
Abstract
Background
Occupational therapists use standardized scales to assess how individuals process and respond to sensory information. Currently, there is limited evidence about the convergent validity between the Adult/Adolescent Sensory History (ASH) and the Sensory Processing Measure 2–Adult Form (SPM-2-Adult).
Purpose
The study examined the convergent validity of the ASH and SPM-2-Adult when completed by young adults.
Methods
Fifty Australian adults aged 21–35 completed the ASH and SPM-2-Adult. Spearman’s rho correlations were used to analyze the data.
Results
Most ASH and SPM-2-Adult subscales were significantly associated with correlations ranging from rho = 0.301 to 0.858 (p < .033–.001). Statistically significant correlations were obtained between the SPM-2-Adult Vision subscale and every ASH subscale (rho = 0.322–0.841, p < .023–.001) while the SPM-2-Adult Taste and Smell subscale yielded the most non-significant correlations with the ASH. Most of the statistically significant correlations between the ASH and SPM-2-Adult were in the moderate range.
Conclusion
Promising evidence of convergent validity between the ASH and SPM-2-Adult sensory subscales and total scales was demonstrated, whereas the convergent validity findings between the ASH Functional-Problems subscales and the SPM-2-Adult sensory subscales were less robust. This adds to the psychometric body of concurrent validity evidence between the two scales.
Introduction
Sensory processing is how our nervous system receives, interprets and responds to sensory information from the environment (Critz et al., 2015; Lin, 2020). Sensory information comes in many forms and has been categorized into the following key groups: visual, auditory, gustatory/taste, olfactory/smell, tactile/touch, proprioception (body awareness), interoception (internal body senses) and vestibular (relating to movement and balance) (Gebuis et al., 2016; Peterka, 2018). The way children and adults receive sensory information is generally consistent, but how each person interprets and responds to sensory stimuli is highly individualized. When a person encounters problems processing and responding to sensory input that negatively impacts their occupational participation and daily functioning, this is referred to as sensory processing disorder (SPD; Galiana-Simal et al., 2020; McArthur, 2022). SPD involves individuals having trouble detecting, modulating, interpreting, and responding to sensory input (DuBois et al., 2017; Passarello et al., 2022). Studies suggest that 5–16.5% of the general population experience some level of SPD (Ahn et al., 2004; Ben-Sasson et al., 2009b; Schoen et al., 2009).
Notably, individuals from some diagnostic groups (such as autism spectrum disorder [ASD], attention-deficit/hyperactivity disorder [ADHD], dyspraxia, developmental coordination disorder, anxiety disorders, obsessive-compulsive disorders) are more likely to present with sensory processing challenges (Bundy et al., 2007; Delgado-Lobete et al., 2020; Jurek et al., 2025; Harrold et al., 2024; Passarello et al., 2022; van den Boogert et al., 2022). These difficulties can impact occupational performance by disrupting daily activities such as self-care, social participation, leisure pursuits, sleep, work activities, or education tasks, highlighting the importance of understanding sensory processing across the lifespan including young adults (Ben-Avi et al., 2012; Costa-López et al., 2021; Escelsior et al., 2025).
SPD is recognized by the Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood (DC:0–5) under the category of “Regulation Disorders of Sensory Processing” (Zeanah et al., 2016). Three specific types of SPDs are mentioned in the DC:0–5: Sensory Over-Responsivity Disorder, Sensory Under-Responsivity Disorder and Other SPD (Zeanah et al., 2017). The DC:0–5 is commonly used by infant mental health professionals and highlights the influence of sensory processing on young children's development and interpersonal relationships. In addition, SPD is also recognized in the Interdisciplinary Council on Developmental and Learning Disorders Diagnostic Manual for Infants and Young Children (ICDL-DMIC) under the label of Regulatory-SPD (Greenspan & Wieder, 2008; Jorquera-Cabrera et al., 2017). Therefore, in the paediatric sphere, it appears that SPD is becoming increasingly recognized by health care professionals who provide services to children and families.
In contrast, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (American Psychiatric Association, 2013), the International Statistical Classification of Diseases and Related Health Problems, Eleventh Revision (ICD-11) (World Health Organization, 2019), the Hierarchical Taxonomy of Psychopathology (HiTOP) (Cicero et al., 2024; Kotov et al., 2017), and the Research Diagnostic Criteria (Spitzer et al., 1978) all do not currently classify SPD as an independent diagnosis. Within the DSM-5, however, sensory processing challenges are typically viewed as characteristics of other conditions, such as ASD and ADHD. Therefore, in the adult age group, SPD is still not officially acknowledged by doctors and psychologists, but occupational therapists are increasingly working with more and more adult clients presenting with sensory processing challenges (Kozidis & Jacobson, 2023; Quint et al., 2019).
Sensory Processing in Young Adults
Historically, much of the research on sensory processing has been centred around the paediatric population aged 0–18 years, with many assessments being created and standardized for this age group as a result (Dean et al., 2018; Diamant & Smet, 2024; Jovellar-Isiegas et al., 2020; Lin, 2020; Shahbazi & Mirzakhani, 2021). However, the same cannot be said when understanding young adults’ sensory processing difficulties (DuBois et al., 2017). Limited information is currently available on examining sensory processing in young adults, however, a common trend in research highlights associations between adults with diagnoses presenting with sensory processing difficulties comorbidity (Escelsior et al., 2025; Kozidis & Jacobson, 2023).
Studies show a strong connection between SPD and mental health issues in young adults, especially concerning anxiety and depression (Escelsior et al., 2025; Serafini et al. 2017). Those with SPD, particularly those who are overly sensitive to sensory input, tend to face internalizing issues such as anxiety and externalizing issues like aggression (Cervin, 2023; Rossow et al., 2019). Additionally, challenges with emotion regulation frequently act as a mediating fact between childhood sensory processing difficulties and anxiety disorders in adulthood (Escelsior et al., 2025). Studies have found that adults with ASD displayed extreme dysfunction on at least one of the quadrants of the Sensory Profile at high percentages, which suggests that difficulties with sensory processing continue throughout the lifespan (Crane et al., 2009; van den Boogert et al., 2022). In addition, young adults presenting with sensory processing challenges often have co-occurring mental health conditions, with patterns of sensory avoidance, sensory sensitivity and low registration being linked to mental health problems (Abernethy, 2010; Escelsior et al., 2025; Harrison et al., 2019; van den Boogert et al., 2022).
Several studies have utilized the Adult/Adolescent Sensory Profile (A/ASP; Dunn & Brown, 2002) to examine the relationship between sensory processing and mental health in adults (Pfeiffer et al., 2014; Serafini et al., 2017; van den Boogert et al., 2022). These findings further acknowledge the significance of sensory processing in understanding and managing mental health conditions in adults (Goycolea Martinic et al., 2024; Kozidis & Jacobson, 2023). Studies by Kozidis and Jacobson (2023) and Pfeiffer et al. (2014) indicated that people with sensory sensitivity (heightened awareness of sensory stimuli) and low registration (reduced awareness of sensory stimuli) tend to participate less in daily activities, while those with sensory-seeking behaviours show increased engagement. These findings emphasize how sensory processing preferences could provide crucial insights for occupational therapists, aiding intervention planning and improving occupational engagement (Cascio et al., 2016). Similar conclusions were determined by Metz et al. (2019), who acknowledged that there is a variability in sensory thresholds among individuals, which can impact daily activities. Thus, ongoing research is necessary to better understand how adults process sensory information and how this understanding can improve their quality of life and participation in daily activities (Costa-López et al., 2021; Wong & Fisher, 2015).
