
Abstract
Introduction
According to the results from the Canadian COVID-19 Antibody and Health Survey (CCAHS) about 1 in 9 (11.7%) of Canadian adults who had or thought they had COVID-19 still have lingering symptoms 3 months after their initial infection, which represents about 3.5 million Canadian adults (Government of Canada, 2023). Long COVID is currently being defined as “the continuation or development of new symptoms 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 months with no other explanation” (WHO, 2022). The most reported symptoms by Canadians include fatigue, coughing, shortness of breath, brain fog, and general weakness (Government of Canada, 2024). Individuals living with COVID-related symptoms for more than 6 months have also reported cognitive dysfunction, sensorimotor symptoms, headaches, and memory issues (Davis et al., 2021). About 1 in 5 of those affected report that the symptoms limit them in their daily activities (Government of Canada, 2023).
Furthermore, post-exertional malaise (PEM), affects the majority of individuals with long COVID (Twomey et al., 2022). PEM is a worsening of symptoms and reduction in function following physical, emotional, or cognitive activities (Twomey et al., 2022). The effort exerted to engage in these activities leads to a malaise characterized by fatigue post-exertion (Twomey et al., 2022). This malaise can vary in length of time: from hours to days to weeks, depending on the individual (Provincial Health Services Authority, 2022), and may impact individuals’ daily activities, family, and societal roles (Twomey et al., 2022). Considering the persistent symptoms in their daily lives, a decrease in overall function seems to be preventing individuals from returning to work. Indeed, delayed return to work (RTW) has been prominent in this population (Jacobsen et al., 2022). Long COVID was also linked to an increased risk of unemployment and a lower likelihood of maintaining full-time employment (Perlis et al., 2023). Among those who have attempted a return to the workforce while living with long COVID, many experience relapses triggered by exposure to stress, physical activity, or mental stress (Davis et al., 2021).
Rehabilitation may reduce the burden of long COVID symptoms and is therefore recommended to support the recovery of individuals living with this condition (Gerlis et al., 2022). Recovery for individuals with long COVID is mostly focused on optimizing function rather than trying to return to their pre-COVID functioning (DeMars et al., 2022b). Although it seems to be distinct for every person, one study reported that the majority of individuals with long COVID required at least 35 weeks of recovery (Davis et al., 2021). While existing rehabilitation guidelines recommend the involvement of a multidisciplinary team in the rehabilitation trajectory of individuals with long COVID (Alberta Health Services, 2022; NICE, 2022; WHO, 2023), occupational therapists play a crucial role in long COVID rehabilitation, specifically in regards to returning to work (von Zweck et al., 2023). Recommended rehabilitation strategies for the long COVID population are patient education, which includes recognizing individual symptoms and triggers of PEM, identifying activities within tolerable limits, as well as applying energy conservation principles (Alberta Health Services, 2022; WHO, 2023). Although these recommendations are based on a combination of expert opinions and evidence from comparable health conditions and disease processes, there is no direct evidence on the effectiveness of these interventions for long COVID rehabilitation, particularly regarding PEM (WHO, 2023). Additionally, it is unclear how to implement RTW interventions while respecting timelines that best accommodate the specific needs of individuals with long COVID. This leaves rehabilitation professionals without specific steps to undertake with this population. Seeing as long COVID is an emerging condition with an increasing prevalence in the rehabilitation field, there is a need to establish best practices to promote a sustainable RTW trajectory and optimize recovery.
The purpose of this study was to explore the perspectives of rehabilitation professionals intervening in long COVID rehabilitation with the goal of returning to work. The specific research questions were: (a) What are the treatments and interventions being used by rehabilitation professionals to help re-engage clients in their work? (b) What are the criteria currently being considered by rehabilitation professionals in deciding on whether or not a patient with long COVID is ready to go back to work? (c) How is progress of functional capacity in clients with long COVID monitored by rehabilitation professionals for return to work? (d) What are the challenges to rehabilitation and sustainable return to work in clients with long COVID from the perspectives of rehabilitation professionals? Personal experiences from various rehabilitation professionals will shed light on the treatments and interventions currently advancing rehabilitation, the challenges being faced, and the implications of reintegrating clients back to work. Such findings will allow practitioners to integrate the new knowledge into their everyday practice (Thompson Burdine et al., 2021).
