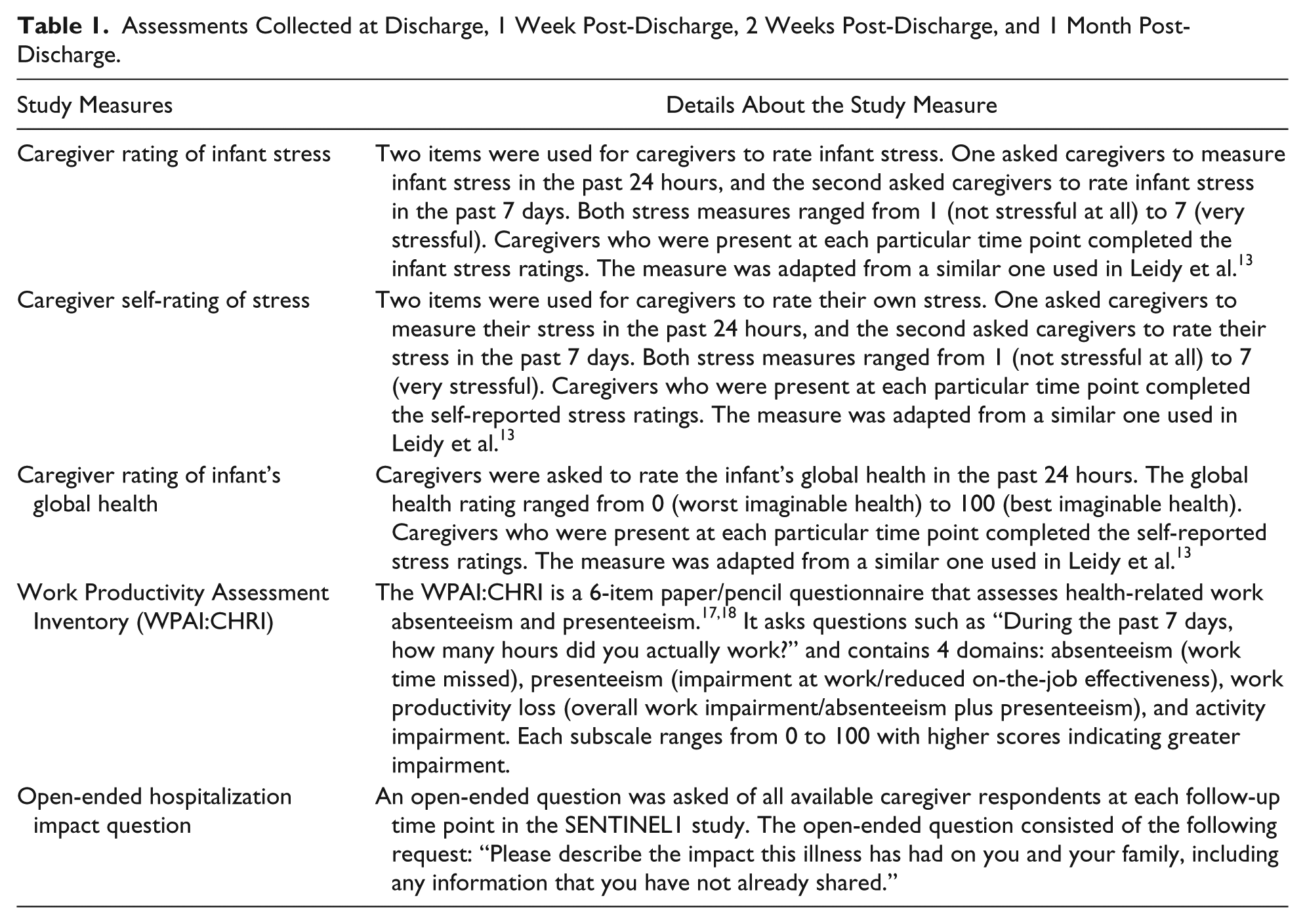
Sociodemographic and clinical data were collected for both infants and caregivers. Data were gathered from caregivers at RSVH discharge, 1 week post-discharge, 2 weeks post-discharge, and 1 month post-discharge. The caregivers completed multiple study measures including ratings of caregiver stress (during the past 24 hours and 7 days), caregiver’s perception of infant stress (during the past 24 hours and 7 days), and the caregiver’s perception of the infant’s current health (past 24 hours). 13 The Work Productivity Assessment Inventory in Caregivers of Children Hospitalized for Respiratory Illness (WPAI:CHRI) was also utilized to measure the effect of RSVH on caregiver work productivity and regular activities during the past 7 days (Table 1).17,18 Additionally, an open-ended question designed for the study was asked of each caregiver: “Please describe the impact this illness has had on you and your family, including any information that you have not already shared.” In general, the caregivers were asked this question at each time point, but for infants enrolled after their hospital discharge, caregivers were asked to retrospectively report this information.
Assessments Collected at Discharge, 1 Week Post-Discharge, 2 Weeks Post-Discharge, and 1 Month Post-Discharge.
Analytic Approach
Defining a Caregiver
“Caregiver” was defined as the infant’s mother, father, grandparent, or other adult family member. Consistent caregiver representation was not a prerequisite for analyses, resulting in varied caregiver appraisals over time. For example, there might have been one appraisal from a father at one time point and multiple caregiver appraisals (eg, mother, father, and grandmother) at other time points. Grandparent(s) and family member caregivers who were not the mother or the father were combined for analysis and listed as “other” caregivers. One infant had same-sex parents, so both caregivers were included in the mother cohort.
Quantitative Caregiver Assessments
Quantitative data were analyzed using SAS software version 9.4 (SAS Institute Inc, Cary, NC). Descriptive statistics (eg, mean, median, range, and standard deviation) were used to characterize the sample, including sociodemographic and clinical characteristics, the caregiver’s perception of their infant’s stress during the past 24 hours and past 7 days relative to each respective time point, the caregiver’s self-rating of stress during the past 24 hours and past 7 days, and the caregiver’s perception of their infant’s current health during the past 24 hours. Group means by caregiver type and time point for caregiver’s ratings of stress and health were analyzed. The WPAI:CHRI data were scored according to the developer’s manual.17,18 Not all caregivers provided data. Absenteeism, presenteeism, and overall work productivity loss were calculated for caregivers who were currently employed. Daily activity impairment was calculated for caregivers regardless of their current employment status.
Open-Ended Question About Hospitalization Impact
A thematic narrative analysis approach was used for the qualitative analysis. Thematic narrative analysis involves a systematic analysis of narratives with the goal of capturing patterns or themes. 18 All available data were used in the analyses, across all caregiver types. The caregiver comments were entered into an electronic data capture tool by clinic site staff in note form and subsequently transferred to a Microsoft Excel file for analysis; some comments were entered using first-person narrative and some in third-person narrative.
Comments were reviewed, impact themes were identified, and the data were coded by the identified themes. Themes were discussed among researchers and agreement on the codes was reached. Each line of data (ie, each infant’s caregiver comment by time point) was then coded using the themes. It should be noted that a single comment could have multiple themes assigned, and the data were not mutually exclusive to the themes. For example, the following quotation reported by the mother of a 34 wGA infant at discharge was coded with both Emotional Impact and Routine Disruption: “Huge impact. We now are very aware and nervous about RSV. Very worried about his health. Running to the doctor every time he is sick now.” Themes were assigned, then, sorted by time point, caregiver type, infant gestational age group (29 to 32 wGA, 33 to 34 wGA, and 35 wGA), ICU admission status, and the need for invasive mechanical ventilation.
The qualitative data were quantified by counting the number of responses in each impact theme at each time point. The numerator was the number of coded responses in each impact theme; the denominator was the number of caregiver respondents.
