
Abstract
Introduction
We begin this paper by recognizing that Canada is a settler-colonial state (Barker, 2014). The vibrant tapestry of Indigenous nations and communities—including First Nations, Métis, and Inuit—was profoundly disrupted by colonization on Turtle Island, now known as Canada (Borrows & Coyle, 2017). Since contact, the settler-colonial state has attempted to eradicate Indigenous Peoples and their knowledge systems through segregation, assimilation, and cultural genocide (Government of Canada, 2024; Newhouse & Belanger, 2020; Truth and Reconciliation Commission [TRC] of Canada, 2015a). These harms persist today, resulting in systemic racism, discrimination, and enduring inequities across health-care, education, housing, food security, employment, and other social determinants (Fijal & Beagan, 2019; Smylie, 2009). Indigenous Peoples who hold intersecting identities—including those who are women, queer, or transgender—face heightened rates of violence and poorer health outcomes (Restall et al., 2019). These disparities are worsened by disproportionate experiences of disability, housing precarity, and low income and are shaped by colonial social structures such as the criminal justice and child welfare systems, which continue to impose harms on Indigenous Peoples (Durand-Moreau et al., 2022; Hajizadeh et al., 2018; Smylie, 2009).
The first decade of the 2000s saw a surge in activism by Indigenous Peoples, who pressed Canada to confront these structures and act on longstanding injustices (Coulthard, 2016). This wave of activism, however, was rooted in a long history of Indigenous advocacy, which had been fighting for justice and reform for many years before the 2000s (Barker, 2014; Bell, 2015; Coulthard, 2016). Between 2007 and 2015, the Truth and Reconciliation Commission of Canada (TRC) investigated the impact of the Residential Schools system, the Indian Act, and colonization on Indigenous Peoples in Canada (TRC, 2015b). Its final report included 94 Calls to Action intended to guide reconciliation, seven of which focus on health (Hojjati et al., 2018; TRC, 2015b).
Recognizing the health-care system's obligation to the Calls to Action, the Canadian Association of Occupational Therapists (CAOT) issued a 2018 statement outlining the profession's role in advancing reconciliation (CAOT, 2018). In 2019, CAOT's Board of Directors unanimously voted to establish the CAOT TRC Task Force, co-chaired by two Indigenous occupational therapists, Angie Phenix and Kaarina Valavaara. The purpose of the Task Force was to encourage leadership in Canadian occupational therapy by supporting sustainable and culturally respectful research, applying trauma-informed principles in practice and education, and working toward reconciliation through decolonizing the profession (CAOT, 2023b). In turn, an action plan was developed (CAOT, 2023b; see also Phenix & Valavaara, 2019). This work led to active participation by the co-chairs, Indigenous occupational therapists, and allies in numerous initiatives—including formal publications, conference presentations, university research, educational partnerships, workshops, webinars, and government meetings. They also contributed to the development of the 2021 Competencies for Occupational Therapists in Canada and the Promoting Occupational Participation: Collaborative Relationship-Focused Occupational Therapy textbook (CAOT, 2023b).
In September 2023, shortly before the task force's work concluded, they produced the Occupational Therapy Statement of Commitment to Indigenous Peoples in Canada (CAOT, 2023a). This document outlines the profession's commitment to effect change through meaningful actions aimed at addressing colonialism in occupational therapy. The issued action items guiding the profession towards reconciliation align with the TRC, the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP), and the Calls to Justice from the National Inquiry into Missing and Murdered Indigenous Women and Girls (MMIWG). After the task force concluded, its work continued through the Indigenous Occupational Therapy Collective, a professional association for First Nations, Inuit, and Métis occupational therapists and students that seeks to decolonize the profession through mentorship, peer support, research and education, knowledge sharing, and advocacy, fostering dialogue and action across practice, education, and research (Indigenous Occupational Therapy Collective, 2025).
Hunter and Pride (2021) emphasize that, while the long-term goal is to develop theories, models, and assessments by and for Indigenous Peoples, there is an immediate need to critically review existing tools and resources. Until such sovereignty is realized, adapting these tools may reduce harms. For instance, Price and Pride (2023) examine the Canadian Occupational Performance Measure (COPM), noting that this tool has been developed within a Euro-Western context, prioritizes individualism, categorizes occupations, and takes a deficit orientation. The nuances of Indigenous values, aspirations, needs, and the impact and assessment of structural inequality are inaccessible to therapists who solely draw from tools developed within a Euro-Western context (Price & Pride, 2023). In response to Price and Pride's (2023) work, the authors of the COPM dismissed the concerns raised by Indigenous scholars and further asserted that the COPM is a universal and culturally sensitive tool (McColl et al., 2024). This exchange highlights the tensions that persist between dominant epistemologies and Indigenous knowledge systems, and the ways in which Indigenous perspectives are devalued. Turning back to the work of Price and Pride (2023), they further emphasize the necessity of training (including the impact of colonialism in the profession) and culturally safer practices in occupational therapy.
White and Beagan (2020) explore specific actions occupational therapists can take to advance reconciliation, such as recognizing and addressing preconceived biases when working with Indigenous clients. Fijal and Beagan (2019) propose developing an integrated Canadian Model of Occupational Performance and Engagement (i.e., ICMOP-E) that incorporates Indigenous ways of knowing. Byrne et al. (2020) further emphasize the importance of cultural safety in pediatric rehabilitation, highlighting how practitioners can develop culturally safer practices by listening to Indigenous communities’ stories, prioritizing relationship-building, and engaging in ongoing reflection to challenge their own biases and cultural assumptions. Despite these suggestions, there remains a lack of reporting on how Canadian occupational therapists currently engage in reconciliation.
Given the emphasis by professional colleges and regulatory bodies on reconciliation, this study investigates how occupational therapists implement these efforts in practice. This study seeks to answer: (1) How do occupational therapists in Alberta incorporate reconciliation into their everyday practice? (2) What are the interrelated factors influencing reconciliation efforts for occupational therapists in Alberta?
