
Abstract
Introduction
Access to mental health services in Canada is problematic, with over 56% of people who are struggling with mental health issues not getting the help they need (Mental Health Research Canada, 2022). Access to evidence-based psychotherapy and counseling approaches, such as cognitive-behavioural therapy (CBT) and mindfulness-based interventions (MBI), are a key focus of national initiatives to promote access to mental health services (Mental Health Commission of Canada [MHCC], 2017; Vasiliadis et al., 2017). Many approaches have substantive evidence for their impact on reducing symptoms, from anxiety and depression to substance use and post-traumatic stress disorder (Roth & Fonagy, 2006), even though drop-out rates can be an issue (range from 15–46%) (Swift & Greenberg, 2012; Wierzbicki & Pekarik, 1993).
Canadians seek psychotherapy services from a range of providers, including occupational therapists, psychologists, psychiatrists, social workers, nurses, and mental health counselors (Bartram, 2019; Moroz et al., 2020; Vesely et al., 2023). Access can be a problem, however, since most services are not funded publicly outside of hospital or physician-based therapy (MHCC, 2017). Active lobbying efforts for public funding of psychotherapy services in Canada are fueled by arguments about efficacy, cost-effectiveness (MHCC, 2017; Vasiliadis et al., 2017), and access (Moroz et al., 2020). A Mental Health Commission of Canada (2018) discussion paper called for expanded access to publicly funded psychotherapy services, citing successful implementation in other countries and the importance of equitable access to evidence-based approaches. Psychologists, physicians, and social workers were cited as potential psychotherapy service providers, but occupational therapists were excluded. Other professions, service users, and decision makers may not be aware of the unique and important contribution that occupational therapists can make in the delivery of occupation-based psychotherapeutic services, and in advancing research and practice related to occupational outcomes. Evidence regarding psychotherapy typically focuses on changes to symptoms rather than function, even though people typically seek out psychotherapy to cope with functional challenges in their day to day lives (Cook et al., 2017; Roth & Fonagy, 2006). In this changing landscape, occupational therapists must establish and promote their competence and convey their unique and longstanding contributions to the field.
Occupational therapy (OT) has a long history of incorporating psychotherapeutic techniques into practice. A recent scoping review of the occupational therapy literature noted that occupational therapists offered psychodynamic arts-based therapy in research and practice as early as 1947 with evolution over time in the modalities provided (Marshall et al., 2022). There continue to be debates, however, about whether psychotherapy is part of the occupational therapy scope of practice. Some have argued that occupational therapists should not use generic interventions such as CBT, since this could exacerbate role confusion and loss of professional identity (Reeves & Mann, 2004), whereas others argued that psychotherapy approaches outside the profession can be adopted as long as we do not lose our focus on occupation and occupational performance (Ashby et al., 2017; Harrison, 2003). Since psychological theories dominate mental health practice, it can be difficult for occupational therapists to balance the pressures of adopting psychological approaches with occupation-focused treatment (Ashby et al., 2017).
Over time, unique occupational therapy approaches are being reported, rooted in the importance of activity and occupation in improving mental health, such as the occupation-centred framework for trauma intervention (Edgelow & Cramm, 2020), the combined model of human occupation and dialectical behavioural therapy (DBT) approach for treatment of women with borderline personality disorder (Lee & Harris, 2010), the Tree-theme method for exploring the narratives of individuals with anxiety and depression (Gunnarsson et al., 2010; Gunnarsson et al., 2018), and CBT approaches to occupational engagement (Ikiugu & Taff, 2025). An occupation-based approach centres activity participation in the therapy process, including a focus on functional outcomes related to occupational participation at work, home, school and/or community (CAOT, 2024; Fisher, 2014).
A small, but growing number of studies support how occupational therapists integrate evidence-based psychotherapies or approaches validated by psychologists into their practice, including cognitive-behavioral therapy (CBT) (Ikiugu & Taff, 2025; Jones, 2025; Slepecky et al., 2017), interpersonal therapy (Horton et al., 2022), acceptance and commitment therapy (du Toit, 2023; Rider & LaVerdure, 2025, Rise et al., 2015), dialectical behavior therapy (DBT) (Lee & Harris, 2010; Moro, 2007; Ward et al., 2025) and mindfulness approaches (e.g., MBCT, MBSR) (Dean et al., 2017; Reid et al., 2013; White et al., 2020), in a range of inpatient and outpatient settings (Marshall et al., 2022; Moll et al., 2013). There is also a growing number of studies in the occupational therapy literature which focus on the importance of occupation-based outcomes (Ikiugu & Taff, 2025; Jones, 2025; Slepecky et al., 2017), but evidence to date continues to be primarily descriptive rather than a systematic evaluation with robust research designs.
One of the important issues which exacerbates current tensions in this area is the broad definition of psychotherapy. Psychotherapy refers to “planned and structured interventions aimed at influencing behaviour and function, by psychotherapeutic means” that is “delivered through a therapeutic relationship to change an individual's disorder of thought, cognition, mood, emotional patterns, perception, or memory that may impair the individual's judgement, insight, behaviour, communication, or social functioning as it relates to the performance of daily activities” (COTO, 2018, p. 1).