Results
Sample
Among the 212 enrolled infants, 53% were males, 42% of infants were 29 to 32 wGA, 38% were 33 to 34 wGA, and 20% were 35 wGA. The majority of infants were White and not Hispanic. Additional infant characteristics and caregiver characteristics are presented in Tables 2 and 3, respectively.
Infant Characteristics.
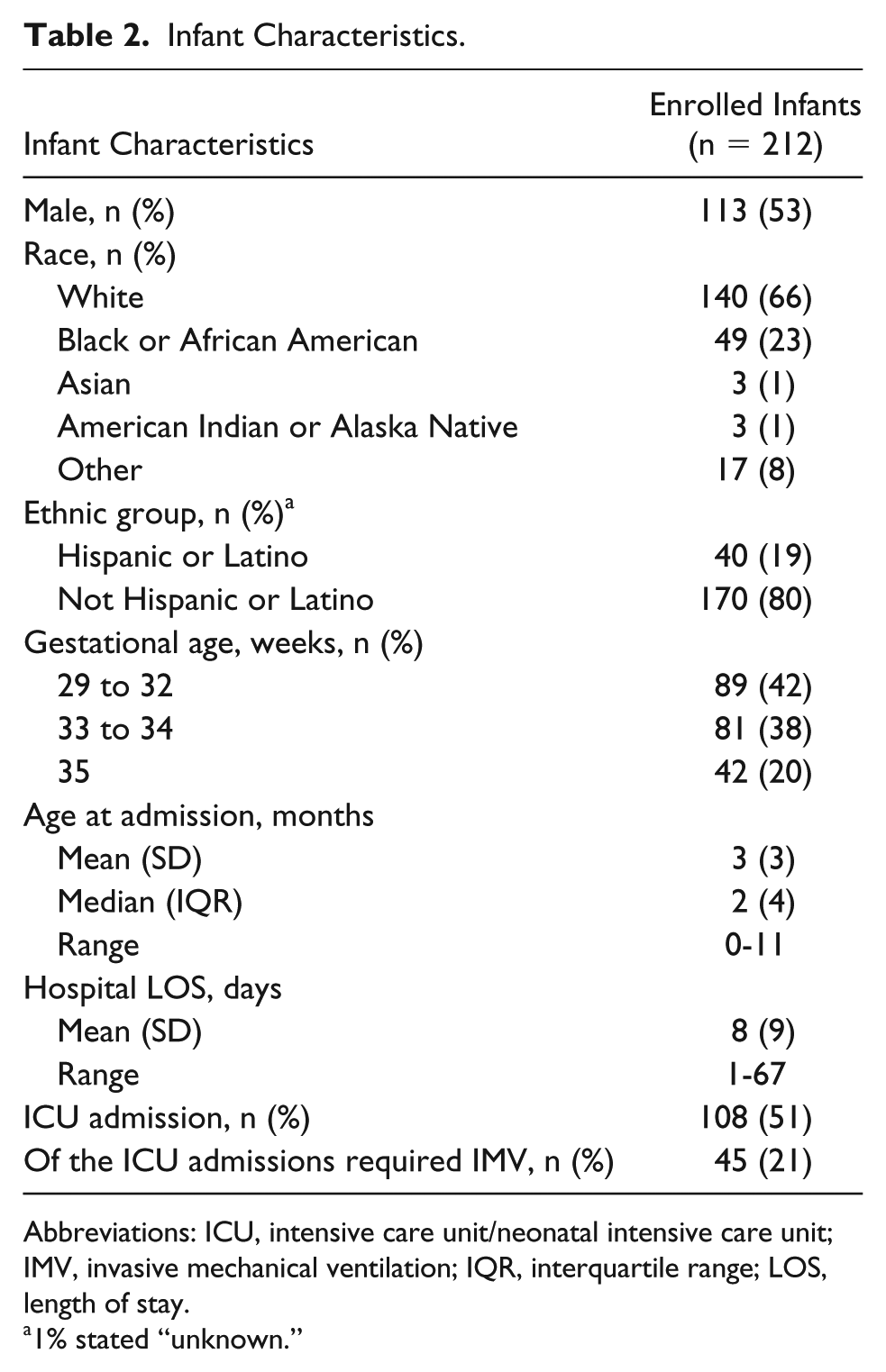
Abbreviations: ICU, intensive care unit/neonatal intensive care unit; IMV, invasive mechanical ventilation; IQR, interquartile range; LOS, length of stay.
1% stated “unknown.”
Caregiver Characteristics.
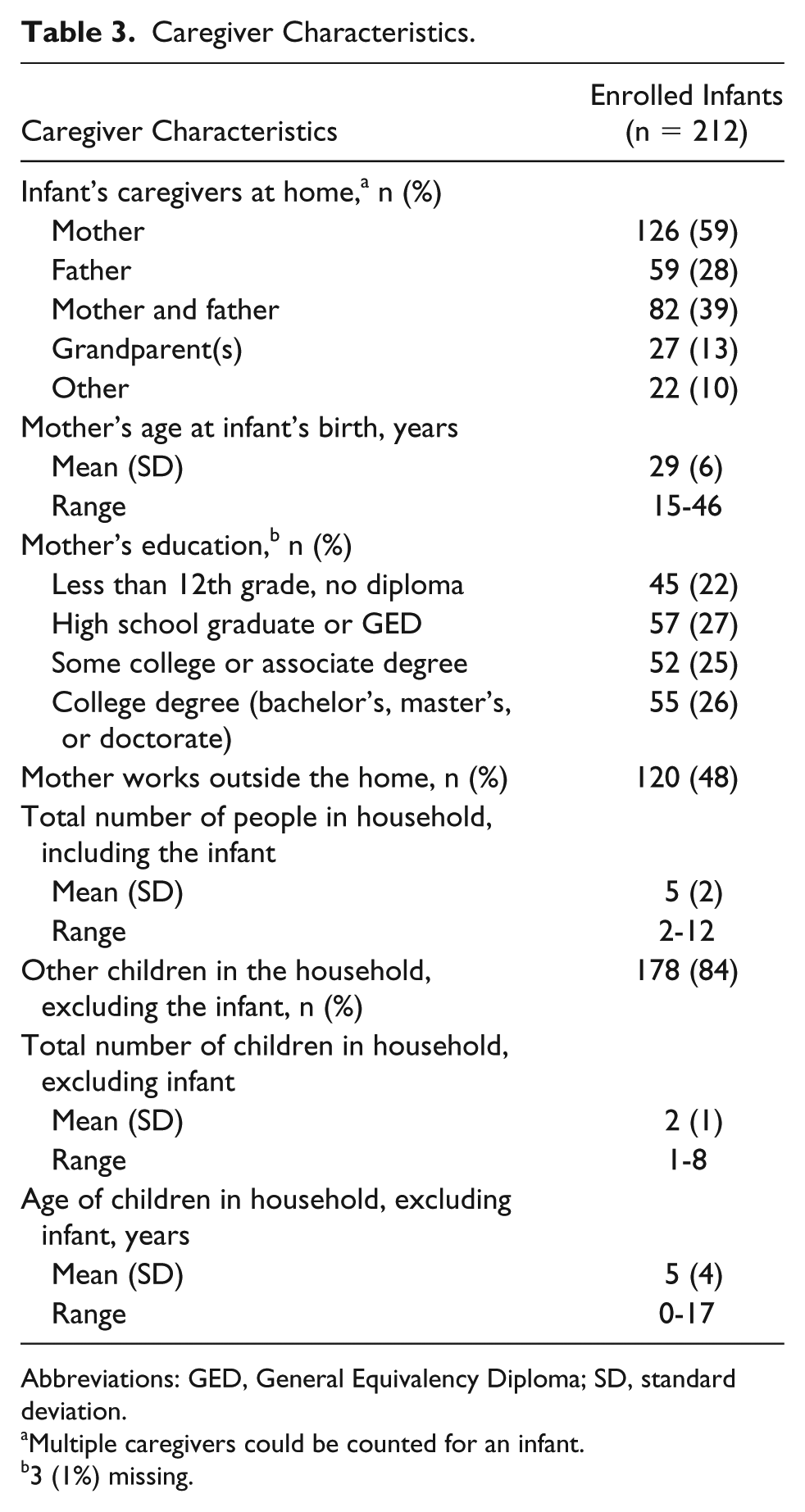
Abbreviations: GED, General Equivalency Diploma; SD, standard deviation.