Method
Study Design
This qualitative study used interpretive description as a guiding methodology to understand how occupational therapists approach reconciliation in their practices and the interrelated factors. Interpretive description is useful for constructing practice-based knowledge and values and prioritizes practice-based interpretation of data (Thorne et al., 1997). As occupational therapists, this methodology offered latitude for us to draw from our own experiences in the construction and interpretation of our findings. This includes our experiences, as Indigenous and non-Indigenous people, in professional training (as both students and educators), and occupational therapy practice. Interpretive description is frequently employed in health-care and health-related research due to its flexibility, value for the analyst's professional and disciplinary experience, and attention to the practical implications of findings (Burdine et al., 2020; Thorne et al., 1997; Turpin et al., 2021). Its flexibility enables researchers to explore and clarify complex phenomena and the interrelationship of practice contexts, socio-political contexts, and individuals’ experiences, revealing both commonalities and unique aspects (Burdine et al., 2020). While interpretive description is useful for making sense of occupational therapists’ experiences of reconciliation in practice (see Bhandal, 2022), it stems from Western qualitative research traditions and is a colonial approach. There is potential, with interpretive description's emphasis on practical outcomes, that findings reassert or prioritize the functioning of health systems that are themselves colonial. Thus, our authorship team sought to reflexively recognize colonial mechanisms at play in our interpretation of the data.
Locating Ourselves and How We Come to This Work
This project began as the first author's Social Sciences and Humanities Research Council (SSHRC) Canada Graduate Scholarship—Master's project in 2021, supervised by the fourth author. She initially planned to develop a study that examined at the influence of social movements, such as #MeToo, on occupational therapy practices. However, during her initial literature review, she frequently reflected on her positioning as a settler (from German and French ancestry) and began grappling specifically with the implications of the TRC's Calls to Action on the occupational therapy profession. Her supervisor, also a settler (from Ukrainian ancestry), is an occupational therapy educator whose training and education has been entirely within a settler-colonial academic context. Together, the first and fourth author began to develop the current project, recognizing their complicity in colonial health services and shared obligation towards responding to both the TRC's Calls to Action and the CAOT TRC Task Force. During the early stages of project development, the first and fourth author met with an Indigenous occupational therapy scholar, who offered feedback and recommendations on the project's methods prior to submitting an ethics application. Following recruitment and data collection, the second author joined the team and participated in the analysis, contributing her perspective as a Blackfoot occupational therapy student from Kainai (Bloodtribe). She is now a practicing occupational therapist working in a community-based return-to-work program. During the final reporting period in 2023, the third author joined the team. The third author is a nehiyaw iskwew (Cree woman) with ties to Poundmaker and Thunderchild First Nations. She works as an occupational therapist in a school-based setting and is currently doing a Doctor of Philosophy focused on addressing settler-colonialism in higher education. Compelled to confront the colonial underpinnings that are prevalent in health and educational structures, the third author has supported our efforts to recognize colonial mechanisms in our analysis and writing of this manuscript.
Participants and Recruitment
All participants were assigned pseudonyms using an online name-generator and self-identified as female. Participants graduated from occupational therapy programs between 2009 and 2022, with 10 completing their education in Canada and one in the United Kingdom. We did not set a minimum years-of-practice requirement, nor did we limit participation based on identity, known engagement in reconciliation-focused practices, or specific practice settings. This reflected our recognition that all occupational therapists share a professional responsibility to engage in reconciliation.
Ethics approval was obtained from the University of Alberta's Research Ethics Board in May 2022. Participants were recruited using convenience and snowball sampling, drawing on professional networks such as the Society of Alberta Occupational Therapists (SAOT) monthly newsletter, the Occupational Therapy and Indigenous Health Network (OTIHN) working group, and social media platforms. Eligibility for participation required that the occupational therapist interviewed be registered to practice in Alberta. In total, 17 occupational therapists inquired about participating in the study via the recruitment email address. Each person who expressed interest in study participation received a response containing further information about the study along with date and time options for the interview. If a response that indicated (dis)interest in participating was not received within 1 week, one follow-up interview with additional dates and times was sent. Non-participation in interviews was primarily due to scheduling conflicts, lack of response to initial or follow-up scheduling emails, or, in one case, an employer's directive prohibiting participation.
Before the interview date, participants were emailed a written consent form outlining information about the study in addition to possible benefits and risks of participating in the study. Before the interview commenced over Zoom, participants were given an opportunity to discuss the contents of and ask questions about the consent form. The written consent form was received by the researcher via email before the interview began. While this approach aligns with institutional research ethics requirements, it reflects Western traditions of research and consent and may not align with decolonial methodologies, which often emphasize relational accountability and oral consent.
Data Collection
The primary author conducted Zoom interviews with 11 occupational therapists between June and September 2022. Interviews were semi-structured and ranged between 40 and 75 min (mean = 52.5 min). The semi-structured approach facilitated focus on the discussion while offering breadth for participants to openly share their understandings, perspectives, and experiences of reconciliation in occupational therapy (see Smith et al., 2009). The interviews were “conversation-like,” allowing probing when important insights were revealed and modification of questions and flow based on information shared (see Chan et al., 2013; Chang, 2010).
Data Analysis
Interviews were audio recorded and transcribed. Recordings were destroyed following transcription completion, and all possible identifying details (e.g., names of places, practice settings) were removed from transcripts prior to analysis. Data were analyzed using reflexive thematic analysis, a theoretically flexible qualitative method suited to exploring deeply personal and diverse participant experiences (Braun & Clarke, 2006). The analysis was iterative and involved several stages: reviewing the transcripts, free coding, and sense-making.
Authors 1 and 2 independently conducted parallel coding and initial analyses, as each was preparing their own capstone project. Both authors met separately with Author 4 during the initial coding phase to clarify and agree on coding structures. After developing preliminary themes, Authors 1 and 2 separately triangulated their analyses with Author 4 to achieve consensus and refine the thematic structure. Following the completion of their individual capstone projects, Authors 1 and 2 worked collaboratively with Authors 3 and 4 to review both analyses, combining and revising the findings until consensus was reached on the final thematic framework. The analysis was primarily inductive, with themes developed directly from the data during coding and interpretation.