Methods
Study Design
This is a cross-sectional qualitative study that uses the interpretive description (ID) methodology to gain an understanding of the perspectives of rehabilitation professionals intervening in long COVID RTW rehabilitation.
Initially introduced in the scope of nursing, ID is a qualitative non-categorical approach that allows to address limitations of a certain phenomenon while also accounting for individual variation. It examines emerging themes or patterns from subjective experiences (Thompson Burdine et al., 2021). Moreover, ID aims to address current gaps in clinical practice and further knowledge about a specific topic (Hunt, 2009; Thorne et al., 2004). Such concepts align with our study, as they allowed us to address the limitations currently faced by many healthcare practitioners with regard to long COVID rehabilitation, while also further examining the individual variations of among their clients. The authors referred to the Consolidated Criteria for Reporting Qualitative Research (COREQ) to report this study (Tong et al., 2007), and ethical approval was obtained from the CER-RDP.
Study Population
We recruited rehabilitation professionals in the province of Quebec who have specifically treated patients with long COVID. Specifically, the occupational therapy, physiotherapy, and kinesiology professions were chosen based on the likelihood of being involved in the rehabilitation care of individuals with long COVID and influencing their return to the workforce (WHO, 2023). The professionals came from multiple rehabilitation centers or private clinics in the province of Quebec. The inclusion criteria were the following: rehabilitation professionals working as physiotherapists, occupational therapists, and kinesiologists who have worked with the long COVID population within their clinical practice, either in-person or remotely. Individuals were excluded if they had not worked with the long COVID population or if they had worked with this population for less than three months. A purposive sampling strategy was used to gain a wide range of views from rehabilitation professionals working with this population. The authors contacted professionals whom they knew were working with such patients through email, and flyers were posted on various social media platforms. The sample size was intended to range between 8 and 12 participants and based on a study by Guest et al. (2006), which suggested that 6 to 12 interviews are typically sufficient to reach saturation in qualitative studies.
Data Collection
Demographics
For each participating rehabilitation professional (RP), we documented demographic data, such as sex, age, profession, location and sector of employment (region, public vs. private) and number of patients with long COVID they have seen thus far. We also collected information on participants’ years of experience in the profession, in their current workplace, as well as working with the long COVID population overall.
Semi-Structured Interviews
Semi-structured interviews were conducted with each participant individually. All interviews were conducted remotely using Zoom and were audio-recorded following written consent. The duration of the interviews varied between 28 min and 60 min (mean = 43 min). A total of 2 interviews were completed in English and 6 in French. A bilingual member of the research team conducted each interview and asked the core set of questions while two others (also bilingual) remained present and asked additional questions at the end of each interview, if deemed appropriate. These follow-up questions were tailored to the information given by each participant and thus could allow more in-depth information gathering on unique topics of each profession. One main interviewer per interview helped maintain consistency throughout interviews. The interviews were guided by a set questionnaire with both open- and close-ended questions for in-depth information gathering on the experiences of the participants with the long COVID clientele. The questions were guided by the research objective and specific research questions we aimed to answer in this study and were co-developed with the help of professionals from all three disciplines targeted for our study. The three occupational therapy master's students transcribed the interviews verbatim to either French or English.
Data Analysis
Inductive thematic analysis was used for this study. This type of data analysis is often used for ID studies as it allows for a more in-depth understanding of the phenomenon at hand while also creating nuances of the yielded data (Clarke et al., 2015; Thorne et al., 2004). It not only summarizes the data but also identifies relevant information regarding the research question and interprets key points (Clarke et al., 2015). We followed the six-step method proposed by Braun and Clarke (2006): Phase 1 involved getting familiarized with the data by transcribing and re-reading the transcripts to be able to identify themes, meaning, and patterns (Braun & Clarke, 2006). Phase 2 consisted of generating initial codes to organize the data in meaningful groups by using the Dedoose software to aid the analytic process (Braun & Clarke, 2006). Each author individually reviewed each transcript, and regular meetings were held to discuss emerging themes. Codes with a shared meaning were grouped, and discrepancies were addressed through dialogue and consensus. A codebook was developed to aid in the coding process and updated until no new codes were identified. Phase 3 focused on searching for themes based on the initial coding, by analyzing and sorting them (Braun & Clarke, 2006). This was done collaboratively by all authors. The bilingual investigators in this study translated the codes, themes, and quotes into English. Phases 4 and 5 focused on reviewing and analyzing the identified themes in more depth to define, refine, and name them, ensuring that they were related to the research question (Braun & Clarke, 2006). Lastly, phase 6 involved producing the final report by presenting the data in a clear and understandable way for the readers (Braun & Clarke, 2006).
