
Abstract
Serious mental illness, such as schizophrenia, bipolar disorder, and schizoaffective disorder, often results in consequences such as a deteriorated quality of life, an impoverished everyday life with few meaningful activities, reduced work capacity, risks of cardiovascular problems, and increased mortality. Thus, a serious mental illness is noted to have significant repercussions in numerous areas of life functioning including independent living, employment, and interpersonal skills (McCormick et al., 2022).
Well-being is associated with their every occupation, particularly how individuals perceive the meaning, values, and satisfaction linked with those occupations (Eklund et al., 2017). People with a diagnosis of severe mental illness often show difficulties in engaging in different occupations, such as work, leisure, and personal care, affecting their occupational balance (Backman, 2004). Different authors have suggested the need and the interest to study in-depth the occupational balance in people with serious mental illness. The balance between the different occupations that compose people's daily lives, that is, work, personal care, rest, leisure, and play, has been considered vital since occupational therapy was founded (Backman, 2004; Eklund & Argentzell, 2016).
The use of time in a harmonious and rhythmic way is a core concept underlying the theory and practice of occupational therapy, an important concept since the beginning of the profession (Meyer, 1977): “The whole of human organization has its shape in a kind of rhythm. (…) the big four – work and play and rest and sleep, which our organism must be able to balance even under difficulty” (p. 641). Nowadays, occupational balance might be defined as “the individual's perception of having the right amount of occupations and the right variation between occupations” (Wagman et al., 2012). There are previous studies which showed that being under-occupied is a problem for individuals with serious mental illness people and that they could better control their anger when they showed occupational balance and they felt competent (Leufstadius et al., 2009).
Promoting participation and social inclusion is one of the challenges in mental health rehabilitation and it is a fundamental part of occupational therapy. The lack of participation in social activities in people with severe mental illness has been linked to a deficit in social cognition, especially in the processing of emotions, perception, recognition, and regulation of emotions. This deficit in social cognition makes it difficult to understand social situations and predict the behaviour and intentions of other people (Barrios et al., 2018). These difficulties persist after clinical remission in more than half of the people with mental health illness (Pinna et al., 2013). Thus, emotional regulation could be related to participation in different social activities. In this sense, emotional regulation refers to the ability to control and show emotions according to each situation, being able to initiate, and maintain an emotional state, based on one's own and others’ emotions, facilitating social adaptation and social functioning, controlling negative emotions, and focusing on pleasurable ones (Mayer et al., 2008). There are two main types of strategies for emotional regulation: (1) cognitive reappraisal and (2) expressive suppression (Gross & John, 2003). Cognitive reappraisal can be defined as the mental change that occurs prior to the generation of the emotion and that consequently modifies its emotional impact on the situation (e.g., when we receive news that disappoints us or that we did not expect, new arguments are contemplated that allow us to approach the situation in a different way). On the other hand, expressive suppression involves inhibiting the expression of emotions after the emotional response has been generated (e.g., when someone tells us news we don’t like, keeping a poker face even when we feel very sad or angry) (Gross & John, 2003). Despite the relevance of emotional regulation in people with severe mental illness and the decrease in self-care, work, and social participation activities, to date, to the best of the authors’ knowledge, they have not been found studies that relate occupational balance and emotional regulation in people with severe mental illness or healthy people.
The aim of this study was to analyze perceptions of occupational balance and emotional regulation in people with serious mental illness compared to the healthy population. Additionally, this study aimed to find out if emotional regulation can be related to occupational balance in people with serious mental illness. Based on the current status quo of the literature, we hypothesized that: (1) people with severe mental illness will report lower occupational balance and emotional self-regulation than the healthy population, (2) people who show greater occupational balance will show better emotional self-regulation, with greater cognitive reappraisal and expressive suppression; (3) age and gender moderate the relationship between occupational balance and emotional self-regulation, such that younger age and female gender are associated with better occupational balance, less expressive suppression and greater use of cognitive reappraisal. Understanding the relationship between occupational balance and emotional self-regulation might help to establish appropriate intervention strategies in mental health programs.
Method
Study Design
An observational cross-sectional study was performed. The study is reported using EQUATOR network recommendations for observational studies (STROBE, STrengthening the Reporting of OBservational studies in Epidemiology) (Vandenbroucke et al., 2014). Ethics approval was obtained from the relevant University Human Research Ethics Committee and was conducted following the last version of the Helsinki Declaration. All participants agreed to participate and gave their informed consent before completing the questionnaires.
Participants
Two occupational therapists recruited all participants using convenience sampling (Hernández et al., 2010). People with mental illness were recruited from two public community mental health centers and healthy people through advertisements at a university in Spain. All participants had to be between 18 and 65 years old and all subjects participated voluntarily. Prior to inclusion, participants were asked to fill in a health questionnaire to verify that they did not suffer from any other illness. The eligibility criteria for the serious mental illness group were as follows: being an adult patient, who is diagnosed with mental illness using the DSM-5 criteria; and skills to read and write independently. People with mental illness who were illiterate or had any chronic comorbid physical or neurological disease (e.g., cardiopulmonary disease, lupus) were excluded from the study. In addition, everyone had to have the ability to write and read independently. In each centre, the occupational therapist informed the participants about the aims of the study, the methodology, its duration, that their participation was voluntary, as well as the possibility of leaving the study at any time if they so wished and without any explanation. It was explained to them that their participation did not affect their treatment in any way and the study was independent of it. Once this information was received, people with mental illness decided whether they wanted to participate or not. Those people who gave written informed consent were contacted by the research team to have an appointment for the study. In the case of the healthy sample, they were initially recruited by advertisements at the university indicating that if they were interested in participating, they should contact the main researcher by email. Once the informed consent was signed, the questionnaires were completed.
