
Abstract
Introduction
The early detection of cognitive difficulties and their management may result in improved intervention planning and prognosis. Promoting cognitive health and providing education and support for cognitive health to clients improves health outcomes (McGrath & O’Callaghan, 2014). Difficulties in cognition may manifest as difficulties in performing everyday tasks (Knight, 2000; Manitoba Society of Occupational Therapists, 2005). One of the goals of occupational therapists is to help individuals with various health conditions, such as sensory impairment, to maximize their daily functioning (Giles et al., 2020). Occupational therapists can perform cognitive screening using different approaches such as functional observation, standardized cognitive screening tests (e.g., the Mini-Mental State Examination, MMSE; Folstein et al., 1975), and/or noting clients’ self-reported cognitive complaints (Holmqvist et al., 2014; Manee et al., 2020). The most common approach used by occupational therapists to assess cognitive function is the observation of activities of daily living as a proxy measure of cognitive status (Manee et al., 2020); however, standardized cognitive screening tests can be more streamlined and complement functional assessments (Brown, 2015; Holmqvist et al., 2014).
Cognitive screening tools typically require clients to, for example, remember and repeat a list of spoken words or to identify the image of an animal. For these tasks, it is important to have good hearing and vision to ensure valid and reliable results. Should such a test be administered without accommodations (e.g., assistive technologies such as magnification and pocket talker), it becomes difficult to interpret whether a low score is attributable to cognitive difficulty or a sensory impairment (or both). In addition, when observing functional limitations, these may be misattributed to cognitive difficulties when, in reality, they are caused by impairments in hearing and/or vision (Uchida et al., 2019). This is a rapidly advancing research area, exploring the need to adapt cognitive screening measures for individuals with sensory impairments (Dawes et al., 2023, 2025; Dupuis et al., 2015; Harithasan et al., 2020; Whitson et al., 2018; Wittich et al., 2019; Wolski et al., 2019). Given that this population often presents with multiple comorbidities, sensory loss may be overlooked or given less priority in clinical settings.
A scoping review exploring the various accommodations used in research concerning older adults living with dual sensory impairment has highlighted the critical role of interdisciplinary collaboration in conducting cognitive evaluations (Dumassais et al., 2024). This review was specific to older adults, a population with a high prevalence of sensory impairment. However, sensory loss can present in clients across the age range who are seeking services in occupational therapy. Currently, there is no evidence as to whether occupational therapists recognize that cognitive screening of clients with sensory limitations is a concern in their practice. If they do, then it is not clear which strategies they employ to address sensory limitations. Therefore, it is essential to investigate the existing practices in occupational therapy clinical settings to explore this knowledge-to-practice gap.
Occupational therapists recognize the need for continuing education to increase knowledge on hearing, visual, and dual sensory impairments as well as cognitive rehabilitation (Holmqvist et al., 2014; Wittich et al., 2015). They may lack an in-depth understanding of how to manage and/or address sensory impairments in the context of cognitive screening. Therefore, the aim of the current study was to explore how occupational therapists screen for cognitive difficulties in clients with sensory impairments across the age range, as well as their self-perceived satisfaction with comprehensive service delivery. We explored the relationship between self-rated satisfaction with the ability to provide comprehensive occupational therapy, including the full range of assessments and interventions, and the number of reported accommodations used when working with this clientele. Additionally, we examined whether the reported accommodations and self-rated satisfaction varied based on the professional setting (e.g., clinics vs. long-term care [LTC]) and the extent of their professional experience.
Method
The study protocol received ethical approval from the Clinical Research Ethics Committee of the Université de Montréal (#2021-1252).
Study Design
Through a cross-sectional online survey, we recruited a convenience sample of Canadian occupational therapists working with clients who have potential cognitive concerns alongside preexisting sensory impairments, including (1) hearing impairment (HI; encompassing deaf and hard-of-hearing individuals), (2) visual impairment (VI), or (3) dual sensory impairment (DSI).
Participants and Recruitment
Provincial professional associations, regulatory colleges, and the Quebec order for Canadian occupational therapists were contacted via email by the first author. Invitations to professionals were distributed by these organizations in six provinces (Alberta, Manitoba, New Brunswick, Ontario, Quebec, and Saskatchewan) through their respective email lists and newsletters. The Canadian Association of Occupational Therapists agreed to support recruitment nationally. Only practicing occupational therapists who administer cognitive screening tests to individuals of any age with HI, VI, or DSI were eligible to participate. Invitations were also sent to occupational therapy researchers in a national research organization (Canadian Consortium on Neurodegeneration in Aging, 2024). We are unaware if any of the associations sent reminder emails. Fluency in reading and responding in English or French was required to complete the survey, and participation was voluntary, without financial compensation.
Study Instrument
Section 2 contained Likert-scale questions and multiple-choice questions regarding cognitive screening tools use, self-rated satisfaction with comprehensive service delivery ability, use of accommodations for sensory problems during the administration of cognitive tests, and interest in learning about accommodations for sensory impairments to enhance cognitive test administration. The survey questions about service delivery ability and education pertained to three distinct client groups: HI, VI, and DSI, whereas the questions about accommodations focused on the specific needs of four client groups: (1.1) clients who are hard of hearing (have some degree of hearing loss and may use assistive devices and spoken language), (1.2) clients who are deaf (deaf individuals identify as deaf and belong to this cultural community and may communicate by spoken language and/or use sign language for communication; Skelton & Valentine, 2003; Young & Hunt, 2011), (2) clients with VI, and (3) clients with DSI, considering their unique communication characteristics. For each sensory group, participants were provided with a selection of accommodation choices. Some accommodations could simultaneously apply to HI, VI, and DSI (e.g., encouraging the use of assistive technology). However, some accommodations were unique to specific sensory impairments, such as using Tadoma communication, a tactile method used by deafblind individuals (Sense, 2023). Participants had the option to select multiple accommodations.
Section 3 included questions about professional background and demographics (e.g., age, sex, gender, province of location, years of experience, and professional setting(s)), given their potential effect on cognitive screening with clients with sensory impairments and their influence on self-rated satisfaction with their comprehensive service delivery ability.
Data Collection
The survey was distributed through the LimeSurvey platform (LimeSurvey GmbH, 2022). Data were collected confidentially and stored electronically in a secure OneDrive folder at the Université de Montréal. The survey link was active from December 1, 2021, to March 22, 2022.
Data Analysis
The Jeffreys's Amazing Statistics Program (JASP) statistical software (JASP Team, 2022) was used for data analyses, using descriptive, Spearman's rank correlations and Kruskal–Wallis tests, as appropriate.
Results
Response Rate
The proportion of all provincially licensed occupational therapists who responded could not be calculated accurately because the number of active occupational therapists who were sent invitations to participate by each provincial professional organization was unknown.