Multiple caregivers could be counted for an infant.
3 (1%) missing.
Quantitative Caregiver Assessment Results
Although data from the sample of 212 infants’ caregivers were collected, some time points did not gain responses for all 212 infants. The number of caregivers providing a response at each time point is presented in Table 4. For example, at discharge, caregiver data about stress and health from 206 infants were reported.
Summary of Stress and Current Infant Health Over Time by Caregivers.
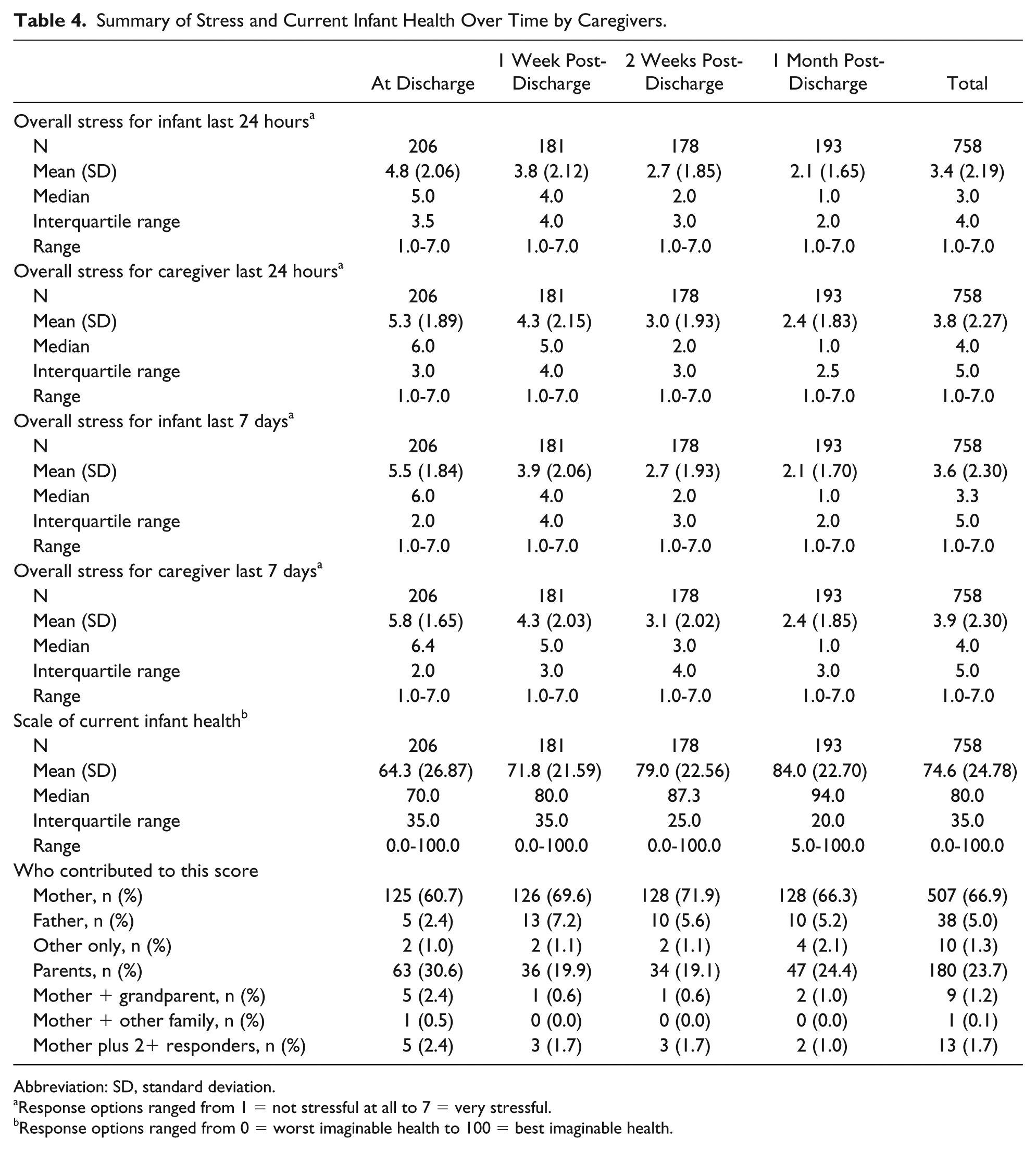
Abbreviation: SD, standard deviation.
Response options ranged from 1 = not stressful at all to 7 = very stressful.
Response options ranged from 0 = worst imaginable health to 100 = best imaginable health.
Infant’s Health and Stress Ratings
Descriptive results from the caregiver’s report about the infant’s stress, the caregiver’s stress, and the caregiver’s perception of the infant’s health are presented by time point in Table 4. Figure 1 illustrates caregivers’ perceptions of infants’ stress over the past 7 days and the caregiver’s self-reported stress over the past 7 days by time point. The mean stress reduced for caregivers and caregivers’ perception of infant stress over time. The stress for both was still present even 1 month post-discharge. The mean caregivers’ stress was consistently higher than the caregivers’ perception of infant stress over time.
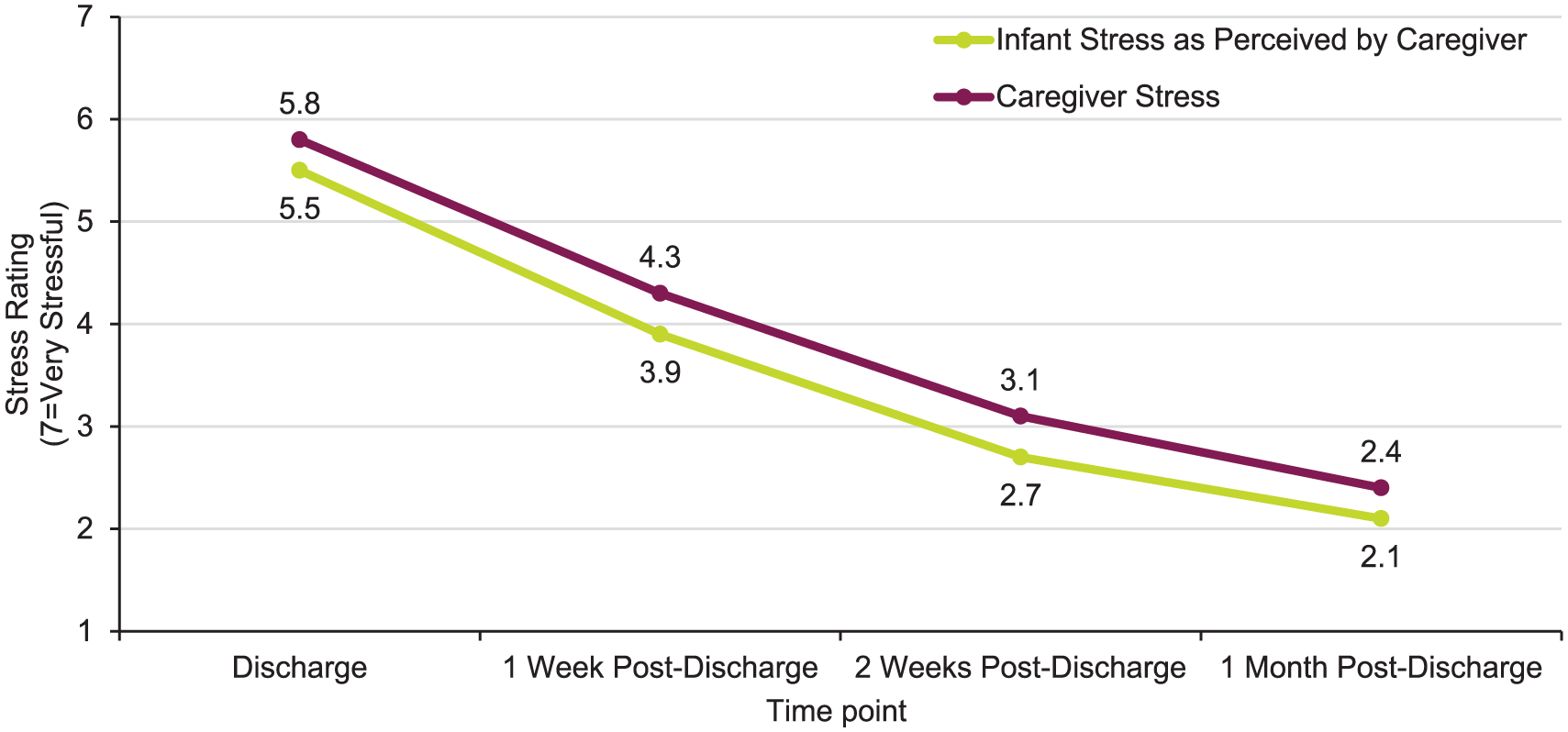
Caregiver rating of stress, past 7 days.