While these studies emphasize the importance of understanding how sensory processing preferences influence adults’ engagement in everyday occupations, a clear gap in the literature remains. Beyond the A/ASP, examined in studies by Kozidis and Jacobson (2023), Pfeiffer et al. (2014), van den Boogert et al. (2022) and Metz et al. (2019), there is minimal research exploring the newly developed Adult/Adolescent Sensory History (ASH) (May-Benson, 2021) and the revised edition of the Sensory Processing Measure 2–Adult Form (SPM-2-Adult) (Parham et al., 2021). This highlights the need for ongoing research into these scales’ psychometric properties including their convergent validity when completed by young adults.
Sensory Processing Assessment
Assessments are vital for gathering and analysing information about a person's abilities and performance (Piernik-Yoder & Beck, 2012). Occupational therapists use assessments to inform goal setting and tailor interventions for optimal client outcomes. In sensory processing, assessments help identify individuals’ preferences and challenges (Aron, 2020; DuBois et al., 2017). However, more information is needed on examinations to assess sensory processing in young adults, with only three standardized assessments currently available for occupational therapists to utilize in practice settings.
Until recently, the only standardized assessment available for occupational therapists to evaluate adult sensory processing was the A/ASP (Dunn & Brown, 2002). This self-report questionnaire includes 60 questions that evaluate sensory processing preferences across different domains. The A/ASP is based on Dunn's Model of Sensory Processing, which examines how sensory processing influences daily life (Dunn, 2001). The core idea of this model is that an individual's response to sensory events is shaped by their sensory threshold (either high or low) and their responding strategy (either passive or active). Through this model, Dunn (2001) categorizes sensory processing into four distinct quadrants: Low Registration, Sensation Seeking, Sensation Sensitivity, and Sensation Avoidance. These four distinct quadrants are assessed using A/ASP. The A/ASP while now being more than 20 years old (which includes its normative data on which its standardized scores are based), the A/ASP does not provide any individual scores on any specific types of sensory processing such as vision, hearing, taste, touch, smell, vestibular or proprioceptive input. This is a notable limitation of the A/ASP besides its now dated normative data.
Since 2021, two new self-report measures—the ASH (May-Benson, 2021) and SPM-2-Adult (Parham et al., 2021)—have been published. Both scales examine specific components of sensory processing. However, further research on the validity and reliability of these assessments is needed, particularly in other cross-cultural contexts, as they were developed and standardized in the United States. The ASH (May-Benson, 2021) and SPM-2-Adult (Parham et al., 2021) based on Ayres’ Sensory Integration® theory (Ayres, 2005), which suggests that to engage with the world effectively, one's brain must be able to process and organize sensory information (Ayres, 2005).
Ayres’ Sensory Integration® theory (Ayres, 2005) “postulates that how the central nervous system integrates and responds to sensations, from outside and within one's own body, influences physiological, regulatory, emotional, motor, and adaptive functioning” (Parham et al., 2021, p. 1). When bodily sensations are not integrated effectively or efficiently, a person may struggle to learn efficiently, manage their emotions, or perform daily occupations as typically expected. Challenges in processing sensations can also impact more complex abilities, such as planning movements (referred to as praxis), and engaging in social interactions (referred to as social participation) (Lane et al., 2019). This highlights how difficulties with learning, behaviour and motor skills can occur if problems with sensory integration and/or sensory processing are present in children and adults (Ayres, 2005).
Given both the ASH (May-Benson, 2021) and SPM-2-Adult (Parham et al., 2021) are grounded on Ayres’ Sensory Integration® theory (Ayres, 2005), it would be anticipated that the sensory processing factors that they assessed would be associated. When two scales claim to measure the same theoretical constructs, like the ASH and the SPM-2-Adult, their convergent validity can be investigated. “Convergent validity is a supporting piece of evidence for construct validity. The underlying idea of convergence validity is that related construct's tests should be highly correlated” (Chin & Yao, 2014, p. 1275). The convergent validity between the ASH and the SPM-2-Adult has not been explored in the empirical literature to date.
The SPM-2-Adult assesses eight aspects of adults’ sensory processing (e.g., vision, hearing, touch, taste and smell, body awareness, balance and motion, planning and ideas and social participation) (Parham et al., 2021). In contrast, the ASH can (i) identify sensory processing issues in five key areas (e.g., sensory discrimination, sensory modulation, postural-ocular skills, praxis and social-emotional functioning), (ii) detect eight sensory processing functional problems (e.g., visual seeking, seeks movement, seeks touch, discomfort with imposed touch, tactile-related hygiene, discomfort with water, atypical pain response, and gravitational insecurity), and (iii) provide information about nine sensory categories: visual, auditory, movement, taste and smell, touch, proprioception, postural control, motor coordination, and social emotional (May-Benson, 2021). Therefore, compared to the A/ASP, both the SPM-2-Adult and the ASH provide a much broader overview or profile of an adults’ sensory processing strengths and difficulties. Investigating how the sensory processing factors measured by the SPM-2-Adult and the ASH in young adults is warranted.
Skocic et al. (2024) examined the convergent validity between the A/ASP and the SPM-2-Adult in a sample of 42 young adults aged 18–30 years. The findings indicated that “significant associations were achieved between the A/ASP Low Registration, Sensory Sensitivity, and Sensation Avoiding quadrant subscales and all nine of the SPM-2-Adult subscales” (Skocic et al., 2024, p. 897). Likewise, by examining the convergent validity between the ASH and SPM-2-Adult, this would add to the body of psychometric evidence of these two scales and inform occupational therapists’ assessment of young adults’ sensory processing.
Aim and Research Question
The literature on sensory processing in young adults has noticeable gaps and more evidence is needed to examine the validity of the ASH and SPM-2-Adult. The literature also indicates an ongoing need to investigate sensory processing challenges in young adult populations to better inform occupational therapy practice. Thus, the aim is to examine the convergent validity of two self-report sensory processing scales, the ASH and SPM-2-Adult, used to assess young adults. To operationalize the aim, the following research question was posed: are the sensory processing factors measured by the ASH and SPM-2-Adult when completed by young adults significantly associated?
Method
Design
This study adopted a cross-sectional quantitative design.
Participant Recruitment
Participants aged 21–35 residing in Australia were recruited using convenience sampling via social media platforms such as LinkedIn, Facebook and Instagram, which has proven to be an effective method of recruiting participants (Leighton et al., 2021). The survey was accessed through a link embedded in the social media post. The inclusion criteria for the study participants were as follows: (1) aged 21–35 years; (2) residency in Australia; and (3) fluency in reading the English language as demonstrated by their ability to read a daily newspaper. Participants were excluded if: (1) they had an existing relationship with any of the research team members; or (2) they had any self-reported diagnosis related to mental illness, cognitive impairment or intellectual disability.