Characteristics of Survey Participants
Ninety practicing occupational therapists completed the survey, based in Quebec (n = 66), Ontario (n = 21), Alberta (n = 1), British Columbia (n = 1), and the Canadian Territories (n = 1), Mage = 42.52 years (SD = 9.29, rangeage = 26–63), respectively. Overall, 40% of occupational therapists had more than 20 years (n = 36) of experience. Participants worked in various settings, with public hospitals being the most common (44%, n = 40). Sixteen occupational therapists were working across two different settings at the time of the survey, and two occupational therapists were working across three settings. The clientele they served most frequently was older adults (42%, n = 38). Most identified as female (96%, n = 86), with far fewer males (3%, n = 3), and one person chose not to disclose their sex (1%). In terms of gender identity, most identified as women, a few as men, and some as other identities (e.g., gender fluid and nonbinary), see Table 1 for details.
Survey Response Percentages and Participant Characteristics
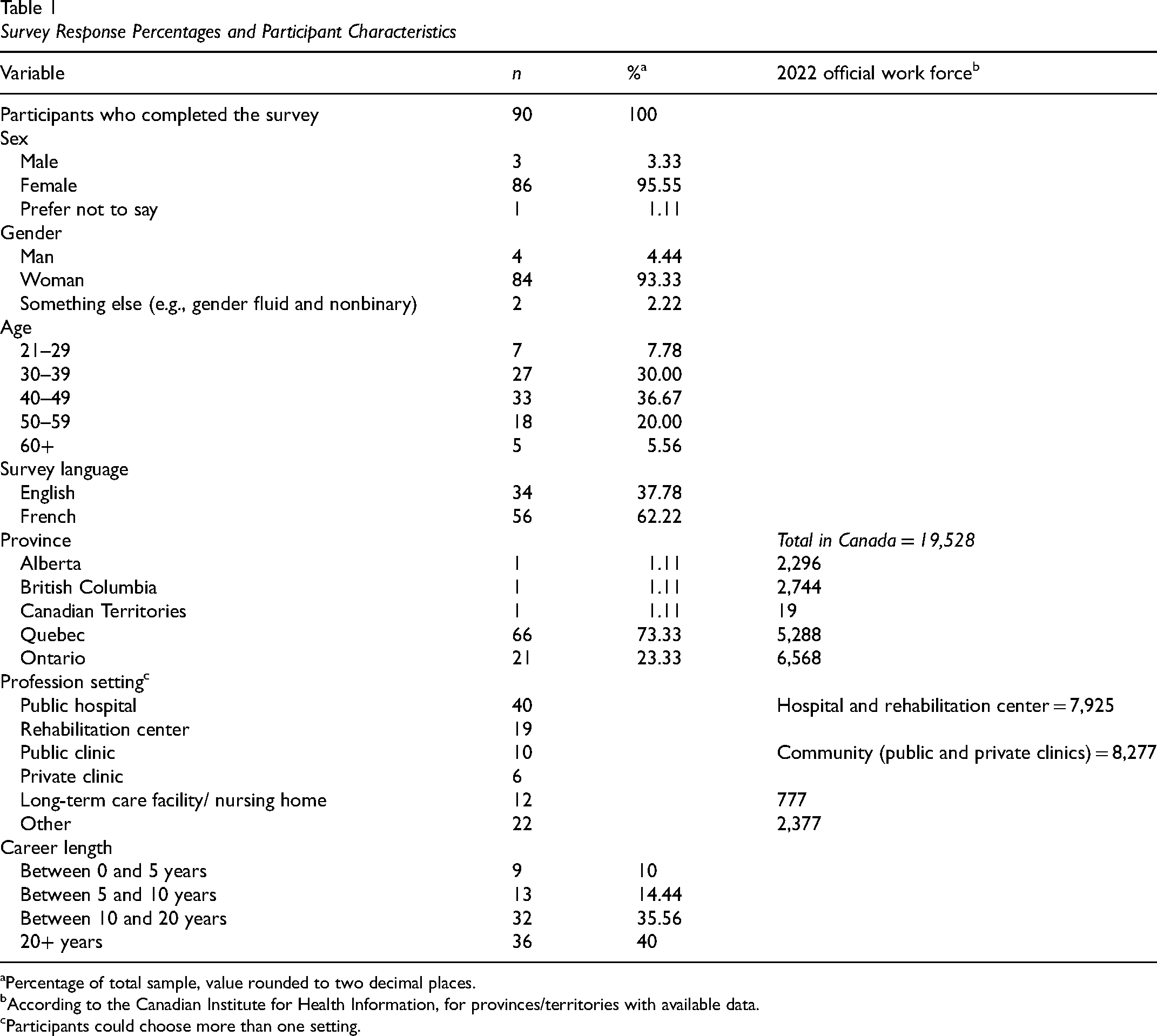
Percentage of total sample, value rounded to two decimal places.
According to the Canadian Institute for Health Information, for provinces/territories with available data.
Participants could choose more than one setting.
Use of Cognitive Screening Tools
Participants most frequently reported using the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005; n = 85) and the MMSE (Folstein et al., 1975; n = 69) to screen cognition in their clients. These results support evidence from global perspectives on cognitive screening, where the MoCA and the MMSE were among the top choices in occupational therapy practice (Manee et al., 2020). The next most frequently reported information source (n = 25) was cognitive complaints expressed by their clients, followed by use of cognitive subtests such as Trail Making tests and clock drawing tasks (n = 20). Other screening tools included the Cognitive Assessment Scale for the Elderly (Geneau & Taillefer, 1995; n = 7), the Rowland Universal Dementia Assessment Scale (Storey et al., 2004; n = 7), as well as functional observations. Only three clinicians specified the use of cognitive screening tests adapted for sensory impairment, including the MoCA in its blind version (Wittich et al., 2010; n = 1), a version of the MoCA adapted for people with HI (Dawes et al., 2023; Lin et al., 2017; n = 1), and the COGnitive Evaluation in VISual impairment (Meyniel et al., 2018; n = 1).
Self-Rated Satisfaction with Comprehensive Service Delivery Ability
Participants rated their overall satisfaction with their own ability to deliver services to individuals from the three sensory impairment groups (i.e., HI, VI, and DSI) on a 5-point Likert scale (1 = extremely unsatisfied to 5 = extremely satisfied). Comparison across the three sensory groups revealed a statistically significant main effect (HI, VI, and DSI), F(2, 178) = 35.58, p < .001, ηp2 = .295. Post hoc tests showed that service ability satisfaction was higher when services were provided to clients with VI (p < .001, d = 0.78) compared to clients with DSI (M = 2.32, SD = 0.91). Similarly, satisfaction was higher for clients with HI compared to clients with DSI (p < .001, d = 0.78). However, there was no statistically significant difference when comparing VI (M = 3.06, SD = 0.94) with HI (M = 3.06, SD = 0.83). Only three participants felt extremely satisfied with their ability to provide services to individuals with VI, while none declared the same for clients with HI or DSI. A greater number of participants were extremely unsatisfied with their ability to provide services to individuals with DSI (n = 19) compared to VI (n = 7) and HI (n = 4). Figure 1 provides a visual representation of the distributions of responses.
