
Abstract
To better understand parental opinions regarding the diagnostic process and use of genetic testing to assess risk for autism spectrum disorders (ASDs) in the younger siblings of affected children in the Unites States, we conducted a survey of parents who had at least one child with ASD. A total of 162 surveys were completed anonymously using an Internet-based survey tool. The mean reported time to ASD diagnosis and age at diagnosis were 35.2 months and 56.6 months, respectively. Seventy-two percent of parents felt there was a delay in diagnosis. Most parents indicated they would want to pursue genetic testing if a test were available that could identify risk in a younger sibling (80%). Earlier evaluation/intervention, closer monitoring, and lessened anxiety were reasons cited for testing. Our survey indicates most parents would pursue genetic risk assessment testing in children at high risk for ASD.
Introduction
Autism spectrum disorders (ASDs) are a group of highly heritable developmental disorders that can cause significant social, communication, and behavioral challenges. The Centers for Disease Control and Prevention (CDC) estimates the prevalence of ASD is approximately 1 in 88 children and that the majority of children with an ASD are not diagnosed until after they are 4 years old. 1
The American Academy of Pediatrics has developed surveillance guidelines with the goal of identifying children who are at risk of an ASD at an early age. 2 Early identification of children at risk for ASD is important since it permits referral for a comprehensive diagnostic evaluation and early intervention for affected children. Several studies have documented that children who receive early intervention show significant improvements in IQ scores, cognitive and adaptive behavior, language skills, daily living skills, educational placement, and severity of ASD diagnosis. 3 -6
Although there is a recognized need for early identification of children at risk for ASD, there remains a significant time lag between the age when parents first express concern about a child’s development and the age of ASD diagnosis. 7 -9 Sivberg 7 reported that there was a delay of 18 to 60 months between parental suspicion and diagnosis of an ASD, with more prolonged delays in higher functioning children with autistic disorder or Asperger disorder. More recently, Wiggins et al 10 reported that there was an average delay of 13 months from the first documented ASD evaluation by a qualified professional and eventual ASD diagnosis. Since the mean age of the first ASD evaluation for the patient series reported in their study was 48 months, the average age of eventual ASD diagnosis was 61 months for this cohort.
Genetic factors have been shown to have a significant role in the development of ASD. Numerous studies have shown that ASDs have a strong genetic component with most estimating heritability from 70% to 90%. 11 A recent study reported that the average recurrence risk for siblings of affected children is 18.7%, a 20-fold increase compared to the prevalence of ASD in the general population. 12 The authors also report differential recurrence risks based on gender with a recurrence rate of 25.9% for males and 9.6% for females. 12 Although genetic factors have a prominent role in the etiology of autism, there are few genetic tests available for children with ASD. 13 The genetic tests currently available are limited to diagnostic use only and include chromosome microarray, fragile X DNA analysis, and tests for a small number of genetic syndromes associated with ASD. These tests serve to identify the underlying genetic etiology in a child already diagnosed with an ASD. Recently, a new DNA-based test has become available which assesses the risk of ASD in children who have an older sibling diagnosed with ASD (ARISk® Test, IntegraGen, Inc, Cambridge, MA). The test detects common single nucleotide polymorphisms that have been shown to be associated with ASD. Based on the number of variants detected, a child’s reported risk for ASD would be increased, decreased, or unchanged when compared with the baseline recurrence risk. Although not diagnostic or indicative of a specific etiology, this test is designed to identify children at increased risk of ASD, allowing for early referral for a diagnostic evaluation and earlier intervention.
The purpose of this study was to better understand parental experiences with the ASD diagnostic process in the United States, to assess anxiety levels regarding the recurrence risk of ASD, and to obtain parental opinions regarding the use of a genetic risk assessment test to evaluate risk for ASD in a younger child.
Materials and Methods
Participants
We developed a self-administered Internet-based survey using online survey and questionnaire software available from SurveyMonkey, Inc, Palo Alto, California (http://www.surveymonkey.com). Requests for participation in the survey were e-mailed to potential participants by representatives from local and regional autism advocacy groups following receipt of an e-mail from 3 of the authors requesting assistance with recruitment for the survey. Contacts at more than 900 organizations were identified using an Internet-based search of local and regional autism advocacy groups in every state of the United States. Internet links to the survey were also posted to selected autism advocacy blog sites.
Survey participation was limited to U.S. residents who were a parent or guardian of one or more children with ASD. Respondent demographics collected included state of residence, age, gender, ethnicity, education level, number of children with ASD, and household income. The survey was conducted in English only. All surveys were completed anonymously and no information was collected that permitted the identification of any individuals completing the survey. A single recruitment request was sent to the potential participants, and responses to the survey were collected from February 13, 2012 until March 23, 2012.
