
Abstract
This study was conducted to assess the perception of US pediatric specialists of respiratory syncytial virus (RSV) disease risk and determine their clinical practices regarding immunoprophylaxis for high-risk children. Separate surveys were sent to neonatologists, pediatricians, pediatric pulmonologists, and pediatric cardiologists. Data were collected using structured questions requiring quantitative responses. Most neonatologists and pediatricians (>82.7%) reported a high clinical need for RSV immunoprophylaxis in preterm infants <32 weeks’ gestational age. Pediatric pulmonologists and pediatric cardiologists suggested that health conditions indicative of chronic lung disease of prematurity and hemodynamically significant congenital heart disease, respectively, confer eligibility for RSV immunoprophylaxis. Agreement with the changes in the 2014 American Academy of Pediatrics guidance for RSV immunoprophylaxis was mixed among respondents from the 4 specialties. Survey findings may provide a basis to improve education about risk for severe RSV disease and evaluate changes in physician use of RSV immunoprophylaxis based on the 2014 guidance.
Introduction
Respiratory syncytial virus (RSV) is the most common cause of bronchiolitis and pneumonia in infants and young children and is associated with substantial childhood morbidity. 1 Severe RSV disease, a major cause of hospitalization among infants and young children, is associated with an increased risk of respiratory morbidity during childhood.2,3 Therefore, the prevention of severe RSV disease is a key component of pediatric care among high-risk children. The American Academy of Pediatrics (AAP) provides guidance on appropriate preventive measures to help reduce the risk of RSV-related morbidity.4,5
Palivizumab is a monoclonal antibody that is the only product currently approved and licensed by the US Food and Drug Administration (FDA) to help reduce the risk of hospitalization attributable to severe RSV lower respiratory tract disease in high-risk children. 6 Palivizumab has been shown to significantly reduce the frequency of hospitalizations resulting from severe RSV disease in preterm infants (born at ≤ 35 weeks’ gestational age [wGA]) and high-risk children with bronchopulmonary dysplasia (BPD)/chronic lung disease of prematurity (CLDP) or hemodynamically significant congenital heart disease (HS-CHD).3,7 Palivizumab is FDA approved for use in preterm infants born at ≤ 35 wGA (≤ 6 months of age at the start of the RSV season), children ≤ 24 months of age who have BPD/CLDP, and children ≤ 24 months of age with HS-CHD. 6 The 2012 AAP guidance regarding RSV immunoprophylaxis included recommendations for use among preterm infants ≤ 34 wGA and children with BPD/CLDP or HS-CHD. 8 In July 2014, the AAP issued updated guidance for RSV immunoprophylaxis use among these high-risk patient groups. 4
Literature on the clinical use of palivizumab based on the AAP recommendations by pediatricians and pediatric specialists is limited. In particular, it is unclear whether all eligible preterm infants are recommended for RSV immunoprophylaxis by their physicians and whether at-risk children with high-risk pulmonary and cardiac conditions are recommended for RSV immunoprophylaxis by their medical care team. Furthermore, details regarding the specific pulmonary and cardiac conditions that physician specialists in practice consider as placing children at high risk for severe RSV disease are not well described. Finally, when immunoprophylaxis is not recommended by the physician, the reasons for not doing so remain unclear.
Objectives
Two surveys were developed and implemented to meet the following objectives. The primary objective of the initial survey was to characterize the current clinical practice regarding the provision of RSV immunoprophylaxis to at-risk children by neonatologists, pediatricians, pediatric pulmonologists, and pediatric cardiologists in the United States. Secondary objectives were (1) to determine which children currently considered to be at risk fell outside of the 2012 guidance and (2) to evaluate, via a follow-up survey, the perceived impact of the 2014 changes to the AAP guidance on the use of palivizumab by these general pediatric and pediatric subspecialty providers.
Methods
Study Design
Specialty-specific cross-sectional surveys were developed and administered online to neonatologists and pediatricians (online Appendix I, available at http://clp.sagepub.com/supplemental), pediatric pulmonologists (online Appendix II), and pediatric cardiologists (online Appendix III). Two surveys were developed for each specialty. The initial survey focused on practice patterns specific to the 2012 guidance and was administered in early 2014. Subsequent to the release of the updated guidance in July 2014, the follow-up survey was developed to understand how practice patterns would change with the new guidance and was administered in late 2014.
This study was conducted in accordance with the ethical principles in the Declaration of Helsinki and was consistent with International Conference on Harmonization Good Clinical Practice, Good Epidemiology Practices, and applicable regulatory requirements. Because this study did not involve the use of human subjects or protected health information, institutional review board approval was not required.