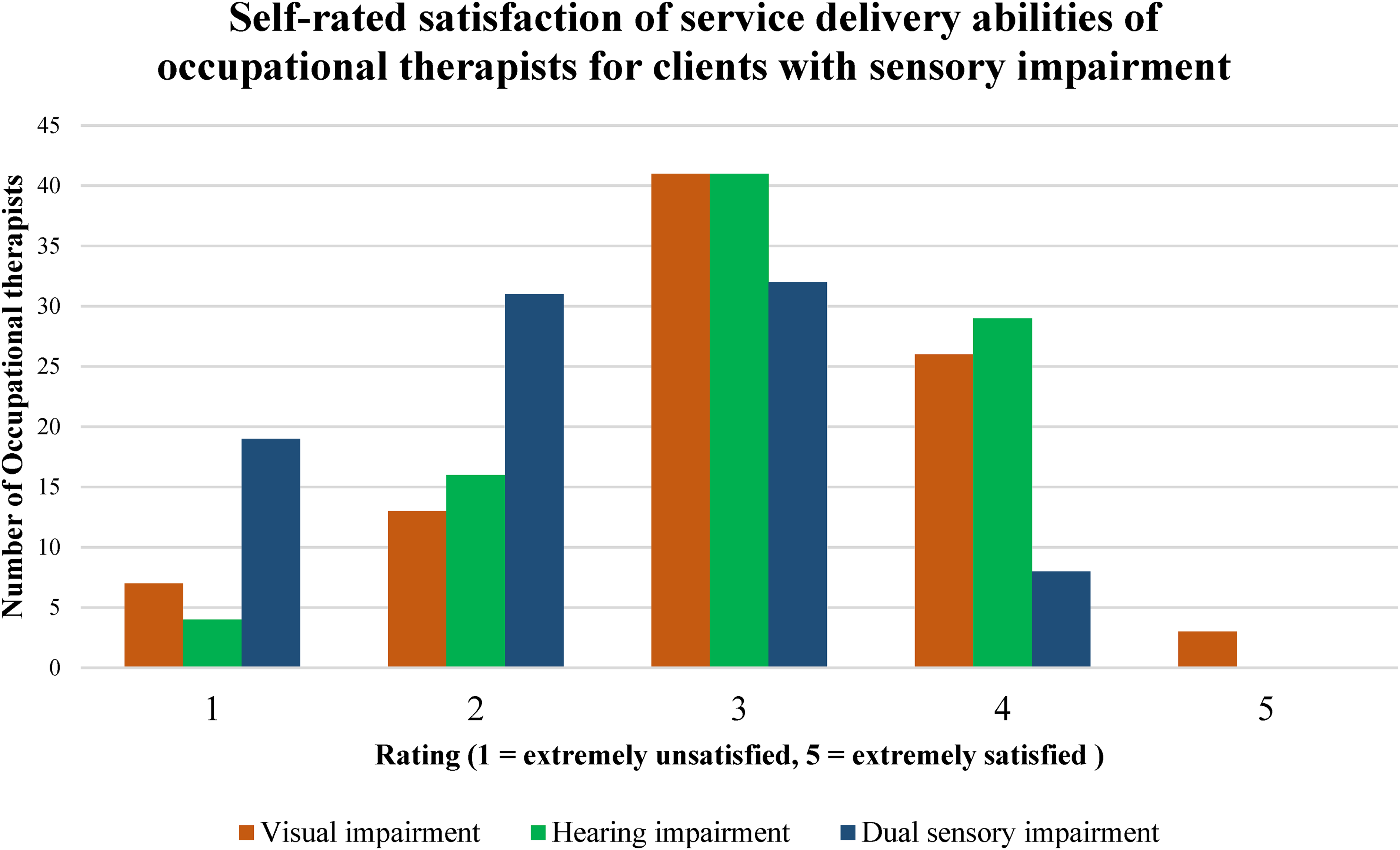
Self-rated satisfaction of occupational therapists in their ability to provide service for clients with sensory impairment.
Accommodations Used During Cognitive Screening Test Administration
Communication challenges for individuals who are hard of hearing differ from the challenges for those who are deaf because of variations in their auditory capabilities (mild, moderate, or severe impairment) and because of how sensory modalities are used for communication (spoken language communication and/or use of signed language). To capture differences in accommodations and communication preferences for specific subgroups of clients with HI, participants were asked separately about each subgroup within the larger HI group.
(1.1) Accommodations for clients who are hard of hearing. The number of accommodations used by participants had a mode of seven (range = 7–12). Eighty-eight participants reported prompting these clients to wear their hearing aid(s), while 87 noted that they conducted cognitive screening in an environment that is as quiet as possible and ensured that they spoke slowly and clearly with an appropriate tone (n = 86). See Table 2 for the complete list of accommodations used with clients who are hard of hearing. (1.2) Accommodations for clients who are deaf. The number of accommodations used by participants had a mode of one (range = 0–12). For clients who are deaf, the most reported accommodations included ensuring face-to-face communication to promote lip- and speech-reading (n = 42), encouraging the use of hearing aids/cochlear implants (n = 35), and speaking at a slower, clearer pace with an appropriate tone (n = 33). Twenty-nine occupational therapists reported ensuring the presence of an intervenor (a trained professional who acts as the eyes and ears of a person who is deafblind) during the interaction. See Table 3 for the complete list of accommodations for working with clients who are deaf. (2) Accommodations for clients with VI. The number of accommodations used by participants had a mode of 6 (range = 2–12). The most reported accommodation was to encourage clients to use their personal visual aids (e.g., such as glasses, magnifiers, or closed-circuit devices) during test administration. Over 95% (n = 86) of participants implemented this strategy in their practice. Seventy-six occupational therapists ensured that the lighting in the room was adequate for reading as an environmental strategy. Screening visual function using a subjective assessment before performing the cognitive test was the third most reported strategy (n = 64). See Table 4 for the complete list of accommodations. (3) Accommodations for clients with DSI.
The number of accommodations used by participants had a mode of 3 (range = 0–9). Nine occupational therapists reported not making use of any unique accommodations for DSI during the administration of cognitive screening tests. Though not unique to DSI, encouraging clients to wear their visual and hearing aids was a commonly reported accommodation (n = 62). Participants also indicated that they asked their clients to self-report any VIs and/or HIs (n = 57). Additionally, when clients did not have their own assistive technologies, participants offered them available options, such as magnifiers and/or pocket talkers, during the cognitive test (n = 41). The complete list of accommodations for working with clients with DSI is available in Table 5.