Psychotherapy encompasses many different approaches from brief solution-focused therapy to more intensive and long-term psychodynamic psychotherapy (College of Occupational Therapists of Ontario [COTO], 2018; Marshall et al., 2022). While some occupational therapists use the term psychotherapy, other terms such as ‘psychosocial intervention/rehabilitation’, ‘counselling’, or “coaching” are used to describe a broader range of mental health interventions that are inclusive of, but not limited to psychotherapy (Government of Manitoba, 2009; Ordre des psychologues du Québec, 2018). The Canadian Counselling and Psychotherapy Association (CCPA, 2021), for example, defines counselling as “the skilled and principled use of relationship to facilitate self-knowledge, emotional acceptance and growth and the optimal development of personal resources”. There is overlap between psychotherapy and counselling since they both refer to a skilled, therapeutic, relational process that is designed to promote personal growth and behaviour change. Psychotherapy can range from brief (1–2 sessions) to extended therapy (12 weeks or more), provided individually or in a group with diverse client populations throughout the lifespan (COTO, 2018; Goldfried, 2013). For the purposes of this paper, the term psychotherapy is used as an approach that is separate from health teaching or purely supportive counselling that has a more pragmatic focus on providing information, problem solving, and encouragement, rather than focusing on changing patterns of thinking or behaviour (COTO, 2018).
In some provinces, there is clear regulation about who can provide psychotherapy. In Ontario, the COTO regulates occupational therapists for use of the title and practice of psychotherapy (COTO, 2018). In Quebec, l’Ordre des psychoglogues du Québec regulates practice and title of psychotherapy for all professions, and occupational therapists must undergo a rigorous process to be authorized to practice (l’Ordre des psychologues du Québec, 2018). There is less clarity about regulation of occupational therapists using psychotherapy in other provinces such as Alberta and Manitoba (Alberta College of Occupational Therapists, 2019; Mandzuk & Wener, 2025). According to the CCPA (2021), there is regulation in place for therapists who provide counselling in New Brunswick, Nova Scotia, and most recently Alberta, with regulatory efforts underway in Prince Edward Island (PEI), Newfoundland and Labrador, Saskatchewan, Manitoba and British Columbia. However, it should be noted this advocacy for regulation is separate from requirements for occupational therapists. CAOT (2024) recently published a Psychotherapy Practice Document acknowledging that occupational therapists engage in psychotherapy; however, there is limited clarity on the regulatory requirements across Canada and processes for attaining competence. Differences in the regulatory context across the country lead to confusion regarding regulatory requirements, professional preparation for building competence, and a lack of a unified voice for our profession. Recently, Canadian researchers explored the scope of psychotherapy-related literature published by occupational therapists (Mandzuk & Wener, 2025; Marshall et al., 2022). Only one study – conducted over a decade ago – surveyed psychotherapy practices in occupational therapy, and focused solely on Ontario (Moll et al., 2013).
The purpose of our study was to explore: 1) the psychotherapy practice approaches adopted by Canadian occupational therapists; 2) therapists’ perceived competence in providing psychotherapy; and 3) perspectives regarding the relationship between occupational therapy and psychotherapy.
Methods
A sequential, explanatory, mixed methods design (quan→ QUAL) was adopted since it provided an opportunity to initially gather a broad cross-section of psychotherapy perspectives and practice patterns, followed by more in-depth regional focus group discussions to unpack the trends noted in the survey findings (Creswell & Plano Clark, 2017). The study was approved by research ethics boards at McMaster, Dalhousie University, University of Manitoba, and Université de Sherbrooke. All survey and focus group participants gave informed consent to participate.
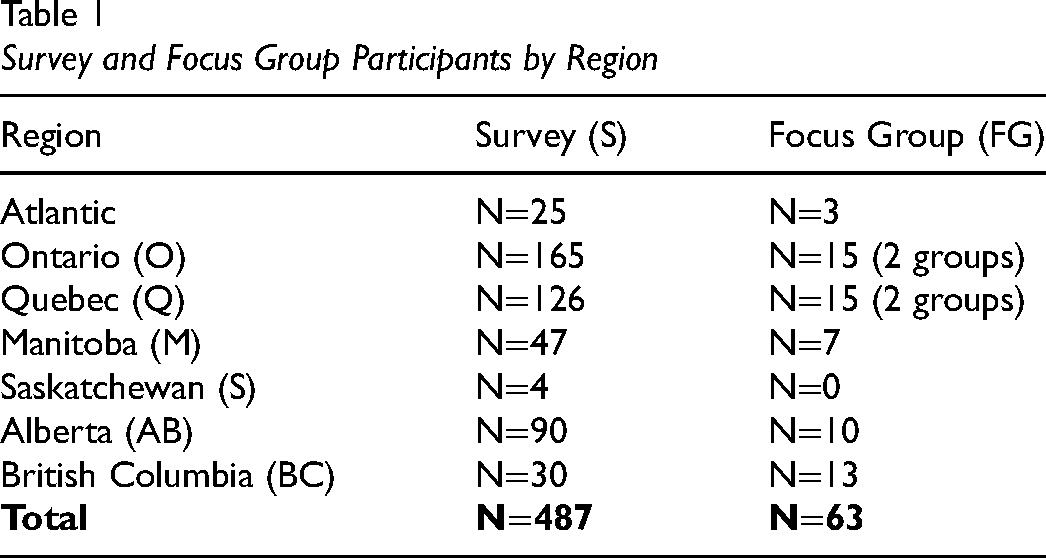
Participants for the online survey were recruited via CAOT and provincial associations, as well as university alumni and professional networks of team members. Participants had to identify as an occupational therapist in Canada who provided mental health services; they did not have to incorporate psychotherapy in their practice. Focus group participants were recruited from the survey participant sample who indicated interest in the focus group discussions as well as through additional connections of the research team. Purposive sampling sought diversity with respect to gender, years of experience, practice context (e.g., hospital, community, private), and geographical location (Teddlie & Yu, 2007). Participants were recruited for eight focus groups in six regions: Atlantic Canada, Quebec, Ontario, Manitoba, Alberta, and British Columbia. Two focus groups were conducted in both Ontario and Quebec where there are the largest number of therapists practicing in mental health.