Target Population and Sample
All US physicians within the American Medical Association (AMA) database who self-identified as practicing neonatology, pediatric pulmonology, or pediatric cardiology were invited to participate in the initial survey. Because of the large number of pediatricians relative to subspecialists registered in the AMA database, a random sample of pediatricians was sent the invitation to reach the target sample size. Physicians who recommended RSV immunoprophylaxis for high-risk children were eligible to complete the survey. All potential respondents were invited to participate in the initial online survey by e-mail, with subsequent e-mail reminders sent to participants who did not complete the survey after the initial invitation. Respondents who provided contact details in the initial survey were also invited to participate in the follow-up survey. All respondents received the option to accept an honorarium of $75 for the initial survey and an additional $25 for the follow-up survey.
For the initial survey, the overarching consideration for the sample size was the need to obtain responses from a large sample of physicians from each specialty, representing a broad array of practice types, years of clinical experience, and patient populations; therefore, usual sample size approaches for quantitative research were less applicable. The target sample size for the initial survey was up to 200 for each group of neonatologists, pediatricians, pediatric pulmonologists, and pediatric cardiologists; this number was selected to be consistent with a recent survey conducted among physicians exploring patient compliance with RSV immunoprophylaxis. 10 However, our potential sample size was ultimately limited by the number of individuals who registered with the AMA with valid e-mail addresses. For the follow-up survey, no separate sample size considerations were made, recognizing that they would be limited by the sample size of the initial survey.
Outcomes
Data were collected using a mix of structured and open-ended questions. Questions focused on a physician’s perceived risk of severe RSV disease and likelihood of recommending RSV immunoprophylaxis (based on 2012 AAP guidance) for children with specific clinical and patient characteristics. There was also a focus on how various clinical conditions of interest are defined and how those factors affect perceived eligibility. The survey aimed to assess the characteristics of children warranting RSV immunoprophylaxis according to specialty; specifically, this included preterm infants without CLDP or congenital heart disease (CHD) for neonatologists and pediatricians; children with CLDP for pediatric pulmonologists; and children with HS-CHD for pediatric cardiologists. Clinical practice was assessed by tabulating the number and percentage of preterm infants (without CLDP or CHD) who were reported by neonatologists and pediatricians to have been recommended for, or who received, RSV immunoprophylaxis and the frequency of recommendation of RSV immunoprophylaxis according to high-risk conditions in young children with CLDP and HS-CHD among pediatric pulmonologists and pediatric cardiologists, respectively.
The follow-up survey focused on understanding the specialists’ perceptions of the impact of the updated 2014 AAP guidance on the eligibility of children currently recommended for immunoprophylaxis and of other potential impacts of the new guidance changes on clinical practice.
Analytical Methods
Survey responses were analyzed separately according to specialty type. When data were available, the distribution of respondent characteristics was compared with the distribution of those characteristics in the overall AMA population. 10 Among neonatologists and pediatricians, the percentage of preterm infants (without CLDP or CHD) for whom RSV immunoprophylaxis was recommended and who were reported to have received at least 1 dose was evaluated, as were the frequencies with which respondents ranked the clinical need for RSV immunoprophylaxis for each gestational age category. Frequencies with which pediatric pulmonologists and pediatric cardiologists responded that selected health conditions: (1) are indicative of CLDP or HS-CHD, respectively; (2) place children at high risk of severe RSV disease; and (3) confer eligibility for RSV immunoprophylaxis were tabulated. For pediatric cardiologists, the proportion of physicians who recommended RSV immunoprophylaxis following surgery with cardiopulmonary bypass was also calculated. Summarized data about respondents and their practice characteristics were presented both in the aggregate and stratified by demographic and clinical characteristics.
For the follow-up survey, respondents were asked to agree or disagree with specific changes in the 2014 AAP guidance and to rate on a scale of 1 (not at all) to 5 (absolutely) whether supporting data justified the changes. A thematic analysis was performed to tabulate respondents’ free-text responses as to whether and how they thought changes to the AAP guidance would affect their day-to-day practice.
Results
Respondent/Practice Characteristics
For the initial survey, all neonatologists (n = 4544), pediatric pulmonologists (n = 1010), and pediatric cardiologists (n = 2382) as well as a random sample of pediatricians (n = 7311) were contacted; demographic and practice characteristics of the 203 neonatologists, 138 pediatricians, 58 pediatric pulmonologists, and 156 pediatric cardiologists who completed the survey are presented in Table 1. The sex and geographic distribution of respondents matched well with the corresponding available AMA data obtained from the overall population of these specialists in the United States. 10 Approximately one-third to half of respondents from each specialty had graduated in the past 10 years. Most pediatric pulmonologists (70.7%) and pediatric cardiologists (69.9%) practiced at a medical school–based teaching hospital, whereas more than half the neonatologists (52.2%) and most pediatricians (81.9%) did not. Of the initial survey respondents who provided contact details, 175 neonatologists, 127 pediatricians, 52 pediatric pulmonologists, and 118 pediatric cardiologists were sent follow-up surveys. Among them, 107 (61.1%) neonatologists, 83 (65.4%) pediatricians, 36 (69.2%) pediatric pulmonologists, and 58 (49.2%) pediatric cardiologists completed the follow-up survey. A schematic of the number of physicians who were invited, initiated, and completed each of the surveys is provided in online Appendix IV (http://clp.sagepub.com/supplemental).