Findings
Findings are organized based on the research questions. Two themes describe “how” occupational therapists engage in reconciliation: (1) building relationships with Indigenous communities and (2) commitment to personal and collaborative learning. Two additional themes capture interrelated factors that influence engagement in reconciliation: (3) addressing systemic and practical barriers and (4) transforming occupational therapy practices.
Summary of Themes
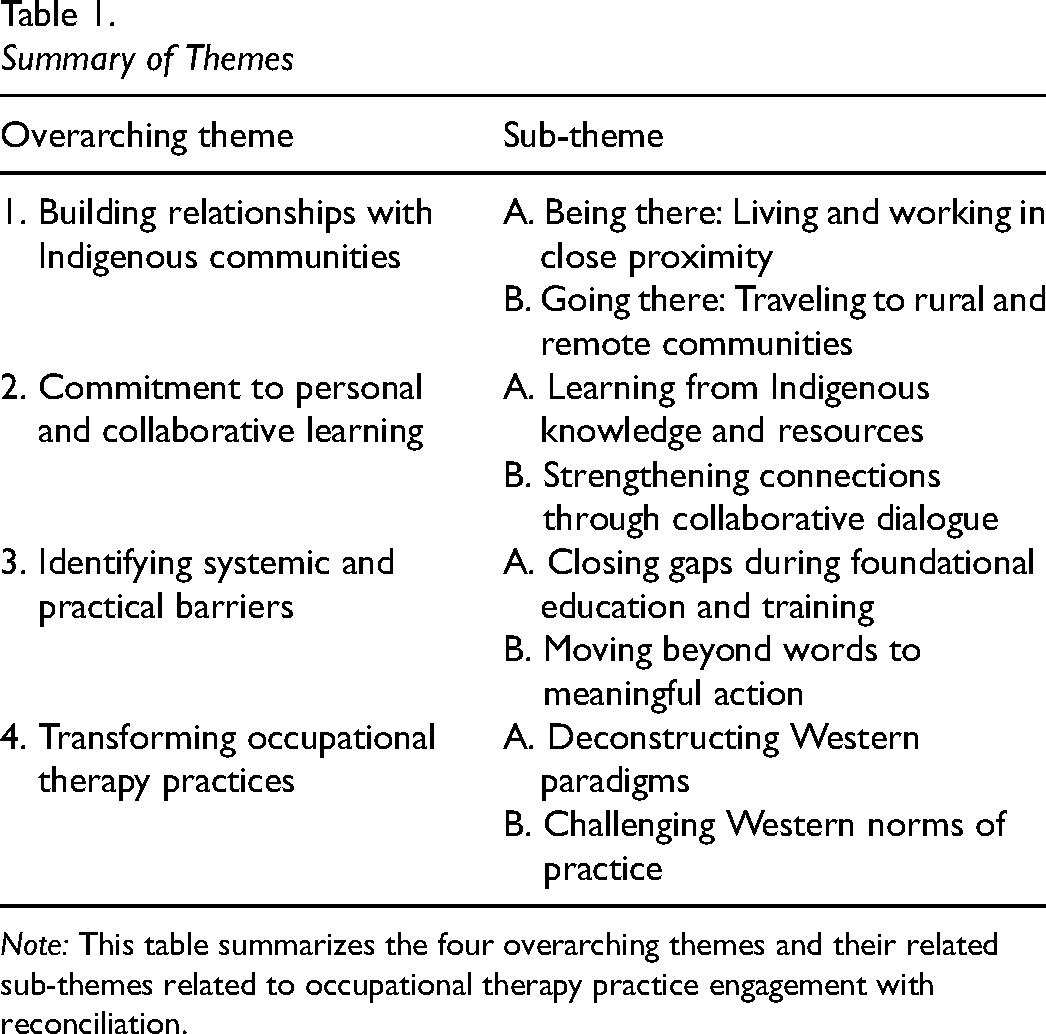
Note: This table summarizes the four overarching themes and their related sub-themes related to occupational therapy practice engagement with reconciliation.
Building Relationships with Indigenous Communities
There was a clear tension in how participants formed relationships in practice, which we describe as being there versus going there. Being there—when therapists live and work within the community—fostered stronger, more generative relationships, characterized by deeper trust, ongoing collaboration, and a sense of mutual investment. In contrast, going there—traveling into communities for periodic visits—often limited relationship-building to more surface-level or transactional interactions.
Being There: Living and Working in Close Proximity
Several participants shared experiences of working in rural and remote locations. Rural areas include countryside homes or small towns with few people and lots of open space. Remote locations are isolated or hard-to-reach areas, often lacking easy access to services and infrastructure. Some participants worked in Canada's territories before transitioning to urban areas. Urban areas are cities with many people, buildings, and services. In these rural and remote communities—typically small both in population and geographical area—close-knit relationships were described as forming more naturally, creating opportunities for deeper and more sustained connections over time. These connections were described as notably reciprocal; therapists not only got to know community members, but community members also came to know the therapists as people beyond their professional roles, learning about their families, daily routines, and personal preferences. This mutual familiarity fostered a sense of trust and accessibility.
Abbie reflected, “in the Territories, you all live together…everybody knows everybody,” emphasizing how shared spaces and close proximity blurred the lines between what the Western world defines as professional and personal life. Therapists and community members encountered each other in not only clinical or formal settings but also at grocery stores or local celebrations, where casual interactions often sparked meaningful conversations. This speaks to the visibility and informality that can make therapists more approachable and trustworthy.
Participants emphasized the value of living within rural Indigenous communities, where traditions, ceremonies, and gatherings played a central role in deepening both relational and cultural connections. Ellis highlighted that proximity facilitated more organic engagement, noting that community members often extended invitations to her on their own, rather than waiting for her to express interest or request inclusion. In turn, attending these gatherings and consistently showing up signaled to community members that she was genuinely invested in them and their community. This visibility allowed relationships to grow more naturally and reciprocally, with community members gradually opening up and initiating connections with her as well.
Similarly, Ramona recounted that her colleague found visiting an Indigenous community to be “a far more enriching experience than some of the basic conversation even with [colleagues],” underscoring how immersive, culturally grounded interactions could deepen relationships beyond surface-level exchanges. Abbie also noted accessing Elders and informal community guidance helped her navigate cultural expectations and values—supports she now misses since moving to an urban setting.