Data Collection
Survey data were collected from November 2019 to January 2020 using the LimeSurvey online platform (LimeSurvey GmbH, 2006-2020). The survey, in both French and English included closed and open-ended questions about: a) demographics (e.g., age, gender, current role, years of experience); b) psychotherapy knowledge and training; c) psychotherapy practice patterns (e.g., client population, approaches, frequency of use, goals of therapy); d) perspectives on the relationship between psychotherapy and enabling occupation; and e) perceived facilitators or barriers to practicing psychotherapy in the context of occupational therapy practice.
Focus groups were conducted online using Zoom (Zoom Video Communications, 2018) from March to May 2020. The focus groups were video recorded and lasted 90 to 120-min. Two of the eight focus groups were in French; the others were in English. In each focus group, findings from the survey results were presented, and participants were asked to comment on each section with their impressions of the findings, including perceived barriers and facilitators to psychotherapy practice, as well as perspectives on psychotherapy from an occupational therapy lens. This approach provided participants with the opportunity to elaborate on their experiences and offer insights that may not have emerged through the survey alone (Creswell & Creswell, 2023).
Analysis
Descriptive statistics were used to analyze closed-ended survey questions. Open-ended survey responses were analyzed using inductive descriptive content analysis (Elo & Kyngäs, 2008), starting with a review of key terms, then grouping them into categories, followed by a frequency count within each category. Focus group data was transcribed verbatim, and uploaded to Dedoose, a cloud-based qualitative data management program (SocioCultural Research Consultants, 2018). Data were coded inductively using thematic analysis to identify common themes within and across focus groups, following an iterative process of familiarization with the data, generating initial codes, developing then reviewing themes, and defining and naming the themes (Braun & Clarke, 2014). VS and SM were involved in coding and analysis of the interview transcripts and identification of themes. Consultations with the full team were done to validate and refine themes and sub-themes.
It should be noted that the team members were primarily academic faculty who were engaged in teaching mental health content in occupational therapy programs across Canada. One team member (VS) was working as a research assistant and one team member joined the group to assist with manuscript revisions and updating (AM). Triangulation of researchers was important in critically reflecting on regional differences in education, and regulatory and practice contexts (Carter et al., 2014).
Results
A total of 487 participants completed the online survey (n = 369 English; n = 118 French), and there were 63 focus group participants. Table 1 outlines the location of survey and focus group participants. Most participants identified as women (88% of survey; 89% of focus group participants), with 9% of survey participants identifying as men and 1.5% as non-binary/non-conforming. The majority (71%) of survey participants identified as frontline clinicians in publicly funded settings, such as hospital (38%) or community (29%); another 21% reported working in private practice.
Survey and Focus Group Participants by Region
Psychotherapy Practice Approaches
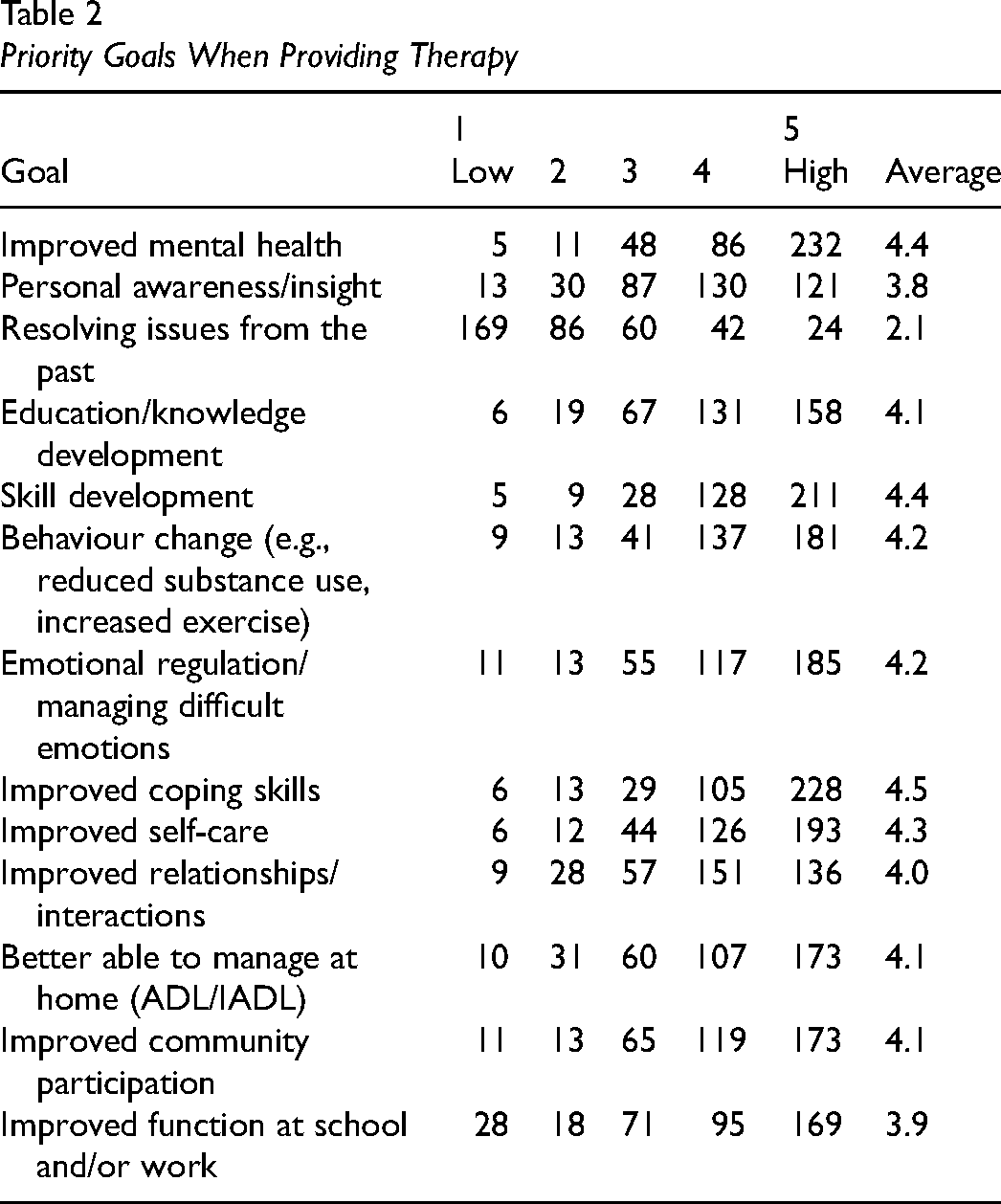