Respondents and Practice Characteristics.

Abbreviations: CLDP, chronic lung disease of prematurity; HS-CHD, hemodynamically significant congenital heart disease; NICU, neonatal intensive care unit; RSV, respiratory syncytial virus; wGA, weeks’ gestational age.
Among neonatologists, the highest levels of nursery service were as follows: Level 1 (ie, normal care nursery), n = 1 (0.5%); Level 2 (ie, continuing care nursery), n = 3 (1.5%); Level 3 (ie, intermediate care nursery), n = 62 (30.5%); and Level 4 (ie, intensive care nursery), n = 137 (67.5%).
Based on American Medical Association classification: Northeast: NJ, NY, PA, CT, ME, MA, NH, RI, VT; North Central: IL, IN, MI, OH, WI, IA, KS, MN, MO NE, ND, SD; South: AL, KY, MS, TN, DE, DC, FL, GA, MD, NC, SC, VA, WV, AR, LA, OK, TX; West: AZ, CO, ID, MT, NV, NM, UT, WY, AK, CA, HI, OR, WA.
Responses may sum to >100%.
Responses available from the 107 neonatologists who completed the follow-up survey.
CLDP for pediatric pulmonologists and HS-CHD for pediatric cardiologists.
Current Clinical Practice (Based on 2012 AAP Guidance)
Data on current clinical practice regarding the provision of RSV immunoprophylaxis to at-risk children by neonatologists, pediatricians, pediatric pulmonologists, and pediatric cardiologists in the United States are presented in Tables 2 and 3 and Figures 1 and 2.
Survey Responses by Pediatric Pulmonologists (n = 58) Regarding Specific Conditions in Children With CLDP.
Abbreviations: CLDP, chronic lung disease of prematurity; RSV, respiratory syncytial virus.
Survey Responses by Pediatric Cardiologists (n = 156) Regarding Specific Conditions in Children With CHD.
Abbreviations: HS-CHD, hemodynamically significant congenital heart disease; RSV, respiratory syncytial virus.
The percentage of preterm infants (without CLDP or CHD) during the most recent RSV season for whom RSV immunoprophylaxis was recommended and who received ≥1 dose of RSV immunoprophylaxis; by gestational age, according to (A) neonatologists and (B) pediatricians.

Ratings of clinical need for RSV immunoprophylaxis (1 = no need; 5 = very high need) as stratified by GA, for neonatologists (n = 203) and pediatricians (n = 138). For each rating category, the percentage of the total number of respondents is given.
The percentage of preterm infants who were recommended for and received RSV immunoprophylaxis by neonatologists and pediatricians varied based on gestational age and the infant’s chronological age at the start of the RSV season (Figure 1). Younger preterm infants were more likely to have been recommended for and to have received RSV immunoprophylaxis compared with older preterm infants. Physicians of both specialties reported that most (range = 51.1%–94.8%) preterm infants <32 wGA were recommended for and received RSV immunoprophylaxis during the most recent RSV season. Whereas most (range = 61.0%–76.1%) preterm infants born at 32 weeks, 0 days’ gestation through 34 weeks, 6 days’ gestation who were <3 months of age at the start of the RSV season with ≥1 AAP 2012 risk factor also were recommended for and received RSV immunoprophylaxis during the last RSV season, a smaller proportion of infants without risk factor(s) in this GA category (range = 9.5%–26.5%) or who were of older chronological age (3 to <6 months) with 1 or more risk factors (range = 34.9%–48.1%) were recommended for or received RSV immunoprophylaxis. Infants born at 35 wGA who were 3 to <6 months of age at the start of the RSV season with ≥1 AAP 2012 risk factor were least frequently (range = 6.2%–17.0%) recommended for or received RSV immunoprophylaxis.
Generally, neonatologists and pediatricians reported that younger preterm infants have a greater clinical need for RSV immunoprophylaxis than older preterm infants. The frequencies with which neonatologists and pediatricians ranked the clinical need (on a scale of 1 = no need to 5 = very high need) for RSV immunoprophylaxis by wGA are presented in Figure 2. For most infants born at <32 wGA, except those born at 29 to 31 wGA who were 6 to <12 months of age at the start of the RSV season, >82.7% of neonatologists and pediatricians reported a high clinical need (rank of ≥4) for RSV immunoprophylaxis. For most infants born at 32 through 34 wGA, >77.4% of neonatologists and pediatricians reported the clinical need for RSV immunoprophylaxis to be low (rank of ≤ 3), unless the infant was <3 months old at the start of the RSV season or had ≥1 risk factor consistent with the 2012 AAP guidance. For infants born at 35 wGA, >84.3% of neonatologists and pediatricians also reported the clinical need for immunoprophylaxis to be low.