Frequency and Percentage of Occupational Therapists Who Selected Each Suggested Accommodation During Cognitive Screening Tests with Clients Who Are Hard of Hearing (i.e., Those Who Use Spoken Communication)
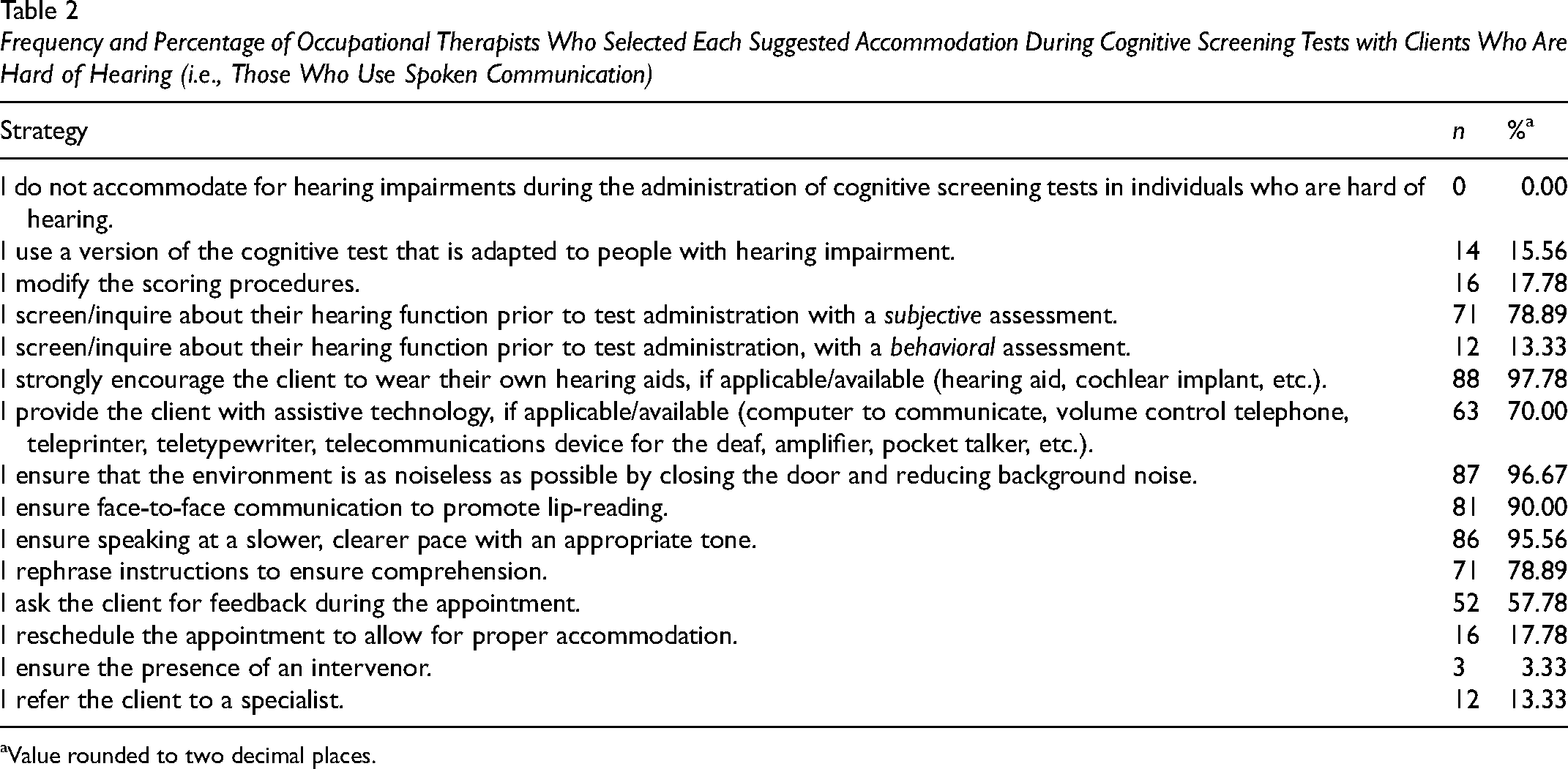
Value rounded to two decimal places.
Frequency and Percentage of Occupational Therapists Who Selected Each Suggested Accommodation During Cognitive Screening Tests with Clients Who Are Deaf and May Use Sign Language
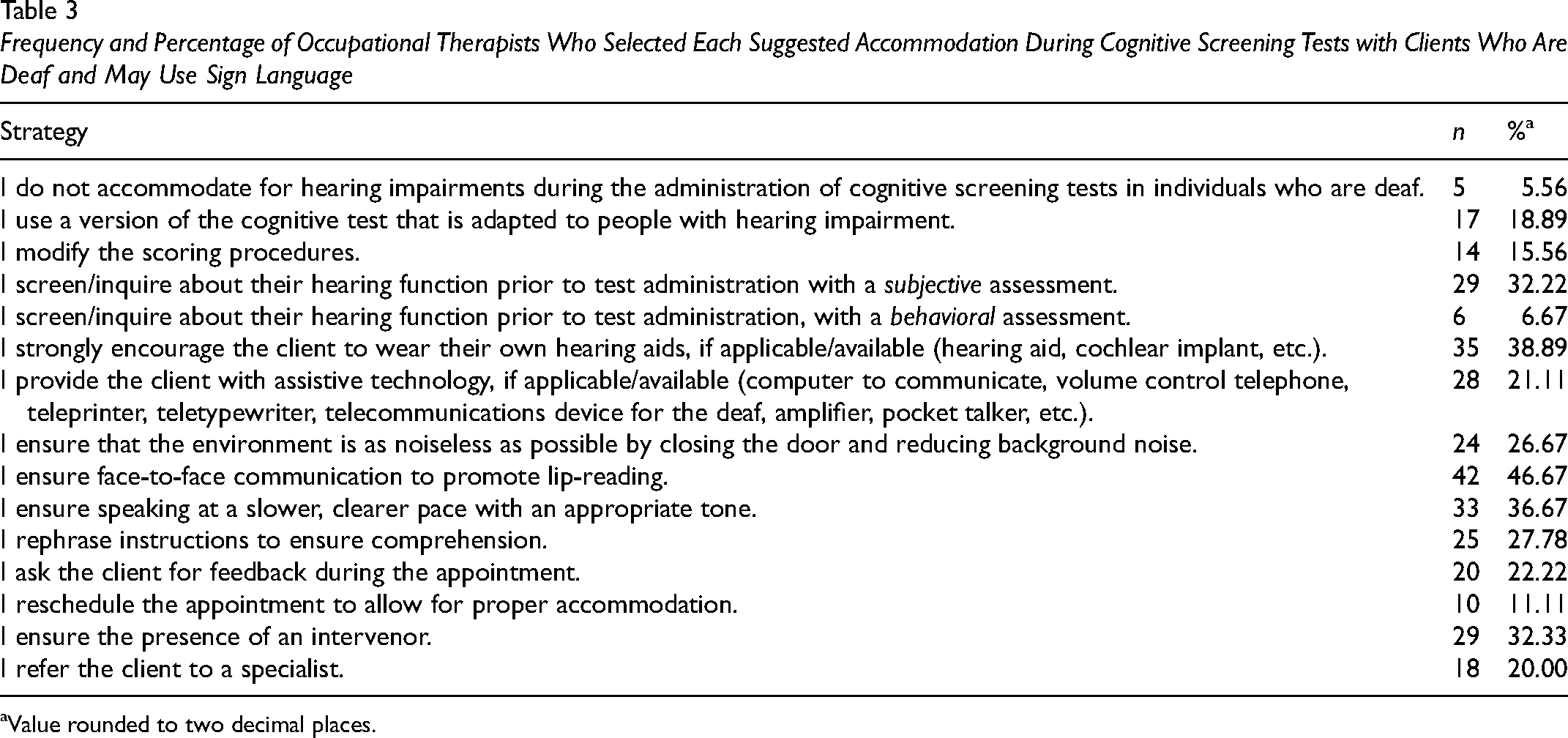
Value rounded to two decimal places.