Survey Design
Survey questions were designed to elicit objective, yes/no, or multiple choice answers. The first portion of the survey focused on parental perceptions regarding the ASD diagnostic process related to the respondent’s most recently diagnosed child. This included questions regarding the timing of initial suspicion of a difference in development, the referral and diagnostic process including the types of specialists encountered, and the time periods required for referral to specialists and eventual ASD diagnosis. Additional questions explored the reasons for perceived delays in the diagnostic process and parental anxiety levels prior to their child receiving an ASD diagnosis. The remaining questions of this portion of the survey focused on the perceived role of genetics in ASD and parental experiences with genetic testing for their child diagnosed with ASD.
Parents who reported having a younger, undiagnosed child less than 48 months of age were eligible to complete the second portion of the survey. This section included questions regarding participants’ perceptions of the recurrence risk of ASD for their younger child, anxiety levels associated with the perceived recurrence risk, and opinions regarding whether they would want to have their younger child receive a genetic test which assessed the child’s risk of ASD, but neither confirmed nor ruled out an ASD diagnosis. This was followed by a series of questions related to why they would or would not want their child to receive a genetic risk assessment test for ASD.
The survey was reviewed and pilot tested with select parents of children with ASD and with specialists who provide clinical care and diagnostic services for children with developmental delays and/or ASD. To avoid any potential bias, the survey did not include any specific reference to IntegraGen, Inc or the ARISk Autism Risk Assessment Test.