Survey participants varied in the extent to which psychotherapy was integrated into their practice, ranging from 24% who reported that it was less than 25% of their practice to 15% who reported that psychotherapy comprised their entire caseload. When asked about approaches they have used over the past five years, the four most frequently reported included: cognitive-behavioral therapy (90%); motivational interviewing (85%), mindfulness (80%), and behavioural activation (74%). Other approaches used by more than a third of participants included: dialectical behavioral therapy (41%), brief, solution-focused therapy (39%), and acceptance and commitment therapy (31%). When asked about their primary goals in providing therapy, the highest rated goals (on a priority scale of 1 to 5 where 5 is highest) included increased coping skills, improved mental health, and skill development (all rated as an average of 4.4–4.5), followed by improved self-care (4.3), emotional regulation (4.2) and behavior change (4.2). Functional performance goals were next, including managing at home, functioning at school/work, improved relationships, and community participation (range of 3.9–4.1). The lowest priority ratings were for goals related to increased insight (3.8) and resolving issues from the past (2.1). See Table 2 for details on the number of participants who provided each priority rating.
Priority Goals When Providing Therapy
Perceived Competence
Approximately half of survey participants (47%) indicated that their entry-level occupational therapy education prepared them at least moderately well for further training in counselling and/or psychotherapy. Comments reflected a desire for more hands-on practice. As one survey participant noted: “…in class learning is quite theory based and there is not too much time dedicated to practical training and skills”. When asked about post-graduate training, there was a wide range of responses, from on-the-job self-directed learning and reading, to years of formal training and supervision in specific approaches (CBT, DBT, ACT, Mindfulness etc.). When asked how important it was to receive training from an occupational therapist, 70% indicated that this was very or extremely important. Lack of training within the profession to establish competence, however, was identified as one of the main challenges for practice.
When asked to rate their perceived competence (scale of 1 to 5), all foundational skills were ranked as at least 3.3/5, with the highest rated skills as: establish a therapeutic alliance (M = 4.6), establish and maintain professional boundaries (M = 4.4), and identify limits to professional competence (M = 4.4). Some of the more complex skills were rated slightly lower, such as applying a trauma-informed approach (M = 3.5), evaluating the risks and benefits of specific approaches (M = 3.3), and discontinuing therapy (M = 3.3). Perceived competence associated with specific approaches had much lower ratings. On a scale of 0 (novice) to 5 (expert), the highest ratings noted moderate competence (average of 3.1–3.2) for CBT, mindfulness and behavioral activation, but the average ratings for other approaches were more in the novice to beginner range (e.g., 1.3 for interpersonal therapy, 1.2 for psychodynamic approaches, and 1.0 for narrative therapy). Less than half of respondents (46%) had accessed psychotherapy supervision.
Positioning Psychotherapy in Occupational Therapy: A Continuum
A key finding from the survey and focus group discussions highlights tensions in the relationship between occupational therapy and psychotherapy. In our analysis, we uncovered a continuum, where those at either end of the continuum were confident that what they offered to clients was (or was not) psychotherapy. Those in the middle wrestled with their perception of the relationship of psychotherapy practice to occupational therapy practice.