Frequency and Percentage of Occupational Therapists Who Selected Each Suggested Accommodation During Cognitive Screening Tests with Clients Living with Visual Impairment
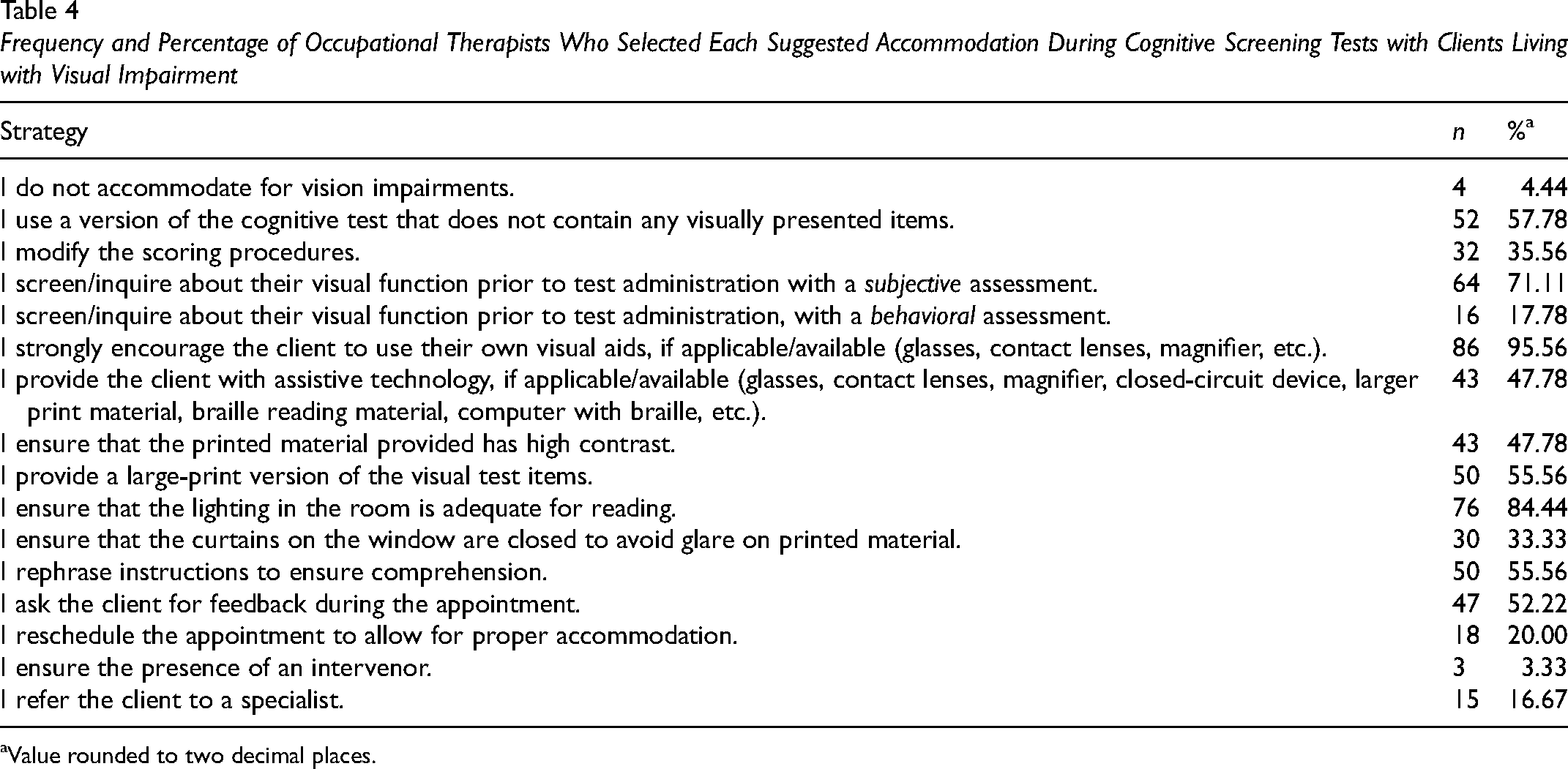
Value rounded to two decimal places.
Frequency and Percentage of Occupational Therapists Who Selected Each Suggested Accommodation During Cognitive Screening Tests with Clients Who Live with Dual Sensory Impairment
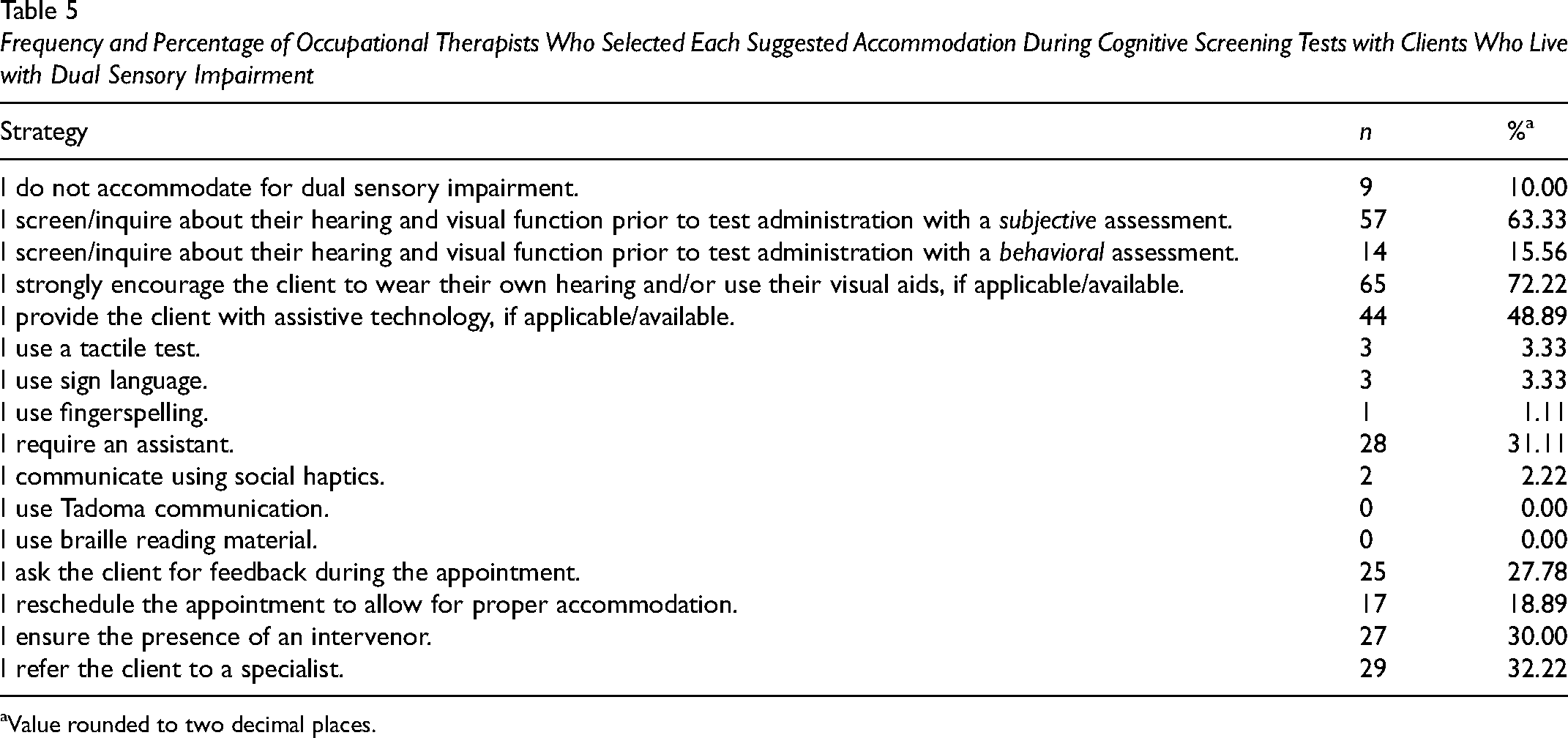
Value rounded to two decimal places.