Across these accounts, participants consistently underscored the importance of community immersion—not just for their ability to engage more meaningfully, but for the ways it allowed community members to engage with them as whole people. This mutual connection, in turn, laid the foundation for more trusting and responsive therapeutic relationships.
Going There: Traveling to Rural and Remote Communities
Urban occupational therapists who travel to Indigenous communities described the travel as exhausting, with Ellis calling it “particularly arduous.” According to participants, the mentally and physically taxing schedule contributes to ongoing therapist turnover and burnout. In turn, this impacts the relationship with the community. Further, long hours of driving and limited time in community means therapists often conduct brief assessments and sessions, which hinders rapport-building and reduces the potential for meaningful follow-up or positive long-term outcomes.
Participants emphasized that face-to-face engagement with community members and stakeholders is essential to effective therapy and genuine understanding, as it signals a commitment to working in partnership with communities and to grasping the local context. Ellis reflected that without adequate time and collaboration, they feel they “are not able to really provide people with the support they need,” highlighting the limitations of fly-in, fly-out models in fostering sustainable and strength-based interventions.
Ramona stressed the importance of building deeper, immersive relationships, noting that “the history of Canada and Indigenous Peoples is put in a museum behind a piece of glass,” a metaphor that speaks to the disconnect many feel when engagement remains surface-level. While the data centered on therapists’ perspectives, their reflections point to the relational limitations of itinerant models of service delivery. The absence of community member perspectives in this study limits our ability to comment on whether this disconnect is similarly experienced by Indigenous clients—an important consideration for future research that centers community voices.
Commitment to Personal and Collaborative Learning
Several participants framed learning about Indigenous history, cultures, and perspectives not only as an opportunity but as a responsibility—particularly in the context of practicing occupational therapy in or alongside Indigenous communities. While no one explicitly stated that therapists should refrain from engagement until they have done some personal learning, participants did express that engaging with available resources and critically reflecting on one's own assumptions were essential first steps. This sense of obligation was often tied to the recognition of systemic harms, professional accountability, and the need to build more ethical, informed, and respectful relationships with Indigenous Peoples. The two sub-themes below reflect how participants approached this learning—both individually and collaboratively.
Learning from Indigenous Knowledge and Resources
Participants recognized their personal and professional obligation to engage in ongoing self-education, especially in light of the growing availability of resources focused on Indigenous histories, cultures, and perspectives. This self-directed learning was seen as foundational to their active engagement with reconciliation, as it encouraged deeper reflection on their own positions within colonial systems. Carmella, Chantelle, and Nichole described seeking out a wide range of resources—books such as Braiding Sweetgrass by Robin Wall Kimmerer or 21 Things You May Not Know About the Indian Act by Bob Joseph; films like Indian Horse; free public offerings such as the University of Alberta's “Indigenous Canada” massive online open course or Cree language classes facilitated by public spaces like the Edmonton Public Library. Carmella noted that engaging with these tools made it “easier to have conversations with friends or family about those deep, heavy issues,” illustrating how personal learning can ripple outward into broader social circles and influence community attitudes.
Importantly, participants framed this learning not as a substitute for direct relationships with Indigenous Peoples but rather a necessary first step in preparing themselves to enter such relationships with greater humility, respect, and cultural awareness. They acknowledged that self-education reduces the burden often placed on Indigenous individuals to explain their histories and experiences—a burden frequently critiqued in reconciliation discourse. As Carmella noted, the increase in publicly available media and educational content reflects a broader societal shift towards amplifying Indigenous voices and creating space for truth-telling. This increased awareness enables more collaborative and reciprocal relationships between occupational therapists and Indigenous communities. In these partnerships, occupational therapists can move beyond performative gestures to engage in shared dialogue, co-learning, and co-creation of programs and interventions that are culturally grounded and community-informed. Such practices, rooted in mutual respect and ongoing critical reflection, are essential to aligning occupational therapy with reconciliation principles and supporting Indigenous self-determination in health-care contexts.
Strengthening Connections Through Collaborative Dialogue
Participants emphasized the importance of building relationships with colleagues to advance reconciliation efforts in occupational therapy. Collaborative connections were seen as crucial for fostering understanding, challenging systemic barriers, and driving positive change. Ellis highlighted the transformative power of collegiate support, sharing that, before finding an ally, she felt isolated in efforts to change occupational therapy practices: ‘I really didn’t have an ally in changing OT practice in the NWT…I was just doing things differently on my own…once [colleague] came, we were better able to…take things together and make decisions…like, this is how we will change things’.
What made these collaborations helpful was not simply shared interest in reconciliation, but the presence of mutual accountability, openness to discomfort, and an intentional focus on reflective dialogue. Several participants described these relationships as spaces where assumptions could be gently challenged and where personal and professional blind spots were surfaced and explored. For example, Carmella credited the University of Alberta's Indigenous Focus certificate program not only for its content, but for its group-based format, which emphasized collective reflection and inquiry: “I was connected to a group that was focused on growing together and learning from each other.”
She noted that hearing others’ interpretations, questions, and uncertainties helped her re-examine her own understandings. This kind of dialogical learning—where peers posed questions, named biases, and offered alternative perspectives—was described as essential for unlearning entrenched ways of thinking. Participants valued colleagues who could name difficult truths without shaming, create space for vulnerability, and model humility in their own learning.
Through respectful and open dialogue, participants reported that, by working alongside colleagues—sharing knowledge, experiences, and perspectives—deepened their understanding of Indigenous history, culture, and contemporary issues. These conversations were most productive when marked by psychological safety, where participants felt able to ask questions and express uncertainty without fear of judgment. In these conditions, learning was not only cognitive but relational, as therapists developed greater self-awareness through connection with others.
However, not all participants had access to such supportive relationships. Nichole, for example, turned to social media to find a sense of collective learning and connection, describing it as “really powerful in terms of connecting, reaching out, and talking to see what other people are working on, what other people are struggling with and what facilitates this.”