Results
Characteristics of Participants
We recruited 12 eligible rehabilitation professionals. Three professionals had to cancel their interviews due to scheduling conflicts, one of which had already signed the consent form. We present data from interviews of 9 participants (8 females, 1 male), including five occupational therapists, three physiotherapists, and one kinesiologist. These 9 individuals were between 20 and 60 years of age. They averaged 14 years of experience in the profession, and about 1.7 years with the long COVID population. Among these participants, seven worked in the private sector and two worked in the public sector and were located across six different regions in the province.
Interviews
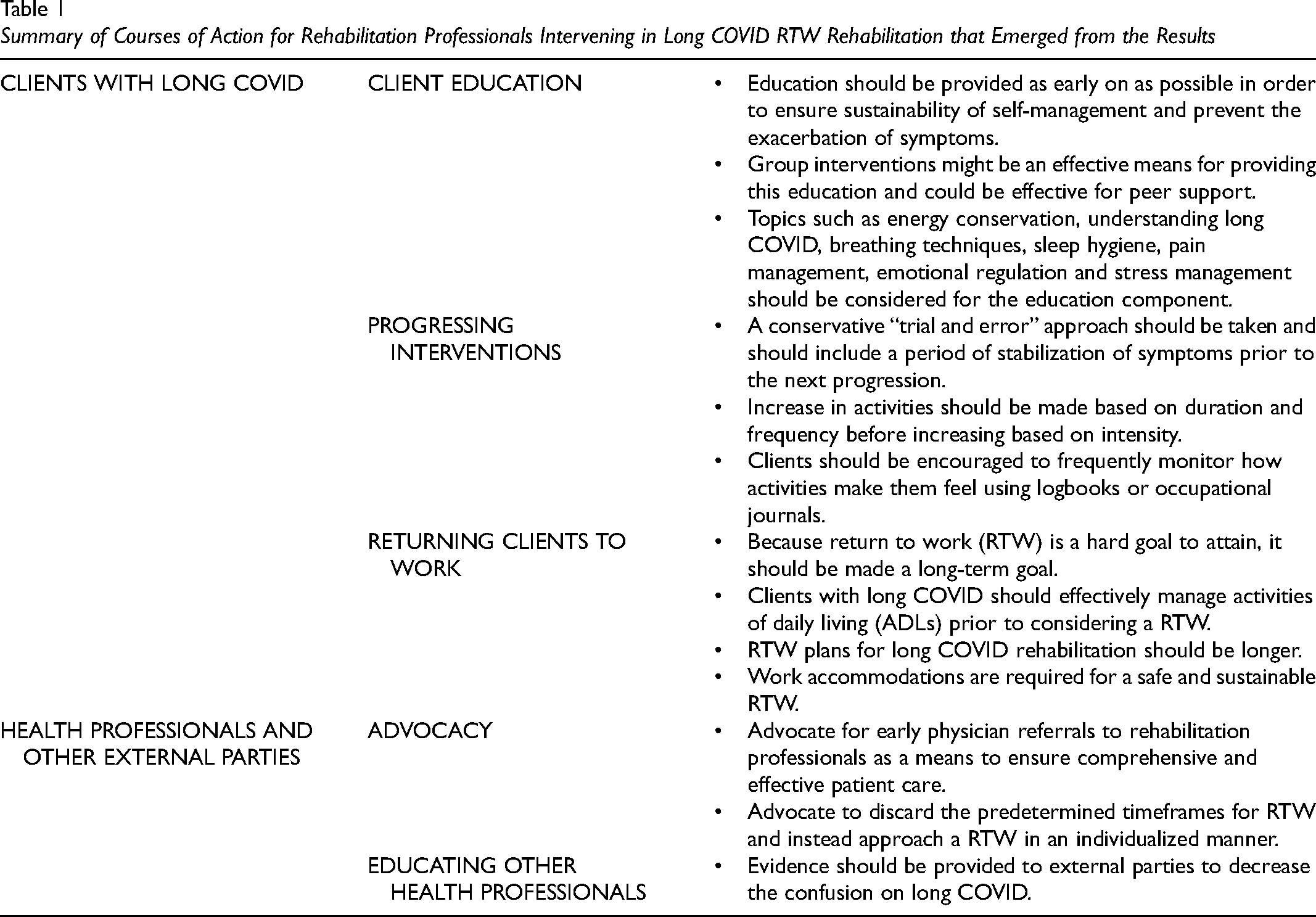
The data from the interviews generated five main themes: (a) reassessment of RTW goals; (b) education and self-management as primary interventions; (c) gradually reintegrating daily activities and life habits; (d) progression of interventions and dealing with PEM; and (e) challenges in long COVID rehabilitation. Key courses of action emerging from our study results for the clinical management of long COVID are highlighted in Table 1.