Pediatric pulmonologists reported, on average, that the most prevalent condition among those with CLDP within their practice was the use of medical therapy (ie, supplemental oxygen, bronchodilator, diuretic, and/or corticosteroid) at the start of the RSV season (58.0%) or within 6 months of the start of the RSV season (60.7%). Generally, pediatric pulmonologists believed that most of the health conditions specified in the survey were indicative of CLDP and put the child at high risk of severe RSV disease, thereby conferring eligibility for RSV immunoprophylaxis (Table 2). Opinions were inconsistent as to whether having feeding difficulties caused by breathing problems, poor growth or weight gain caused by breathing problems, gastroesophageal reflux with breathing difficulties, prior mild to moderate respiratory illness, and comorbid cardiac conditions specifically at the start of the RSV season put a child at high risk for severe RSV disease sufficient to warrant RSV immunoprophylaxis (Table 2).
Pediatric cardiologists reported, on average, that the most prevalent HS-CHD conditions within their practice were the use of medication to control congestive heart failure (35.6%) followed by cyanotic heart disease (26.3%). Similar to pediatric pulmonologists, most pediatric cardiologists believed that many of the health conditions specified in the survey were indicative of HS-CHD, put the child at high risk of severe RSV disease, and conferred eligibility for RSV immunoprophylaxis (Table 3). However, opinions among pediatric cardiologists were inconsistent as to whether prior severe respiratory illness and full/complete corrective cardiac surgery >3 months previously were indicative of HS-CHD, put the patient at high risk for severe RSV disease, and were sufficient to warrant RSV immunoprophylaxis. Of note, although many respondents (39.7%) did not feel that prior severe respiratory illness in an infant or young child with CHD was indicative of HS-CHD, >80% indicated that they believed that such children were at high risk of severe RSV disease and would be eligible for immunoprophylaxis. Following surgery involving cardiopulmonary bypass, most pediatric cardiologists (87.2%) recommend postoperative RSV immunoprophylaxis as soon as the patient is medically stable. Among those who recommend a postoperative dose, 93.4% recommend restarting monthly doses if the RSV season has not yet ended.
Most neonatologists (78.3%), pediatricians (84.1%), and pediatric cardiologists (86.5%) did not think that there were additional patient groups (not recommended under the 2012 guidance) that should be provided RSV immunoprophylaxis. In contrast, more than half of the pediatric pulmonologists surveyed (58.6%) reported the need for inclusion of additional patient groups. Of those respondents who did report a need for additional categories, the most frequent patient types specified by neonatologists (n = 44) were those with congenital diaphragmatic hernia (65.9%) and cystic fibrosis (63.6%); by pediatricians (n = 22) were those with cystic fibrosis (81.8%), history of mechanical ventilation (77.3%), Down syndrome with CHD (72.7%), and early congestive heart failure (68.2%); by pediatric cardiologists (n = 21) were those who were expected to undergo surgery during the RSV season (52.4%) and those anticipated to develop HS-CHD (52.4%); and by pediatric pulmonologists (n = 34) were those with cystic fibrosis (79.4%), congenital anomalies of the respiratory system (79.4%), and congenital diaphragmatic hernia (67.6%).
Follow-up Survey Results Pertaining to the Updated 2014 AAP Guidance
Physicians’ agreement with the changes in the updated 2014 AAP guidance was mixed, and most did not feel that the scientific evidence strongly supported the changes. More than half of the neonatologists (53.3%) and pediatricians (60.2%) who completed the follow-up survey agreed with the change that infants born at 32 through 34 wGA with preschool-aged siblings or daycare attendance who are <3 months of age at the start of the RSV season are no longer recommended for RSV immunoprophylaxis; however, they did not feel strongly (mean ranking = 3.3 and 3.4, respectively [1 = not at all; 5 = absolutely]) that there was evidence to support that particular change (Table 4). Fewer neonatologists (37.4%) and pediatricians (32.5%) agreed that infants born at 29 through 31 wGA who are <6 months of age at the start of the RSV season should no longer be recommended for RSV immunoprophylaxis; they also did not feel strongly (mean ranking = 3.0) that the evidence supported this change. Most neonatologists (67.3%) and pediatricians (67.5%) reported that the updated guidance would lead to a change in their practice and that they would recommend immunoprophylaxis less frequently because fewer children would be eligible.
Survey Responses Among Neonatologists and Pediatricians Regarding Changed Guidance for RSV Immunoprophylaxis for Preterm Infants Without CLDP or CHD.
Abbreviations: CHD, congenital heart disease; CLDP, chronic lung disease of prematurity; RSV, respiratory syncytial virus; wGA, weeks’ gestational age.