Identifying Systemic and Practical Barriers
Participants reflected critically on the systemic and structural limitations that shape their practice, education, and efforts toward reconciliation. Rather than offering solutions, their accounts highlighted persistent barriers—such as inadequate foundational education, performative workplace initiatives, and limited access to meaningful training—that continue to hinder culturally responsive and socially just occupational therapy with Indigenous Peoples. These reflections expose areas where the profession must do better, serving as an important diagnostic step toward future change.
Closing Gaps During Foundational Education and Training
All participants reported receiving minimal education about Indigenous Peoples in their occupational therapy programs. One recent graduate mentioned some exposure through a certificate program but felt it was not enough to support meaningful personal or professional growth. Most participants recognized the value of integrating Indigenous perspectives into core curricula, describing the educational gap as contributing to limited understanding of health disparities, colonial history, and intergenerational trauma. Abbie reflected, “I don’t recall receiving any formal education about Indigenous Peoples and healthcare,” while Adrienne expressed surprise at the lack of content: “I expected there to be more…I wanted to learn more, and I wanted to do better, but I felt [the program] fell a little bit short for me.”
Beyond formal education, participants actively sought continuing education and professional development opportunities. Events such as the CAOT Annual Conference were frequently highlighted as particularly valuable. What made these experiences impactful was the opportunity for live, facilitated dialogue and the space to unpack complex ideas in community with others. Sessions were often framed around storytelling, personal experience, and relational learning, which helped foster emotional connection and a deeper understanding of lived realities. These interactive and humanizing elements stood in stark contrast to the impersonal nature of mandatory workplace training.
Several participants expressed concern about perceived ineffectiveness of required training modules, particularly those delivered through pre-recorded videos. Selena stated, “you can’t build a relationship with pre-recorded videos. People try to get through those as fast as possible anyways, so how much benefit is that?” Two other participants admitted to rushing through required Indigenous health training due to workload pressures, describing it as a box-ticking exercise rather than a meaningful learning opportunity. This disconnect revealed a tension between participants’ desire to engage more meaningfully with Indigenous knowledges and the rigid, compliance-oriented nature of many mandated trainings. The absence of interaction, critical dialogue, and emotional connection in these formats diminished their perceived relevance and impact.
Participants’ reflections point to several features that made training useful: facilitation by Indigenous leaders, opportunities for real-time dialogue and reflection, emotional and relational engagement, and the freedom to move beyond surface-level content. These characteristics created more personally resonant and ethically grounded learning experiences—ones that aligned with participants’ values and commitments to reconciliation.
Moving Beyond Words to Meaningful Action
Participants emphasized that reconciliation is not a static goal but a continuous process requiring honest dialogue, verbal commitment, and, most importantly, concrete actions to address historical injustices and rebuild relationships with Indigenous Peoples. Regan voiced concerns that discussions about reconciliation often remain superficial and fail to translate into meaningful change. Similarly, Abbie reflected on the frustration of performative engagement: ‘it's easy to say we should do this and take action…it's better now, but…a lot of times it was just complaining about how it felt. Like, it was just talking about how terrible things are…it felt like we weren’t doing anything about it. We were just reading and talking’.
Desiree was critical of Canadian occupational therapy programs for inadequately enacting change, particularly highlighting the absence of Indigenous professors. She stressed that while events such as recent discoveries of unmarked graves have spared public outcry, these truths were never hidden from Indigenous communities—what was missing was the willingness of settlers to listen and act. She expressed frustration that Indigenous knowledge and experiences have long been dismissed, reinforcing the gap between awareness and action.
Chantelle acknowledged having access to valuable learning materials such as 21 Things You May Not Know About the Indian Act, but described feeling overwhelmed by the breadth of information and unsure of where to begin. She shared feelings of guilt for past harms and a sense of imposter syndrome, admitting that engaging with these materials made her feel like a “fraud.” Her experience reflects a broader emotional complexity with engaging in reconciliation, especially for non-Indigenous therapists who may grapple with shame, discomfort, or fear of “getting it wrong.”
Nora, an Indigenous occupational therapist, pointed to the structural barriers to professional development, particularly the high costs of accessing advanced training in areas like trauma-informed care. Although free resources exist, she noted they often lack depth or specificity. Her experience underscored the broader challenge faced by many therapists: the limited availability of accessible, high-quality training needed to develop truly culturally responsive practices.
Workplace efforts were also criticized for their superficiality. Ellis described reconciliation initiatives in some organizations as tokenistic, highlighting performative gestures such as hanging multilingual signs: “We’re making it culturally relevant by, like, putting signs up in different languages’…really, that's where you’re going with this? It's much more broken than putting up a sign.” Nichole echoed this concern, warning that when reconciliation becomes reduced to surface-level actions, it risks being co-opted and stripped of its connections to justice, accountability, and Indigenous sovereignty.
Across all participants, there was a shared recognition that reconciliation must involve sustained, long-term effort—far beyond symbolic gestures or one-time events. It requires ongoing learning, self-reflection, relationship-building, and a willingness to confront discomfort and make mistakes. Ultimately, participants called for a shift from passive acknowledgement to active responsibility, where occupational therapists engage in reconciliation not as a checklist item but as an ethical and relational commitment embedded in everyday practice.
Transforming Occupational Therapy Practices
Deconstructing Western Paradigms
All participants acknowledged that the occupational therapy profession is rooted in Western cultures and traditions shaped by colonization, assimilation, and systemic oppression. Its normative focus—defining health and function through Western standards—has both excluded and pathologized Indigenous Peoples’ perspectives and worldviews. Nora highlighted how the profession's origins shape the profession's philosophies, tools, approaches, and research, fostering mistrust and reducing Indigenous Peoples’ willingness to engage in services.
Abbie described a disconnect between existing systems and Indigenous Peoples, identifying “two different worlds.” Ellis saw this gap as the catalyst for transitioning from public to private practice, noting public therapists’ limitations in meeting community needs. Her private work focuses on seeking guidance from Indigenous advisors and governments, emphasizing that Indigenous Peoples should have greater say in or power over the services they are provided. ‘I noticed a gap. The government therapists were doing their best but couldn’t serve people the way they needed to be…I wanted to fill some gaps in a private sense. Initially, I always thought, like, why would you go private and make people pay for you? But actually, it's serving people better…[my work] is very centred on seeking direction from Indigenous advisors and Indigenous governments because that's who employs me. I’m going to do what they want because they deserve it’.