The caregivers’ perception of the infant’s current health improved after discharge and continued to improve to the 1 month post-discharge time point; caregivers reported a 20% improvement in the infant’s health from discharge to 1 month post-discharge (Figure 2). However, the caregivers’ mean health rating at 1 month post-discharge was not “best imaginable health.”
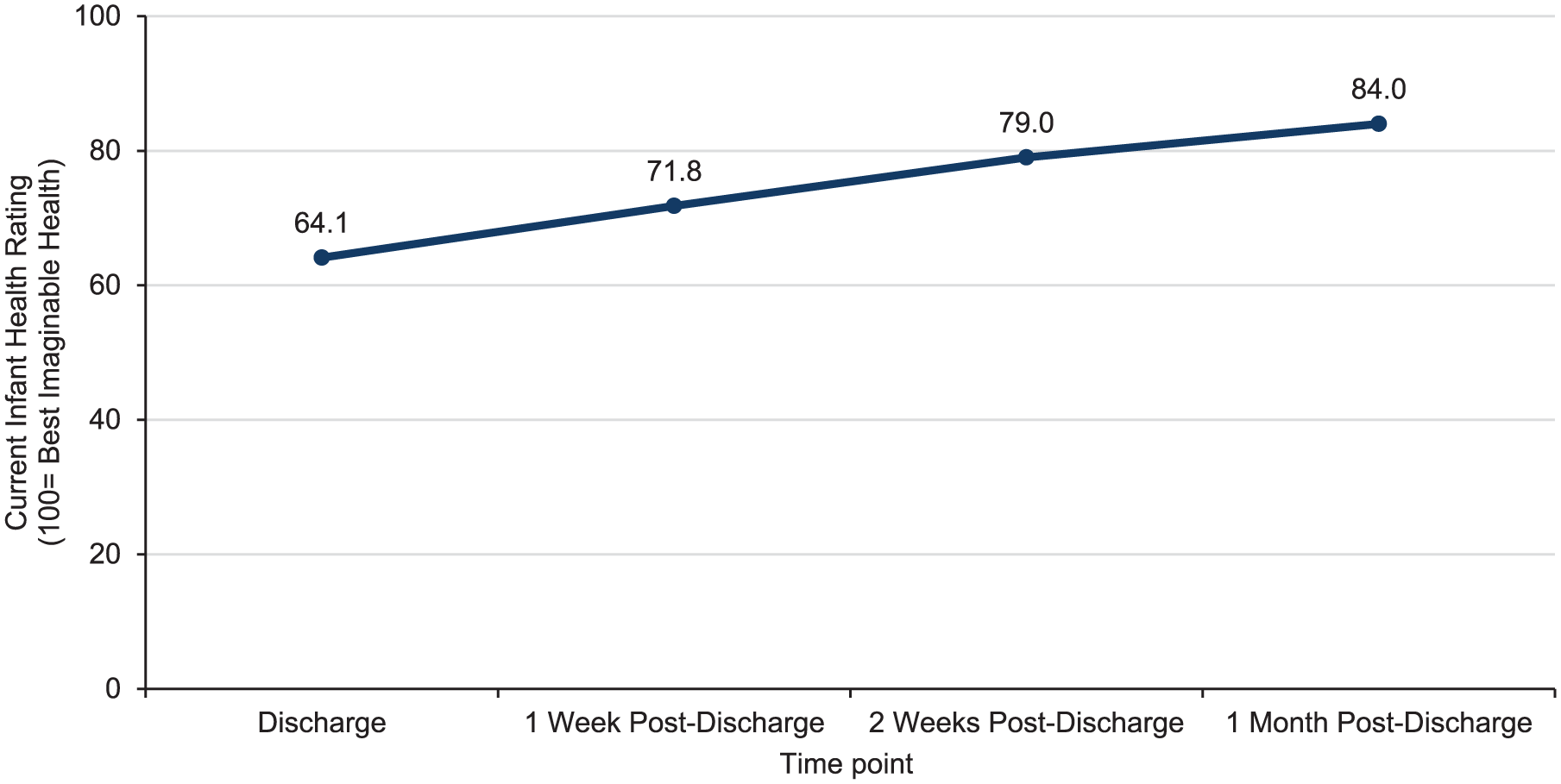
Caregiver rating of current infant health.
Work Productivity Assessment Inventory in Caregivers of Children Hospitalized for Respiratory Illness
As reported using the WPAI:CHRI, impacts on 4 types of productivity parameters (absenteeism, presenteeism, overall work productivity loss, and daily activity impairment) were seen among the sample of caregivers (Table 5 and Figure 3). At discharge, 73% of mothers and 58% of fathers reported absenteeism; at 1 month post-discharge, absenteeism declined for mothers and fathers (15% and 4%). This translated to employed mothers missing an average of 23, 14, 7, and 4 hours of work and employed fathers missing an average of 24, 9, 4, and 2 hours of work at discharge, 1 week, 2 weeks, and 1 month post-discharge, respectively. Presenteeism and daily activity impairment trended similarly for both mothers and fathers; however, mothers were more affected. Although the impact on overall productivity declined over time, productivity impacts were still present for all caregivers at 1 month post-discharge.
Work Productivity Assessment Inventory for Caregivers of Children Hospitalized for Respiratory Illness (WPAI:CHRI) a Results Mothers/Fathers.