Summary of Courses of Action for Rehabilitation Professionals Intervening in Long COVID RTW Rehabilitation that Emerged from the Results
Reassessment of RTW Goals
Although all of our participants stated that RTW was a goal in their rehabilitation programs with their clients living with long COVID, a consensus among them was that it was rarely attainable. “Yes. Is it achieved all the time? No. They want it, but that’s what's hard because their daily lives are already difficult […] So yes, they have it as a goal, but we don’t make it a priority because they have to be able to do their laundry, make lunch and pick up their child from daycare before they can say, I’m going back to work.” (Rehabilitation professional (RP) #8). Indeed, it is often viewed as a long-term goal, with multiple preceding smaller goals. “In fact, all our patients, that’s their ultimate goal. But you know, it’s like stairs, and returning to work is at the top.” (RP #6) One participant mentioned: “[…] effectively, what we’re going to do is recommend a RTW only if the person is able to do a half-day of activity at home that simulates work tasks without causing post-exertion discomfort. Then, often, the most we’re able to achieve is 1 h or 1.5 h, so we never get to the point where I’m able to safely recommend a return to work.” (RP #6)
Moreover, many conveyed that facilitating a successful RTW necessitates appropriate accommodations. “I don’t know of any return to work that was considered without adaptations to the return to work.” (RP #1). More than half of the participants reported that from their clients who did RTW, which constitutes a very small percentage of their caseload, none were able to do so within 3 months. All in all, when comparing RTW rehabilitation with the long COVID clientele to other conditions, rehabilitation professionals are numerous to claim that it takes much longer. “Usually, I'll make return-to-work plans over 8 weeks for other clienteles, for example. With long COVID, I often go to 16.” (RP #5).
Education and Self-Management as Primary Interventions
Participating rehabilitation professionals talked about education on energy conservation, sleep hygiene, pain and stress management, emotional regulation, breathing techniques, day-to-day management, and understanding the condition and its symptoms as a central intervention, often provided in the initial stages of long COVID rehabilitation. A summary of the education pieces implemented by the rehabilitation professionals participating in this study can be found in Figure 1. Many rehabilitation professionals prefer to use a group intervention format to provide this education, as exemplified by RP #1: “It’s a way of optimizing our services […] in the group, you know, there’s support and guidance, reassurance, a lot of teaching.” The primary aim of providing this education early on is to ensure each individual is well-equipped to self-manage and self-monitor their condition and symptoms. “We work a lot from the perspective of self-regulation and self-management of one’s health condition, so we’ll be working on tools that will enable the person to understand his or her condition and develop a toolbox to help manage these signs and symptoms.” (RP #1). Indeed, clients are given complementary written or online documentation and materials they can access and refer to while applying them to their daily lives. This type of intervention draws from principles of cognitive-behavioral therapy (CBT) approaches, as highlighted by RP #1: “[…] when you teach, when you help a person to gradually re-expose themselves to their occupations, you are doing CBT.” Ultimately, when it comes to long COVID, clients are the experts of their condition, “The patient is the expert on his problem, he knows more about it than we do, so we're going to follow him/her.” (RP #9). Therefore, instead of prescribing specific exercises or interventions, which would be the norm with other conditions in the RTW context, rehabilitation professionals are more likely to take on a more supportive role during the process. Acceptance of their condition is vital for successful self-management and often needs to be addressed early in rehabilitation: “[…] there are a lot of acceptance challenges. You know, in the sense that often people will have the tools, they’ll know, they’ll understand, but it’s going to be difficult to implement the changes in everyday life.” (RP #1). Rehabilitation professionals discussed various ways clients are able to report back to them about their progress which helps guide further steps in the rehabilitation process: “We encourage them to use an occupational journal, […] to follow their symptoms, […] to use the Borg scale to follow their dyspnea, […] to measure their heart rate to also find out what’s the limit they can tolerate, and when it’s safe to add, maybe some more reactivation.” (RP #3). Many rehabilitation professionals work together in interdisciplinary teams or refer patients to other health care professionals so as to ensure they are adequately informed throughout the whole process, “The inter- or multidisciplinary approach is extremely important because long COVID is multi-systemic so it’s going to affect more than one sphere […] So, I think that all professionals, massage therapists, osteopaths, […] acupuncturists, physiotherapists, occupational therapists, nutritionists and psychologists would be the ones to prioritize.” (RP #4).