Associations Between Self-Rated Satisfaction with Comprehensive Service Delivery Ability and Number of Reported Accommodations
For each of the four sensory impairment client groups (hard of hearing, deaf, VI, and DSI), Spearman's rank correlations were used to determine whether there were associations between self-rated satisfaction with the ability to provide services (between 1 and 5) and the number of accommodations used. Statistically significant positive correlations between satisfaction ratings and number of accommodations were found when occupational therapists were working with clients who are hard of hearing, ρ(88) = .26, p < .05, 95% confidence interval (CI) [0.05, 0,44], and clients with DSI, ρ(88) = .35, p < .05, 95% CI [−0.15, 0.52], whereby higher numbers of accommodations were associated with greater self-perceived satisfaction with service ability. There was no statistically significant correlation between self-rated satisfaction with ability to provide services and the number of reported accommodations for the client group with VI, ρ(88) = .16, p = .143, 95% CI [−0.05, 0.35], or the clients who are deaf, ρ(88) = .20, p = .058, 95% CI [−0.01, 0.39].
Effects of Professional Experience on Satisfaction with Comprehensive Service Delivery Ability and on Number of Reported Accommodations
Kruskal–Wallis tests were conducted to compare whether ratings of self-rated satisfaction with ability to provide services differed across the four different levels of professional experience (between 0 and 5 years, between 5 and 10 years, between 10 and 20 years, and 20+ years); separate analyses were conducted for each sensory client group (HI, VI, DSI). These analyses indicated that self-rated satisfaction with ability to provide services did not differ as a function of how long occupational therapists had been working in the profession and this applied to all three sensory impairment groups, HI: F(3, 86) = 3.91, p = .272, ηp2 = .038; VI: F(3, 86) = 3.26, p = .354, ηp2 = .037; and DSI: F(3, 86) = 0.31, p = .957, ηp2 = .004.
The same analysis was conducted to compare whether the number of accommodations differed across the same levels of professional experience. They did not differ as a function of professional experience for three of the sensory impairment groups, deaf: F(3, 86) = 2.74, p = .433, ηp2 = .022; VI: F(3, 86) = 7.55, p = .056, ηp2 = .090; and DSI: F(3, 86) = 5.31, p = .151, ηp2 = .060. Although a main effect was observed when occupational therapists worked with clients who are hard of hearing, F(3, 86) = 8.83, p = .032, ηp2 = .096, post hoc tests with Bonferroni corrections did not identify any group that significantly differed from the others. The lack of significance may be attributed to the unequal number of participants across the various professional experience groups (i.e., between 0 and 5 years (n = 9), between 5 and 10 years (n = 13), between 10 and 20 years (n = 32), and 20+ years (n = 36), as well as the small overall effect size.
Effects of Professional Setting on Satisfaction with Comprehensive Service Delivery Ability and on Number of Reported Accommodations
Kruskal–Wallis tests indicated that there were no differences in self-rated satisfaction with ability to provide services for the different professional settings of participants (six levels, i.e., hospital, rehabilitation center, public clinic, private clinic, LTC facilities, and nursing homes) for any of the three sensory impairment client groups, HI: F(4, 72) = 2.47, p = .650, ηp2 = .029; VI: F(4, 72) = 0.60, p = .964, ηp2 = .014; and DSI: F(4, 72) = 1.52, p = .824, ηp2 = .023. Additional Kruskal–Wallis tests indicated that there were no differences in the number of accommodations used among participants working in the six different professional settings, for any of the sensory conditions, hard of hearing: F(4, 72) = 1.83, p = .767, ηp2 = .017; deaf: F(4, 72) = 3.41, p = .492, ηp2 = .035; VI: F(4, 72) = 3.16, p = .532, ηp2 = .048; and DSI: F(4, 72) = 4.56, p = .333, ηp2 = .050.
Desire for Continuing Education Related to Sensory Accommodations for Cognitive Testing
All 90 participants were asked about the accommodations for working with clients with DSI that they would like to learn more about. The survey targeted this question about clients with DSI specifically, given existing gaps in Canadian occupational therapy academic training regarding this particular population (Wittich et al., 2017). The most frequently indicated learning needs included communication accommodations (n = 79) and cognitive test alterations to be used when administering existing cognitive screening tests, such a modified scoring (n = 78).
The nine participants who indicated that they did not accommodate cognitive screening assessment protocols for the needs of individuals with VI (n = 4) or HI (n = 5) expressed a greater interest in expanding their knowledge about potential test accommodations for sensory impairments that can be applied when administering existing cognitive screening tools such as adjusting scoring criteria or omitting specific tasks or subtasks. They preferred this focus over other accommodations, such as the use of communication strategies and technology. No qualitative data were collected to explain why increased knowledge on test accommodations was preferred over other initiatives.