As the study used correlation analysis, the required statistical power using the program titled “Sample size calculators for designing clinical research” (Hulley et al., 2013) was calculated. For a simple correlation (r = 0.5) using a two-sided test with 80% power (β = 0.2) and significance level set at 5% (α = 0.05), the study required a minimum of 29 participants, which explains the minimal sample size target for participant recruitment for the current study.
Instrumentation
Data were collected via an online survey comprised of three parts: (i) demographic questionnaire, (ii) ASH and (iii) SPM-2-Adult. Participants completed the survey anonymously via Qualtrics and completed the ASH, followed by the SPM-2-Adult. Details of each assessment are detailed below.
Demographic Form
The demographic form was developed to determine participants’ eligibility for the study and to collect data to inform findings and establish connections among them. Participants were asked about age, gender identity, language, country of residence and diagnosed conditions. Quality control measures were implemented, including field testing, to ensure the demographic form had face and content validity.
ASH
The ASH is a 163-item questionnaire that identifies difficulties in five key areas: Sensory Discrimination, Sensory Modulation, Postural-Ocular Skills, Praxis and Social-Emotional Functioning (May-Benson, 2021). The ASH has eight Functional-Problem subscales: Visual Seeking, Seeks Movement, Seeks Touch, Discomfort with Imposed Touch, Tactile-Related Hygiene, Discomfort with Water, Atypical Pain Response, and Gravitational Insecurity (May-Benson, 2021). It is further divided into nine sensory sub-categories: Visual, Auditory, Movement, Taste and Smell, Touch, Proprioception, Postural Control, Motor Coordination, and Social Emotional (May-Benson, 2021). The ASH takes 15–20 min to complete and is suitable for people aged 13–95. To complete the ASH, individuals use a 5-point Likert-type rating scale to rate the frequency of a behaviour: always, often, sometimes, rarely, never. To score the ASH, scores within each domain are calculated and then it is determined whether they fall within typical, atypical or significantly atypical ranges when compared against normative data (May-Benson, 2021).
The ASH was correlated against the A/ASP sensory subscales to assess the validity and reliability of the scale (May-Benson, 2021). The test-retest reliability coefficients for the ASH's total score, modulation, discrimination and sensory sections for a 3–4-week interval ranged from 0.74 to 0.87, indicating a strong correlation (May-Benson, 2021). In contrast, inter-rater reliability coefficients for the ASH's total score, modulation, discrimination and sensory sections ranged from 0.52 to 0.68 (May-Benson, 2021). Internal consistency of the Total Score and sensory sections was assessed using Cronbach’s coefficient alpha, which ranged from 0.80 to 0.97 (May-Benson, 2021). Evidence supporting the validity of the ASH includes content, convergent and construct validity demonstrated through confirmatory factor analysis for both scales (May-Benson, 2021).
SPM-2-Adult
The SPM-2-Adult is an 80-item self-report questionnaire designed for persons aged 21–87 to assess their sensory functioning and social interaction in various situations. Developed by Parham et al. (2021), the SPM-2-Adult comprises eight subscales within sensory processing: vision, hearing, touch, taste and smell, body awareness, balance and motion, planning and ideas and social participation (Parham et al., 2021). Similar to the ASH, the SPM-2-Adult is grounded in Ayres’ Sensory Integration® theory (Ayres, 2005).
The SPM-2-Adult uses a Likert-type scoring system on a 4-point scale: never, occasionally, frequently or always. The assessment is estimated to take 20–30 min to complete. The SPM-2-Adult scoring consists of totalling the subcategory raw scores and then transferring them to the score summary sheet. The raw scores, corresponding t-scores and percentile rank are presented graphically, showing the difficulty level ranging from normal to moderate to severe difficulties (Parham et al., 2021).
The SPM-2-Adult was also correlated against the A/ASP. The test-retest reliability coefficients for a two-week interval ranged from 0.78 to 0.93 for its subscales, while its internal consistency Cronbach alpha coefficients for its subscales ranged from 0.73 to 0.96 (Parham et al., 2021). The SPM-2-Adult's inter-rater reliability coefficients were in the moderate range for all age levels, with a median correlation of 0.63 (Parham et al., 2021). Evidence of validity reported in the SPM-2-Adult's manual includes content, convergent and construct validity demonstrated via confirmatory factor analysis (Parham et al., 2021). The SPM-2-Adult user manual explored numerous diagnostic groups, including ADHD, ASD, Cerebral Palsy and Down Syndrome, with findings indicating sensory integration and processing challenges are common among these populations (Parham et al., 2021).
Data Analysis
Following data collection, the raw subscale scores of each participant's ASH and SPM-2-Adult were analysed using the Statistical Package for Social Sciences program (SPSS) version 29.0 (IBM Corp, 2021). To examine the associations between the ASH and SPM-2-Adult subscales, Spearman Rho correlations were used with the statistical significance being set at p < .05 (Onwuegbuzie & Leech, 2006). To determine the strength of the correlations between the ASH and SPM-2-Adult, guidelines outlined by Schober et al. (2018) were applied. These guidelines define the following correlation ranges: 0.00–0.10 as negligible, 0.10–0.39 as weak, 0.40–0.69 as moderate, 0.70–0.89 as strong and 0.90–1.00 as very strong (Schober et al., 2018).
Data Management
Data were collected via Qualtrics, a platform approved and utilized by Deakin University and entered into SPSS for analysis. All data were de-identified and stored electronically in password-protected folders on the Deakin University server. As per the Deakin University ethical guidelines, all electronic data related to the study will be securely stored for a five-year period, after which it will be securely disposed of.
Procedures
The Deakin University Human Research Ethics Committee approved the study on June 14, 2024 (approval number: HEAG-H 83_2024). Participants were recruited from three social media platforms: LinkedIn, Facebook and Instagram. A message was posted on these three platforms with an explanation of the study's aim and a link that participants could click on that took them to the Qualtrics questionnaire. Participants then gave informed consent by reading a participant information form on the first page of the online Qualtrics survey and selecting ‘yes’ before completing the two sensory processing scales.
Results
Demographics
A total of 70 individuals accessed the online Qualtrics link. Table 1 summarizes participant data, including a breakdown of incomplete versus complete online survey attempts with explanations. Five individuals opened the link but provided no information; two opened the link but did not complete the survey in its entirety; eight were excluded for being known to the researcher; and four were excluded for not meeting the inclusion criteria. Thus, 50/70 participants (71.4% of participants) were included in the study sample with complete datasets.
Participant Completion Information (n = 70).