Participants from both the survey and focus groups argued that psychotherapy permeates all aspects of mental health service delivery; survey participants reported that it is “embedded” in the work that we do, and “inseparable” from our practice. A survey participant shared; “I have trouble identifying what I'm doing as a psychotherapy because what I'm doing is OT” noting that psychotherapy with a focus on occupation is occupational therapy. Many focus group participants agreed with this comment. One participant stated that “the idea of using a therapeutic relationship and influencing behaviour and function, that to me is basically the definition of occupational therapy (FG-MB). They noted the broad definition of psychotherapy which seemed to encompass much of what they did in practice.
In contrast, other participants expressed tension and lack of clarity about the fit between psychotherapy and occupational therapy explaining that psychotherapy is not universally considered part of core occupational therapy practice. One focus group participant stated, “I've experienced a little bit of my own kind of impostor syndrome about: Am I really an OT if I'm doing psychotherapy?”(FG-NS). Another participant with specialized psychotherapy training, explained that she has been questioned by colleagues about whether she is practicing as an occupational therapist. Although she clearly felt that she was “very much doing OT”, other therapists within the profession ask her “Do you miss OT?” (FG-M). One participant explained that they had completed extensive psychotherapy training, but deliberately did not link their work with psychotherapy. I've gotten, over the years, certifications in trauma psychotherapy, including cognitive processing therapy. I've mentored under a psychiatrist for dialectic behavior therapy, done groups and individual for cognitive therapy. I would never have called myself a psychotherapist or having provided psychotherapy (FG-BC)
An alternate position was a middle ground, arguing that psychotherapy is a separate yet complementary practice. This distinction was elaborated upon during the focus group discussions: I find that occupational therapy adds to psychotherapy and psychotherapy adds to occupational therapy. In some cases, I clearly see more advantages in working with OT approaches, in some other cases there are clearly more advantages in using more psychotherapy approaches (FG-Q).
Many survey participants referred to psychotherapy as being one “tool in our toolbox”. This perception was echoed by focus group participants: “I think the benefit our profession has to mental health, how we get there– it might be through psychotherapy. It might be through something else. We have maybe more tools in the toolbox than some professions when it comes to working with mental health. (FG-NS). This position foregrounded an occupational therapy perspective which may or may not include psychotherapy approaches.
Unique Occupational Therapy Approach
The idea that occupational therapists practice psychotherapy differently from other professions, was endorsed by over 72% of the survey participants. There were 263 survey responses to the open-ended question asking them to explain how our focus was different. Approximately 40% of participants referred to our unique focus on “function”; and 38% used the term “occupation” to describe our unique lens, therapeutic focus, and/or outcome of therapy. As one therapist stated: “…my [primary] goal when working with clients is not to improve their mental health, but to improve their functional capacity”. Survey respondents emphasized that an OT approach focused on application of psychotherapy strategies to enable activity engagement or participation in the context of clients’ day to day lives. For example, one respondent wrote: “The expertise of occupational therapists is the relationship between people and their occupations as an object of identity building, as a therapeutic lever, as a central object which structures and guides life, as a source of experience, etc.. Putting this into action is at the heart of our approach”. Respondents noted that our focus was more ‘practical’, ‘present focused’ and ‘action based’, as opposed to other professions who might have more of an insight-oriented approach. Approximately 11% of survey respondents emphasized the ‘holistic’ approach of occupational therapy as unique, but the term was not consistently defined. Some, for example, noted a focus on the client in the context of their environment, whereas others noted a focus beyond mental health, to consider physical and social needs. There were a small number of survey respondents (approx 3%) who weren’t sure whether our approach was significantly different. Areas of overlap were noted by some in application of psychotherapy methods (“the steps are the same”), and some expressed a desire for more direction regarding what constitutes an occupation-based approach.
In the focus group discussions, there were similar reflections from therapists on the unique focus on occupation and application to day to day life. One therapist from Manitoba, for example, explained she has many different tools (e.g., DBT, MI) that she uses on the “path toward occupation” (FG-M). Similarly, a therapist from Quebec explained that psychotherapy practiced by psychologists is about “why”, while occupational therapy is about “how” to apply principles to daily life: …I think we really have something unique to offer. I often say to my patients, “The psychologist will help you understand the why, and I'll help you figure out the how. So, defusing obstacles by grading the activity as you do it… (FG-QC)
Overall, participants perceived that there was a unique lens, grounded in the importance of occupation, that occupational therapists bring to their work and that this shapes how they practice psychotherapy.
Impact of Regulatory Context
Perspectives on the relationship between occupational therapy and psychotherapy also appeared to be influenced, in part, by the regulatory and practice context which varies between provinces. The nature of professional regulations surrounding counselling or psychotherapy was often cited as shaping not only the language used to describe what they did, but the extent to which psychotherapy was considered to be within occupational therapy scope of practice. For example, in open-ended survey answers, participants described the varying regulations of psychotherapy across Canada, contributing to the confusion about whether psychotherapy is within the scope of occupational therapy.
Unique to Quebec, several focus group participants talked about the difficult and often frustrating process to acquire the license from a college of another discipline (psychology), making licensure inaccessible for many OTs.