Ellis explained that working outside government policies, procedures, and expectations allows for more culturally appropriate practices. For instance, standardized assessments such as the Kettle Test, often fail with Indigenous Elders unfamiliar with items like electric kettles due to their upbringing. Realizing their inappropriateness, Ellis abandoned such assessments in private practice, choosing methods better suited to the cultural context of her clients. ‘A lot of the time we’d be asked to do cognitive assessments, or even any assessment at all, right. And the use of standardized assessments with Indigenous Peoples…all these things just make [the tests]…for example…it uses an electric kettle. These Elders grew up in the bush. Of course they’re gonna do shitty on a Kettle Test. I learned pretty quick…it was not appropriate. Even though I was told this is how you do it…I really don’t use them at all in my private practice’.
Ramona also questioned the reliance on assessments and productivity in occupational therapy, arguing that it can detract from what truly matters—connection. She emphasized focusing on meaningful relationships rather than rigid measures: ‘I would like to get rid of the whole notion that you need to do activities to be useful, that you need to do assessments to be productive. That whole notion of productivity, I feel, really, at times, takes away from the core of what's actually really important’.
Similarly, Nora shared that her approach involves “following [her] heart,” cultural teachings, and guidance from Elders, prioritizing connection over traditional goal-oriented therapy. “What I know is true and what I’ve been taught, what I’ve discussed with family members and Elders from my community [and] in the community I’m in now.” This contrasts with conventional occupational therapy, which emphasizes treatment tied to clear objectives.
Challenging Western Norms of Practice
Traditional occupational therapy methods are often grounded in Western biomedical frameworks that may not align with Indigenous Peoples’ worldviews, healing practices, or relational ways of being. Participants described how institutional norms and time constraints limit their ability to practice in culturally responsive ways. Ellis, for example, reflected on the constraints of brief visits and task-oriented sessions, which she described as superficial “in and out” treatments. Similarly, Abbie recounted referrals that prioritized functional concerns over relational or emotional needs ‘I'll get a referral for a raised toilet seat or something. And then, I'm in a bathroom with someone who's talking about all the abuse they've been through…we sit in the bathroom for two hours talking about their trauma and decide we don't need a raised toilet seat’.
These experiences highlight the disconnect between standardized occupational therapy goals and the lived realities of Indigenous Peoples, particularly when deeper issues—like trauma or social context—are not accounted for in the referral or session design.
Some participants described intentionally resisting institutional norms to meet clients’ needs more meaningfully. Regan, for instance, spoke about deliberately choosing not to follow her health authority's “three-strike rule” (a policy that discontinues services after three missed appointments), recognizing that structural barriers like housing instability, transportation, or trauma often underlie missed sessions. For her, flexibility and compassion were more ethical and culturally aligned approaches.
Rather than framing their actions as explicitly “Indigenous” approaches, participants described them as forms of resistance to rigid, standardized models—making space for more human-centered, relational, and context-aware care. These early efforts to challenge dominant Western norms responded not only to the specific needs of Indigenous communities but also suggest broader possibilities for making care more flexible, relational, and less oppressive for all clients.
Discussion
This study provides valuable insights into the ways occupational therapists in Alberta engage with reconciliation in their practice, with a central theme emerging around the significance of relationship-building within Indigenous communities. Participants emphasized that meaningful partnerships extend beyond formal or goal-oriented engagements and include the development of authentic relationships grounded in genuine friendship, love, and community connection. These relationships are often cultivated through everyday actions without specific professional objectives in mind. This perspective challenges dominant Western norms of “professionalism” and rigid professional boundaries, which typically frame relationship-building as a means to an end—such as increasing cultural awareness or fulfilling professional responsibilities. Instead, participants highlighted the importance of approaching relational work with humility, openness, and a long-term commitment to mutual respect and care. When guided by principles of respect, reciprocity, and Indigenous sovereignty, such relationships can support culturally responsive practice and uphold the self-determination of Indigenous Peoples in health-care (Bauer et al., 2022; Gibson et al., 2015).
Having Indigenous practitioners from within the community itself may be an effective means of supporting the autonomy and self-determination of both individuals and the broader community. The presence of practitioners from within the community creates opportunities for deeper connections and a better understanding of local traditions, cultural practices, and the nuances of community relationships (Wylie et al., 2021). Participants in this study reinforced this sentiment, acknowledging that Indigenous practitioners from the community would bring invaluable insights that foster trust and ensure culturally appropriate care. Specifically, Desiree, a non-Indigenous occupational therapist working in an Indigenous community, remarked that she would “graciously” relinquish her role to an Indigenous occupational therapist. Pride's (2023) doctoral research also supports Indigenous practitioners, identifying that sovereign occupational therapy services may be most appropriately created by Indigenous occupational therapists for Indigenous occupational therapists, for the betterment of all Indigenous Peoples. However, Indigenous people are currently underrepresented in the occupational therapy profession, and the only pathway to increasing representation is for Indigenous students to endure and contort themselves to colonial higher education. Additionally, Pride (2023) identified that while numbers of Indigenous students are increasing, very limited efforts have been made to support the retention of Indigenous health-care professionals, as called for by the TRC. Indigenous occupational therapists on Turtle Island that have gone through this process have described their educational experience to be wrapped up in “imposed isolation, lack of support, exclusion, a devaluing of their merit and skills, and the need to navigate between two worldviews” (Pride et al., 2025, p. 18). Therefore, simply increasing the enrollment of Indigenous students in current occupational therapy programs would be ill-advised without simultaneously undertaking a critical overhaul of these programs to incorporate Indigenous voices and uphold Indigenous sovereignty in occupational therapy education (Pride, 2023).