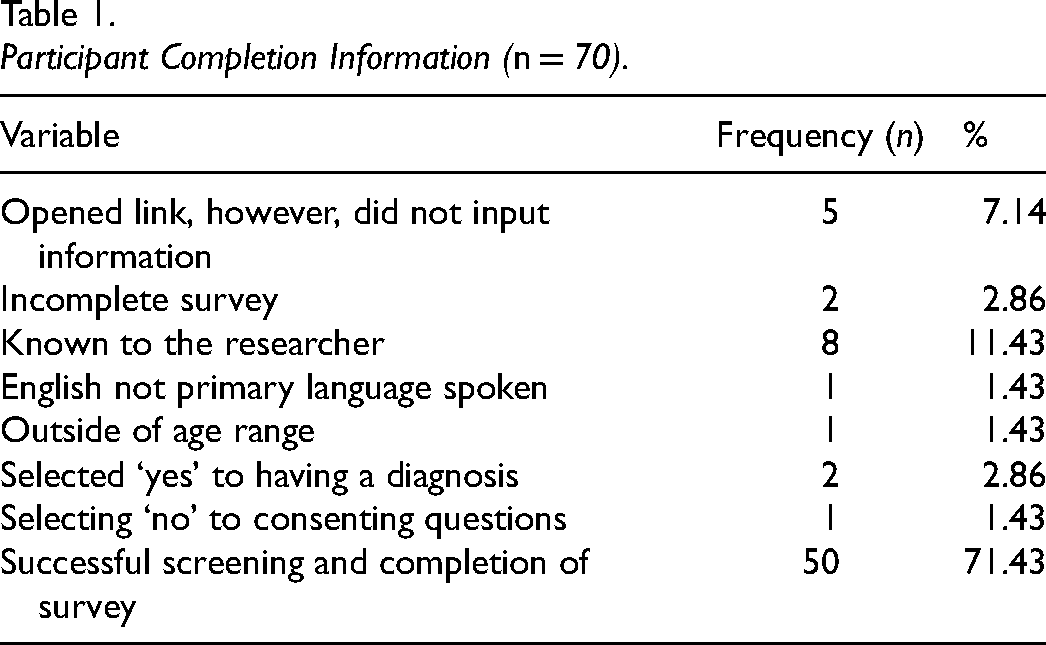
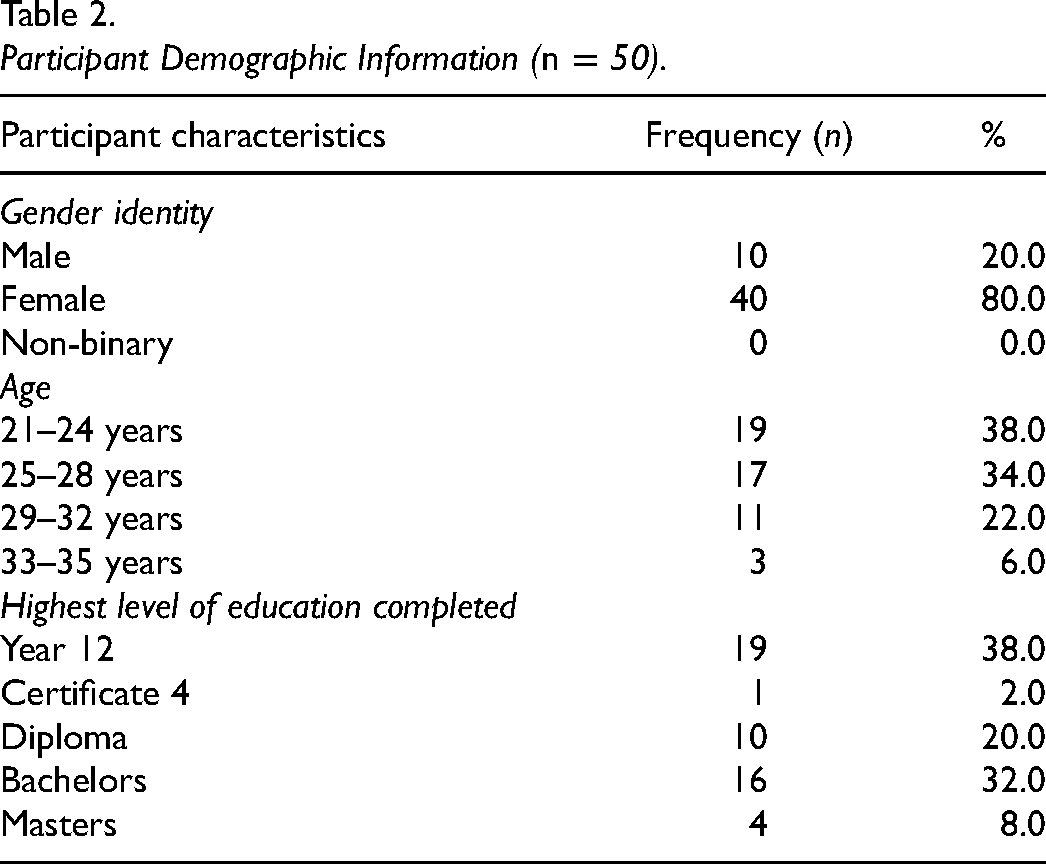
Table 2 outlines the descriptive statistics of the study participants. Within the sample (n = 50), 40 (80%) identified as female and 10 (20%) identified as male. Participants’ level of educational achievement ranged from completing Year 12 to completing a Master’s Degree. The average age of participants fell into the 21–24 age range (38%).
Participant Demographic Information (n = 50).
Spearman rho Correlations Between the SPM-2-Adult Subscales, SPM-2-Adult Total Score Scale, ASH Sensory Section Subscales and ASH Total Score Scale
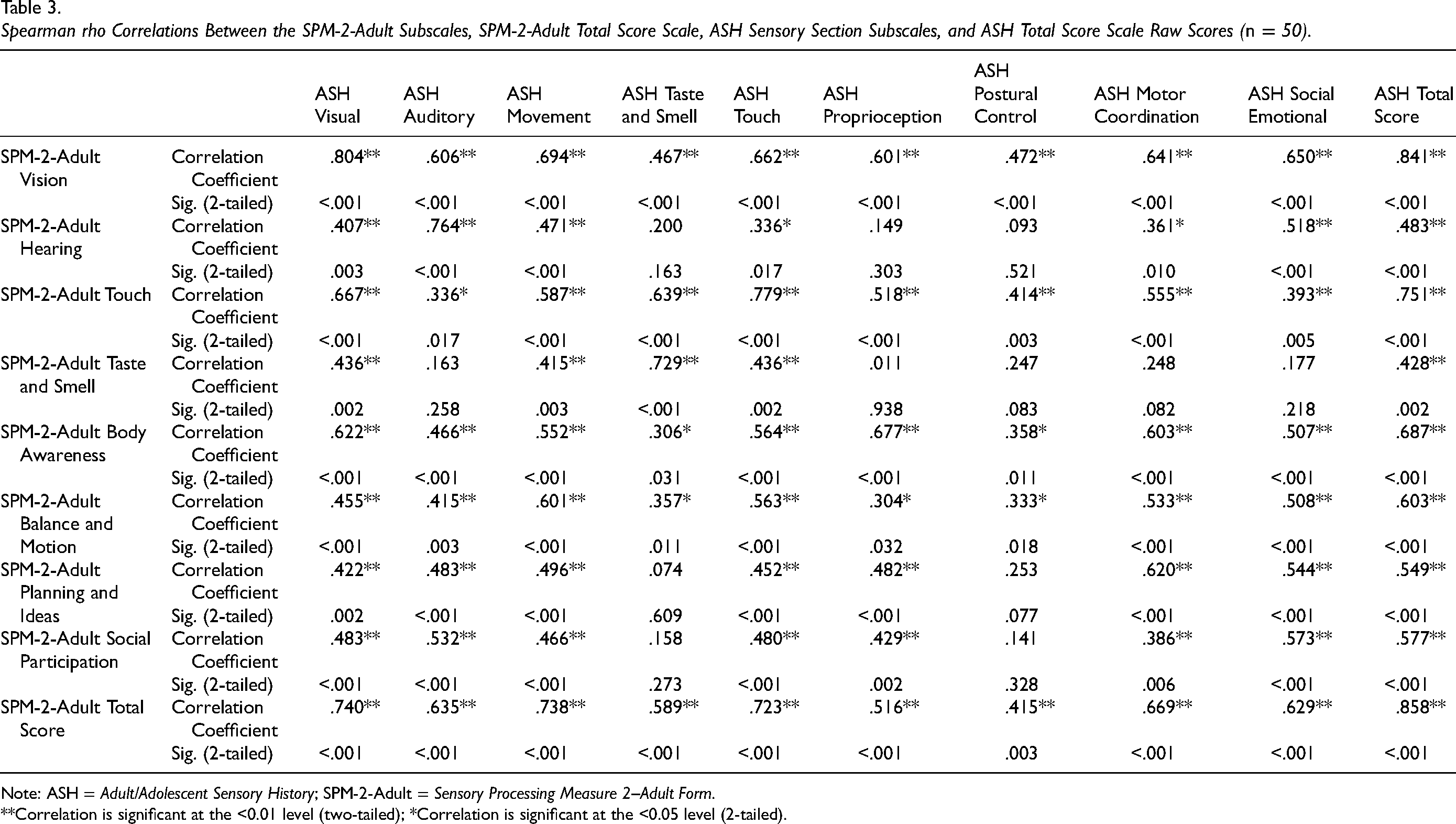
Table 3 presents the Spearman rho correlations between the SPM-2-Adult and ASH sensory subscales. It also reports the correlations between the SPM-2-Adult Total Score and ASH Total Score scales. Overall, statistically significant weak to strong correlations ranged from 0.304 to 0.858 (p < .05 to p < .001) respectively. However, most of the statistically significant correlations fell in the moderate strength range (see Table 3). None of the correlation coefficients were negative (see Table 3). In total, Table 3 reports the results of 90 Spearman rho correlations. Of those correlation coefficient results, based on the correlation coefficient size descriptors provided by Schober et al. (2018), 12 (13.3%) were not statistically significant, 10 (11.1%) had statistically significant correlations that were weak, 63 (70%) were categorized as moderate, and 5 (5.6%) were categorized as strong.
Spearman rho Correlations Between the SPM-2-Adult Subscales, SPM-2-Adult Total Score Scale, ASH Sensory Section Subscales, and ASH Total Score Scale Raw Scores (n = 50).
Note: ASH = Adult/Adolescent Sensory History; SPM-2-Adult = Sensory Processing Measure 2–Adult Form.
**Correlation is significant at the <0.01 level (two-tailed); *Correlation is significant at the <0.05 level (2-tailed).
The SPM-2-Adult Total Score subscale exhibited moderate to strong positive correlations with all nine ASH subscales and the ASH Total scale, ranging from 0.516 to 0.858 (p < .001) (see Table 3). Specifically, the SPM-2-Adult Total Score scale was significantly correlated with the ASH Visual (rho = 0.740, p < .001), ASH Movement (rho = 0.738, p < .001), ASH Touch (rho = 0.723, p < .001), and ASH Total Score (rho = 0.858, p < .001) displaying strong positive correlations respectively. The remaining ASH subscales achieved moderate level positive correlations ranging from rho = 0.415 to 0.669 (p < .001), respectively.
The SPM-2-Adult Vision subscale displayed moderate to strong positive correlations with all nine ASH subscales and the ASH Total Score scale, ranging from 0.467 to 0.841 (p < .001). Specifically, the SPM-2-Adult Vision subscale has a strong positive correlation with the ASH Visual (rho = 0.804, p < .001) subscales and the ASH Total Score scale (rho = 0.841, p < .001). The remaining ASH subscales all displayed moderate positive correlations with the SPM-2-Adult subscale (see Table 3).