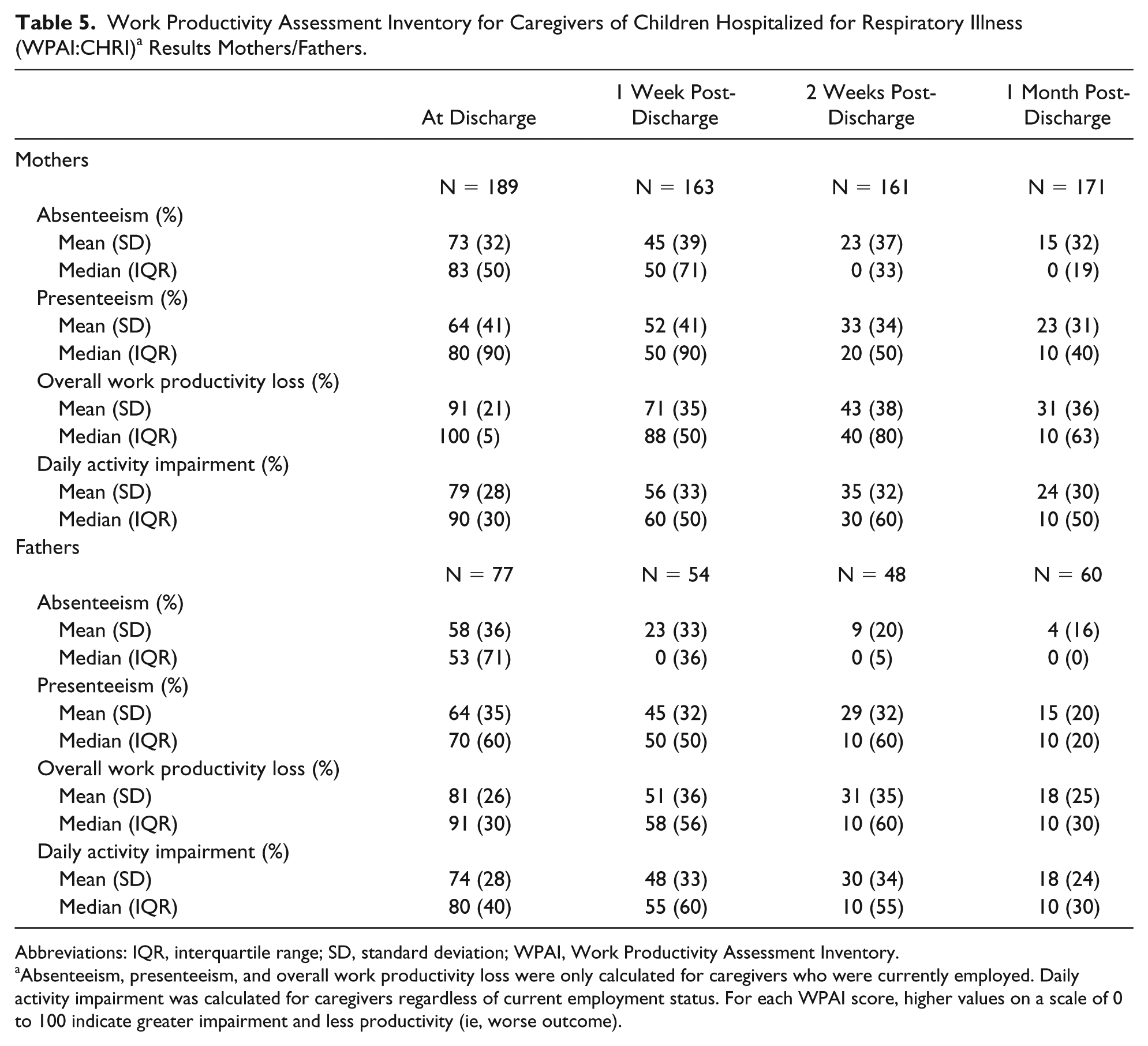
Abbreviations: IQR, interquartile range; SD, standard deviation; WPAI, Work Productivity Assessment Inventory.
Absenteeism, presenteeism, and overall work productivity loss were only calculated for caregivers who were currently employed. Daily activity impairment was calculated for caregivers regardless of current employment status. For each WPAI score, higher values on a scale of 0 to 100 indicate greater impairment and less productivity (ie, worse outcome).
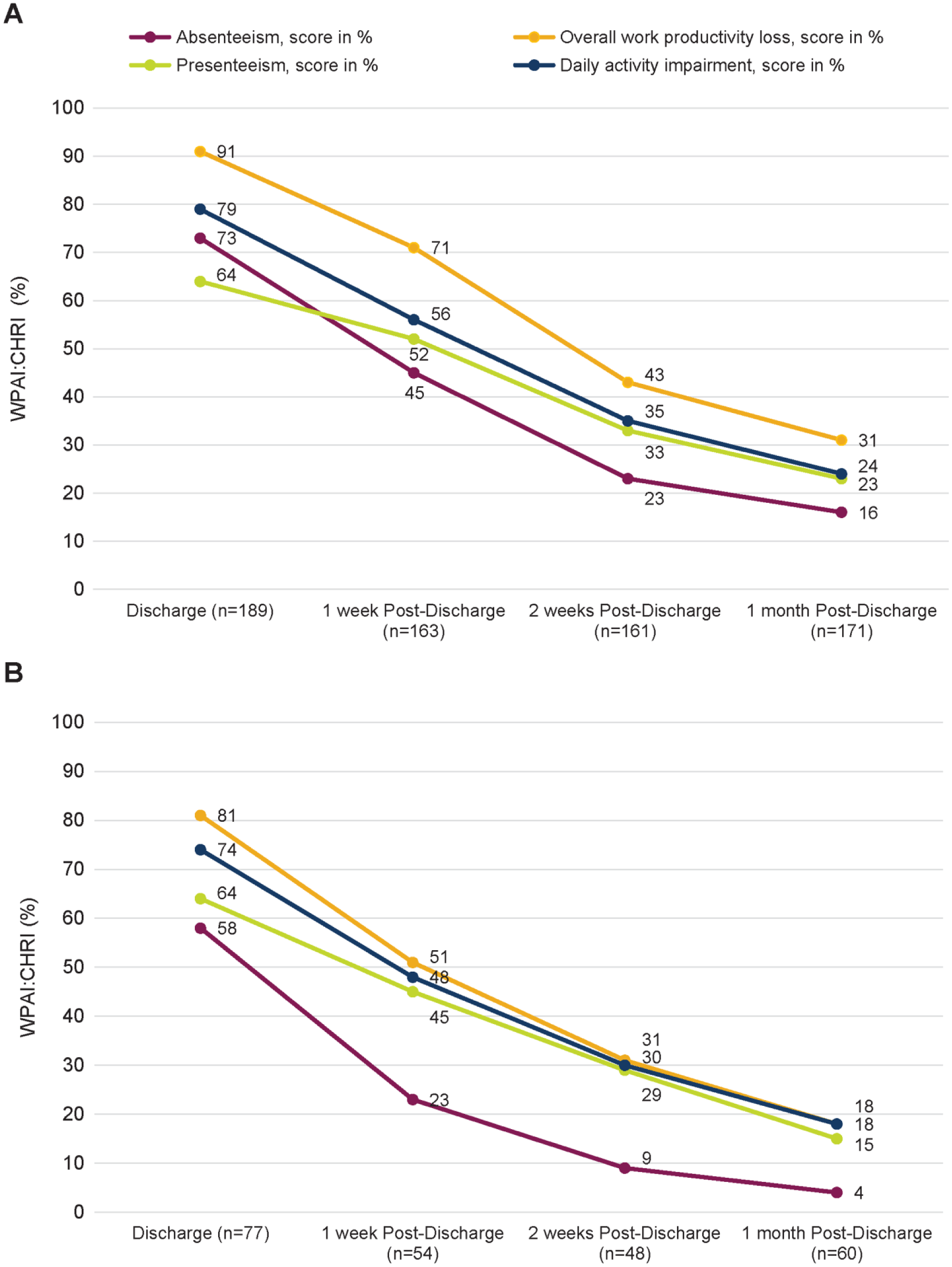
Work Productivity Assessment Inventory in Caregivers of Children Hospitalized for Respiratory Illness (WPAI:CHRI) results. Panel A, Mothers; Panel B, Fathers.
