
Abstract
Introduction
Migration is one of the most important drivers of change and transformation in the post-modern world (Ozkazanc-Pan, 2019), with 3.6% of the world's population, that is, 281 million people, comprising international immigrants (McAuliffe, 2021). They migrate as individuals or with their families to a new host country (McAuliffe, 2021).
Immigrant families are often socially positioned as the “other” by their host community (Udah & Singh, 2019). This phenomenon of “othering” has been defined as the process by which the dominant group maintains control by disregarding certain identities and creating new ones (El-Lahib, 2016). In the case of immigrants, othering leads to group-based inequality and marginalization of those who are racially, culturally, and linguistically different from the host community, essentially creating an imbalance in their social positioning (Powell & Menendian, 2016). This feeling of being the “other” is further enhanced by their own social-cultural perceptions and experiences of being different to their host community (Udah & Singh, 2019). These challenges are compounded when disability intersects with ethnicity and other causes of marginalization (El-Lahib, 2016), as in the case of immigrant families with disabled children (Nicholas et al., 2017). The limitations and the restrictions imposed by the attitudinal, environmental, and institutional barriers on disabled children while they interact with the world around them, impact and influence their entire family unit (Reichman et al., 2008).
Occupational therapists work with children and their families from diverse cultural backgrounds to support performance, engagement, and participation in their valued occupations in their physical and social contexts (Restall & Egan, 2022). Building and sustaining the therapeutic relationship is central to initiating, facilitating, and maximizing occupational participation (American Occupational Therapy Association, 2020; Restall & Egan, 2022). Establishing the therapeutic relationship between the occupational therapist and the immigrant families of disabled children requires an understanding of what each brings into the interaction (Grandpierre et al., 2018; Iwama et al., 2009). Immigrant families bring into the therapeutic relationship the cultural ties and bonds they grew up with (Hon et al., 2011), along with the new agreed upon and at times imposed set of values and principles they take on from their new host society (Grandpierre et al., 2018). Culture is a set of implicit and explicit guidelines that individuals inherit being members of a particular society which influences how they view, experience, and behave in the world (Helman, 2007). For immigrant families, their definition of culture is their way of expressing shared ideas and concepts influenced by their original society and often challenged and redefined by the new culture (Grandpierre et al., 2018). Occupational therapists bring their own experiences, values, and perspectives into the relationship (Iwama et al., 2009).
It is therefore essential to acknowledge the lived experiences, roles, perceived social positioning, familial roles, routines, and perceptions of health and disability and cultural influences of the immigrant families and the occupational therapists in the relationship (Grandpierre et al., 2018; Iwama et al., 2009; Turpin et al., 2011). Cultural approaches are adopted to acknowledge these diversities of contexts, envision change and enable application while facilitating the therapeutic relationship (Beagan, 2015). Some cultural approaches predominately used in occupational therapy with immigrant families include cultural competence, cultural sensitivity, cultural relevance (Agner, 2020; Beagan, 2015; Grandpierre et al., 2018), and cultural humility (Agner, 2020; Beagan, 2015). These approaches are defined in Table 1. Although, literature reveals the purpose and the use of cultural approaches with culturally diverse populations in occupational therapy (Beagan, 2015), a better understanding is needed of how these cultural approaches are used to build and sustain the therapeutic relationship with immigrant families of disabled children. Understanding how these approaches are currently applied when working with immigrant families of disabled children can help critically evaluate the power relations in the therapeutic relationship. This is essential in formulating professional processes and frameworks that embrace the decolonial and anti-oppressive ways in this diverse cultural society (Beagan et al., 2023; Grenier, 2020; Murphy et al., 2024; Ramugondo, 2018). Therefore, the objective of this scoping review was (1) to determine whether cultural approaches are used to build the therapeutic relationship between immigrant families of disabled children and their occupational therapists, and (2) to determine how the cultural approaches build and sustain the therapeutic relationship between the immigrant families of disabled children and their occupational therapists.
Understanding the Cultural Approaches Used in Occupational Therapy.