The SPM-2-Adult Hearing subscale was significantly correlated with six out of the nine ASH subscales with the coefficients ranging from weak to moderate (rho = 0.361–0.518, p < .01–.001) (see Table 3). The SPM-2-Adult Hearing subscale was significantly and positively correlated with the ASH Total Score scale at a moderate level (rho = 0.483, p < .001). There were three ASH subscales that did not significantly correlate with the SPM-2-Adult Hearing subscale: the ASH Taste and Smell, ASH Proprioception, and ASH Postural Control subscales respectively.
The SPM-2-Adult Touch subscale was significantly correlated with all nine of the ASH subscales with the coefficients ranging from weak to moderate (rho = 0.336–0.779, p < .017–.001) (see Table 3). The SPM-2-Adult Touch was significantly and positively correlated with the ASH Total Score scale at a strong level (rho = 0.751, p < .001).
The SPM-2-Adult Taste and Smell subscale presented the weakest positive correlations, with five of the nine ASH subscales having no statistically significant coefficients ranging from 0.011 (p < .938) to 0.248 (p < .082). These ASH subscales included ASH Auditory (rho = 0.163, p < .258), ASH Proprioception (rho = 0.011, p < .938), ASH Postural Control (rho = 0.247, p < .083), ASH Motor Coordination (rho = 0.248, p < .082) and ASH Social Emotional subscales (rho = 0.177, p < .218). The SPM-2-Adult Taste and Smell subscale was significantly and positively correlated with the ASH Total Score scale at a moderate level (rho = 0.428, p < .002).
The SPM-2-Adult Body Awareness and SPM-2-Adult Balance and Motion subscales were significantly and positively correlated with all nine of the ASH subscales at weak to moderate levels (rho = 0.304–0.677, p < .032–.001) (see Table 3). Similarly, the SPM-2-Adult Body Awareness and SPM-2-Adult Balance and Motion subscales were significantly and positively correlated with the ASH Total Score scale at moderate levels (rho = 0.603–0.687, p < .001).
The SPM-2-Adult Planning and Ideas and SPM-2-Adult Social Participation subscales were significantly and positively correlated with seven out of the nine ASH subscales at weak to moderate levels (rho = 0.386–0.573, p < .006–.001) (see Table 3). Notably, the SPM-2-Adult Planning and Ideas and SPM-2-Adult Social Participation subscales were not significantly correlated with the ASH Taste and Smell and ASH Postural Control subscales respectively (rho = 0.074–0.253, p < .609–.077) (see Table 3). In addition, the SPM-2-Adult Planning and Ideas and SPM-2-Adult Social Participation subscales were significantly and positively correlated with the ASH Total Score scale at moderate levels (rho = 0.603–0.687, p < .001).