Results
Demographics
A total of 162 eligible participants completed the online survey. Demographic information for individuals who completed the survey is shown in Table 1. The majority of participants were female (89%), highly educated (76.5% having at least a college degree), and of those respondents who reported ethnicity (n = 140), 84.2% were non-Hispanic Caucasian. More than one third (41.4%) were between 36 to 45 years old, and more than half of participants who reported annual income (n = 119) indicated a household income of $75, 000 or higher.
Demographic Characteristics of Survey Participants
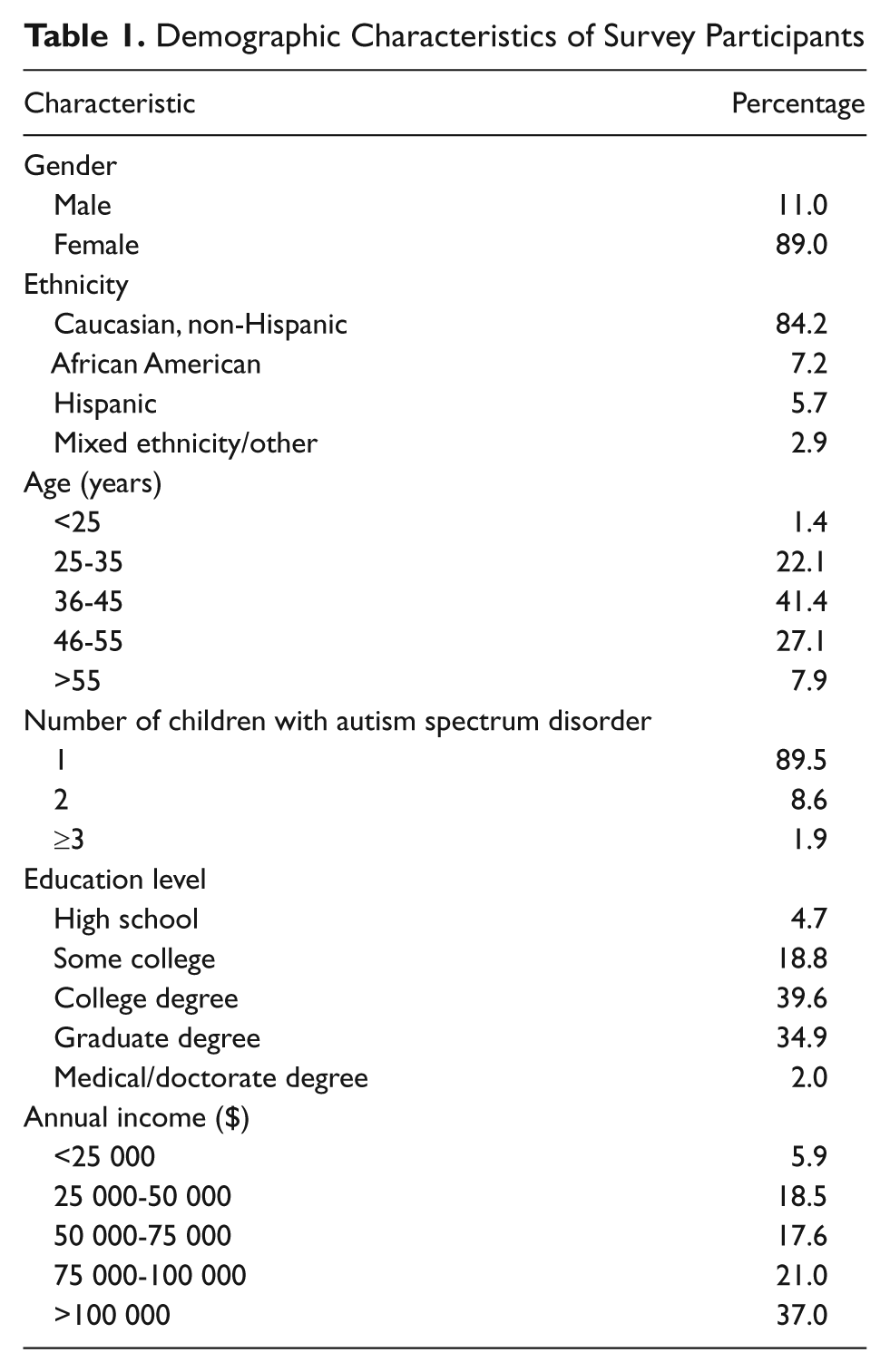
Survey responses were received from individuals residing in 24 states representing all regions of the United States and the District of Columbia. Virginia, Georgia, Arizona, Kansas, Texas and Tennessee disproportionately represented nearly one half of the total survey responses. No other state was associated with greater than 5% of the total responses.
All survey participants reported that they had at least one child who had been diagnosed with an ASD. Of these, 89.5% had one child with ASD, whereas 8.6% and 1.9% had 2 or ≥3 children with ASD, respectively. The majority of responders (94.3%) indicated that they were the biological parent of a child or children with ASD, 3.1% indicated that they were a grandparent, and 1.9% reported that they were an adoptive parent. One participant (0.6%) indicated that he or she was a stepparent of a child with ASD.
Experiences With the Diagnostic Process for Autism Spectrum Disorders