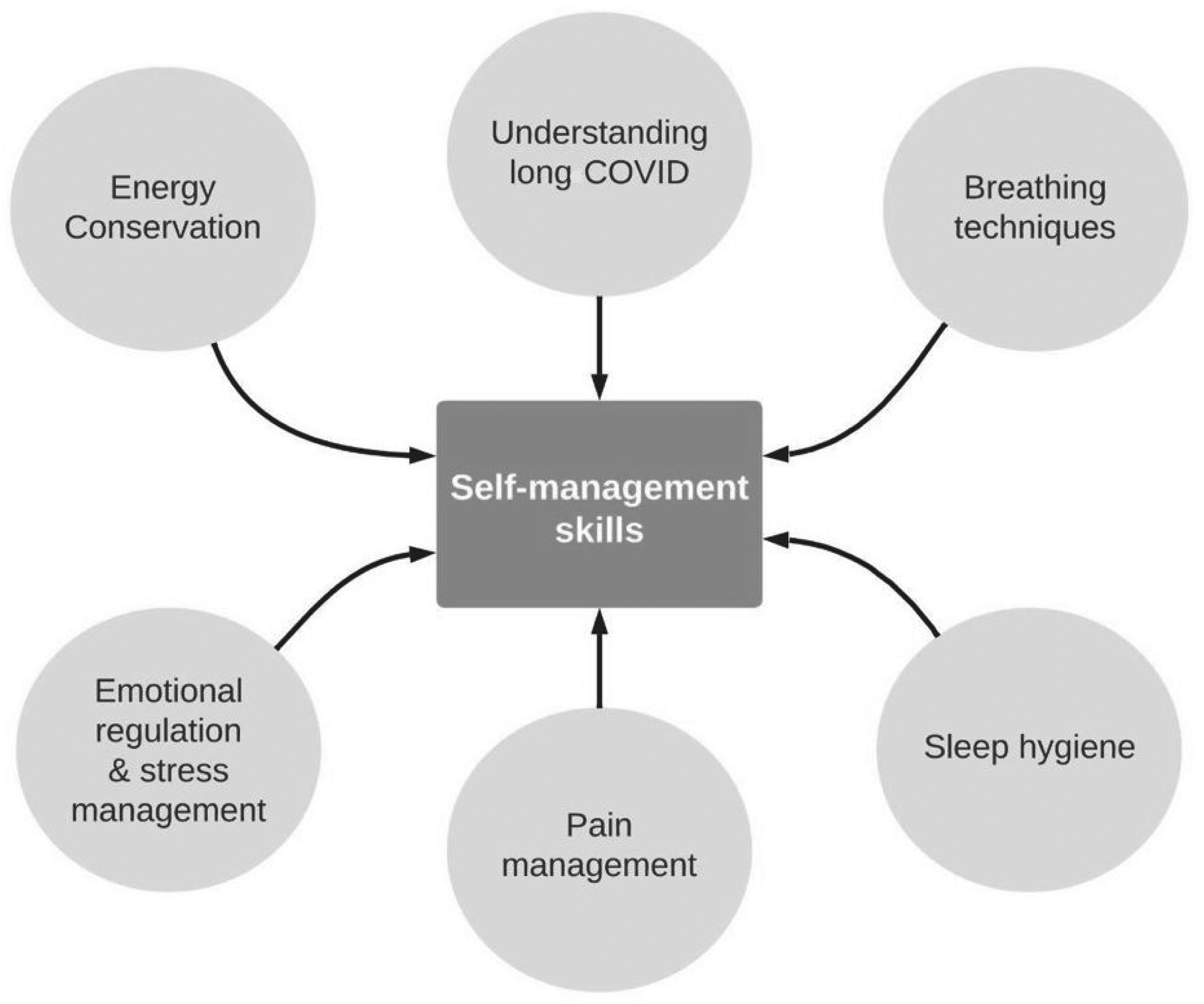
Education interventions implemented by rehabilitation professionals to promote self-management skills in patients with long COVID.