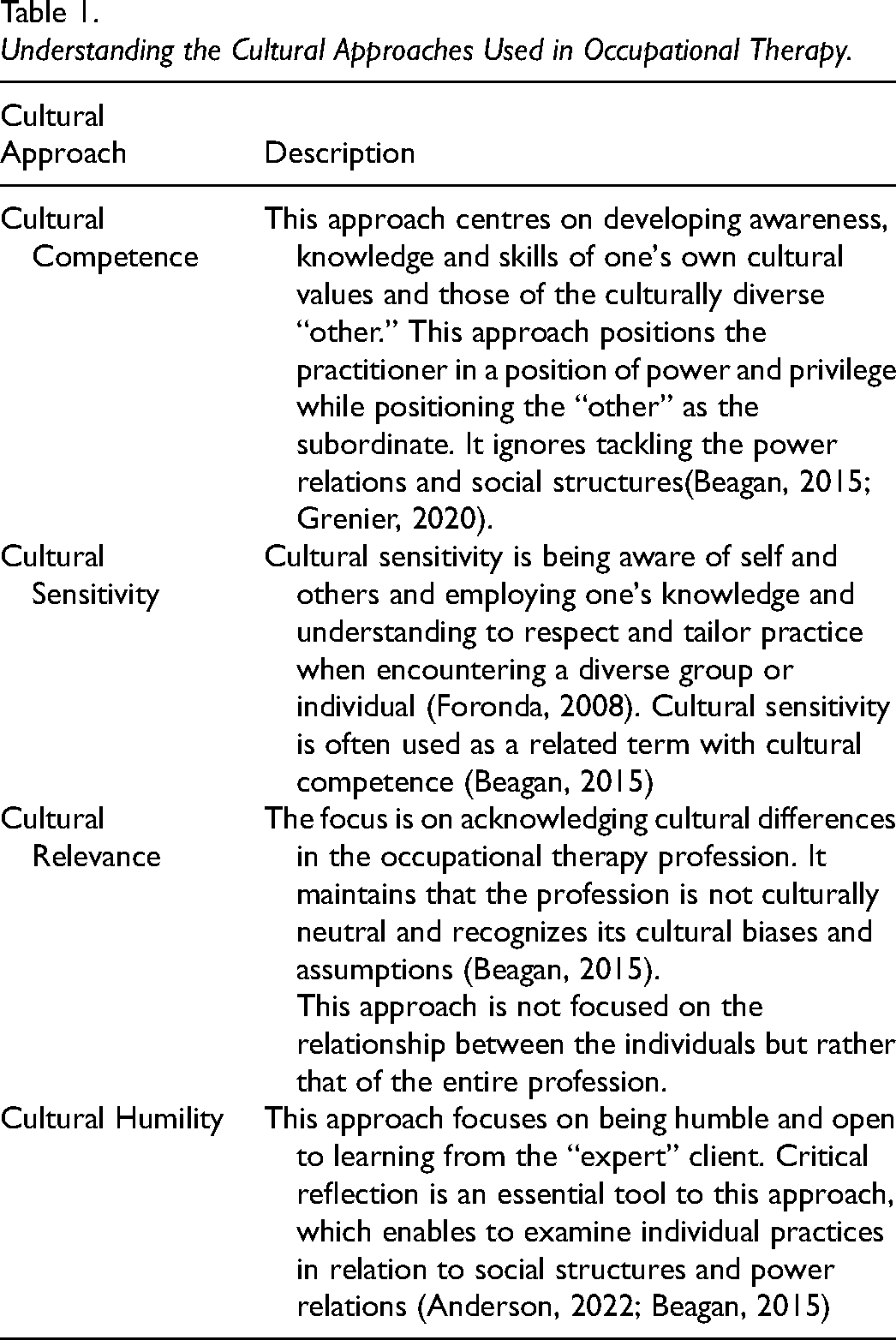
Beagan's (2015) critical synthesis of occupational therapy literature on the subject has been used to outline the scope of this review. Beagan (2015) synthesizes the purpose and the use of four cultural approaches: cultural competence, cultural relevance, cultural safety, and cultural humility, in occupational therapy, with culturally diverse populations. Since there are many ways to view and interpret culture and diversity, Beagan's (2015) critical synthesis provides a guide to initiate discourse specific to establishing therapeutic relationship with immigrant families of disabled children and occupational therapy, where there is a significant void. Identity-first language: immigrant families of disabled children have intentionally been used to identify the child’s disability as a natural circumstance which forms an accepted part of their identity (Ferrigon & Tucker, 2019).
Methods
This review has been analyzed and written through the lens of an immigrant occupational therapist from the Global South, which positions the first author as the “other” in the professional and socio-political context. The first author acknowledged this position, maintaining a reflexive approach through ongoing reflection and discussion with the co-authors, one of whom also migrated from the Global South.
A preliminary search of PubMed Central, the Cochrane Database of Systematic Reviews, JBI Evidence Synthesis, and Open Science Framework registries was conducted in January 2022. No current or underway systematic or scoping reviews on the topic were identified. The study protocol was registered with the OSF Registries on March 31, 2022. https://doi.org/10.17605/OSF.IO/AXF2R.
The Joanna Brigg's Institute methodology (Peters et al., 2020) for scoping reviews was used to conduct this review, which is based on the 5-step methodological framework developed by Arksey and O'Malley (2005).
(1) Defining the Research Question/s
The research question for this scoping review was “How are cultural approaches used to establish and sustain the therapeutic relationship between immigrant families of disabled children and their occupational therapists?”