Participants were asked to rank between 1 (not at all) and 5 (absolutely) whether they believed that the supporting data justified the change.
Most pediatric pulmonologists who completed the follow-up survey agreed with 2 of the changes in the 2014 AAP guidance: 75.0% agreed that CLDP is defined as <32 weeks, 0 days’ gestational age and a requirement for >21% oxygen for at least the first 28 days after birth; 69.4% agreed that the requirement for medical support during the 6-month period before the start of the second RSV season applies only to those in the second year of life (Table 5). However, pediatric pulmonologists did not feel strongly (mean ranking = 3.6 and 3.1, respectively [1 = not at all, 5 = absolutely]) that there was evidence to support these changes. Fewer respondents (38.9%) agreed that the updated definition of CLDP is the only criterion for determining whether an infant with CLDP should qualify for RSV immunoprophylaxis and did not feel strongly (mean ranking = 2.8) that the evidence supported this change. Fewer than half of pediatric pulmonologists (41.7%) reported that the change in the guidance would have a strong impact on their day-to-day practice and would change to whom they could recommend immunoprophylaxis.
Survey Responses Among Pediatric Pulmonologists (n = 36) Regarding Changed Guidance for RSV Immunoprophylaxis for Young Children With CLDP.
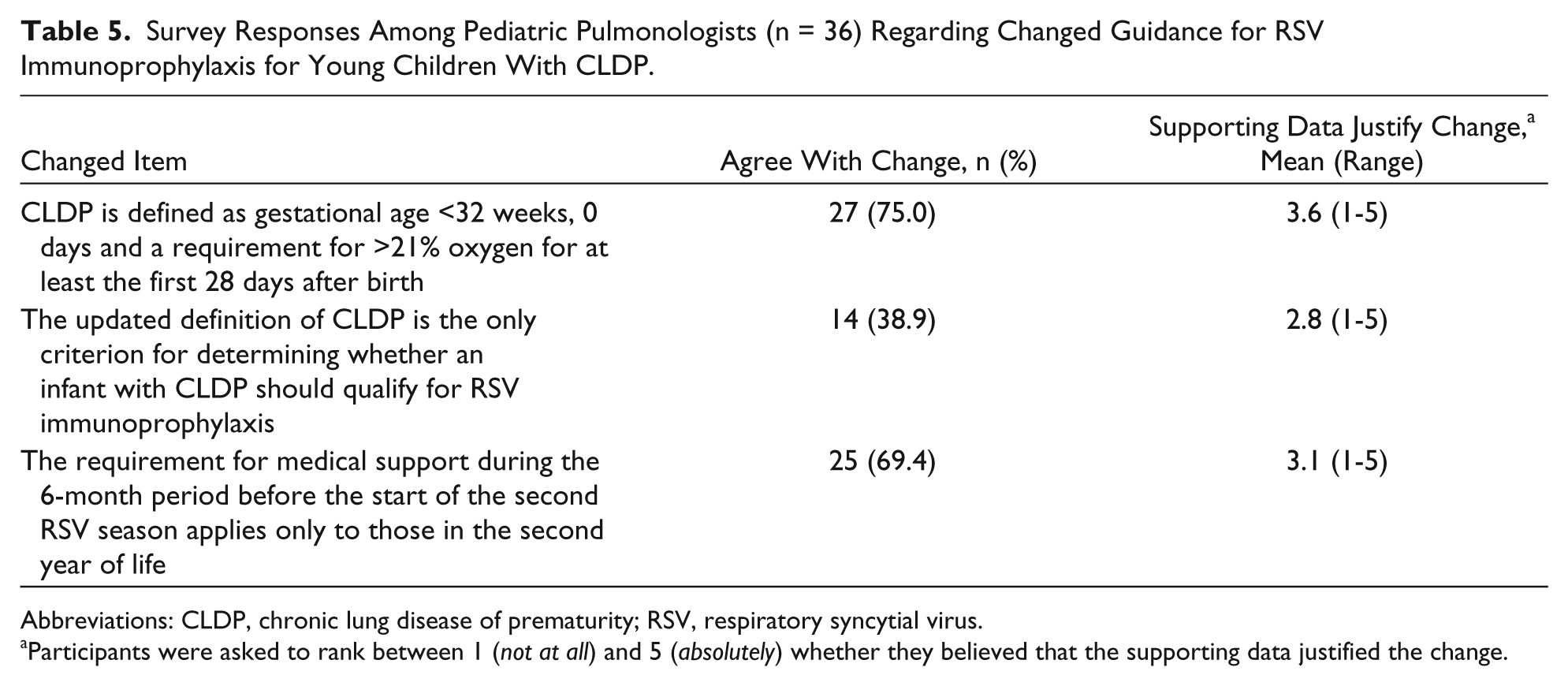
Abbreviations: CLDP, chronic lung disease of prematurity; RSV, respiratory syncytial virus.