The mean age when a difference in development was suspected for the children cared for by survey participants was 21.4 months (Figure 1). Although a reported decrease in age was observed with each subsequent child in the family, initial concern was not raised at a substantially earlier age until the third child presented with symptoms. Participants reported differences in development were first noticed by the surveyed parent or their partner in most cases, followed by another family member, the child’s caregiver, or the child’s educator. Only 5.7% of survey participants reported that the child’s pediatrician was the first to identify a potential difference in development (Figure 2).
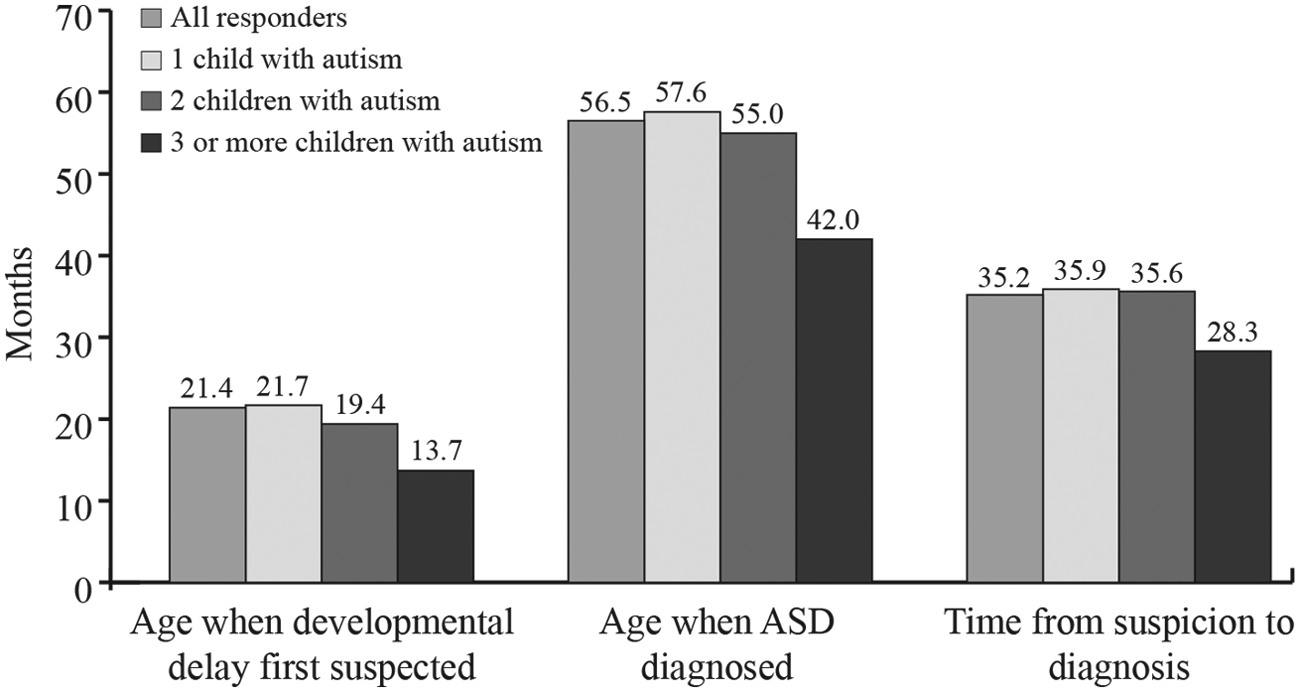
Mean reported ages when difference in development suspected and autism spectrum disorder (ASD) diagnosed
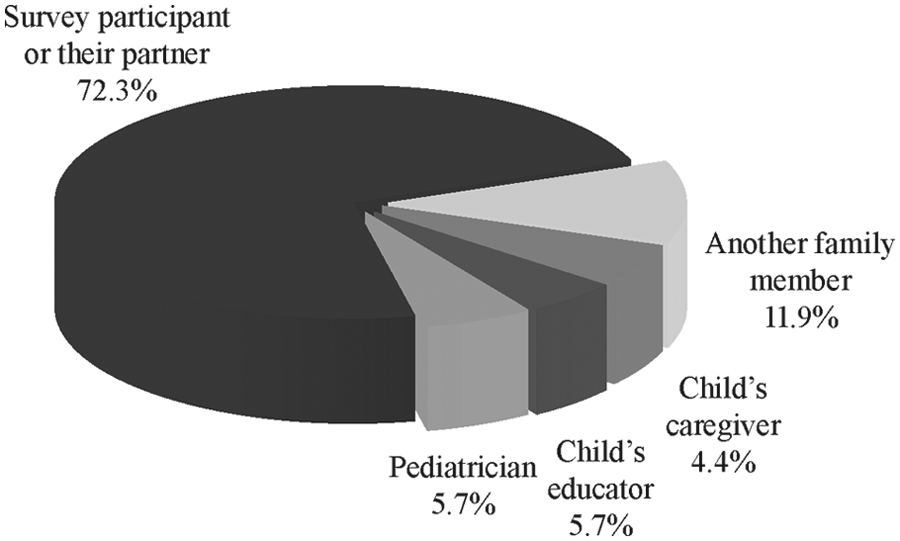
Who first noticed developmental delay?
The mean reported age when ASD was diagnosed was 56.6 months (Figure 1). Similar to the age at which a difference in development was first suspected, there was no substantial difference in mean reported age for ASD diagnosis between the first and second child to be diagnosed in the family. A considerable reduction in the age of ASD diagnosis was not reported until there were three or more children in a family diagnosed with ASD. When asked to provide a specific diagnosis for their child, more than half of the respondents indicated autistic disorder (Table 2). Finally, survey participants indicated that the ASD diagnosis was made most often by a child psychiatrist/child psychologist.
Reported ASD Diagnosis
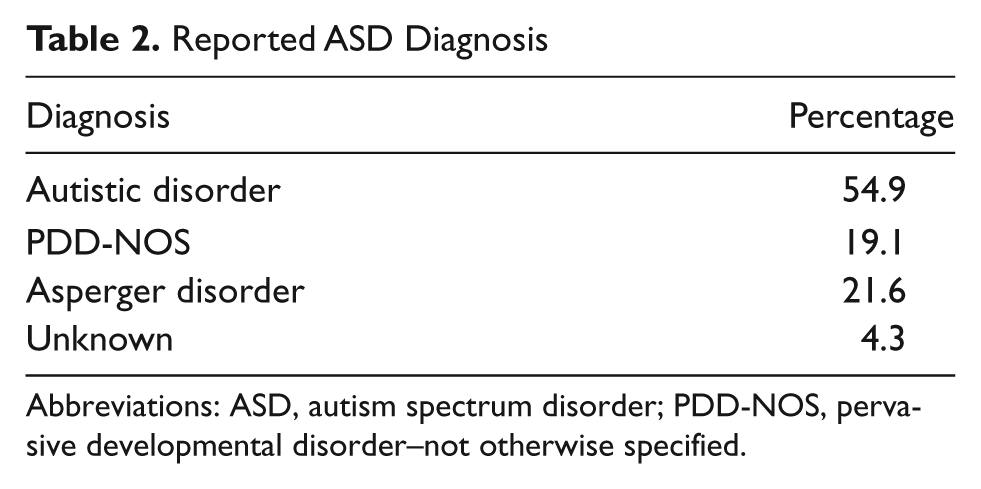
Abbreviations: ASD, autism spectrum disorder; PDD-NOS, pervasive developmental disorder–not otherwise specified.