(2) Identifying Relevant Studies
The search terms used to scope the literature included “immigrants,” “disabled children,” and “occupational therapy.” These terms yielded articles that satisfied the inclusion criteria. Terms included in these articles were used to refine the search terms, which included “cultural sensitivity,” “cultural awareness,” “cultural competence,” “cultural humility,” and “cultural relevance.” Multiple search strings were used to broaden the scope of the area and increase the possibility of identifying literature (Appendix 1). The first author searched health and social sciences databases freely available in the university library system, between March and May 2022, updated in April 2024 and February 2025. The databases included PubMed Central, Medline, CINAHL, Web of Science, Scopus, and PsychInfo, as these offered a broad coverage of articles in the health and social sciences.
(3) Study Selection
The inclusion criteria were refined after the preliminary searches (Table 2). Constraints of time and resources led to restricting the search to articles published in English and peer-reviewed journals.
(4) Charting the Data
Inclusion and Exclusion Criteria.
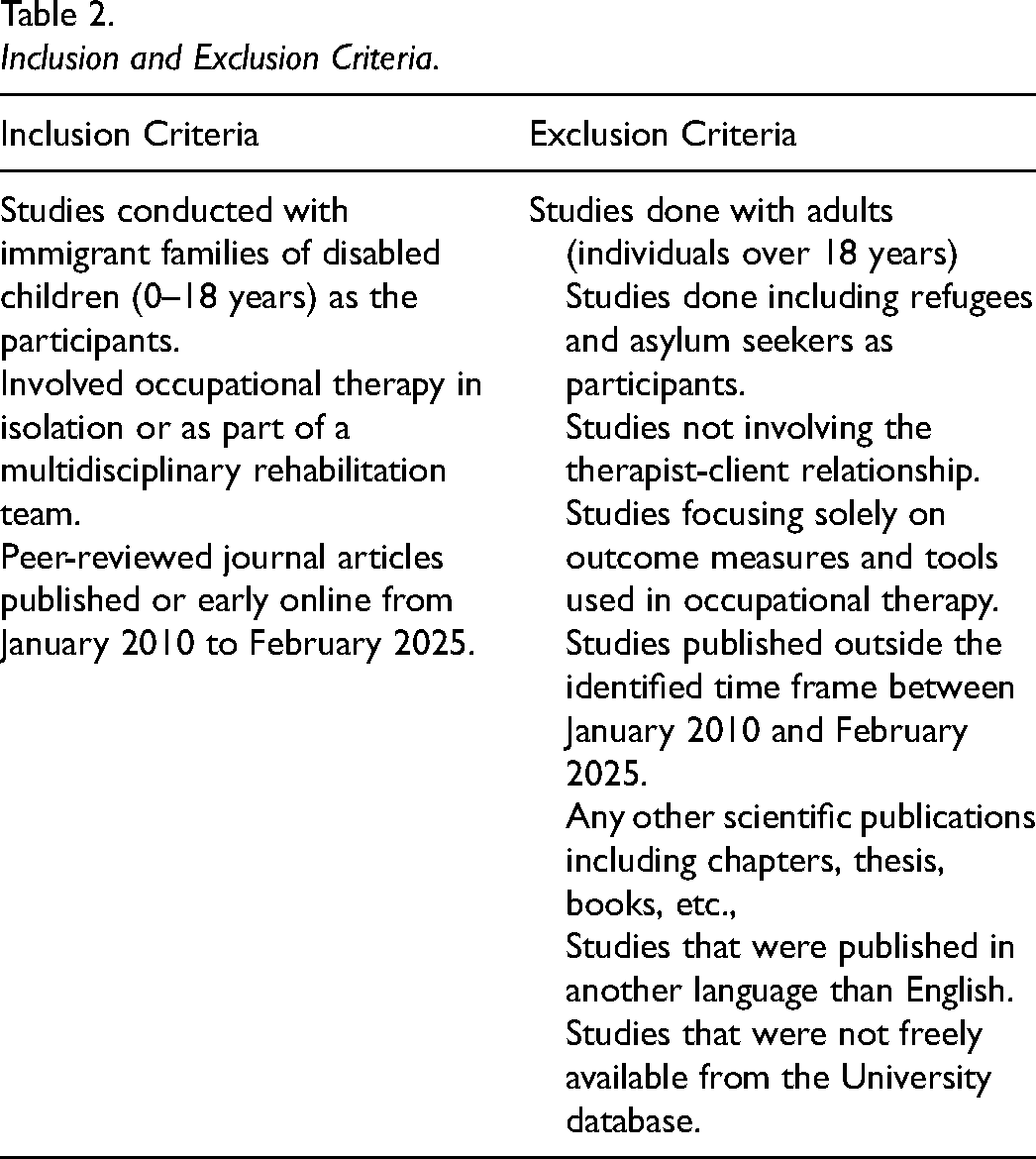
Following the search, all identified citations were uploaded into Covidence (Veritas Health Innovation, Melbourne Australia, 2019) by the first author. Titles and abstracts were screened against eligibility criteria by the first author. The first author and the fourth co-author reviewed and screened full texts against the eligibility criteria (Table 2). The reasons for full-text exclusions were documented in Covidence (Veritas Health Innovation, Melbourne Australia, 2019) and reported within the scoping review. Disagreements during the screening and selection process were resolved by consensus between the first author and the fourth co-author through deliberation.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed using the PRISMA extension for scoping reviews (PRISMA-ScR) checklist (Peters et al., 2020). The PRISMA Flow diagram depicting the different phases of the review is attached (Figure 1).