Discussion
The purpose of this study was to survey Canadian occupational therapists about the accommodations they use for clients with sensory impairments during cognitive screening and explore their self-perceived satisfaction with comprehensive service delivery. We also explored participants’ levels of satisfaction with their own ability to deliver services to their clients with HI, VI, and DSI and how self-satisfaction may be associated with the number of reported accommodations, professional experience, and professional settings. The accommodations utilized by the participants with clients varied depending on the sensory client group. The highest number of accommodations was reported for clients who are hard of hearing, followed by clients with VI, clients who are deaf, and clients with DSI. Occupational therapists reported using a combination of communication and environmental accommodations for each client group. The number of each type of accommodation varied across each of the sensory impairments. Factors influencing this variation likely included the awareness of sensory function by both the occupational therapist and the client. Additionally, the resources available, such as assistive technology, may have also played a role. Both self-rated satisfaction with ability to provide services and the number of reported accommodations did not differ as a function of professional setting or years of professional experience working with clients with any type of sensory impairment. Greater self-rated satisfaction with the ability to provide services was associated with using a larger number of accommodations, but only for clients who are hard of hearing and clients with DSI. As a result, future studies might benefit from investigating the decision-making process of clinicians for these specific sensory impairment client groups, including the factors that help them choose which accommodations to use and how these accommodations facilitate service delivery.
Previously, occupational therapists have reported relying on their clinical experience as a guide in clinical decision making in comprehensive service provision (Dysart & Tomlin, 2002). Consequently, it was expected that occupational therapists with more years of clinical experience would use more accommodations than occupational therapists with less experience. Our sample consisted mainly of experienced occupational therapists, with 76% having worked as occupational therapists for 10+ years, of which 40% had worked as occupational therapists for 20+ years. An absence of differences in service delivery satisfaction among the four different levels of professional experience could be due to the uneven distribution across experience categories or the sample size being simply too small to detect differences between the subgroups. Additionally, we speculate that factors such as the quality of professional experience, engagement in continuing education, adaptability to service delivery contexts, mentorship, and individual differences in attitudes toward conducting cognitive screening might also be influential. These attitudes include confidence in administering cognitive tests and appropriately approaching clients with these tests (Dumassais & Wittich, 2024). These factors collectively may influence the development and maintenance of professional skills over time. However, other factors, relating to the geographical and regional differences of our sample, could also play a role. Our sample is not representative enough of the Canadian occupational therapy workforce for us to make any generalizable inferences.
Aside from the characteristics of the workforce, the profile of their clientele is also changing. Aging is correlated with the development of HI and/or VI, and cognitive dysfunction (Court et al., 2014; Maggi et al., 1998; van der Flier, 2005), and both VIs and HIs have been identified as potentially modifiable risk factors for dementia (Livingston et al., 2024). Notably, sensory impairment and cognitive difficulties are prevalent conditions among patients in LTC (Guthrie et al., 2018; Kwan et al., 2022). Residents in LTC are mostly older individuals with chronic comorbid illnesses (Ontario Long Term Care Association, 2019), with a high prevalence of sensory loss. Consequently, we expected that occupational therapists working in LTC would rate themselves as being more satisfied with their ability to provide services to clients with sensory impairments compared to those working in other settings that serve a wider variety of age groups. However, our results did not indicate this relationship. In line with previous data on curricula and sensory health education, we speculate that occupational therapists may simply not have enough knowledge on how to manage and/or address sensory impairments (Wittich et al., 2017). Other factors may influence occupational therapists’ self-rated satisfaction with their ability to address the needs of individuals with sensory impairment, such as their clients’ health status. Additionally, the occupational therapists’ academic training, which is unequal across Canada, can play a role (Wittich et al., 2015). Limited resources and the extent of interprofessional collaboration are also significant factors (Dunsmore et al., 2024). Finally, organizational culture (e.g., promoting teamwork, communication, and collaboration) is likely important for the overall performance of healthcare professionals as well as patient outcomes (Almutairi et al., 2022; Braithwaite et al., 2017; Mannion & Davies, 2018). Although not directly linked to clients’ sensory abilities, these factors may influence occupational therapists’ self-perceived satisfaction with their practice.
Professional education related to serving clients with DSI is not covered well in Canadian occupational therapy training compared to the training received on unisensory impairments (Wittich et al., 2017). This gap could explain why over 86% of occupational therapists expressed an interest in learning about adaptations to existing cognitive screening/assessment that could be used to screen cognition in clients with DSI. The only published cognitive screening tools adapted for this population are tactile tests (Bruhn & Dammeyer, 2018; Janssen et al., 2007; Papagno et al., 2017); however, these have not been standardized and validated for use in clinical practice. Moreover, it remains unclear if these tactile tests are sufficiently specific, sensitive, and/or reliable to detect cognitive impairment. Therefore, it is meaningful to explore evidence-based accommodations such as the use of assistive technology, communication accommodations, and environmental modifications designed to enhance the validity of screening tests for DSI that are already used in practice. Such accommodations could improve the sensitivity and specificity of cognitive tests with individuals with DSI; however, as an alternative, it may be informative clinically to observe the client's functioning in everyday life when standardized procedures cannot be followed.
Occupational therapists must learn to navigate the heterogeneous profiles and needs of clients with DSI given that this clientele's communicative abilities depend on the etiology of the DSI and the age of onset of the HI and VI (Wittich & Simcock, 2019). The complexity of their care is reflected in clinical practice, where, in the current study, occupational therapists reported significantly lower self-rated satisfaction in their ability to provide services for their clients with DSI than their clients with a single sensory impairment. In addition, our participants reported using the fewest number of accommodations when conducting cognitive screening tests with individuals with DSI. Few occupational therapists employed communication accommodations specifically adapted for clients with DSI, such as using fingerspelling, Tadoma communication, or tactile tests. In the absence of specialized support services such as intervenors, interpreters, and/or care partners, the effective use of these communication accommodations would require a considerable amount of time, training, and resources, and may not be practical in daily occupational therapy practice. Such support services are especially important considering that DSI significantly challenges patient/client-provider communication (Saunders & Echt, 2007). Although we recognize the practical limitations for occupational therapists to undertake such specialized training, alternatives may be helpful. For example, a curriculum is currently being developed to incorporate key competencies aimed at enhancing service provision for individuals with vision loss (Foster et al., 2024); however, to our knowledge, such curricula are currently absent for hearing or DSI. These key competencies include knowledge of eye conditions, the exchange of best practices among colleagues, the recognition of the need for expert support, and, above all, the promotion of awareness of vision loss (Foster et al., 2024). If occupational therapists do not receive specific training on these competencies through formal education, continuing education serves as a viable alternative.
The most frequently reported accommodations require awareness (i.e., expecting the individual to be aware of their vision/hearing difficulties) and resources (i.e., expecting the individual to own suitable assistive technology). These approaches place the responsibility for effective adaptation on the client; however, this approach may be at times problematic because not all clients may be aware of their level of sensory impairment or the tools and services available to them (Jacob et al., 2022). Furthermore, certain clients may be reluctant to disclose sensory and/or cognitive difficulties due to the associated stigma (Shakarchi et al., 2020; Werner & Heinik, 2008). We speculate that some clients who may have had access to such resources did not use them during the cognitive screening tests. In such instances, the occupational therapist can support only if the necessary resource is available in their professional environment. A significant problem arises when neither party has access to these resources or awareness about sensory difficulties, which may partially be responsible for the satisfaction scores observed in the current study.