Spearman rho Correlations Between the SPM-2-Adult Subscale and ASH Functional-Problem Subscale Scores
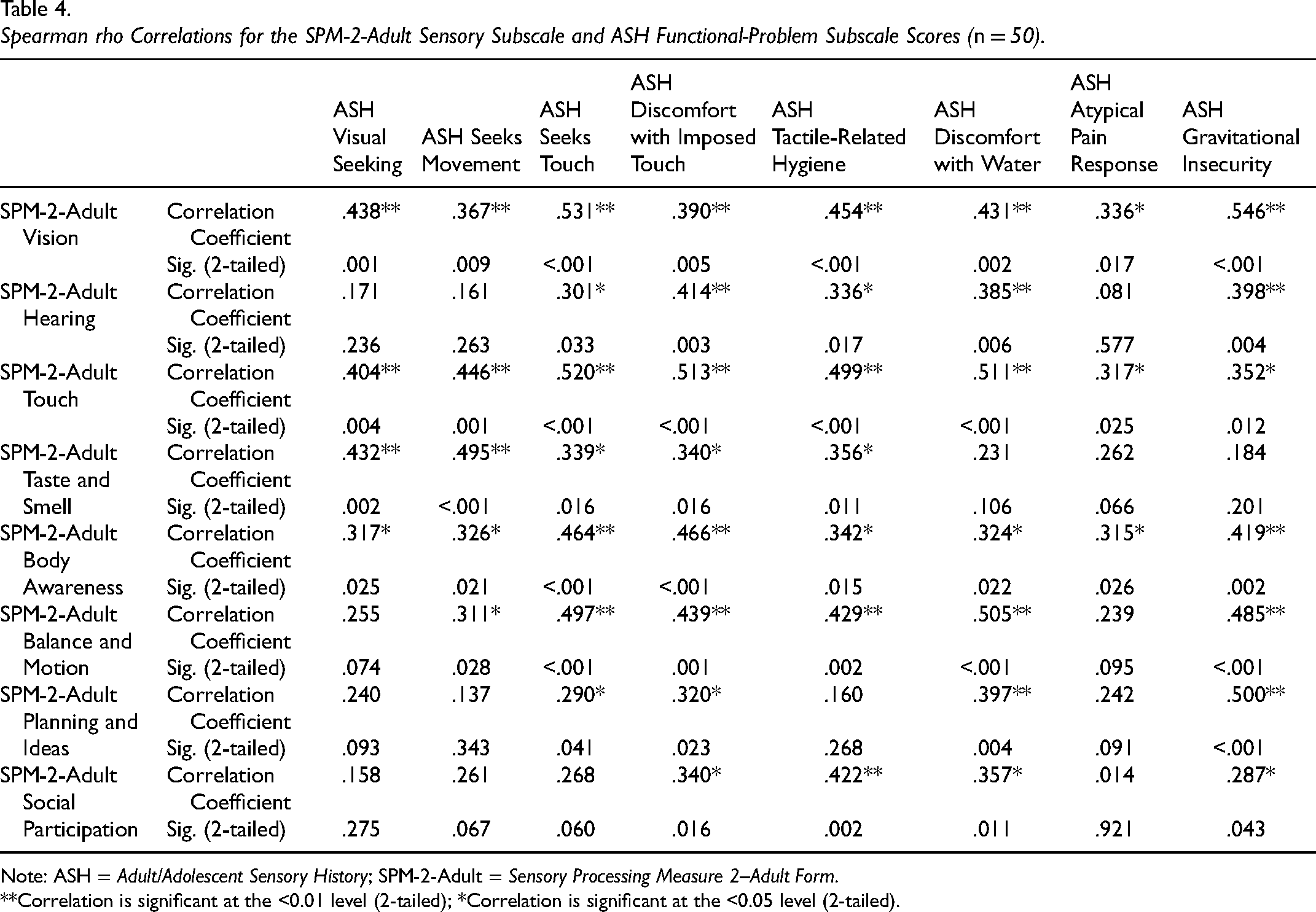
Table 4 presents the Spearman rho correlations between the SPM-2-Adult subscales and the ASH Functional-Problem subscale scores. Overall, all the statistically significant positive correlations fell in the weak to moderate strength range (see Table 4). None of the correlation coefficients were negative (see Table 4). Statistically significant correlations ranged from the lowest, the SPM-2-Adult Social Participation subscale with the ASH Gravitational Insecurity subscale (rho = 0.287, p < .043), to the highest, the SPM-2-Adult Vision with the ASH Gravitational Insecurity subscale (rho = 0.546, p < .001). In total, Table 4 reports the results of 64 Spearman rho correlations. Of those correlation coefficient results, based on the correlation coefficient size descriptors provided by Schober et al. (2018), 16 (25%) were not statistically significant, 23 (35.9%) had statistically significant correlations that were weak, 25 (39.1%) were categorized as moderate in level and 5 (5.6%) were categorized as strong in level.
Spearman rho Correlations for the SPM-2-Adult Sensory Subscale and ASH Functional-Problem Subscale Scores (n = 50).
Note: ASH = Adult/Adolescent Sensory History; SPM-2-Adult = Sensory Processing Measure 2–Adult Form.
**Correlation is significant at the <0.01 level (2-tailed); *Correlation is significant at the <0.05 level (2-tailed).
Statistically significant correlations were obtained across the board for the SPM-2-Adult Vision, SPM-2-Adult Touch and SPM-2-Adult Body Awareness with all eight of the ASH Functional Problem subscales. Within the SPM-2-Adult Vision subscale, the lowest and highest significant positive correlations were with the ASH Atypical Pain Response (rho = 0.336, p < .001) and ASH Gravitational Insecurity (rho = 0.546, p < .001) subscales, respectively. For the SPM-2-Adult Touch subscale, the lowest statistically positive significant correlation was with ASH Atypical Pain Response subscale (rho = 0.317, p < .025), while the highest significant correlation with ASH Seeks Touch subscale (rho = 0.520, p < .001). Finally, the SPM-2-Adult Body Awareness had the lowest significant correlation with ASH Atypical Pain Response subscale (rho = 0.315, p < .026), and the highest significant correlation with ASH Discomfort with Imposed Touch subscale (rho = 0.466, p < .001) respectively (see Table 4).
The SPM-2-Adult Hearing, Planning and Ideas, and Social Participation subscales were significantly correlated at the weak to moderate level with only four of the eight ASH Functional Problem subscales (rho = 0.290–0.500, p < .043–.001) (see Table 4). They showed non-significant correlations with three of the same ASH subscales, which were ASH Visual Seeking, ASH Seeks Movement, and ASH Atypical Pain Response subscales (rho = 0.014 to 0.171, p < .921–.067) (see Table 4).
The SPM-2-Adult Taste and Smell subscale was statistically significantly correlated with five of the eight ASH Functional Problem subscales (rho = 0.339–0.495, p < .016–.002) (see Table 4). The SPM-2-Adult Balance and Motion subscale was statistically significantly correlated with six of the eight ASH Functional Problem subscales (rho = 0.311–0.505, p < 0.028–.001) (see Table 4). The statistically significant correlation coefficients between the SPM-2-Adult Taste and Smell and SPM-2-Adult Balance and Motion subscales and the ASH Functional Problem subscales were in the weak to moderate strength range (rho = 0.311–0.505, p < .028–.001).
Discussion
Correlations Between the SPM-2-Adult Subscales, SPM-2-Adult Total Score Scale, ASH Sensory Section Subscales and ASH Total Score Scale Scores
The present study examined the convergent validity of two newly established sensory processing assessments: the ASH (May-Benson, 2021) and the SPM-2-Adult (Parham et al., 2021). As the importance of addressing sensory processing in young adults with known conditions or diagnoses becomes more recognized, accurate and reliable assessments are needed to guide clinical practice and support its implementation. Thus, establishing the convergent validity between these two scales is critical for contributing to the current evidence base and supporting healthcare professionals in making informed decisions when selecting sensory processing assessments.