Participants were asked to rank between 1 (not at all) and 5 (absolutely) whether they believed that the supporting data justified the change.
Finally, most pediatric cardiologists who completed the follow-up survey agreed with the following changes: children in the second year of life should not receive immunoprophylaxis (60.3%); decisions regarding immunoprophylaxis in children with cyanotic defects may be made in consultation with a pediatric cardiologist (91.4%); and children <2 years of age who undergo cardiac transplantation during the RSV season may be considered for RSV immunoprophylaxis (94.8%; Table 6). However, as with other pediatric groups, they did not feel strongly (mean ranking = 3.2, 3.6, and 3.8, respectively [1 = not at all, 5 = absolutely]) that there was evidence to support these changes. Fewer respondents (41.4%) agreed that children who are most likely to benefit from immunoprophylaxis include infants with acyanotic heart disease who are receiving medication to control congestive heart failure and will require cardiac surgical procedures and infants with moderate to severe pulmonary hypertension. They also did not feel strongly (mean ranking = 2.9) that the evidence supported this change. Fewer than half (39.7%) of pediatric cardiologists reported that the revised guidance would change their day-to-day practice, and fewer than one-third (31.0%) reported that they would recommend immunoprophylaxis less frequently because fewer children would be eligible.
Survey Responses Among Pediatric Cardiologists (n = 58) Regarding Changed Guidance for RSV Immunoprophylaxis for Young Children With HS-CHD.
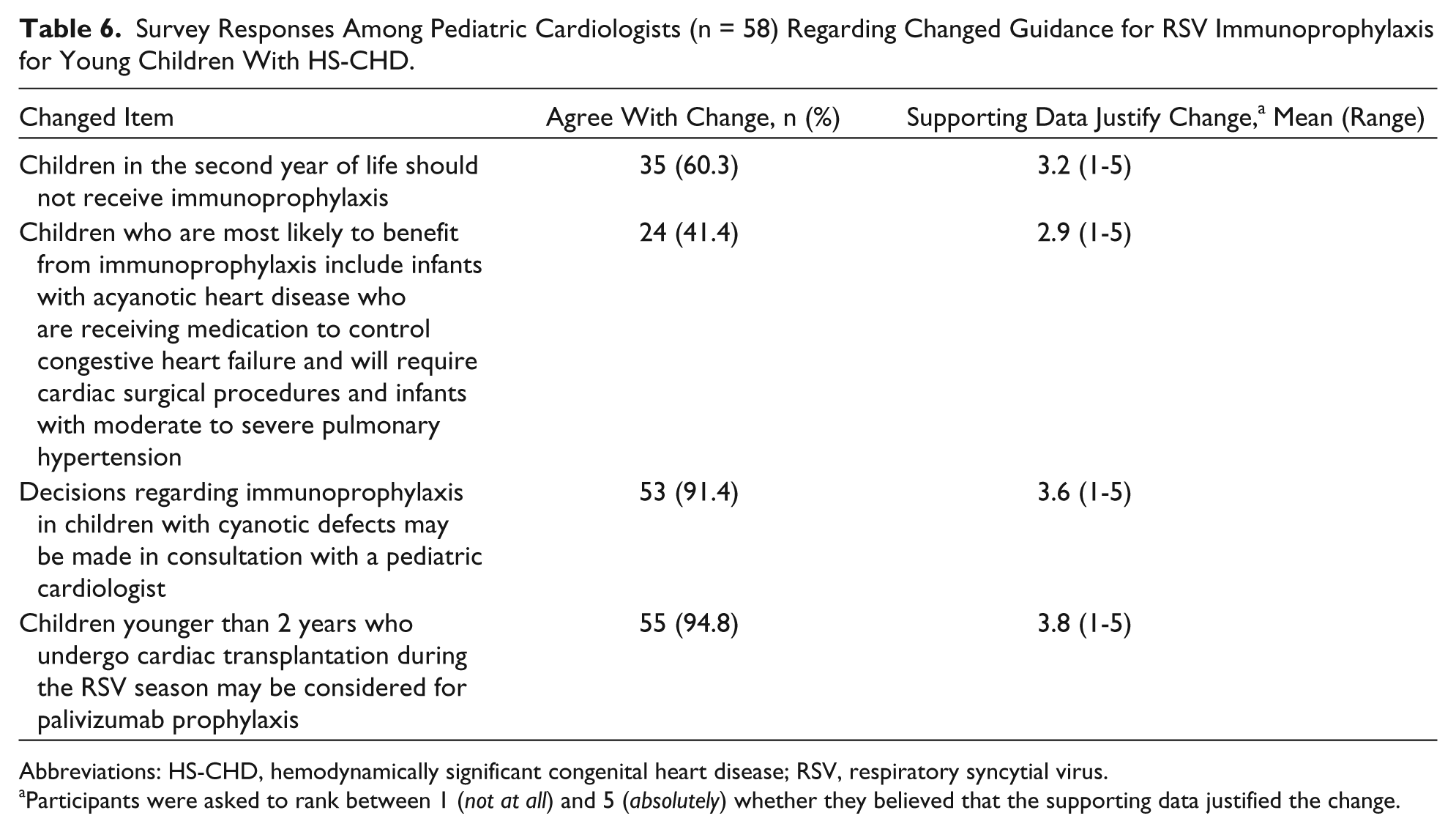
Abbreviations: HS-CHD, hemodynamically significant congenital heart disease; RSV, respiratory syncytial virus.