Gradually Reintegrating Daily Activities and Life Habits
Many rehabilitation professionals suggest that clients should engage in their regular daily activities, within safe limits, as a way to promote their reactivation. This in turn promotes their autonomy and optimizes functionality. Indeed, clients are told to gradually re-enter their daily activities, starting with basic activities of daily living (ADLs). Once these basic activities can be completed without exacerbating any symptoms, then the clients can move on to more complex tasks to eventually complete their daily activities independently and fulfil roles that are meaningful to them without worsening their condition. By the end of this process, the goal is to have the capacities required to return to their jobs. “When we’ve integrated quite a bit of ADL/iADLs [instrumental activities of daily living], we can now think more about work, and start doing simulations and strengthening tasks.” (RP #5). When talking about gradual activation to promote autonomy and function, most rehabilitation professionals continued to highlight the self-management role of each client. “We’re really talking about self-activation at their home, which I’m monitoring. So, the aim is for them to slowly increase their level of activation while, at the same time, monitoring the signs and symptoms they’ve learned about […] with an analytical capacity […] where we say, well OK, things didn’t go so well this week because of such-and-such-and-such. So, with their ability to analyze the activity, that leads us to the gradual integration in activities.” (RP #7). This requires a very individualized approach for each client, as highlighted by RP #3: “it’s all individualized. It’s really asking them what they’re doing right now, what they can tolerate.”
Progression of Interventions and Dealing With PEM
Progressing interventions and dealing with PEM go hand in hand when working with the long COVID population in that the presence or absence of a PEM can dictate whether or not progressing interventions is warranted. “Once the symptoms have stabilized, i.e., once there's a reduction in post-exertional malaise, and a faster recovery from post-exertional malaise, that's when we can make gradual progress.” (RP #4). Furthermore, many rehabilitation professionals mentioned that increasing exertion levels is done on a trial-and-error basis, by adding and removing activities on a day-to-day basis, and that it is best to wait between two and seven days after slightly increasing exertion levels or integrating a new activity prior to increasing further. “So I prefer to go really, really gradually in increasing the exercises and then really wait for a good week, for example, to see how it went. Then maybe we can think about increasing it again.” (RP #5). Rehabilitation professionals emphasize that when gradually increasing exertion levels, the focus should be on elevating duration and frequency before increasing intensity. “[…] to increase first the duration really just a few minutes more. Then, maybe the frequency, so doing it more often. And the intensity would be the last one.” (RP #3). Many added that gradual activation typically involves incorporating activities that are part of one's daily routine rather than focusing on specific isolated exercises. It is therefore important to acknowledge that this is done on a case-by-case basis, contingent on the capacities of the client and the activities they wish to reintegrate. When PEM does occur, rehabilitation professionals state that they work with clients to implement strategies to recognize these symptom exacerbations when they happen and identify the triggers and warning signs. This is primarily achieved through education, which can be supported by encouraging the client to keep a logbook or activity journal to constantly track how specific activities make them feel. “So we use a symptom journal. I’ll ask the client to fill in a symptom journal so that we can really keep track of what's going on, and so that they too can better understand what they’re feeling, and when they need to take action.” (RP #5).
Challenges in Long COVID Rehabilitation
Participants discussed challenges they have met in working with the long COVID clientele with the goal of returning to work and how they overcame them. The three main challenges identified can be summarized as follows: the recency of the condition and lack of clear recommendations for rehabilitating this clientele, the need to adapt standard rehabilitation protocols due to the complexity and variety of symptoms, and dealing with misinformed and uncooperative third parties, such as employers, insurance companies and even physicians. “There isn’t much documentation on long COVID […] it was especially difficult to know how […] to carry out our interventions with this population. We also had to get rid of the idea that you have to push yourself really hard to improve your capacities. […] You had to go much more gradually […]” (RP #5). “It’s a really hard concept to understand that they have to limit themselves and it’s not the usual typical rehab that you have to, like, have goals and do always more. You know, it's really less and trying to find the limit or whatever you can tolerate, it's hard for patients themselves […] We had some, we have some issues with medical team also, that, it's been better I would say in the last year, but we still have some doctors that don’t recommend the same thing.” (RP #3).