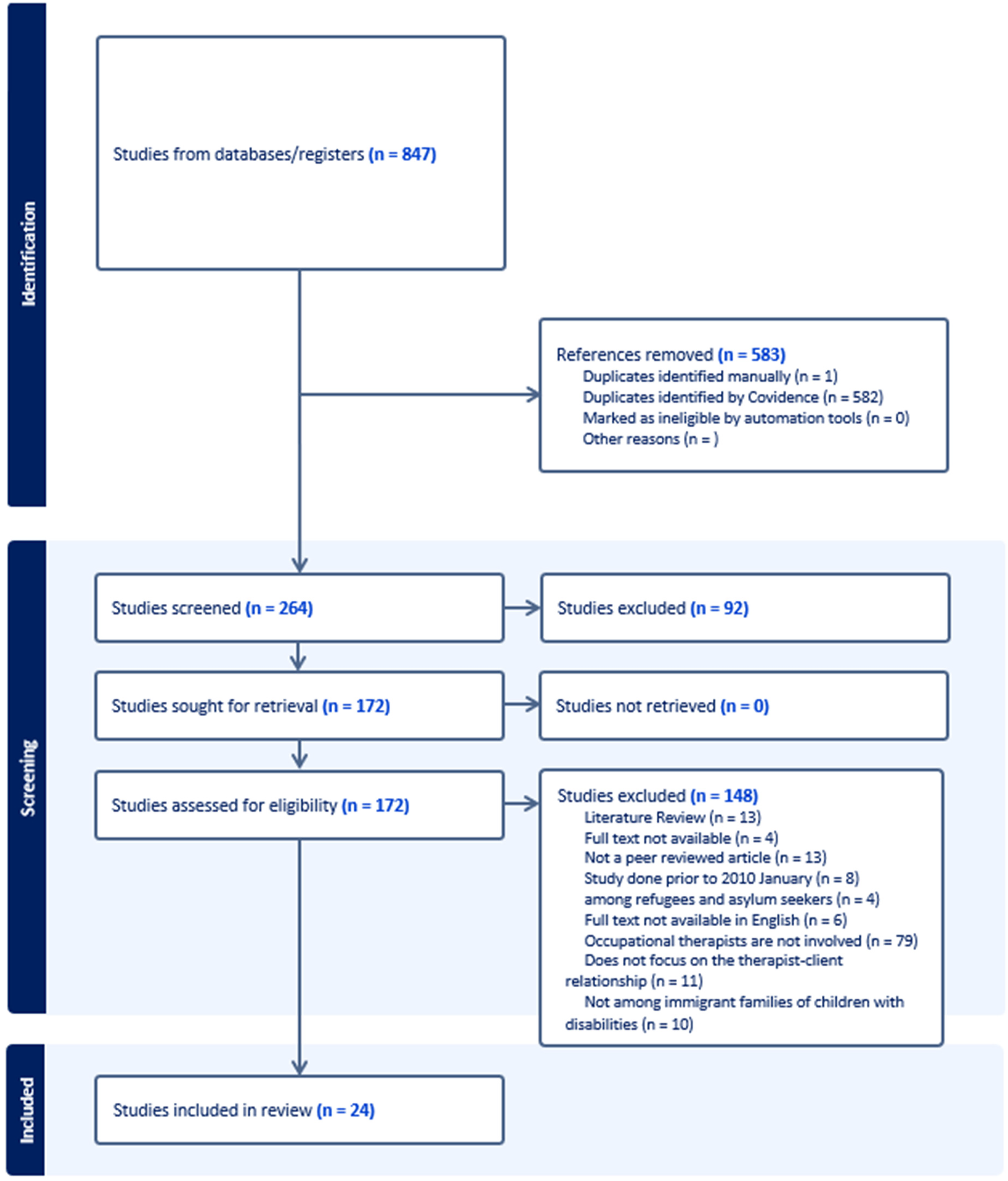
PRISMA flow diagram.
The data extraction form (Appendix 2) was used to chart the data obtained from the included studies.
(5) Collating, Summarizing, and Reporting the Results
The charted data was collated in ExcelTM and the common characteristics were summarized. The data was analyzed using deductive and inductive analysis to generate the results (Azungah, 2018). All the research team members deliberated and refined the results.
Results
Descriptive Analysis
Table 3 presents the focus and the variations observed across the 24 articles which met the inclusion criteria. The table has been chronologically organized according to the year of their publication.