Spearman rho correlations examined the associations between the SPM-2-Adult and ASH subscale and Total Score scale raw scores. This study's findings indicated weak to strong statistically significant correlations (p < .05–.001) ranging from rho = 0.304 to 0.858 between the subscales of the SPM-2-Adult and ASH subscale and Total Score scales. It is important to note that the majority of the statistically significant correlations fell in the current study in the moderate range as proposed by Schober et al. (2018) who specified that coefficients falling between 0.40 and 0.69 represent this level of associations. This indicates a moderate degree of association between the sensory processing factors that both tools measure in terms of sensory processing patterns in young adults based on the results of the current study.
Given these benchmarks, the strongest relationships were obtained between the SPM-2-Adult Vision and ASH Visual subscales (rho = 0.804, p < .001) and the total scores of both assessments (rho = 0.841, p < .001). In the SPM-2 User Manual, Parham et al. (2021) explored the convergent validity between the SPM-2-Adult and the A/ASP. Findings highlighted that SPM-2-Adult Sensory Total had the highest correlation, which was 0.63 (Parham et al., 2021). This is supported by the findings in this study, with both the SPM-2-Adult Total Score and ASH Total Score having moderate to strong level correlation coefficients ranging from 0.415 (p < .003) to 0.858 (p < .001). However, contextually in the current study, most of the statistically significant correlation coefficients fell in the moderate range.
Of further significance, SPM-2-Adult Vision (rho = 0.467‒0.841), Touch (rho = 0.336‒0.779), Body Awareness (rho = 0.306‒0.687), Balance and Motion (rho = 0.304‒0.603) and Total Score (rho = 0.415‒0.858) all had statistically significant correlations (p < .05‒p < .001) with all of the ASH subscales and the ASH Total Score scale, respectively. These results suggest that since both assessments are based on the same theoretical framework of Ayres’ Sensory Integration® (Ayres, 2005), their high levels of correlation indicate that they are aligned in measuring critical aspects of that theory. Further, either scale can be used to identify sensory processing patterns that may influence participation in daily activities, social interactions and overall well-being (Dunn & Brown, 2002). However, slight differences in correlation coefficient levels indicate potential differences that could guide the choice of the most suitable scale for specific sensory domains or clinical groups.
Moderate-level positive correlations between the SPM-2-Adult Vision subscale and various ASH subscales (such as ASH Auditory, ASH Movement and ASH Touch) indicate that although vision can be a critical sensory domain, auditory and tactile processing systems also significantly contribute to the overall sensory profile of an individual. These results align with studies emphasising multimodal sensory integration as essential for everyday functioning (Ben-Sasson et al., 2009a; Schaaf & Lane, 2015). For example, in the study by Ben-Sasson et al. (2009a), 925 school-aged children aged 7–11 participated in a study exploring sensory over-responsivity (SOR) towards tactile and auditory input. Findings indicated that 16.5% (n = 148) had SOR scores above the cut-off of having at least four bothersome sensations. These results further concluded that difficulties responding to different sensory stimuli can interfere with a person's participation in daily activities (Ben-Sasson et al., 2009a). While Ben-Sasson et al.'s (2009a) study focused on children, studies conducted in the United States by Metz et al. (2019), Pfeiffer et al. (2014) and Miller et al. (2023), with sample sizes of 139, 95 and 11, respectively, explored sensory processing in adults and obtained similar findings. This indicates that difficulties interpreting and responding to sensory stimuli can affect the occupational performance of individuals in this age group.
Furthermore, the weaker correlations observed for the SPM-2-Adult Taste and Smell subscale, particularly with the ASH subscales (e.g., rho = 0.011‒0.248), suggested that this domain might be less consistently measured between the two scales. The SPM-2-Adult Hearing, Taste and Smell and Balance and Motion subscales are composed mostly of over-reactivity items; thus, a high raw score indicates more intense responses to stimuli (Parham et al., 2021). However, this study's results suggested that 50% of the time, there are weak correlations between the ASH Auditory, Proprioception, Postural Control, Motor Coordination and Social Emotional subscales.
In sum, the nine SPM-Adult sensory subscales were all significantly correlated with the each of their corresponding ASH sensory subscales. For example, the SPM-2-Adult Hearing, Taste and Smell and Balance and Motion sensory subscales were all significantly correlated with their matching ASH Auditory, Taste and Smell, Postural Control, and Motor Coordination sensory subscales respectively. In addition, the SPM-2-Adult Total Score was significantly correlated with all nine of the ASH sensory subscales and the ASH Total Score. This provides convincing evidence of convergent validity between the ASH and SPM-2-Adult subscales and total scale scales when completed by young adults. However, it is important to note that the majority of the statistically significant correlations obtained between the SPM-2-Adult subscales, SPM-2-Adult Total Score scale, ASH Sensory Section subscales and ASH Total Score Scale scores fell in the moderate range.
Correlations Between the SPM-2-Adult Sensory Subscale and ASH Functional-Problem Subscale Scores
This study also aimed to explore the relationship between the SPM-2-Adult and the ASH Functional-Problem subscales. The results indicate weak to moderate correlations. This suggests different levels of connection between sensory processing challenges and adult functional problems. Within the ASH Functional-Problem subscales, items are categorized into ‘sensory seeking’ or ‘sensory over-responsivity’. Kirby et al. (2015) characterized sensory-seeking individuals as those who actively look for more sensory stimulation. Examples of these behaviours include jumping, fidgeting and touching things to receive more sensory input from one's environment. Meanwhile, sensory over-responsivity is a behavioural response in which individuals experience sensations too easily, intensely and for prolonged periods (Ben-Sasson et al., 2009a). This may involve extreme sensitivity or avoidance of sensory stimuli like scratchy fabrics, foods with certain consistencies, strong smells or loud noises.
Using sensory processing assessments such as the ASH or SPM-2-Adult, occupational therapists can gain a holistic understanding of how sensory seeking and sensory over-responsivity behaviours affect people's daily functioning. In the context of sensory seeking or over-responsivity behaviours, occupational therapists can assist in developing compensatory strategies to improve engagement in meaningful occupations. They can also implement environmental modifications to support individuals’ sensory processing difficulties and promote occupational participation (Bass et al., 2024).
The strongest relationships were observed in the SPM-2-Adult Vision, Touch and Body Awareness subscales, which demonstrated statistically significant correlations with various ASH Functional-Problem subscales in the weak to moderate range. Specifically, the SPM-2-Adult Vision subscale exhibited a moderate correlation with the ASH Gravitational Insecurity subscale (rho = 0.546, p < .001); the SPM-2-Adult Touch subscale had a moderate correlation with the ASH Seeks Touch subscale (rho = 0.520, p < .001); and the SPM-2-Adult Body Awareness subscale was moderately correlated with the ASH Discomfort with Imposed Touch (rho = 0.466, p < .001).