…in Quebec it is very complicated, there are incredible criteria, you have to redo another master's degree, in fact, to obtain a licence … it is a huge investment to become a psychotherapist… (FG-Q)
In Ontario, psychotherapy is regulated by the provincial college (COTO). Survey participants expressed concerns about the lack of clarity in COTO guidelines. Many reported feeling uneasy and threatened by potential scrutiny from COTO, especially newer therapists, who were uncertain about how to gain competence in psychotherapy. The Ontario-based focus group discussions expanded on the survey findings, elaborating on the implications of the regulatory context in Ontario and the standards outlined by the College. Some expressed concerns that the new regulatory requirements left therapists questioning if they were meeting College standards. Focus group participants talked about fears of getting “in trouble with the college,”(FG-O) therefore they were careful to engage in work that “aligns with what the [regulatory] college finds acceptable (FG-O)”. Other participants described not using the term psychotherapy to avoid complications with the regulatory college.
In other provinces, psychotherapy is not regulated as a separate mental health intervention. Rather some provinces use terms such as, “counselling” or “psychosocial intervention” that neither specify nor exclude psychotherapy. While most occupational therapists are included in the regulation to practice psychosocial interventions, survey participants commented on other professions not viewing occupational therapists as mental health professionals. Focus group participants further elaborated on concerns. We're included as somebody who is allowed to provide the psychosocial interventions, and yet, nurses and social workers and psychologists are also on there, and they all seem to know amongst each other, that they are able to do it, but for whatever reason, even though we're in that same sentence, people are always surprised when I tell them that OTs are able to provide those services (FG-AB).
In provinces moving towards regulation, there was some ambivalence and even resistance to this process, feeling that regulation might be restrictive, or exclude occupational therapy. Several focus group participants from British Columbia spoke passionately against regulation: “In BC, we don't regulate those titles or terms. And thank goodness our college is resistant to have them regulate because our Health Professions Act has really been quite clear about the harms that go with regulating terms such as like psychotherapy” (FG-BC).
In contrast, some survey participants commented that psychotherapy regulation could offer clarity and confirmation of our profession's knowledge and skills in this area. In Manitoba, where occupational therapy is included as a profession providing psychosocial interventions, focus group participants hoped that regulation could provide clarity and credibility for therapists who are trained to provide these services. The potential benefit was noted by one participant; “this is somebody that I can vouch that they have the certification necessary to operate at an official psychotherapy level.” (FG-M)
Differences from one province to the next in terms of the regulatory context were noted to be confusing for therapists who may be trained in one province and then practice in another, or who move provinces during their career. This was elaborated in focus group discussions: The lack of clarity, the lack of definition, the different legislation. Being trained in Quebec where it's very, very, very strict, I had to kind of learn that I could say I'm doing CBT in Manitoba and chart it. So even the difference between each province makes it hard (FG-M).
Lack of Recognition of Occupational Therapy Roles
When survey participants were asked to rank the main challenges or barriers for occupational therapists related to psychotherapy practice, the category of “lack of recognition of psychotherapy as part of the scope of OT practice” was ranked second highest. There were comments about lack of recognition from employers, other professionals, and the general public.
Interprofessional settings reportedly led to tensions about who can provide psychotherapy services. As one survey participant explained: “My biggest barrier has been convincing other members of my interdisciplinary team that I am trained and competent at this work. They don't understand what OT's do in general, but they are SURE we don't do psychotherapy… or at least don't do it well”. This issue was further elaborated on in the focus group discussions where participants described similar experiences of “push back” from other mental health professionals sometimes relegating occupational therapists to doing assessments and reports (FG-BC).
Lack of recognition of occupational therapists as a psychotherapy provider in some cases had an impact on how therapists were paid. Survey participants highlighted the fact that insurance companies do not provide funding for occupational therapists to deliver psychotherapy, and that other professions offering the same services are paid more. This was further supported by an Alberta focus group participant's experience of colleagues doing the same work, but with the title of ‘clinical therapist,’ earning significantly more money (FG-A).
When asked about how to address the challenges with the lack of recognition for occupational therapy, there was consensus regarding the importance of public advocacy to build recognition of our role and to access public funding for occupational therapy. One survey participant recommended that we “… promote ourselves by defining a niche or certain types of expertise such as return to productive roles, [or] specialists in reintegrating people into meaningful occupations; linking psychotherapy with real life.” Another survey participant talked about advocating for the return on investment that occupational therapists can bring: “I think given our skill set, if OT were more publicly funded or funded by insurance companies, the government and companies would get a lot of bang for their investment”. These sentiments were echoed in the focus groups, with participants recommending education of the public, employers, and insurance companies regarding the unique value that occupational therapy offers providing psychotherapy services.
Discussion
This is the first pan-Canadian mixed methods study to identify the perspectives and psychotherapy practices of occupational therapists working in mental health. The study findings raise important questions about: 1) the concept of ‘occupation-based psychotherapy’ and the extent to which this is being practiced by occupational therapists, 2) the need for competency development within the profession; and 3) how national efforts towards education and advocacy need to consider provincial differences in the regulatory context.