The Integrated Care for Older People (ICOPE) Handbook supports community health workers in identifying and addressing difficulties in daily functioning, encompassing cognitive function, mobility, nutrition, sensory impairments, and depressive symptoms, using an interprofessional approach to integrated care (World Health Organization, 2024). This resonates with occupational therapy principles, striving to prevent care-dependency and improve well-being. The results of the current study support the promotion of knowledge exchange initiatives like ICOPE within the occupational therapy community. Such initiatives could facilitate the integration of evidence-based practices for cognitive screening and intervention by expanding occupational therapists’ professional capacities as part of the interprofessional care team, ultimately resulting in improvement of the well-being of individuals with sensory impairments. Our sample expressed significant interest in continuing education to learn new accommodations for conducting cognitive screening in individuals with DSI, with nearly 80% of our sample expressing this need for at least one focus, such as communication accommodations. Despite the availability of some webinars on single sensory impairments, with less information on DSI, these may not be sufficient, as evidenced by low satisfaction with the ability to deliver services. Future research should investigate whether these educational initiatives are adequate and understand why satisfaction with service delivery to clients with DSI remains low among occupational therapists.
Limitations and Future Directions
The nature of our multiple-choice questions limited the participants’ responses regarding the available choices of accommodations. We did not collect additional details on the specific assistive technologies used by clients or provided by occupational therapists, or information on whether these technologies were monitored for usability and functionality (e.g., battery charge). We did not gather information about environment-specific variables such as ambient noise levels where cognitive screening tests are conducted. The questions were instead designed to rapidly gather essential information to inform future research. Future qualitative interviews could provide a means of acquiring greater in-depth information and could explore how occupational therapists can identify individuals with HI and/or VI, particularly those who have not sought help. It is important to consider whether it is appropriate to assume that individuals with sensory loss necessarily use assistive technology such as hearing aids or magnifiers.
The categorization of clients into the various sensory impairment client groups (hard of hearing, deaf, VI, DSI) was applied very broadly. It is evident that sensory impairments can be related to different etiologies and levels of severity and can vary in age of onset and present in different ways across the lifespan. Individuals with sensory impairment are a highly heterogeneous population, and grouping them so broadly does not provide a nuanced perspective on the different contributing factors. Future studies should aim to incorporate a diverse range of causes of sensory impairment in their samples to identify condition-specific nuances and compare these with a control group of individuals without sensory impairments. Alternatively, studies could focus on understanding these interactions within specific populations, exploring more precise, individualized approaches to addressing the issues. Rather than adopting a broad, inclusive approach that may dilute insights, researchers should carefully examine different ages and etiologies.
A notable characteristic of this study sample is that we neither specifically targeted nor excluded occupational therapists who self-identified as having expertise in sensory impairment. In fact, only four occupational therapists self-identified as having expertise in vision impairment, while none reported expertise in hearing or DSI. Had we focused on occupational therapists specializing in this area, the findings regarding identified strategies and satisfaction with service delivery for this population likely would have differed. Therefore, the results of this study reflect the experiences of a broader representation of occupational therapists. Notably, between 5% and 10% of our sample reported not accommodating sensory loss at all during cognitive assessments. Future research should investigate whether this is influenced by a lack of expertise or training in accommodating for sensory impairments, particularly among older adults, or perhaps by a perceived need to adhere strictly to the standardized administration protocols for cognitive measures. Furthermore, the disproportionate representation of women/females compared to men/males in the sample highlights the ongoing sex and gender imbalance within the current Canadian workforce, where, in 2023, 90.3% of the occupational therapy workforce was female (Canadian Institute for Health Information, n.d.). Additionally, the study sample is biased toward participation from Quebec, where occupational therapy training differs somewhat from the rest of the Canadian provinces (Wittich et al., 2017). Future research should include a more balanced sex and gender distribution, along with proportional representation across Canadian provinces, to enhance the validity and applicability of the results.
Conclusion
Our study provides preliminary insight into how satisfied Canadian occupational therapists are with their own ability to provide services to their clients with sensory impairment(s) and what accommodations they put in place to facilitate the administration of cognitive screening tests to these clients. Our findings raise important points that can be considered in future studies that may encourage innovation in the development of new tools and technologies designed to facilitate cognitive assessments in those with sensory impairment(s). Understanding how occupational therapists perceive their ability to provide services to clients with sensory impairments can also lead to targeted training and improvements in service delivery.
Despite our sample being primarily composed of experienced occupational therapists, service delivery to clients with DSI was identified as a significant challenge in their practice. This challenge is further highlighted regarding cognitive screening, where fewer accommodations are applied for this population compared to clients with only HI or VI. The need for continuing education opportunities focused on DSI is outlined in this study, as occupational therapists have expressed significant interest in these initiatives, particularly in addressing this complexity. Educational institutions could incorporate more comprehensive training on sensory accommodations and cognitive screening procedures tailored for clients with single sensory impairment. However, for DSI, such procedures still need to be developed and validated before they can be implemented. Ultimately, improving occupational therapists’ confidence and ability to provide services for clients with sensory impairments can lead to better outcomes as clients are more likely to receive accurate assessments and appropriate interventions.
Key Messages
The accuracy of cognitive screening tests can be compromised in clients with VIs and/or HIs, emphasizing the need for tailored approaches in occupational therapy.
Occupational therapists in Canada employ various accommodations during cognitive screening, such as enhancing lighting for those with VIs and adjusting communication techniques for clients with HIs. However, greater challenges were reported when screening the cognition of clients with DSI, as indicated by the fewer strategies used to address sensory needs and the lower satisfaction with their overall ability to provide the full range of occupational therapy services with this population.
The study underscores the necessity for standardized strategies and enhanced training for occupational therapists to effectively conduct cognitive screenings, especially for clients with DSI.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174251361594 - Supplemental material for Navigating Cognitive Screening and Service Delivery for Sensory Impairment in Occupational Therapy
Supplemental material, sj-docx-1-cjo-10.1177_00084174251361594 for Navigating Cognitive Screening and Service Delivery for Sensory Impairment in Occupational Therapy by Shirley Dumassais, Jennifer Campos, Margaret Kathleen Pichora-Fuller, Joseph B. Orange, Marie Savundranayagam, Paul Mick and Natalie A. Phillips, Walter Wittich in Canadian Journal of Occupational Therapy
Footnotes
Acknowledgments
The authors gratefully acknowledge the invaluable contributions of the principal investigators and trainees of Team 17 of the Canadian Consortium on Neurodegeneration in Aging, whose collaboration was essential to the conception, execution, data analysis, and interpretation of this study, as well as the writing of the manuscript. We also express our sincere appreciation to the Canadian Association of Occupational Therapists and the Canadian Consortium on Neurodegeneration in Aging for their assistance in recruiting occupational therapists across Canada. Additionally, we thank the various provincial regulatory bodies for occupational therapy for their crucial support in facilitating recruitment.
ORCID iDs
Funding
Dumassais was supported by a Canadian Institutes of Health Research Canada Graduate Scholarships for her master’s studies.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.