Mitigation strategies for these challenges were discussed and included the importance of staying up to date with new research and educating themselves on an ongoing basis, listening, guiding, and educating patients throughout the whole process, communicating with the interdisciplinary team, as well as providing documentation and information to third parties about long COVID, collaborating with them, and advocating for the needs of their clients. RP #5 stated: “A lot of “soft learning” too, reading the research, trying to talk to other therapists too who work with the long COVID population.” RP #8 added: “It’s to listen to our patient, more than with others where we’re going to be more interventionist. […] You have to listen to them, because they’re all alone. The family doesn’t understand them, the medical system doesn’t understand them, they don’t understand themselves, so they’re able to seek a little comfort, and that’s often where we make our difference.” When it comes to facilitating understanding in doctors, RP #4 stated: “With doctors, we try to do a lot of education, to send out informative pamphlets, […] I now allow myself to be a little more directive and less suggestive, and to back things up more with evidence and support.” RP #1 added: “We’ve got a lot of advocacy to do here, we’ve got to demonstrate why and explain why we’re doing this, and then try to influence the decisions that are made to facilitate the client's return-to-work.”
Discussion
In this qualitative study, we explored the perspectives of rehabilitation professionals intervening in long COVID rehabilitation with the goal of returning to work. We identified five main themes: (a) reassessment of RTW goals; (b) education and self-management as primary interventions; (c) gradually reintegrating daily activities and life habits; (d) progression of interventions and dealing with PEM; and (e) challenges in long COVID rehabilitation.
While the participants unanimously highlighted the significance of having a RTW goal in the rehabilitation programs of their patients with long COVID, this goal was rarely attained within the rehabilitation services of the professionals we interviewed. Professionals agreed that it should be regarded as a long-term goal rather than an immediate priority. Indeed, participants emphasized that a focus on incremental steps and smaller objectives aimed at promoting autonomy in daily activities should precede the RTW objective, resulting in longer rehabilitation periods. Hence, there is no specific or predictable recovery timeline for long COVID rehabilitation. While this is one of the key findings from this study, it aligns with previously published recommendations for RTW for people living with long COVID. In fact, in a guidance document by DeMars et al. (2022a), the authors highlight that the episodic and unpredictable nature of long COVID leads to an extended non-linear RTW trajectory. Recommendations in the guide also included the need for reasonable work accommodations, modified tasks, reduced work hours, more breaks, and even the possibility of remote work. However, depending on each individual's pre-illness employment, these may not always be possible.
Moreover, as per the guidelines by the Alberta Health Services (2022), rehabilitation professionals must first consider if patients are managing their home life within the constraints of their available energy resources before considering RTW. This was also a consistent opinion among participants we interviewed and is further substantiated by our identified themes. Progressing activities and tasks at home, both in frequency and in duration, is seen as an important indicator for the readiness of someone to safely re-enter the workforce. Patients are required to be very self-directed when progressing their domestic responsibilities. This requires a certain degree of acceptance of their condition and limitations and self-awareness of their symptoms.
The interventions highlighted by the rehabilitation professionals working with the long COVID population were similar across interviews. Among these interventions, education was by far mentioned the most. This education includes understanding the condition and its symptoms, identifying triggers, and developing self-management skills early on to avoid consistently over-exerting oneself and worsening symptoms over time, particularly concerning PEM.
As expected, dealing with PEM was of great concern to rehabilitation professionals due to its unpredictability and lack of knowledge surrounding the symptoms. Existing guidelines on the clinical management of long COVID recommend avoiding the prescription of exercise or activities with fixed increments if the patient is experiencing PEM (Alberta Health Services, 2022; WHO, 2023). Only after a period of sustained symptom stabilization should the RP consider modifying or increasing activity levels (WHO, 2023). While this was consistent across our findings, the duration of this period remains unclear and may differ based on several factors, namely the number of permitted therapy sessions or weeks of rehabilitation. Interestingly, we discovered that many rehabilitation professionals decided to opt for a conservative approach. Once more, the unpredictability of the condition and its uniqueness to each patient makes it difficult to gauge if even a slight increase in activities will cause a PEM. RP thus described their approach as trial and error. Given the risks of increasing exertional levels too quickly, particularly with trial and error, rehabilitation professionals implement journaling and logbooks to help the patients track their symptoms. This allows both the rehabilitation professionals and the patients to frequently monitor their symptoms, as well as identify their limits and tolerable activities.