Overall, there was nearly a 3-year time period (35.2 months) between the initial suspicion of a difference in development and an ASD diagnosis for children cared for by survey participants (Figure 1). This time period was somewhat reduced if the family had two previous children diagnosed with an ASD. Parents indicated a perceived delay in diagnosis was primarily due to a “wait and see” approach by the child’s pediatrician or a delay in seeing a specialist. Only 28% of parents indicated that there was no delay in receiving a diagnosis (Figure 3). The majority of parents (84.3%) indicated that they had a high level of anxiety about their child’s development prior to receiving an ASD diagnosis (Figure 4).
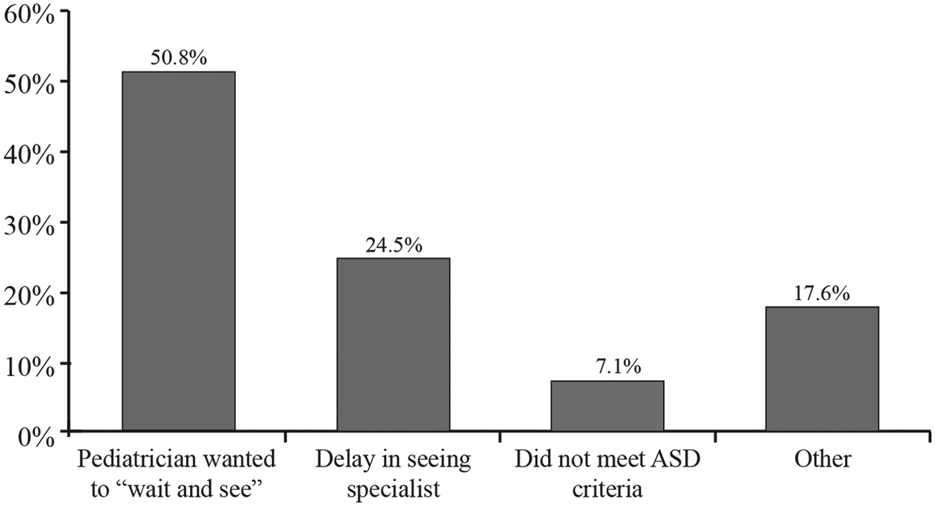
Perceived reasons for delay in autism spectrum disorder (ASD) diagnosis
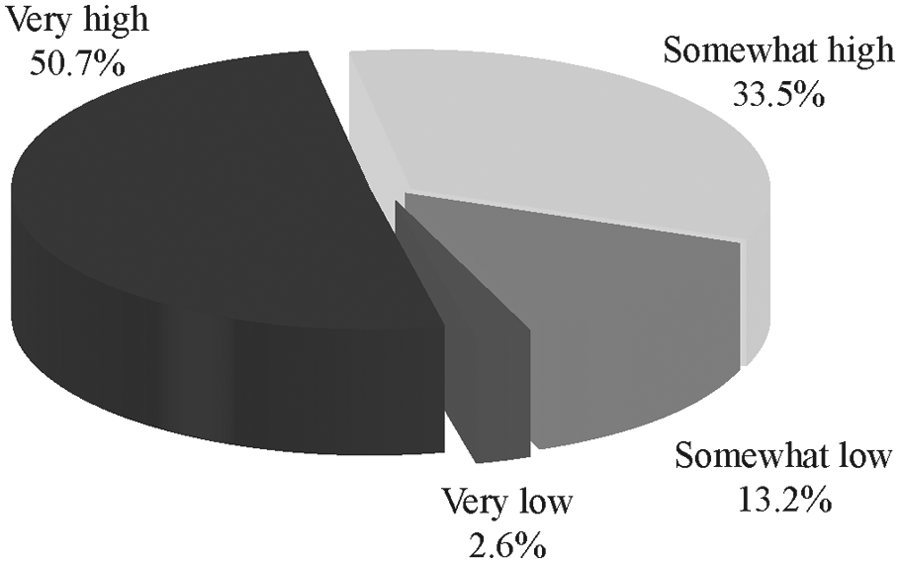
Level of parental anxiety prior to autism spectrum disorder (ASD) diagnosis
Diagnostic Genetic Testing for Children With Autism Spectrum Disorders
The majority of survey participants indicated that they believed genetic factors contributed to the development of ASD with 82.1% indicating that it was a combination of genetic and environmental factors and 11.9% indicating that ASD was almost entirely a result of genetic factors. Six percent of responders indicated that they believed ASD was caused almost entirely by nongenetic factors.