Description of Included Studies.
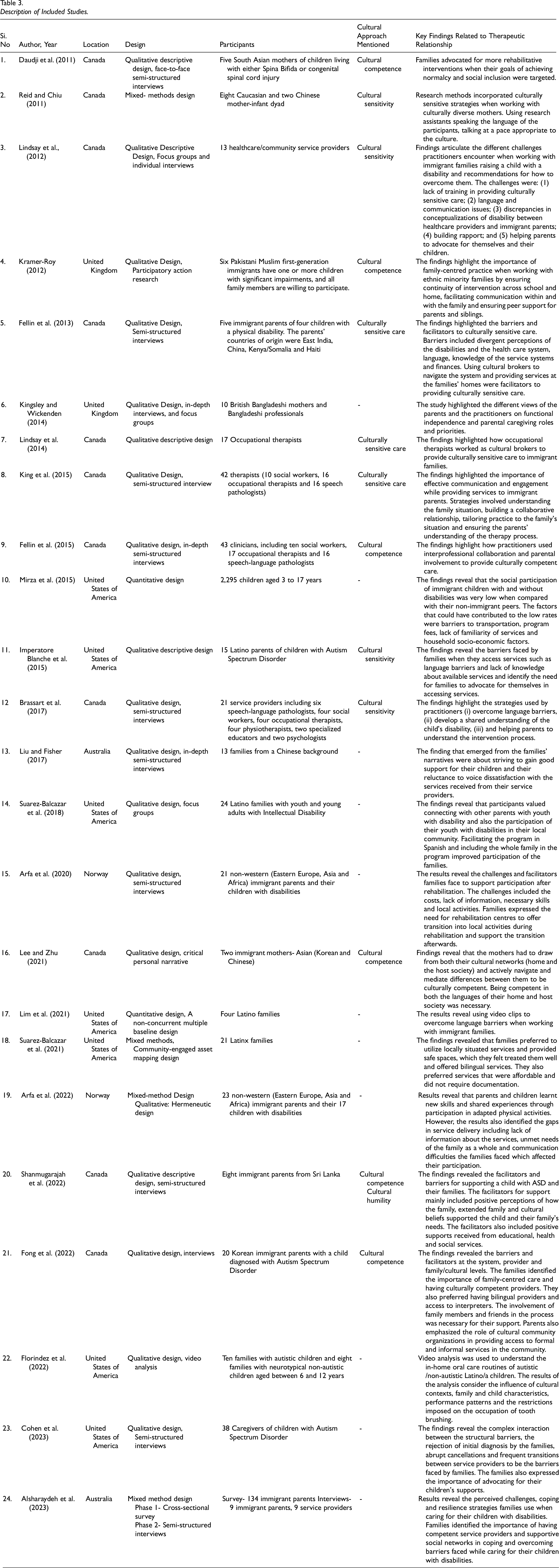
Description of Included Studies
Among the 24 studies incorporated into this analysis, a predominant focus emerged in high-income countries, with 11 studies conducted in the Canadian context. Additionally, a cohort of 13 studies extends across the United Kingdom, the United States of America, Australia, and Norway. The immigrant families considered in the included studies predominantly originated from middle and low-income countries including Eastern Europe, Asia, Africa, and Latin America.
Qualitative methodologies, to understand the perspectives of immigrant families of disabled children and their practitioners were used in 21 of 24 studies. These studies used data collection strategies including semi-structured and in-depth interviews, focus groups, and critical personal narratives. Of the studies published between 2011 and 2015, six out of 10 studies conducted predominantly encompassed the perspectives of the practitioners (Fellin et al., 2015; King et al., 2015; Kingsley & Wickenden, 2014; Lindsay et al., 2012, 2014; Reid & Chiu, 2011). From 2017 this trend shifted, with 11 out of 13 studies predominantly focused on the perspectives of the immigrant families of disabled children (Arfa et al., 2020, 2022; Cohen et al., 2023; Florindez et al., 2022; Fong et al., 2022; Lee & Zhu, 2021; Lim et al., 2021; Liu & Fisher, 2017; Shanmugarajah et al., 2022; Suarez-Balcazar et al., 2018, 2021). Three studies focused on how research methods (Reid & Chiu, 2011) and intervention strategies (Florindez et al., 2022; Lim et al., 2021) were used to respond culturally to immigrant families of disabled children.