Caregiver Comments About Hospitalization Impact
From the open-ended question about hospitalization impact, there were a total of 974 comments across all caregiver types and all time points. After removing duplicate data, missing data, and comments that were equivalent to missing data (eg, “n/a,” “no comment”), there were 742 comments to review across the 4 time points. The comments were specific to an infant; multiple caregivers could have responded about the same infant.
At discharge, 235 total caregiver comments were recorded, and these comments could have been from multiple caregivers for the same infant. Post-discharge comments were also recorded: 174 comments at 1 week post-discharge, 151 comments at 2 weeks post-discharge, and 182 comments at 1 month post-discharge. Mothers of infants contributed the most comments. Specifically, the percentage of comments from mothers were 75% at discharge, 80% at 1 week post-discharge, 79% at 2 weeks post-discharge, and 78% at 1 month post-discharge. Fathers contributed 21% of comments at discharge, 18% at 1 week post-discharge, 18% at 2 weeks post-discharge, and 19% at 1 month post-discharge. Other caregivers provided 4% of comments at discharge, 2% at 1 week post-discharge, 3% at 2 weeks post-discharge, and 3% at 1 month post-discharge.
Nine themes characterizing the impact of RSVH on the caregiver were identified: emotional impacts; routine disruption/separation from other children; family relationship impacts; financial impacts; coordinating care; medical concerns; sleep/energy impacts; no impacts on the family; and miscellaneous comments. Additionally, some comments were grouped under the theme, “Better/infant back to normal.” The 742 comments were coded; themes were not mutually exclusive. A selection of caregiver comments by time point is presented in Table 6. The caregiver comments represented 86% of infants at discharge, 72% at 1 week post-discharge, 63% at 2 weeks post-discharge, and 73% at 1 month post-discharge. As a visual representation, Figure 4 presents the open-ended stress impacts by theme and time point for the combined caregiver responses. Emotional impacts (eg, stress, worry, and fear) were the most common theme reported among the comments for each time point. Emotional impacts were still being reported even at 1 month post-discharge. Disruption to the family routine (eg, needing to travel for medical visits), financial concerns, and medical concerns (eg, monitoring infant’s breathing) were also among the most frequently raised issues that persisted through 1 month post-discharge.
Select Caregiver Comments About Impact of Infant’s RSVH.
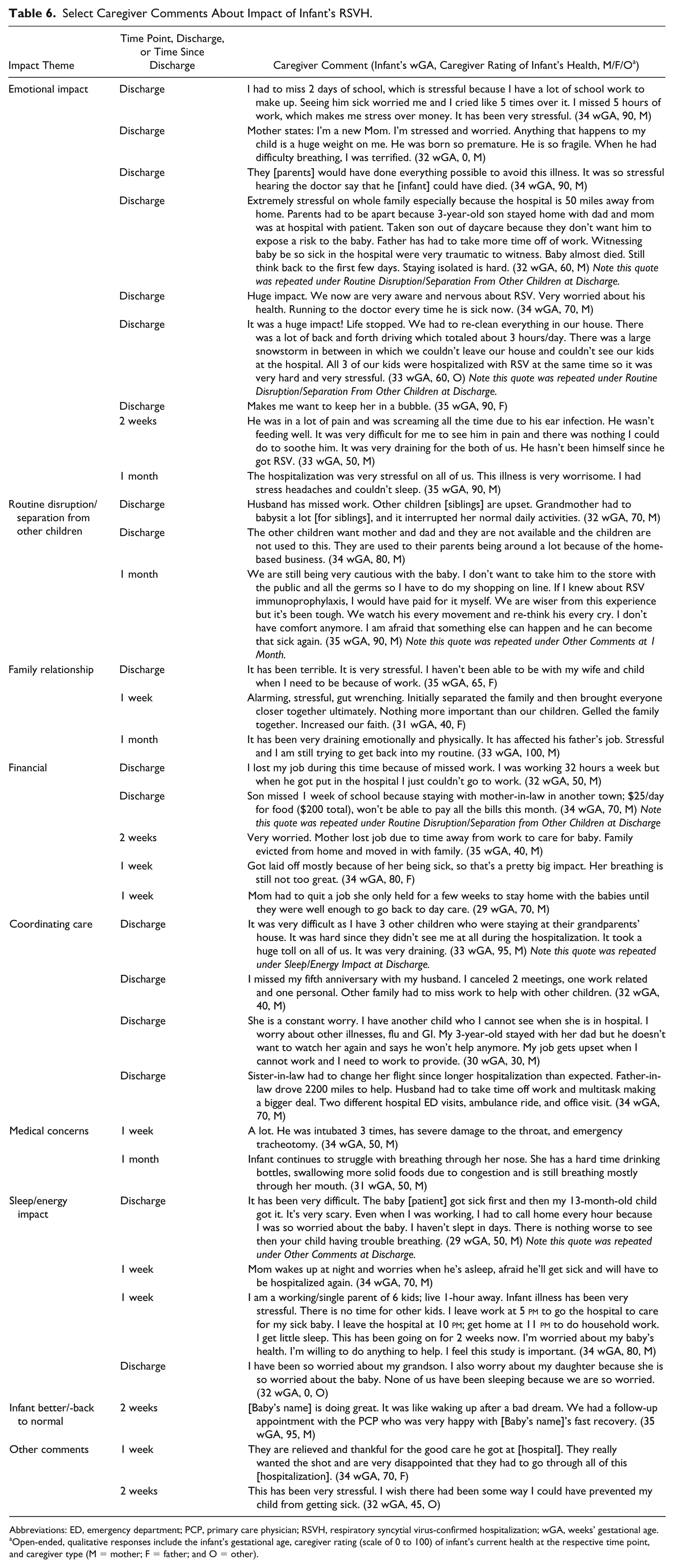
Abbreviations: ED, emergency department; PCP, primary care physician; RSVH, respiratory syncytial virus-confirmed hospitalization; wGA, weeks’ gestational age.
Open-ended, qualitative responses include the infant’s gestational age, caregiver rating (scale of 0 to 100) of infant’s current health at the respective time point, and caregiver type (M = mother; F = father; and O = other).