Only 27.8% of participants indicated that their child/children diagnosed with ASD had undergone diagnostic genetic testing with abnormal results being reported for only 7.3% of the children tested. The majority of children who underwent genetic testing did not receive this testing until after an ASD diagnosis had been made. More than two thirds of children (69.5%) reportedly had not undergone genetic testing. A minority of parents (2.7%) were unsure if their child/children had undergone genetic testing.
Beliefs Regarding Recurrence Risk and Attitudes Toward Genetic Risk Assessment Testing in Younger Siblings
Seventy-two survey participants (46.8%) indicated that their family included at least one younger sibling, as of yet not diagnosed with an ASD. Of those, 78.1% reported one younger child, 17.8% reported 2 younger children, and 4.1% reported 3 younger undiagnosed children. Of these younger siblings, 25 (15.4% of the total sample) were reported to be younger than 48 months. More than 50% of these younger undiagnosed children were between 13 and 24 months old at the time the parents were surveyed (Figure 5).
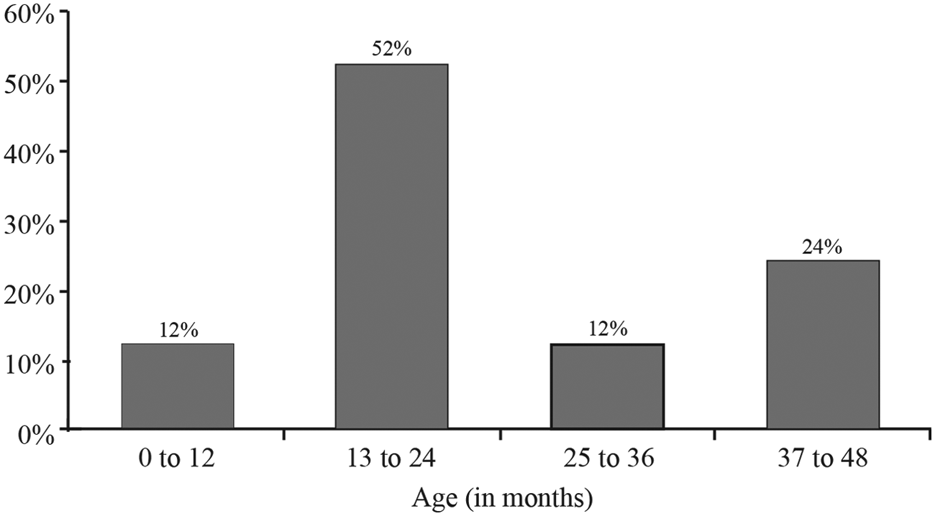
Age of undiagnosed younger sibling (months)
Fifty-two percent of respondents whose families included a younger undiagnosed child less than 48 months old felt that the younger child was somewhat or highly likely to develop ASD. Forty-eight percent indicated that they had a somewhat or very high level of anxiety associated with the possibility that the younger undiagnosed child could develop ASD (Figure 6). There was no correlation between the perceived risk of ASD for the younger sibling and the reported anxiety levels with some survey participants indicating that although they felt it was unlikely that the younger child would develop autism, they still had an increased anxiety level and others who felt their child had an increased likelihood of autism expressed a lower level of anxiety.
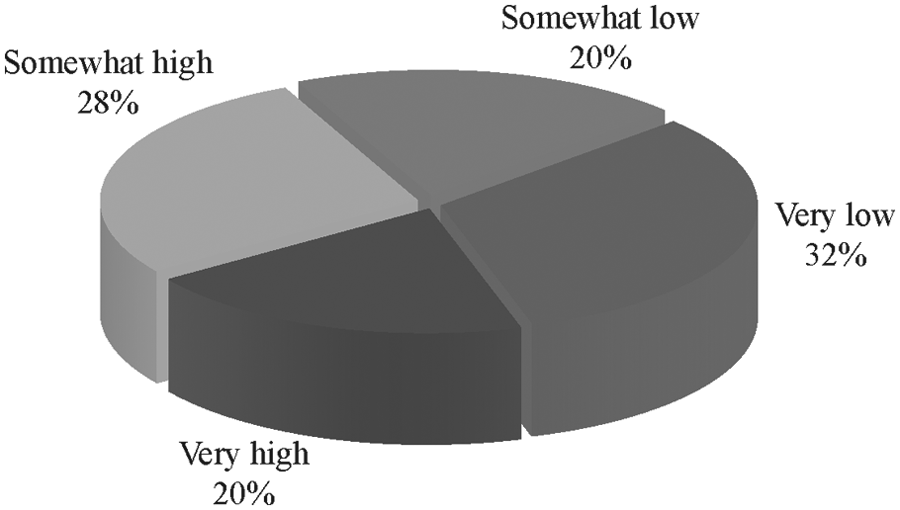
Level of parental anxiety associated with the possibility of the younger sibling (<48 months) developing autism
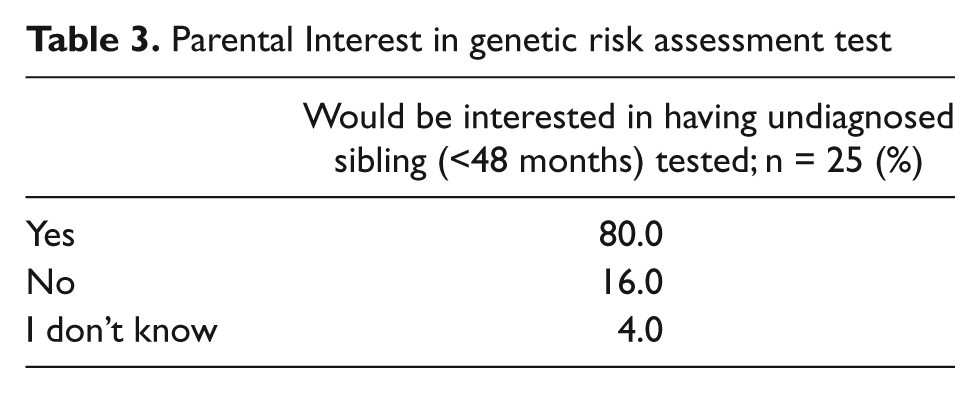