Participants were asked to rank between 1 (not at all) and 5 (absolutely) whether they believed that the supporting data justified the change.
Discussion
Palivizumab was first approved by the US FDA in 1998 for the prevention of serious lower respiratory tract infection caused by RSV in select children at increased risk of severe disease. 6 Immunoprophylaxis with palivizumab is currently recommended by the AAP to help prevent severe RSV disease in high-risk children in the United States 4 and has been widely accepted and incorporated into the routine clinical practice of US pediatric specialists who manage patients at high risk of severe RSV disease. The guidance has been reviewed at least every 3 years and updated periodically, based on a review of the prevailing literature. 4 The evolution of the guidance to date has the potential to convey conflicting messages to clinicians as they seek to understand the rationale for the changes and their clinical applicability.
Literature addressing recommendations by physicians for RSV immunoprophylaxis in the clinical setting is lacking. This study surveyed neonatologists, pediatricians, pediatric pulmonologists, and pediatric cardiologists to characterize the patterns of clinical practice regarding RSV immunoprophylaxis use for preterm infants and high-risk young children in the United States as well their views on the 2012 AAP guidance and the updated 2014 AAP guidance. The findings from the present study identify current practice patterns among not only pediatricians but also neonatologists, pediatric pulmonologists, and pediatric cardiologists. The data from this study can be used to inform pediatric specialists regarding prevailing common use of RSV immunoprophylaxis.
The initial survey results pre-date the release of the updated 2014 AAP guidance, thereby providing important information regarding the administration of palivizumab to high-risk children in the United States prior to release of the 2014 AAP guidance. The follow-up survey provides further insight into the perceptions of US pediatric specialists following the issuance of the 2014 AAP guidance. The findings from the initial survey showed that a large majority of neonatologists, pediatricians, pediatric pulmonologists, and pediatric cardiologists recommend RSV immunoprophylaxis for children at high risk for severe RSV disease, as described by the 2012 AAP guidance.
Neonatologists and Pediatricians
Neonatologists and pediatricians consistently reported that most preterm infants <32 wGA in their practice were recommended for and received RSV immunoprophylaxis during the most recent RSV season; there was less perceived need for immunoprophylaxis for infants born at 32 through 34 wGA who meet the 2012 AAP criteria, including those with ≥1 AAP 2012 risk factor (ie, childcare attendance or non–multiple-birth siblings <5 years of age). However, a large proportion of infants fall into this late-preterm category, and a substantial number of these infants are susceptible to severe RSV disease. Ambrose et al 11 demonstrated that RSV-related hospitalization rates were highest among infants 32 to 34 wGA and 35 wGA who were <6 months of age during the RSV season with ≥1 AAP 2012 risk factor (8.9 and 9.3 per 100 infant-seasons, respectively, vs 3.5 for all other infants, P < .001).
The practice patterns of neonatologists and pediatricians demonstrated by the initial survey may change based on the findings from the follow-up survey, which indicated that a substantial number of respondents believed that the changes outlined in the 2014 AAP guidance would affect their clinical practice. However, there was a notable lack of uniformity in agreement with many of the new recommendations. Among neonatologists and pediatricians, fewer than 60% agreed with the update that infants 32 through 34 wGA with risk factors should no longer receive immunoprophylaxis, and fewer than 40% agreed with the update that immunoprophylaxis should not be given to infants born at 29 through 31 wGA who are <6 months of age at the start of the RSV season.
Pediatric Pulmonologists and Pediatric Cardiologists
Based on the initial survey results, pediatric pulmonologists and pediatric cardiologists overwhelmingly favored immunoprophylaxis for children who had “well-established” clinical conditions that placed them at high risk for severe RSV disease, indicating widespread consensus for the generally accepted 2012 AAP recommendations that applied to their particular subspecialties. However, most pediatric pulmonologists and pediatric cardiologists were not in agreement with some of the changes listed in the 2014 AAP guidance. In addition, they were not convinced that the supporting data and literature cited in the guidance adequately supported these changes. This lack of consensus regarding the strength of supporting literature suggests that further studies may be necessary. 12 In contrast to neonatologists and pediatricians, most pediatric pulmonologists and pediatric cardiologists reported that the updated guidance would not change their day-to-day practice.