Participants described reconciliation in occupational therapy as requiring not only relationship-building and critical reflection, but also deliberate acts of resistance. Acts of resistance disrupt colonial norms that continue to marginalize Indigenous Peoples and, in doing so, can serve as meaningful practices of reconciliation (Turcotte & Holmes, 2021). These may take shape through refusing deficit-based language in documentation (MacLachlan & Grenier, 2022), adopting collective models of care such as Pirate Care (Graziano et al., 2025), or challenging professional conventions through everyday forms of disobedience. Far from being symbolic, such strategies actively contest harmful norms and affirm Indigenous sovereignty in health-care.
Participants highlighted that occupational therapy training is a critical time to introduce discussions on Indigenous perspectives and reconciliation. However, only one participant recalled receiving any education, and it was minimal. This aligns with Moon et al. (2018) findings about the University of Alberta's Department of Occupational Therapy, which recognized their reconciliation efforts “had only just begun” (p. 28). Desiree pointed out the absence of Indigenous faculty, an issue faced across Canadian occupational therapy programs. While faculty representation is vital, it must be part of broader efforts to avoid tokenism and alleviate the burden on Indigenous peoples (see Gaudry & Lorenz, 2018). Including Indigenous faculty is especially significant in the context of reconciliation, as they bring lived experience, cultural knowledge, and perspectives that are often missing from Euro-Western curricula. Importantly, increasing Indigenous faculty should include permanent positions and opportunities to teach across the curriculum—not only on “Indigenous-related topics”—to challenge Western norms in areas such as assessment practices, documentation, and clinical reasoning. Their presence supports the creation of culturally safer learning environments, challenges dominant narratives, and contributes to building relationships rooted in respect and reciprocity—central goals of reconciliation. While not every marginalized group is represented among faculty, the TRC has specifically called for action in education and health disciplines, highlighting the unique and urgent need to address historical and ongoing harms affecting Indigenous communities in Canada.
The TRC emphasizes that post-secondary programs must provide education that not only acknowledges the negative effects of colonization but also incorporates Indigenous self-determination and perspectives in practice. Reconciliation requires concrete actions to address these impacts, moving beyond dialogue to implement policies and practices that promote equity and autonomy for Indigenous Peoples. Grenier et al. (2020) suggest a pedagogical shift that not only focuses on developing students’ cognitive skills but invites students into reflective processes around structural inequality and culturally safer approaches that prioritize relationship and partnership.
Gaudry and Lorenz (2018) offer a spectrum of steps to be taken by the academy to be more inclusive for Indigenous peoples—steps that are critical for most if not all programs, including health profession programs. Along the spectrum offered by Gaudry and Lorenz (2018), there are three markers: Indigenous inclusion, reconciliation Indigenization, and decolonial Indigenization. Indigenous inclusion is when the university seeks to increase numbers of Indigenous students, faculty, and staff, without changing the oppressive structures of the institution itself. Reconciliation Indigenization includes genuine inclusion of Indigenous ways of being and doing for students, faculty, and staff, and led by Indigenous peoples for Indigenous peoples. Lastly, decolonial Indigenization includes the re-envisioning the academy, starting with Indigenous ways of being and knowing as the central guide point, upholding and reorienting the academy to affirm Indigenous self-determination and sovereignty.
Pride et al. (2025) note that Canadian occupational therapy education programs are primarily positioned within “Indigenous inclusion,” where curriculum content and pedagogical approach may remain inappropriate and exclusionary for Indigenous students. For example, Pride et al. (2025) highlight that Indigenous occupational therapy students often question their place within the program and describe the burden of educating both peers and faculty about Indigenous health. They also report the pressure to “stick through” the experience by conforming to pedagogical approaches that do not align with their own ways of knowing. The third author of this paper has experienced similar tensions in practice as an occupational therapist, noting a disconnect between how they strive to practice and the expectations shaped by their educational training, alongside constraints imposed by regulatory body requirements. Furthermore, Pride et al. (2025) note that the process of re-envisioning the education experience is just as important as the shift in content and that Indigenous occupational therapists can lead this. Ahmed-Landeryou (2023) echoes this, noting that to make changes to the current climate of the occupational therapy profession and education, consultation with Indigenous students and practitioners is necessary, as well as continually and regularly re-evaluating the process. These recommendations align with the CAOT TRC Task Force's emphasized importance of full and direct involvement of Indigenous Peoples in discussions and decisions affecting them, albeit the report was completed in 2023 (CAOT, 2023a). We ask, then: when will the formalized accreditation bodies that oversee Canadian occupational therapy programs begin to bear the repercussions of limited Indigenous representation—rather than continuing to place that burden solely on Indigenous students navigating these systems?
Although participants spoke to the ethical responsibilities of individual practitioners, there is a risk that reconciliation in occupational therapy becomes framed solely as a matter of personal commitment rather than a systemic obligation. At present, most reconciliation efforts rely on voluntary engagement, with limited institutional mechanisms to ensure accountability. Without enforceable requirements, both programs and practitioners can disengage from reconciliation without consequence. Stronger policies and accreditation standards are therefore needed to embed concrete expectations, particularly within occupational therapy program accreditation bodies and professional licensing boards. Without such measures, reconciliation risks remaining symbolic.
Just as educational structures need to engage in an ongoing process of learning and unlearning, participants in our study described pursuing reconciliation in occupational therapy practice as an ongoing process of learning and unlearning. This echoes calls from within the profession for practitioners to engage in ongoing critical reflexivity (Farias & Rudman, 2019). Occupational therapist and researcher Janna MacLachlan emphasizes this process of self-reflection: ‘the more I listen to Indigenous voices, learn about Indigenous worldviews, and reflect on my practice, the more I recognize how much I am implicated in systems and practices that do just that. I discovered I didn’t know how much I didn’t know, and I still don’t. I was so grounded in the Western worldview being the taken-for-granted norm that I had no idea how many assumptions I had been making or what other ways of knowing and being there might be’ (Boivin & MacLachlan, 2019, p. 12).
While practitioners aim to avoid mistakes, Viengkone (2019) advises making the most of them. She recounts a situation where she asked an Indigenous colleague to speak at an event, unknowingly placing them in the position of a Knowledge Keeper, which led to discomfort. Viengkone reflected on the mistake, recognizing the need for further learning to avoid repeating it. This approach aligns with the broader understanding that reconciliation and cultural competency require continual learning and self-reflection, acknowledging that mistakes are part of growth in this journey.