Utilization of Cultural Approaches in Facilitating the Therapeutic Relationship
Deductive and inductive analysis identified three approaches—cultural sensitivity, cultural competence, and cultural humility—that promote the therapeutic relationship, as described in 15 of the 24 studies included. Cultural sensitivity and cultural competence were mentioned in 14 of the 24 studies (Brassart et al., 2017; Daudji et al., 2011; Fellin et al., 2013, 2015; Fong et al., 2022; Imperatore Blanche et al., 2015; King et al., 2015; Kingsley & Wickenden, 2014; Kramer-Roy, 2012; Lee & Zhu, 2021; Lindsay et al., 2012; 2014; Reid & Chiu, 2011; Shanmugarajah et al., 2022), and cultural humility was mentioned once as an approach to move towards (Shanmugarajah et al., 2022). Nine studies mentioned terms that were not included and defined in Beagan's (2015) critical synthesis of occupational therapy literature on culture and diversity such as culturally relevant, culturally tailored, culturally aware, culturally adapted and culturally responsive treatment to depict ways of responding culturally in the therapeutic relationship (Arfa et al., 2020, 2022; Cohen et al., 2023; Florindez et al., 2022; Lim et al., 2021; Liu & Fisher, 2017; Mirza et al., 2015; Suarez-Balcazar et al., 2018, 2021).
The notion of being culturally sensitive and responding competently was described to be the responsibility of the practitioners and not of the immigrant families of disabled children (Brassart et al., 2017; Daudji et al., 2011; Fellin et al., 2013, 2015; King et al., 2015; Kramer-Roy, 2012; Lim et al., 2021; Lindsay et al., 2012, 2014). These approaches require the practitioners to adopt strategies to accommodate the needs of the families accessing their services, such as addressing language barriers, taking time to understand the needs of the families, etc. (King et al., 2015; Lindsay et al., 2012). However, two studies in the review reveal how families used culturally competent strategies to interact within the therapeutic relationship (Lee & Zhu, 2021; Liu & Fisher, 2017). These strategies included acknowledging and informing how their views and beliefs were different to the ones held by their practitioners and finding ways to overcome the language and cultural barriers (Lee & Zhu, 2021; Liu & Fisher, 2017).
The occupational therapists and the families identified and trialed strategies that would facilitate the therapeutic relationship as further explained in the themes below. These strategies were independently described in the studies and were not specific to any one approach.
Themes
Following inductive thematic analysis, an overarching theme of using communicative and collaborative strategies was identified to facilitate the therapeutic relationship. The therapeutic relationships were built and sustained when these communicative and collaborative strategies were used to:
Build rapport and trust between immigrant families, their disabled child and their occupational therapist. Align goals and interventions to the values and resources of the immigrant families, and Facilitate advocacy and participation of immigrant families and their disabled children, in their community.
Sub-Themes
The strategies adopted to build rapport and trust were primarily described as the responsibility of the practitioners. Rapport and trust were built by using three strategies as described below:
Setting culturally responsive goals is challenging and can only be done when both the immigrant families and the occupational therapists contribute to the process (King et al., 2015). Families found it challenging to understand how they contributed to the process of goal setting (Arfa et al., 2022; King et al., 2015; Kramer-Roy, 2012). Practitioners described challenges in getting families involved in identifying priorities and getting them to understand the importance of their role in collaborative goal setting (Lindsay et al., 2012). The families viewed the practitioners as the experts in the relationship, thereby expecting them to make all the decisions and set the goals for the therapeutic process (Lindsay et al., 2012). Modifying goals and incorporating contextually relevant meaningful occupations tailored to the values, culture, and routines of the families facilitated culturally competent care (Fellin et al., 2015; Kramer-Roy, 2012).
To enable a culturally responsive intervention plan, practitioners adopted various strategies. Practitioners collaborated with the other team members, did home visits and tried to match practitioners with similar backgrounds or formed interprofessional teams with more ethnically diverse staff (Lindsay et al., 2012). Interprofessional collaborations allowed practitioners to share information, make decisions and support immigrant families holistically to provide culturally competent care (Fellin et al., 2015). They enabled immigrant families to access different services on the same day, reducing the burden of multiple visits (Fellin et al., 2015). Practitioners explained how they worked across professional lines and negotiated their professional roles to support immigrant families effectively (Fellin et al., 2015). Using tools to facilitate communication such as writing down instructions to take home, using emails rather than telephone calls to schedule appointments, using visual strategies such as pictures, photos, and drawings and using translation software (Brassart et al., 2017) enabled the implementation of the identified goals.
Strategies to facilitate advocacy among immigrant families have been suggested both by the families and the practitioners. The immigrant parents’ education and participation in the host country contributed to their awareness and capacity to advocate for their children (Liu & Fisher, 2017). Some immigrant parents organized meetings and lectures, met with policymakers and engaged in other related activities to advocate for change to the existing programs and support services catering for disabled children (Liu & Fisher, 2017). Facilitating constructive peer support among the families to support each other in similar situations and facilitating collaborations within and among community organizations enabled immigrant families to make the right links to facilitate advocacy (Florindez et al., 2022; Kramer-Roy, 2012; Lindsay et al., 2012). However, engaging immigrant families with each other should be considered cautiously as some families will be hesitant to share their child's disability with others of the same background (Alsharaydeh et al., 2023). Some families also identified their disabled youth as peer advocates for other families in similar situations (Suarez-Balcazar et al., 2018). Engaging the immigrant families to develop a directory of local community services that were affordable, bilingual/bi-cultural and had experience working with particular cultures (Suarez-Balcazar et al., 2021) also facilitated self-advocacy skills. Practitioners being aware of community resources also aided families in fostering their self-advocacy skills (Fellin et al., 2015; Lindsay et al., 2012).