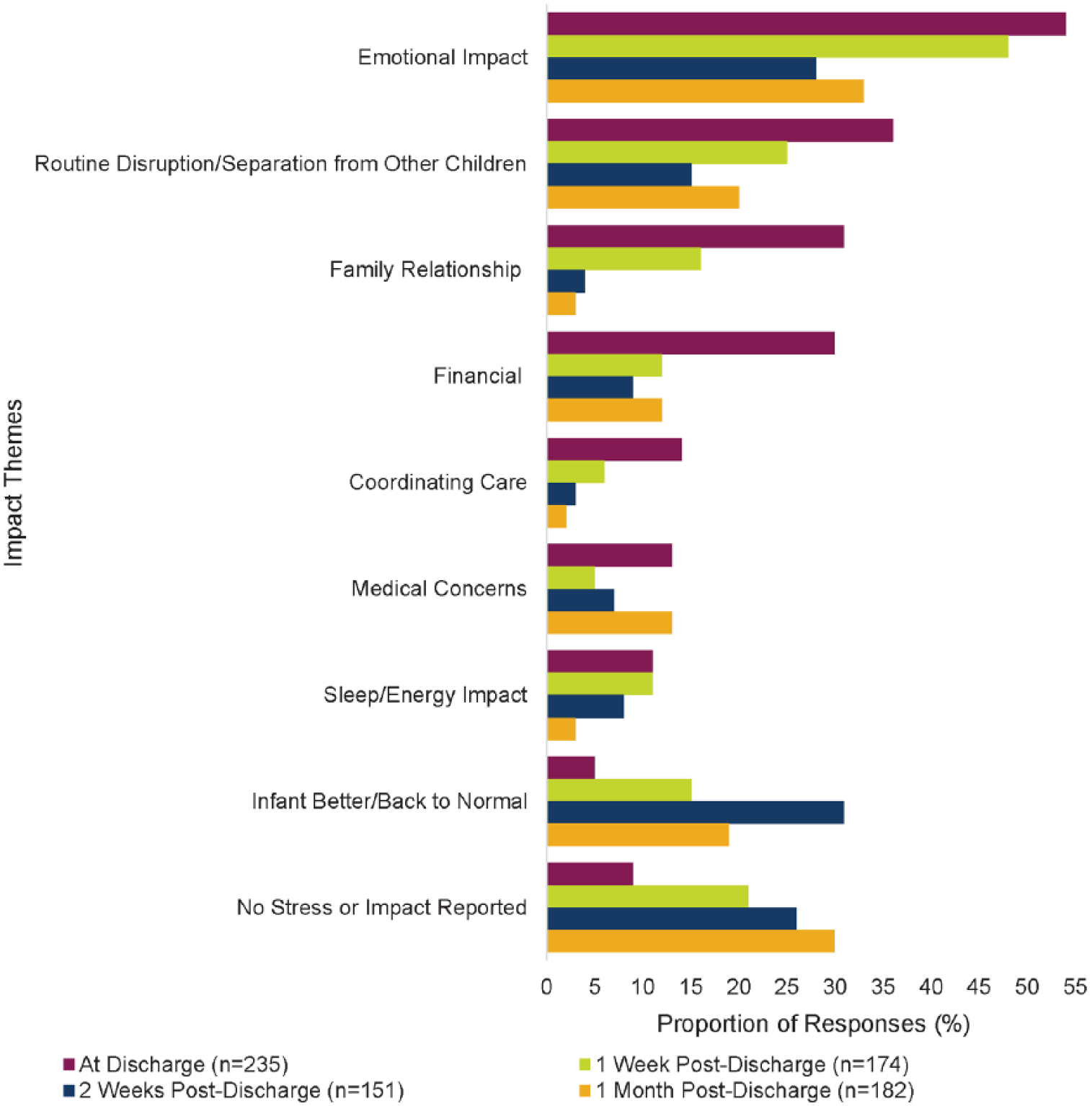
Caregiver-reported impact of infant’s RSVH. Caregiver responses could be grouped into multiple impact themes so the percentage at each time point will be >100%. More than one caregiver could provide responses for an infant.
Caregiver Comments by Infant Gestational Age
To explore potential caregiver impact differences by infant gestational age, all time points and all caregiver responses were combined and the proportions of themes by the gestational age of the infant were produced (Figure 5). The most frequently raised issues (emotional impact, routine disruption/separation from other children, medical concerns, financial impact, and family relationship impact) that were uncovered by time point were still the most highly endorsed when viewing the data by infant gestational age. There were some variations in caregiver responses by infant gestational age. For example, caregivers of infants 33 to 34 wGA reported a greater number of emotional impacts than caregivers of infants 29 to 32 wGA or 35 wGA. The caregivers of infants 29 to 32 wGA reported more disruptions to their routines than caregivers of infants in the other gestational age groups. Medical concerns were reported in similar frequency by caregivers in the 29 to 32 wGA and 33 to 34 wGA groups but much less in the 35 wGA group.
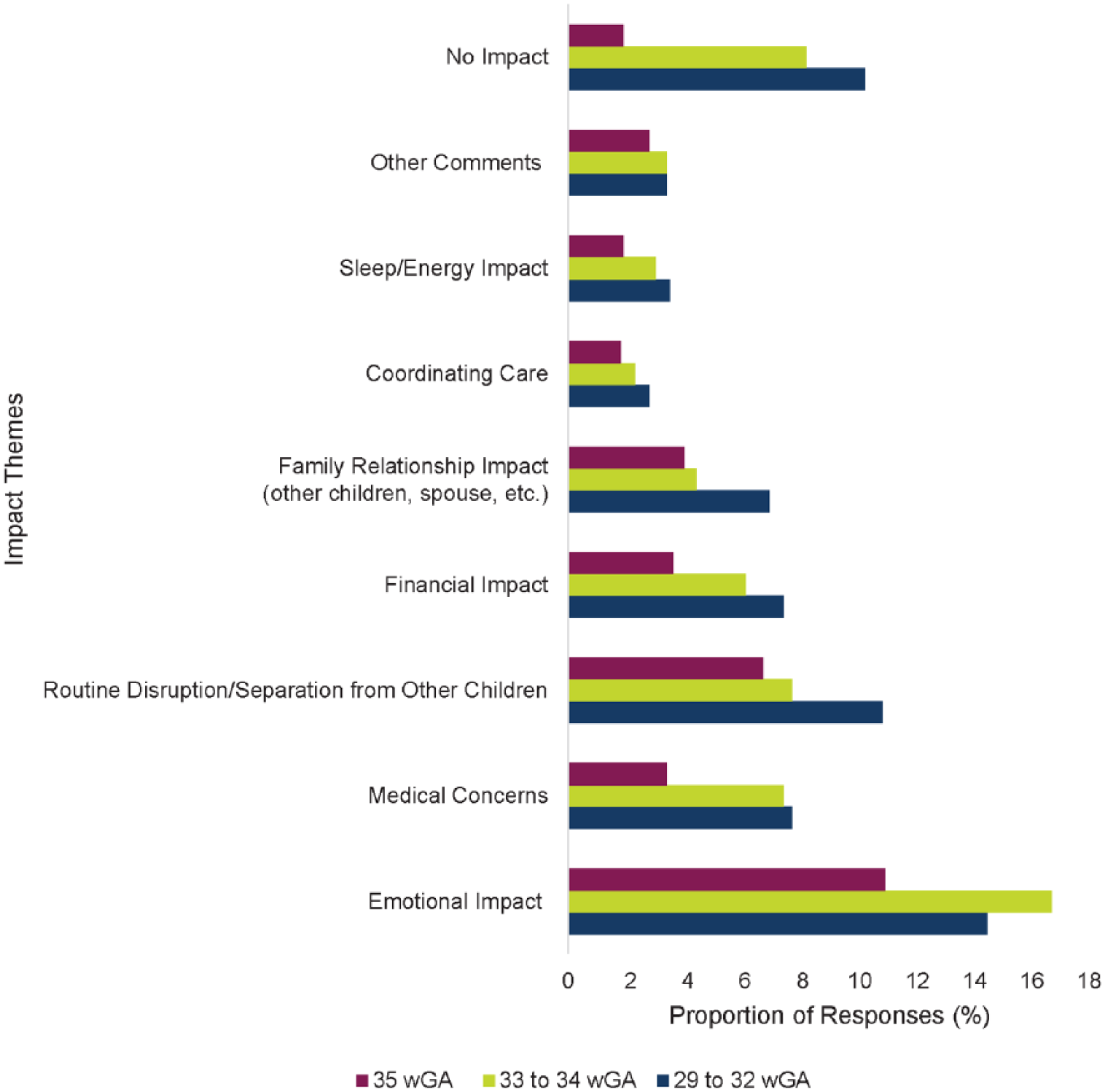
Caregiver-reported impact of infant’s RSVH by gestational age group. The caregiver comments by wGA (weeks’ gestational age) cohort included 311 caregiver comments from the 29 to 32 wGA group, 283 comments from the 33 to 34 wGA group, and 148 comments from the 35 wGA group.
Discussion
The SENTINEL1 observational study aimed to characterize the infant and caregiver experience of RSVH among families of preterm infants 29 to 35 wGA who did not receive RSV IP following the 2014 update of the COID guidance. 7 Caregivers of preterm infants hospitalized with confirmed RSV disease reported the highest levels of family and infant stress, absenteeism, presenteeism, and activity impairment at the time their infant was discharged from the hospital. Stress and impairment levels declined over time for all outcomes, but still persisted at 1 month post-discharge.