These moderate-level correlations highlight the critical role vision, touch and body awareness have on tactile, balance and movement-related sensory stimuli. In a practical context, the connection between body awareness and discomfort with imposed touch may imply that challenges in perceiving one's body in space could result in unease with unexpected touch, thus influencing how individuals engage with the world around them.
In a study conducted by Choi et al. (2022), the importance of understanding how sensory stimuli interact with each other for occupational therapists was emphasized. The study involved 104 Taiwanese students, 62 (59.6%) of whom were visually impaired. It aimed to investigate the impact of visual impairment on balance and visual processing functions. The findings indicated that visual impairments were associated with decreased postural control and spatial awareness (Choi et al., 2022). This highlights the significant role of various sensory processes in individuals’ functional abilities, which are crucial for their development and learning. The study, along with findings from Hutmacher (2019), which identified vision as our most important and complex sense, emphasizes the importance of occupational therapists recognising the potential connection between vision and other sensory processes.
On the other hand, the SPM-2-Adult subscales for Planning and Ideas and Social Participation exhibited lower-level significant correlations with the ASH Functional-Problem subscales. Specifically, four out of eight ASH Functional-Problem subscales were not significantly linked with these two SPM-2-Adult subscales. Furthermore, the ASH Atypical Pain Response subscale was not significantly correlated with most of the SPM-2-Adult subscales and when significant correlations did occur, they were at a weak level. These results suggest that sensory processing challenges in planning and social participation could involve more complex factors beyond sensory input, such as cognitive, social-emotional or environmental elements.
This is supported by the results of a study conducted by Jaiswal et al. (2020). Sixteen older adults (mean age = 86 years, SD = 7; 9 female) were interviewed to explore the barriers and facilitators that influence social participation in older adults with dual sensory impairment. Findings highlight that environmental factors, such as societal and personal attitudes, access to technology, availability of transportation and the accessibility of the built environment, were key factors in minimising social participation instead of sensory impairment. This highlights the need for further research to better understand the factors affecting functional problems, excluding sensory processing difficulties.
Compared to the correlation results between the corresponding ASH and SPM-2-Adult sensory subscales, there was a mixed pattern of both significant and non-significant correlations between the ASH Functional-Problem subscales and the SPM-2-Adult sensory subscales. For example, the ASH Visual Seeking subscale was not significantly correlated with the SPM-2-Adult Hearing, Balance and Motion, Planning and Ideas and Social Participation subscales. Likewise, the SPM-2-Adult Social Participation subscale was not significantly correlated with the ASH Visual Seeking, Seeks Movement, Seeks Touch, and Atypical Pain Response subscales. Finally, the ASH Atypical Pain Response subscale did not significantly correlate with five out of the eight SPM-2-Adult sensory subscales. In summary, the convergent validity evidence between the ASH Functional-Problem subscales and the SPM-2-Adult sensory subscales was not as consistent or robust even though both scales are based on Ayres’ Sensory Integration® theoretical principles (Ayres, 2005).
Implications for Occupational Therapy
This study indicated a moderate degree of correlation between the ASH and SPM-2-Adult subscales and total scales. This has several notable implications for occupational therapy practice. Since both self-report scales are based on Ayres’ Sensory Integration® theory (Ayres, 2005), they were predicted to significantly correlate, which the study findings confirmed. This suggests practitioners can confidently choose either the ASH or the SPM-2-Adult, knowing they reflect similar sensory constructs. It should be noted however that there was moderate convergent validity evidence between the ASH and SPM-2-Adult sensory subscales whereas the convergent validity findings between the ASH Functional Problems subscales and the SPM-2-Adult sensory subscales was less consistent and robust.
Secondly, the findings contribute to the overall convergent validity body of evidence between the ASH and SPM-2-Adult. The significant correlations indicate that both scales appear to measure similar sensory processing constructs, providing additional psychometric evidence and understanding about the assessment of adults’ sensory processing. Furthermore, by recruiting Australian adults, this study provides crucial evidence for the ASH's applicability in Australia, where it has not been formally examined previously. The confirmed correlation between the ASH and SPM-2-Adult underscores their utility in cross-cultural enviroments like Australia.
Limitations
The following limitations are notable for the study. The use of convenience sampling through social media may have introduced bias, which could limit the generalisability of the results. The gender imbalance, with significantly more participants who self-identified as female, also limits the applicability of the findings across genders. Additionally, self-report measures are susceptible to social desirability bias, potentially affecting participants’ responses.
Future Research
Going forward, future research could use random sampling methods to ensure an unbiased representation, making the results more generalizable. To address the gender imbalance observed in the current study, future studies should aim for a more balanced distribution of participants across gender identities. To reduce the order effect, further studies should consider randomizing the order in which participants complete the ASH and SPM-2-Adult. This will help minimize potential bias and improve the robustness of the data.
Conclusion
The study examined the convergent validity between the ASH and SPM-2-Adult, finding frequent and statistically significant correlations between their respective subscales and total scales. However, the percentage of statistically significant correlations between the ASH and SPM-2-Adult sensory subscales and total scales were larger than the percentage of significant correlations between the ASH Functional-Problem and SPM-2-Adult sensory subscales even though both scales are based on Ayres’ Sensory Integration® theoretical principles (Ayres, 2005).
The statistically significant correlations between the ASH and SPM-2-Adult sensory subscales and total scales ranged from weak to strong, with most falling in the moderate range. In contrast, the significant correlations between the ASH Functional-Problem subscales and the SPM-2-Adult sensory subscales were limited to the weak to moderate range. In sum, the study results significantly contribute to the psychometric evidence based on the ASH and SPM-2-Adult within the Australian context and support their use with adults. The study findings will inform occupational therapists’ decision making and professional reasoning when assessing adults’ sensory processing needs and their impact on their daily occupational participation.
Key Message
Many ASH and the Sensory Processing Measure 2–Adult Form (SPM-2-Adult) sensory subscales and total scales were significantly correlated with each other, demonstrating promising evidence of convergent validity between the two scales.
Significant weak to moderate level correlations were obtained between ASH Functional-Problems and SPM-2-Adult sensory subscales.
This study provides concurrent validity evidence to support clinicians in the informed selection of sensory processing measures for young adult populations.
Plain Language Statement
Occupational therapists often use standard assessments to help clients and their families understand how people process sensory information. This is called sensory processing, which is how our brains receive and respond to information from our senses, like smell, taste, and sound. There are not many studies comparing different sensory assessments, like the ASH and the SPM-2-Adult. This study looked at how well these two assessments agree with each other. Fifty adults aged 21‒35 in Australia took part by completing both assessments online. The researchers used statistical methods to see how the ASH and SPM-2-Adult were related. Consumers and community members did not help with the study's design or analysis. They found that the pattern and number of significant correlations between the ASH and SPM-2-Adult sensory subscales were more consistent than the number and range of significant correlations between the ASH Functional-Problem and SPM-2-Adult sensory subscales. Overall, the study gives important insights into how sensory processing can be assessed in young adults using either the ASH or SPM-2-Adult.
Footnotes
Acknowledgements
The authors acknowledge the Traditional Custodians of the Australian lands where this study was conducted and thank the participants who volunteered their time.
Author Contributions
All four authors contributed to the following components: study design, data analysis, methodology, review, editing and supervision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.