A large majority (80%) of survey participants with a younger undiagnosed child less than 48 months old indicated they would want their child tested if a genetic test were available that could identify risk for ASD, even if it could not confirm or rule out the diagnosis (Table 3). All the parents who indicated an interest in having their child tested reported that they believed the test results could allow for closer monitoring and earlier access to evaluation and intervention (Figure 7). Eighty-five percent of these parents indicated that their anxiety level would be decreased based on the results of this test. Reasons provided for the disinterest in having a child tested included a concern that knowing this information would increase anxiety (12%), the availability of this information would result in their child being labeled (12%), and a lack of awareness of what could be done with this information (8%). One survey participant was unsure whether they would want their younger undiagnosed child tested or not.
Parental Interest in genetic risk assessment test
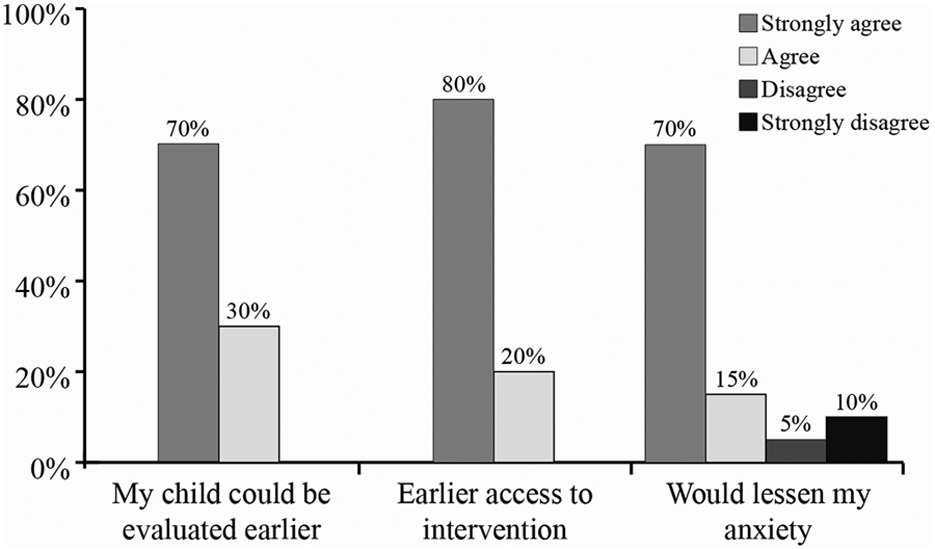
Reported reasons why parents would want their younger, undiagnosed child (<48 months) to undergo testing to determine the genetic risk for autism spectrum disorders even if the test were not diagnostic
Discussion
Early identification of children at increased risk of ASD can provide for an increased opportunity to diagnose ASD and initiate beneficial behavioral treatments for these children. The results of our survey coincide with the CDC’s most recent data and other reports in the literature, which indicate that there remains a significant time lag between initial parental suspicion of a difference in development and an ASD diagnosis for the child. 1,7 -11,14 The average age of ASD diagnosis reported for the children represented in our survey was 4.7 years. This is similar to the average age of ASD diagnosis of 4.4 years reported by the CDC. 1 A more recent report from the CDC and the National Center for Health Statistics indicates that 40% of children with ASD are 6 years or older when they are first identified as having ASD and only 20% of children are identified before the age of 2 years. 14 Delays in diagnosing a child with ASD have significant consequences since infants and toddlers have an increased level of neural plasticity, the ability to develop new neurological pathways in the brain, and less severe interfering behaviors compared with older children. 15 Therefore, in general, the largest improvements in developmental outcomes are reported when intervention services are begun at a younger age.