Leidy et al 13 studied the magnitude of infant and family stress associated with RSV-related hospitalization and included a control cohort. The control group was matched on infant age, similar geographic area, preterm birth, and recruitment from hospital pediatric or neonatal ICU records. The sample included 46 RSV infants and 45 control infants. The study found that caregiver distress persisted after the infant was discharged from the hospital. Although the levels of anxiety among the caregivers declined after the infants were discharged, the levels of caregiver anxiety were still significantly higher than the caregiver control anxiety levels after 2 months from discharge (P < 0.001). Our findings were similar, in that the levels of caregiver stress improved after the infant’s discharge but were still present 1 month later.
The caregiver comments support the quantitative findings from this study and provide a description of the impacts from the perspective of caregivers. The caregivers reported impacts on all areas of their daily lives, including missed work, disruption in their routines, separation from their other children, impacts on their family relationships, needing to coordinate care for their children, and financial impacts. Although caregiver stress, infant stress, and caregiver-perceived infant health improved over time, the caregivers continued to report impacts such as emotional stress, disruption to their daily routines, financial concerns, and infant health concerns at the 1 month post-discharge time point. These impacts are often difficult to measure quantitatively, but the factors impacting the caregivers, the magnitude of the impacts, and the lasting nature of these impacts on caregivers should be considered when evaluating the RSV disease burden in preterm infants.
The caregiver comments from this research provide caregiver perspective into previously published RSVH research. For example, Leader et al 19 studied time and out-of-pocket costs associated with RSVH. The research involved 36 full-term and 48 preterm infants (33 to 35 wGA). Caregivers were interviewed about their time and costs at discharge and 1 month post-discharge. The primary caregivers of the preterm infants reported an average total travel time of 6.8 hours (range = 0.13-48 hours) and an average of 133.6 hours in the hospital (range = 14-1080 hours). 19 The out-of-pocket expenses for the preterm cohort was an average of $643.69 ($21-$16 867; standard deviation = $2403). 19 The caregiver comments collected in this study illuminate quantified economic impact reports and present a humanistic quality to the caregiver’s experience.
Preventing severe RSV disease in this vulnerable preterm infant population could provide health benefits for the infants and avoidance of RSVH-related stress, as well as avoidance of stress and productivity loss for their caregivers. Our research quantifies the stress the caregivers were experiencing and their perception of the infant’s stress and includes qualitative data that have been systematically organized to summarize the caregiver burden. Caregiver stress should not be trivialized, particularly for caregivers of infants who were born preterm and may already be under stress from their newborn’s early arrival. Research among parents of hospitalized children from general pediatric wards shows elevated stress, which persisted after discharge. Franck et al 20 conducted a prospective study among 107 parents who had a child hospitalized for at least 3 nights. The parents completed a questionnaire during their child’s hospitalization and again 3 months post-discharge. Even at 3 months post-discharge, 32.7% of the parents reported some post-traumatic stress symptoms. 20 Another study, a meta-analysis of 13 studies, found that caregivers of children with chronic illness (asthma, cancer, cystic fibrosis, diabetes, epilepsy, juvenile rheumatoid arthritis, and/or sickle cell disease) had significantly higher general parenting stress than caregivers of healthy children (effect size d = 0.40, 95% confidence interval = 0.19-0.61, P ≤ .0001). 21 Although the cohort included in this research among preterm infants with RSVH is different from other studies of caregiver stress, the insights to the caregivers’ ongoing stress are enlightening. The qualitative data throughout the caregiver experience demonstrate an impact that should be considered for holistic treatment and RSVH indirect burden. The data from this research suggest that there is a burden of RSVH on caregivers that would be important to have represented when assessing the impact of RSV. Often economic modeling of preterm birth is limited to health care resource utilization and caregiver productivity lost due to the infant’s hospitalization. Hodek et al 22 suggest including intangible costs such as emotional distress and impacts on quality of life.
Unlike other countries, in the United States many mothers return to work when their infants are only a few weeks old, and they may not have the family support structure to help care for their newborns. A severe illness that results in hospitalization has many ramifications for the family, including inability of the parents to work. A substantial burden among caregivers was reported using the WPAI:CHRI and shown by the negative impact on absenteeism, presenteeism, daily activity impairment, and overall work productivity loss. The WPAI:CHRI scores at index RSVH discharge were higher for mothers compared with fathers, and this trend continued out to 1 month post-discharge. Notably, absenteeism scores indicated that fathers had far less absenteeism than mothers at 1 month post-discharge. A Canadian study by Mitchell et al 23 also showed lost work productivity for both parents associated with their infant’s RSVH. The study included 67 infants and 19.4% were preterm (born before 34.5 weeks). 23 The study revealed that average absenteeism was 49.0%, presenteeism was 51.4%, overall work impairment was 77.8%, and activity impairment was 81.7%. 23 Although working fathers experienced more absenteeism, presenteeism, and overall work impairment compared with working mothers, working mothers reported more activity impairment than working fathers. 23 In the Canadian study, only 9% of the mothers were employed or working at the time of the study. Although results cannot be directly compared, both the Canadian study and our study showed a negative impact on productivity for both mothers and fathers. The data from our research support the need for representation of the caregiver burden in decision-making for severe RSV disease.
There are several limitations to this study that should be noted. This research was observational, and no control group was included. The caregiver reports were collected by hospital research staff; therefore, verbatim quotations may not have been collected. Recall bias may be a factor as some caregivers reported their outcome information for all time points at 1 month post-discharge rather than at each time point as it occurred. Because the infants’ health and infant/caregiver stress levels improved over time, potential recall bias would likely be toward better health and less stress.
This research is consistent with previous findings reporting caregiver stress related to infant RSV-related hospitalization. 13 The qualitative reports from caregivers over time provide a unique contribution to the literature. Data directly from the caregiver’s perspective open a window to the degree and breadth of the impacts on the whole family. These impacts should be considered when evaluating RSV disease burden.
Conclusions
Preterm infant RSVH adversely affects caregivers, resulting in missed work, diminished work productivity, emotional stress, disruption of family routine, and financial concerns. The impact of RSVH continues through at least 1 month post-discharge and should be included in evaluations of RSV disease burden in preterm infants. Preventing severe RSV disease in this vulnerable population would provide health benefits for the infant while avoiding RSVH-related stress for these infants and their caregivers.
Author Contributions
All authors participated in data analysis and interpretation and contributed to the development of the manuscript. The authors maintained control over the final content of the manuscript.
Footnotes
Acknowledgements
This study was sponsored by AstraZeneca. The authors would like to thank the families for participating in the SENTINEL1 study, the hospital study teams for their research, Maxine Langenfeld, MPH, for her analysis support, and Nancy K. Leidy, PhD, of Evidera for her comments on earlier versions of this article. Editorial support was provided by The Lockwood Group, which was in accordance with Good Publication Practice (GPP3) guidelines and funded by AstraZeneca.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Robin Pokrzywinski and Laura Swett are employees of Evidera, a contract research organization that received funds from AstraZeneca to conduct these analyses. Pia Pannaraj has received personal compensation for research support from AstraZeneca/MedImmune during the conduct of the study, and research support from Pfizer. Jumi Yi has received personal compensation from AstraZeneca/MedImmune for participation in speaker bureau activities. Veena Kumar was an employee of AstraZeneca at the time the study was completed. Melissa Pavilack and Kimmie McLaurin are employees of AstraZeneca.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this secondary analysis of the SENTINEL1 data was provided by AstraZeneca (Gaithersburg, MD).