The survey data highlighted that the most common approaches adopted by 75–90% of participants included cognitive-behavioral therapy, motivational interviewing, mindfulness and behavioral activation; trends that are similar to a 2013 study of Ontario-based occupational therapists (Moll et al., 2013). It is important to note that these are self-report data; the degree to which therapists adopted best practice guidelines was not explored or systematically valuated, nor the extent to which these approaches were adapted to reflect an occupation-based approach to therapy. Most survey respondents were of the opinion that occupational therapists practiced psychotherapy differently from other professions, with more of a focus on occupation and promoting day-to-day function. This assertion, however, does not necessarily match the reported goals for therapy noted by the same survey respondents. When asked about the primary goals for therapy, there were some related to functional performance at home and in the community, but many were more psychologically oriented regarding improving mental health, emotional regulation and coping skills. A study of occupational therapists in Australia noted that therapists often experience tensions with respect to reconciling the pull towards psychologically oriented versus occupation-based approaches, given the dominance of psychological frames of reference (Ashby et al., 2017). Similar tensions were noted in a study of New Zealand therapists regarding adoption of counseling skills and the extent to which they were embedded in occupation-based practices (Whitcher & Tse, 2004). The varied perspectives noted by participants in this study regarding the extent to which psychotherapy was considered to be part of occupational therapy practice is therefore not unique to the Canadian context. Without clear guidelines for what constitutes an occupation-based psychotherapy approach, it may be difficult for occupational therapists to know when and how to apply their occupational therapy lens in a way that is congruent with the established practice principles of established psychotherapy interventions.
Another significant issue relates to establishing competence. The highest ratings of perceived competence were in foundational skills related to establishing a therapeutic alliance. This is particularly significant, as research consistently identifies the therapeutic alliance as the strongest predictor of therapy effectiveness, regardless of the specific intervention used (Crits-Christoph & Connolly Gibbons, 2021; Horvath et al., 2011; Norcross & Lambert, 2011). As noted in the CAOT (2024) practice document on psychotherapy, “all OTs graduate with the fundamental skills for mental health service provision including assessment skills; case conceptualization; collaborative, relationship-focused practice; and therapeutic use of self and activities” (p.1) which are foundational to competent psychotherapy practice. Competence ratings were lower, however, for specific psychotherapy approaches, reflecting that more training may be needed to provide quality services with fidelity to the established approach. A wide range of post-graduate training was reported related to specific approaches (e.g., CBT, DBT and ACT), but partcipants also noted gaps related to access to supervision and to training from an occupational therapy lens. Without clear guidance within the profession regarding an occupational therapy approach to competence development, therapists risk practicing with uncertainty, which can contribute to role confusion and dissonance and impact client outcomes (Mandzuk & Wener, 2025; Walder et al., 2022). As members of a self-regulated profession, occupational therapists must ensure they are competent by undertaking formal psychotherapy training and supervision, therefore a clear pathway is needed for occupational therapists to establish and maintain their competence in psychotherapy that is grounded in an occupational perspective (Mandzuk & Wener, 2025). Quebec is an exception, however, with clear restrictions and requirements to practice (LegisQuebec, 2012).
In Canada, occupational therapists’ scope of practice and competence development is shaped by varied provincial and territorial regulations regarding psychotherapy and the title of psychotherapist. Regulatory requirements have been clarifying for some and confusing for others. For example, participants in Ontario and Quebec reported greater regulatory clarity regarding psychotherapy practice compared to other provinces, whereas those in provinces like Manitoba and British Columbia described ongoing uncertainty about competence requirements. Despite the existence of standards for psychotherapy in Ontario, some still described the guidelines as vague, leading to hesitancy in their practice. Others even perceived the regulation as threatening, prompting them to take additional precautions to mitigate risk by avoiding the term “psychotherapy”, and labeling their practice in “acceptable” terms, such as psychoeducation (with the exception of Quebec, where psychoeducation is a profession, with a separate regulatory college) (Ordre des psychoéducateurs et psychoéducatrices du Québec, n.d.). Lack of consensus about the definition of psychotherapy across provinces and overlap with terms such as counseling and psychosocial therapy adds to uncertainty and inconsistency in how therapists position their role in the field. It can also perpetuate occupational therapists’ struggle with understanding their practice and negatively impact their professional identity (Mandzuk & Wener, 2025).
The consequences of either making a distinction between occupational therapy and psychotherapy or embracing it as part of our practice has risks and benefits for; the nature and quality of services we provide, access for service users to evidence-based care, therapist competency development, and recognition of the profession in mental health policy and practice. Benefits of embracing psychotherapy in occupational therapy practice allow for implementation of evidence-based strategies for clients with mental health issues, thereby increasing their access to services. There is a risk, however, that the pull towards a psychological approach focused on symptom reduction may detract from our occupational therapy role in enabling occupation, particularly given the dearth of OT-specific training and research evidence on an occupation-based approach to psychotherapy practice. Establishing and asserting our profession's credibility can create opportunities for employment and funding for our services, particularly given the current lobbying for public funding of psychotherapy. There is a risk, however, of ‘turf wars’ between professionals from different disciplines who do not acknowledge occupational therapists’ scope of practice and competence in psychotherapy and in mental health. Credibility must be established through clear avenues to competence, articulation of our unique approach, evidence-based research, and education outside of the profession regarding our role in providing evidence-based service to the public.
Recommendations
Given the key risks and benefits associated with linking psychotherapy and occupational therapy practice, we identify four key recommendations for the profession of OT in Canada.
Build National Guidelines for Psychotherapy
It is time to build consensus within the profession regarding terminology and utilization of psychotherapeutic techniques, highlighting occupation and occupational participation. National guidelines should build on the foundation established by the recently published Psychotherapy Practice Document (CAOT, 2024) and provide a structured framework for developing and demonstrating competence in occupation-based psychotherapy. To promote consistency across the country, these guidelines must account for differences in provincial regulations and standards and be responsive to changes over time. Establishing greater consistency within the profession will strengthen occupational therapists’ ability to present clear messages to others, including other professions, decision makers, and service users.