Discussion
This study is a step towards understanding how cultural approaches are used to build and sustain the therapeutic relationship between immigrant families of disabled children and their occupational therapists. Cultural competence, cultural sensitivity, and cultural humility were the three approaches considered across 15 studies. Nine studies did not use any specific cultural approach to consolidate how the therapeutic relationship was built and sustained rather focused on the strategies facilitating the relationship. To facilitate the therapeutic relationship, culturally appropriate communication and collaboration strategies were used to: (i) establish a relationship of rapport and trust, (ii) align goals and intervention to the values and resources of the family, and (iii) facilitate advocacy and participation of the children and their families in the community.
The overarching theme of using communication and collaboration strategies to build and sustain the therapeutic relationship translated between those studies using specific cultural approaches and those that did not mention any specific cultural approach (Arfa et al., 2020, 2022; Brassart et al., 2017; Cohen et al., 2023; Daudji et al., 2011; Fellin et al., 2013, 2015; Florindez et al., 2022; Fong et al., 2022; Imperatore Blanche et al., 2015; King et al., 2015; Kingsley & Wickenden, 2014; Kramer-Roy, 2012; Lee & Zhu, 2021; Lim et al., 2021; Lindsay et al., 2012, 2014; Liu & Fisher, 2017; Mirza et al., 2015; Reid & Chiu, 2011; Shanmugarajah et al., 2022; Suarez-Balcazar et al., 2018, 2021) . This could imply that, in practice, the practitioners and the families did not rely on any specific cultural approach, but rather focused on how the therapeutic relationship could be built and sustained. Thereby reinforcing the essential occupational therapy process of building and sustaining the therapeutic relationship, as portrayed in the Canadian occupational therapy inter-relational practice process (COTIPP) framework (Restall et al., 2022). According to the COTIPP framework, the six action points that build and sustain the therapeutic relationship, which in turn promotes occupational participation are similar to the findings of this study: connect; explore occupational participation, seek understanding and define purpose; co-design priorities, goals, outcomes, and plan; trial plan, explore change and refine plan; and plan for transition (Restall & Egan, 2022). It may also point to the need to embrace the individuality and subjectivity of the individuals involved to guide the therapeutic relationship (Affun-Adegbulu & Adegbulu, 2020; Iwama et al., 2009), rather than universally defining cultural approaches. Cultural approaches often shape discourses on diversity and culture through their influence on formulating frameworks and models in the profession (Grenier, 2020). They also help educate and assist occupational therapists in understanding the cultural needs and expressions of the people involved in the relationship (Tilstra et al., 2023).
Findings reveal therapeutic relationships established with immigrant families of disabled children are an extension of family-centred care which involves viewing the entire family as a unit when building and sustaining the therapeutic relationship (King et al., 2015; Lindsay et al., 2012). This approach facilitates the families’ and their children's ongoing occupational participation even when direct therapeutic support ends. This supports transition planning as a crucial part of sustaining occupational participation, as emphasized in the COTIPP framework (Restall et al., 2022).
Finally, many of the strategies adopted to facilitate the therapeutic relationship were described as the practitioner's responsibility. Strategies initiated to build rapport and trust, align intervention and facilitate the participation of the families in the community were done mainly by the practitioners. This reinforces the expectation of the practitioners to be the expert in the therapeutic relationship and social positioning of the immigrant families that inadvertently produces a sense of the “other” (El-Lahib, 2016). The perception of the “other” is also imposed by the approaches of cultural competence and cultural sensitivity (Beagan, 2015), positioning the occupational therapist in a position of power and privilege and the immigrant families as the subordinate “other”(Grenier, 2020). The use of these approaches also reveals that the strategies suggested mainly focused on the race and ethnicity of immigrant families originating from low or middle-income economies; positioning the immigrants as the lesser “other” (Grenier, 2020; Ramugondo, 2018). This positioning and power imbalance also pose the question of whether this feeling of the practitioner being the expert (El-Lahib, 2016) would change if the immigrant families had a chance to contribute more actively to establishing the therapeutic relationship. Cultural humility is one of the cultural approaches that allows critical reflexivity of the social positioning of the families and occupational therapists in the therapeutic relationship (Agner, 2020). Cultural humility critically questions whose ways of knowing and being are valued and considered in the therapeutic relationship (Beagan, 2015; Beagan et al., 2023). However, the results show that this approach has not yet been translated into practice (Agner, 2020; Singh et al., 2022), which is true in the broader landscape of occupational therapy education and practice (Grenier, 2020). Tackling the power imbalance requires addressing the challenges and attitudes at the social and political systems rather than at the individual level (Grenier, 2020; Ramugondo, 2018). To name and act on the iniquities and power imbalances, it is important to engage with activist groups and politicians, transform educational frameworks and pedagogies, and recognize regional and global indigenous practices (Beagan et al., 2023; Grenier, 2020; Murphy et al., 2024). Educating and retaining a diverse occupational therapy workforce is also critical in catering to people from all ethnic and racial backgrounds (Lerner & Kim, 2022). These initiatives embrace decolonial and anti-oppressive ways (Pooley & Beagan, 2021; Ramugondo, 2018) and can contextually situate the profession in the rapidly evolving diverse cultural society (Beagan et al., 2023; Grenier, 2020; Murphy et al., 2024; Ramugondo, 2018).