Delayed evaluation and diagnosis of a child in whom a parent suspects a difference in development or ASD can also lead to increased parental anxiety. Parents of children with ASD experience increased anxiety levels and the uncertainty of an autism diagnosis can increase parental anxiety and delay the introduction of behavioral therapy and other beneficial efforts. 16 Many clinicians dismiss parental concerns regarding suspicion of developmental issues or advise a “wait and see approach,” which prolongs the diagnostic process. Research by Pisula 16 and Avdi et al 17 suggests that most parents consider themselves as the person who knows their child best and often feel frustrated when healthcare professionals control information or try to protect them by not telling them all of the information about their child and the risk of ASD.
Unresolved parental concern for a child suspected of having a developmental delay contributes to a parent’s anxiety about the child and their prognosis. A recent study by Weiss et al 18 demonstrated that a parent’s psychological acceptance of having a child with a developmental delay or ASD is an important component for the development of coping mechanisms leading to reductions in parental stress. The above coincides with the responses from the parents in our present survey as to whether or not they would want a younger at-risk sibling to undergo genetic risk assessment testing for ASD even if the test was not diagnostic. Eighty-five percent of parents who reported they would want their child tested indicated that their anxiety levels would be lessened if their child were tested (Figure 7). This suggests that concerns clinicians may have about the potential for increasing parental stress if a child is identified as having an increased risk of ASD may be unwarranted for most families.
A key limitation of the study was that it relied solely on retrospective self-reporting rather than prospective data collection. Parental self-reporting questionnaires, however, have been widely used by other researchers to provide parental feedback and to obtain demographic data for individuals with ASD and their families. 8 -10,13,19 Of note are several studies based on data obtained from the Interactive Autism Network, a national, Internet-based, voluntary autism family register (http://ianproject.org/) where parents provide information on their children with ASD and biological siblings via standardized questionnaires. 20 -23 Similar to our survey, participants in the Interactive Autism Network project and other parental surveys were limited to parents or legal guardians who were English-speaking.
The parents responding to our survey were also not representative of the US population with an overrepresentation of individuals with higher levels of education and income and an increased percentage of Caucasian non-Hispanics. This may partially have been because of the fact that participants were recruited through local and regional advocacy groups rather than using a randomized approach, which may have introduced ascertainment bias. However, the overrepresentation of these groups in our study is similar to other ASD surveys. 13,19 The higher educational level and socioeconomic status of our survey participants also coincide with reports from the literature that these demographic groups are disproportionately represented in the ASD population. 24 -28 The administration of the survey via the Internet only may have also contributed to the above since access to a computer and the internet were requirements for participation in the study. The underrepresentation of Hispanic and African American survey participants coincides with the historical decreased incidence of ASD reported for these 2 ethnic groups. 1
Finally, survey participants were not asked to indicate the gender of the affected child within their care. Therefore, all mean ages reported are of males and females combined. It is unknown what impact gender would have had, if any, on the age at which developmental differences might have been detected or an ASD diagnosis might have been made.
In summary, our study is consistent with previous studies that delayed diagnosis and access to specialty care remain problematic for children with ASD. Our results showed a considerable amount of time between the initial suspicion of a difference in development and the diagnosis of ASD, and that these time lags are primarily related to delays in referrals to specialists by pediatricians and the wait times to see a specialist once a referral is made. The results of our survey also indicate that the majority of parents would be interested in using a genetic test that assessed the risk of ASD in younger siblings of affected children and that the results of such a test would help to reduce their anxiety levels.
Footnotes
Acknowledgements
The authors wish to thank the individuals at the autism advocacy organizations who kindly forwarded the link to our survey to parents within their organizations. We would also like to express our sincere gratitude to those parents who took the time to participate in our survey.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E. Couchon is an employee of IntegraGen, Inc, V. Narcisa, M. Discenza, and E. Vaccari received financial compensation from IntegraGen, Inc, associated with their support of this project. A. Hardan and B. Rosen-Sheidley are paid consultants to IntegraGen, Inc. This project was neither reviewed nor endorsed by Arcadia University, the Boston University School of Medicine, Boston Children’s Hospital or Stanford University.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This survey was sponsored by IntegraGen, Inc, Cambridge, Massachusetts.