Clinical Practice Beyond the AAP Guidance
In addition to the populations eligible to receive RSV immunoprophylaxis in the 2012 AAP guidance, there were a number of other important health conditions that pediatric specialists felt might place a child at high risk for severe RSV disease and/or warrant use of immunoprophylaxis. Findings from this survey suggest that pediatricians and pediatric subspecialists felt comfortable recommending the use of RSV immunoprophylaxis to patients not included in the 2012 or 2014 AAP guidance. For instance, cystic fibrosis was reported by neonatologists, pediatricians, and pediatric pulmonologists as a high-risk condition that, although not presently recommended for RSV immunoprophylaxis, should be. This recommendation is consistent with findings from previous studies showing that RSV contributes to early lung injury among infants with cystic fibrosis and that it is the leading pathogen among children with cystic fibrosis hospitalized for persistent or severe respiratory disease. 13 Similarly, pediatric specialists suggested use in children who have a history of mechanical ventilation, Down syndrome with CHD,14,15 and congenital diaphragmatic hernia as well as in situations where cardiac surgery or hemodynamic decompensation is anticipated. These areas are in need of study.
Variability in Clinical Practice
Although pediatric cardiologists and pediatric pulmonologists tended to consistently report eligibility for immunoprophylaxis among children whom they believed were at high risk for severe RSV disease for most conditions, for some specified health conditions considered to put children at high risk for severe RSV disease, the level of agreement with eligibility for immunoprophylaxis was not necessarily the same, which suggests that other factor(s) contribute to the perceived need for immunoprophylaxis. The variability in practice within each specialty type may be a result of differences in perceived RSV disease risk based on the physician’s own clinical experiences. Alternatively, the variability may reflect different perceptions regarding conditions that define infants and young children as being at high risk for severe RSV disease; perhaps, further prospective study of these differences in clinical practice is warranted.
Strengths of the current study are that a large sample of respondents was selected from the entire pool of AMA-registered physicians. To reduce the potential for selection bias and ensure the generalizability of the sample, all individuals who self-identified as neonatologists, pediatricians, pediatric pulmonologists, or pediatric cardiologists in the AMA physician master file were invited to participate. The characteristics of the survey respondents were representative of the overall target population. Limitations of the study include the use of self-reported data because response bias may have affected the study findings. In addition, individuals who volunteered to participate in the survey may be more interested in RSV immunoprophylaxis than those who did not participate, and their responses may not reflect the opinions of all practicing physicians responsible for caring for those at high risk for severe RSV disease.
Conclusions
This study investigated current clinical practice surrounding RSV immunoprophylaxis use among neonatologists, pediatricians, pediatric pulmonologists, and pediatric cardiologists. The findings from this study verify that a majority of pediatric specialists agree with and implement the commonly recognized recommendations for RSV immunoprophylaxis for select high-risk patients. Moreover, many believe that immunoprophylaxis should be provided to certain patient groups not included in the current AAP guidance. However, regarding the updated 2014 AAP guidance, agreement and implementation among the various pediatric specialists was decidedly mixed. The results from this study provide a basis to improve education about risk for severe RSV disease and to evaluate changes in physician use of RSV immunoprophylaxis based on the recent 2014 AAP guidance. Prospective evaluation of RSV immunoprophylaxis use is warranted to determine the impact of the updated guidance on the burden of severe RSV disease in high-risk children.
Author Contributions
All authors contributed to the design, analysis, and interpretation of the study, critically revised the manuscript, provided final approval, and agree to be accountable for all aspects of work ensuring integrity and accuracy. DMF, KKM, and VRK also contributed to the conception of the study. IAS, SMS, KKM, and VRK also contributed to the acquisition of data and drafted the manuscript.
Footnotes
Acknowledgements
The authors also thank Diana Swanson, PhD (AstraZeneca), for assistance with manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Deborah Friedman has served on the Speakers Bureau and advisory board for and has received travel expenses from MedImmune/AstraZeneca. Joseph Domachowske has received grants and consulting fees from AstraZeneca. Pierre Wong has served on a medical advisory board for AstraZeneca. Michael Marcus has served on the Speakers Bureau for MedImmune. Iqra Syed’s and Shelagh Szabo’s employer, ICON plc, was paid for services related to the study design and data analysis of this study. William La Via, Kimmie McLaurin, and Veena Kumar are employees of AstraZeneca and may hold stock or stock options. Prabhu Parimi and Daniel Garcia have no conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by AstraZeneca. Medical writing assistance was provided by Anny Wu, PharmD, and Candace Lundin, DVM, MS, of Complete Healthcare Communications, Inc (Chadds Ford, PA) and funded by AstraZeneca.