Build Opportunities for Psychotherapy Training, Supervision, and Support
Canadian guidelines and resources regarding competence development are needed from an occupational therapy perspective, to define safe, ethical, competent practice, and standards for training across different approaches (e.g., DBT, CBT, ACT). Dialogue across university occupational therapy training programs can create coordinated approaches to teaching foundational knowledge in the entry-to-practice curriculum, with opportunities for advanced counseling skills either within or beyond their occupational therapy degree. For ongoing training, the Compendium of Counselling and Psychotherapy Resources for Occupational Therapists developed in Ontario (Moll et al., 2015) could form a foundation for a national resource. The Compendium was designed to guide therapists to explore evidence, training requirements and resources across five psychotherapy approaches used by occupational therapists, including consideration of how they relate to occupational therapy practice. Workshops offered by provincial and national occupational therapy organizations are important opportunities for OT-specific training; they should be linked to defined pathways to competence (Mandzuk & Wener, 2025). Finally, formal supervision processes are needed to establish and build practice competence over time given the gap in access to supervision noted in this study. Supervision has been identified as a key method of attaining and maintaining competence (Mandzuk & Wener, 2025). In Ontario, the provincial association created a tool to help therapists find a qualified supervisor and set up a process of supervision; this could be expanded nationally (Ontario Society of Occupational Therapists, 2019).
Conduct Systematic Research on the Implementation and Impact of Occupation-Based Approaches in Mental Health
Much of the literature on psychotherapy is published by other professions including psychologists with an emphasis on addressing symptoms rather than a focus on occupation (Cook et al., 2017; Roth & Fonagy, 2006). Systematic research is urgently needed to establish the efficacy of an occupation-based approach in order to build credibility and raise the profile of the role of occupational therapists in mental health (Ashby et al., 2017; Mairs, 2003). This includes establishing guidelines regarding the ‘fidelity’ of occupation-based approaches on occupational challenges, and rigorous methods to evaluate the efficacy and cost-effectiveness of occupation-based therapy in mental health.
Educate the Public on the Role of Occupational Therapy in Psychotherapy
Mental health is a Canadian healthcare priority, and it is essential that resources – including healthcare providers – are utilized effectively and optimally. The political environment makes this an ideal time to raise the profile of occupational therapy at all levels in the health system and ensure inclusion in policy and program planning regarding access to psychotherapy services. Education initiatives will look different between provincial jurisdictions, given differences in terminology and regulation; therefore, cooperation and coordination are needed between national and provincial associations. Given the national lobbying by mental health advocates for public funding of psychotherapy services, it is important to raise awareness of occupational therapists’ education and skills in providing counseling and/or psychotherapeutic services. Improved documentation of training, models of occupation-based psychotherapy, and the occupational therapy role is needed with an emphasis on our unique and valued occupational perspective.
Study Strengths and Limitations
Strengths of this study include triangulation of data sources, and inclusion of a range of perspectives (diversity in age, job tenure, location, practice context). While there were over 480 survey participants, the findings cannot be generalized to all occupational therapists in Canada who work in mental health. A notable gap includes therapists working in the territories and Prince Edward Island. In addition, the healthcare environment is inherently fluid, therefore the cross-sectional nature of the data collected in 2020 represents one moment in time, and occupational therapy practice continues to evolve. It should also be noted that this study focused on therapist-reported practices, but did not evaluate the impact of these practices or the extent to which therapists followed evidence-based protocols. Future research is needed on implementation and impact before definitive claims can be made about the strength of the evidence regarding OT and psychotherapy.
Conclusion
Given the ongoing mental health challenges facing Canadians, we must understand and articulate how psychotherapy strategies provided by occupational therapists can have an integral role to play in providing equitable and fair access to psychotherapy services, particularly with respect to promoting function and community participation. Increased awareness of this role is needed both within and outside the profession. This study underscores the importance of ongoing provincial and national efforts aimed at advancing the credibility of occupational therapists in contexts where their psychotherapy role may be contested. It is important to position the profession in the local, provincial and national conversations about psychotherapeutic approaches, and speak with a clear, unified national voice regarding the unique perspective that occupational therapists contribute to the field.
Key Messages
Occupational therapists often adopt psychotherapeutic approaches such as cognitive-behavioral therapy in supporting clients with mental health issues, but there is variation in the extent to which they recognize psychotherapy as part of their scope of practice.
Differences in the regulatory context across Canada impact how occupational therapists define their role in providing counselling and psychotherapy.
Defining the unique role of occupational therapy in psychotherapy and clarifying pathways to competence is needed to raise our profile in the changing landscape of mental health service provision in Canada.
Footnotes
Acknowledgements
Thank-you to the occupational therapists across Canada who contributed to the survey and focus group discussions.
Data Availability
Corresponding author can be contacted regarding access to data
Ethics
Approval for this project was obtained through the Hamilton Integrated Research Ethics Board (2019–7485-GRA) affiliated with McMaster University. Delegated approval was also obtained through Dalhousie University, University of Manitoba, and Université de Sherbrooke. All participants (survey and focus group) provided informed consent to participate as per the ethics protocol.
Funding
Canadian Occupational Therapy Foundation, (grant number 2019-COTF).