Challenging established colonial ways of thinking and acting in health-care requires considerable effort, dedication, and action. As outlined in the TRC s Calls to Action, health-care professionals, due to our positions of privilege, have the responsibility to acknowledge systemic harms and take action. In the long term, we advocate for Indigenous sovereign health services across the country, such as the First Nations Health Authority in British Columbia or the Cree Board of Health and Social Services of James Bay in Québec, whereby health and wellness services are Indigenous-led (Halseth & Murdock, 2020). As an initial step that increases collaboration and in-community support, and moves towards Indigenous sovereignty, could include prioritizing and advocating for community-located occupational therapy assistant roles to carry out more hands-on intervention. Community occupational therapy assistants could be supported by an occupational therapist who may not be present in the community, ideally an Indigenous therapist. Advocating for and supporting occupational therapist assistant roles in First Nations, Metis, and Inuit communities was noted within the CAOT position statement (2018) regarding occupational therapy and Indigenous peoples, referencing Call to Action #23. Further, in order to affirm the self-determination of Indigenous communities, occupational therapy assistants could be employed by Indigenous-governed institutions (e.g., the band, an on-reserve school) funded by Indigenous Services Canada. Until there are Indigenous occupational therapists in the community, supervision agreements could be made with local health authorities, rather than having assistants employed by colonial systems. Still, supervising occupational therapists remain in a position of power and must reflexively offer guidance and education that affirms the leadership and community-based knowledge of occupational therapy assistants. Without this, we would reify existing colonial hierarchies.
Methodological Considerations & Limitations
The participants for this project were all located in one Canadian province—Alberta—and do not necessarily reflect the experiences of all occupational therapists in Canada. While this may be seen as a limitation, it also offers a strength: participants shared experiences within a shared provincial health-care system, shaped by Alberta-specific policies, histories, and structures. Moreover, this local focus is both necessary and appropriate, as reconciliation efforts must be grounded in the unique histories, Nations, treaties, and contexts of specific regions. Attempting to define a single, uniform approach to reconciliation risks re-inscribing colonial thinking by imposing “one right way” across diverse Indigenous communities and provincial contexts.
Understanding the local practice landscape is, therefore, critical to interpreting the participants’ insights. Alberta's occupational therapy practice is largely situated within a publicly funded health system—Alberta Health Services—which oversees most clinical care across the province. In community-based settings, clinicians may also work for First Nations—governed health organizations, non-profits, or private practices, contributing to a complex and often fragmented system of care. The history of occupational therapy in Alberta is intertwined with broader settler-colonial health systems, where care has typically been shaped by Western biomedical models and inconsistent efforts toward cultural safety. Alberta sits on the territories of Treaty 6, 7, and 8 First Nations, and is home to the Métis Nation of Alberta, which includes six regional areas and eight Métis Settlements. There is also a growing Inuit population living in urban centers across the province. Despite this diverse Indigenous presence, participants noted ongoing systemic barriers to accessing equitable and culturally safer care—including underfunding, jurisdictional ambiguities between federal and provincial services, and a lack of sustained institutional commitment to reconciliation. Against this backdrop, participants shared diverse experiences spanning acute care to community roles, offering rich insights into the challenges and possibilities for reconciliation in occupational therapy. Their reflections invite all occupational therapists to consider how place, policy, and power influence their practice and relationships with Indigenous communities.
Conclusion
Reconciliation in occupational therapy is not merely an aspirational goal but a necessary commitment to addressing colonial harms and advancing justice for Indigenous Peoples. This study underscores the centrality of building genuine relationships with Indigenous communities and engaging in lifelong learning as foundational steps toward reconciliation. Participants highlighted the critical need to deconstruct Western paradigms and integrate culturally responsive, non-Western approaches into occupational therapy practices. However, systemic barriers such as insufficient education, superficial workplace actions, and the gap between rhetoric and meaningful change continue to hinder progress.
Occupational therapists must embrace reconciliation as a dynamic and ongoing process, demanding self-reflection, humility, commitment, and action to challenge entrenched colonial structures. There is a pressing need to address the perceived inferiority of Indigenous knowledge and consider whether current actions are advancing or disrupting coloniality (Ramugondo, 2018). To achieve transformative change, the profession must prioritize culturally safer practices, amplify Indigenous voices, and embed Indigenous ways of knowing into every facet of care, from education and policy to research and practice. Reconciliation requires action—not symbolism—a collective effort that moves beyond token gestures to foster equity, healing, and mutual respect.
By reframing occupational therapy through a lens of reconciliation, the profession can contribute to the broader movement for Indigenous sovereignty and justice, ensuring that its practices honor the diversity, strength, and resilience of Indigenous Peoples. Meaningful action is not only possible but imperative for a future rooted in equity and collaboration, and reoriented practices that affirm and uphold Indigenous sovereignty.
Key Messages
Building respectful, long-term relationships with Indigenous communities is essential for reconciliation in occupational therapy, but must not rely on Indigenous Peoples to provide education or emotional labor.
Systemic barriers such as underfunding, fragmented services, and policy constraints limit occupational therapists’ ability to deliver culturally safe and community-driven care in Alberta.
Occupational therapy education, as well as the profession's governing structures, regulatory and licensing bodies, and accreditation bodies, must undergo structural transformation to move beyond token inclusion, embracing decolonial approaches that center Indigenous knowledge, leadership, and self-determination.
Footnotes
Acknowledgements
The authors thank Kaarina Valavaara, who played a guiding force in the development of this study. Kaarina is a leader who has made significant contributions to the occupational therapy profession through her work in response to disparities faced by Indigenous Peoples in healthcare.
Funding
The first author received funding from the Social Sciences and Humanities Research Council of Canada (SSHRC) Canada Graduate Scholarship—Master's (CGS-M) award. The first author was also supported by the University of Alberta's Faculty of Graduate Studies and Research (FGSR) Mary Louise Imrie Graduate Student Award and the University of Alberta's Graduate Students’ Association Travel Grant.