Several professionals agreed that a notable challenge faced during rehabilitation of the long COVID population was in fact the involvement of external parties, such as Commission des normes, de l’équité, de la santé et de la sécurité au travail (CNESST) agents and physicians. CNESST agents are accustomed to predetermined RTW timelines according to the diagnosis and are held responsible for ensuring RTW within certain timeframes. Thus, they often overlook the individualized nature of this condition. This warrants frequent discussions between agents and rehabilitation professionals, where the latter find themselves having to support their RTW plans with literature. Moreover, the lack of understanding of long COVID among other healthcare professionals, such as physicians, was named as an additional challenge by rehabilitation professionals as it impacts their ability to effectively carry out their rehabilitation efforts.
Our results are consistent with findings in other studies that have shown that rehabilitation professionals have often needed to independently seek resources to support their requests for referrals. It also sheds light on the insufficient long COVID patient referrals to rehabilitation (Ladds et al., 2020; Seang et al., 2022). This highlights the need for advocating for early physician referrals to rehabilitation professionals as a means to ensure comprehensive and effective patient care, as suggested by the participants in our study. The deficiency of referrals and comprehension of other parties ties into the bigger challenge of understanding long COVID as a distinct condition, which is further compounded by its recent nature.
This study included in-depth interviews with a diverse group of 9 rehabilitation professionals working in various rehabilitation centres and clinics in the province of Quebec. Because of this small sample size and the fact this study only offered a portrait of long COVID rehabilitation within the Quebec context, our findings might not be generalizable to a broader population of rehabilitation professionals. However, this is generally not expected of a qualitative study (Leung, 2015). We also experienced difficulties recruiting rehabilitation professionals in the public sector due to institutional regulations in regard to recruitment in those centres. While we initially desired to interview 12 individuals, we believe we reached saturation of data given the consistency of perspectives that emerged among participants. The inclusion of three disciplines with differing practices in our study did not appear to impact achieving data saturation. In spite of the aforementioned limitations, this study enhances the understanding of long COVID rehabilitation with the goal of returning to work, offering insights that could guide clinicians and help steer future research.
Conclusion
Although long COVID rehabilitation is not clear cut, the findings from our interviews provide valuable insights into the rehabilitation strategies employed by professionals working with the long COVID clientele with a focus on RTW. While early education, gradual activation, and client self-management emerge as central components in the rehabilitation trajectory for long COVID, the findings highlight that RTW remains a challenging goal to attain without proper accommodations and individualized support. Future research and collaboration among healthcare stakeholders will continue to shape the evolving landscape of long COVID rehabilitation.
Key Messages
Rehabilitation practices for long COVID with the goal of returning to work seem to revolve around:
Adopting an individualized approach due to the complex symptomatology and diverse range of environmental factors at play. Providing early education in order to ensure the sustainability of self-management and prevent the exacerbation of symptoms. Ensuring long COVID patients can effectively manage activities of daily living (ADLs) prior to considering a return to work.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174241312510 - Supplemental material for Perspectives of Rehabilitation Professionals on Long COVID Interventions to Facilitate Return-to-Work
Supplemental material, sj-docx-1-cjo-10.1177_00084174241312510 for Perspectives of Rehabilitation Professionals on Long COVID Interventions to Facilitate Return-to-Work by Cassandra MacKinnon, Cassandra Castro-Barquero, Alexandra Kontis, Vanessa Patrice, Mayoore Nadarajah and Tania Janaudis-Ferreira in Canadian Journal of Occupational Therapy
Supplemental Material
sj-docx-2-cjo-10.1177_00084174241312510 - Supplemental material for Perspectives of Rehabilitation Professionals on Long COVID Interventions to Facilitate Return-to-Work
Supplemental material, sj-docx-2-cjo-10.1177_00084174241312510 for Perspectives of Rehabilitation Professionals on Long COVID Interventions to Facilitate Return-to-Work by Cassandra MacKinnon, Cassandra Castro-Barquero, Alexandra Kontis, Vanessa Patrice, Mayoore Nadarajah and Tania Janaudis-Ferreira in Canadian Journal of Occupational Therapy
Footnotes
Acknowledgments
The authors thank the rehabilitation professionals who participated in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.