Gaps Identified for Future Research
The findings of this scoping review reveal that practitioners and immigrant families adopt various strategies to facilitate the therapeutic relationship, rather than relying on a specific cultural approach. The cultural approaches mentioned were co-opted and defined in very different ways, making it difficult to consolidate the techniques into any particular approach.
Future research is required to contextually situate how social positioning impacts the therapeutic relationship between immigrant families of disabled children and occupational therapists including understanding the social positioning when occupational therapists themselves are immigrants. Using anti-oppressive and decolonial perspectives in understanding power relations in the therapeutic relationship can further expand discourse in this area (Lerner & Kim, 2022; Pooley & Beagan, 2021). Understanding the social positioning of each party in the relationship is particularly important in aligning therapeutic goals. Occupational therapists and immigrant families identified that this was often a challenging process compounded by the difficulties in identifying the priorities of immigrant families and understanding the roles and responsibilities of both the immigrant families and the occupational therapists. Therefore, exploring the roles and responsibilities assumed by immigrant families of disabled children and occupational therapists while aligning goals and exploring the process of goal-setting is necessary.
Strengths and Limitations
The study protocol was registered with the OSF registries ensuring that no other scoping reviews were conducted on this topic, making the findings novel. A strength of this scoping review was that it had been developed using the PRISMA checklist and the methodological framework proposed by Arksey and O'Malley (2005), which ensures the trustworthiness of the results and a comprehensive review of high quality. The study's trustworthiness was also increased through deliberation and collaboration with the research team, which comprised experts from the field of occupational therapy, including two immigrant researchers.
Limitations of this review included eliminating studies not published in English potentially excluding articles published in the Global South. Also, the scoping review methodology did not require critically appraising the rigour of the included studies.
Conclusion
The therapeutic relationship is facilitated through strategies adopted by occupational therapists and immigrant families of disabled children. Often these strategies do not align specifically with any of the cultural approaches, thereby making it difficult to define the use of cultural approaches in facilitating therapeutic relationships. Cultural competence, cultural sensitivity, and cultural humility are the three approaches mentioned in some of the reviewed studies to establish and sustain the therapeutic relationship, but more work is required to understand the impact of social positioning on the therapeutic relationship.
Key Messages
Understanding the discourses the various cultural approaches create in the therapeutic relationship should be considered in occupational therapy practice.
The relationship between occupational therapists and the immigrant families of disabled children can be built and sustained by building rapport and trust, aligning goals and interventions, and facilitating advocacy and participation.
There is a need to sustain the occupational participation of the families and their children even when direct therapeutic support ends.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174251363011 - Supplemental material for Establishing Therapeutic Relationships with Immigrant Families of Disabled Children: A Scoping Review
Supplemental material, sj-docx-1-cjo-10.1177_00084174251363011 for Establishing Therapeutic Relationships with Immigrant Families of Disabled Children: A Scoping Review by Sarah Ninan Fenn, Stephen Isbel, Claire Pearce and Daniela Castro de Jong in Canadian Journal of Occupational Therapy
Supplemental Material
sj-docx-2-cjo-10.1177_00084174251363011 - Supplemental material for Establishing Therapeutic Relationships with Immigrant Families of Disabled Children: A Scoping Review
Supplemental material, sj-docx-2-cjo-10.1177_00084174251363011 for Establishing Therapeutic Relationships with Immigrant Families of Disabled Children: A Scoping Review by Sarah Ninan Fenn, Stephen Isbel, Claire Pearce and Daniela Castro de Jong in Canadian Journal of Occupational Therapy
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
Sarah Ninan Fenn: conceptualization, methodology, acquisition of data, analysis and interpretation of data, writing the original draft. Dr. Stephen Isbel: conceptualization; methodology; supervision; writing—review and editing. Dr. Claire Pearce: conceptualization; methodology; supervision; writing—review and editing. Dr. Daniel Castro de Jong: conceptualization; methodology; supervision; writing—review and editing. All the authors have given final approval for the version to be published. All the authors have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All the authors have been involved in drafting the manuscript or revising it critically for important intellectual content.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.