Data Collection
The evaluation was performed in one session, lasting 1 h. The answers of the included participants were collected in writing on an electronic form developed for this study. The questionnaire was self-administered. In the case of the people with mental illness, a 4th-grade Occupational Therapy student trained in the administration of both questionnaires performed the evaluation and supervised the process while they completed it. None of the participants had received financial incentive for participating in the study. A total of two patient-reported outcome measures were completed by the participants to register occupational balance and emotional regulation. Gender and profession were collected using a survey. Other demographic data collected was age, because of its importance in the incorporation into the labour market, in turn related to economic independence and emancipation, aspects that could have a significant impact on the occupational balance in adulthood (Carpenter et al., 2020; Klodnick et al., 2014). Considering that in the European Union, in 2020, the average age of young people leaving the parental household was 26.5 years (EUROSTAT, 2020), age was dichotomized into two categories (18–27 years; ≥ 28 years).
Occupational Balance Questionnaire
Occupational balance was measured with the Spanish version of the Occupational Balance Questionnaire (OBQ-E) (Peral-Gómez et al., 2022). This has been described as an adequate questionnaire to register occupational balance in the Spanish population. This questionnaire focuses on a person's experience of her /his amount and variation of occupations in everyday life (Wagman et al., 2021). It consists of 13 questions measured on a six-point Likert scale from 0 “strongly disagree” to 5 “strongly agree.” The rating of the instrument can be assessed at the level of the individual item or as a summed total score (ranging between 0 and 65; the higher score, the better occupational balance). OBQ-E has good internal consistency with a Cronbach's alpha value of 0.87 (Peral-Gómez et al., 2022).
Emotion Regulation Questionnaire
Emotional regulation was assessed with the Spanish version of the Emotion Regulation Questionnaire (ERQ) (Marco et al., 2021). It is a 10-item measure with two subscales evaluating the perception of the use of cognitive reappraisal (six items) and expressive suppression (four items) to regulate emotions. These two factors have been shown to operate independently of each other. Items are rated on a 7-point Likert-type response scale from 1 “strongly disagree” to 7 “strongly agree.” An example of items from the cognitive reappraisal and expressive suppression subscale respectively are: “When I’m faced with a stressful situation, I make myself think about it in a way that helps me stay calm,” and “I control my emotions by not expressing them.” Higher scores on each scale indicate greater use of the corresponding emotional regulation strategy. The reliability of the scale was good, with a Cronbach's alpha value of 0.93.
Data Analysis
Sociodemographic characteristics (gender, range of age, and educational level) were described using absolute and percentage values. To detect the differences between the two groups (serious mental illness group and healthy group) in the distribution of gender, age-range and educational level, it was performed Pearson's χ2 test or Fisher's exact test when the expected values in any of the cells of the contingency table were below five (Sánchez Villegas et al., 2006).
Normal distribution was checked for occupational balance, emotional regulation, cognitive reappraisal, and expressive suppression using the Kolmogorov–Smirnov test. As these variables followed a non-normal distribution (Kolmogorov–Smirnov's test p-value < .05), median and interquartile range (IQR) were used for their description. According to the number of items in the ERQ and the sample size of this study, the internal consistency of the scale can be considered moderate for a Cronbach's alpha value > 0.75, good if > 0.80, and excellent if > 0.85. In the case of the OBQ-E, given that it has 13 items, and the sample size, the internal consistency can be considered moderate for a Cronbach's alpha value > 0.80, good if > 0.85 and excellent if > 0.90 (Ponterotto & Ruckdeschel, 2007). To analyze the differences in occupational balance, emotional regulation, cognitive reappraisal, and expressive suppression between the two groups, the Mann–Whitney U-Test was used. To know the differences between groups in percentages of answers for each item of the OBQ-E, Pearson's χ2 test or Fisher’s exact test was conducted when the expected values in any of the cells of the contingency table were below five (Sánchez Villegas et al., 2006).
The analysis of the association between two categorical variables was conducted using Spearman's correlation coefficient. An analysis of covariance (ANCOVA) with OBQ-E was conducted, including those variables that showed a significant correlation controlling for age, gender, educational level, and group. Statistical significance was set at p < .05. The analysis was performed with IBM Statistical Package for Social Sciences software (IBM Corp. Published 2012. IBM SPSS Statistics for Windows, Version 28.0 Armonk, NY).
Results
A total of 65 people with serious mental illness from the Vocational Rehabilitation Centre were invited to participate, of whom 22 service users agreed to participate. Of the 95 patients from the psychosocial rehabilitation center, a total of 37 volunteered/consented to participate, of which four were ineligible due to exclusion criteria (two of them had obesity and hypertension, one patient had heart disease, and another patient had psoriasis and uncontrolled thyroid disease), leaving a total of 33 participants from this setting. The 55 patients were in clinical follow-up and with pharmacological treatment. Regarding the healthy group, it was composed of 57 people (Table 1).
Characteristic of the Participants Included in the Study (n = 112)
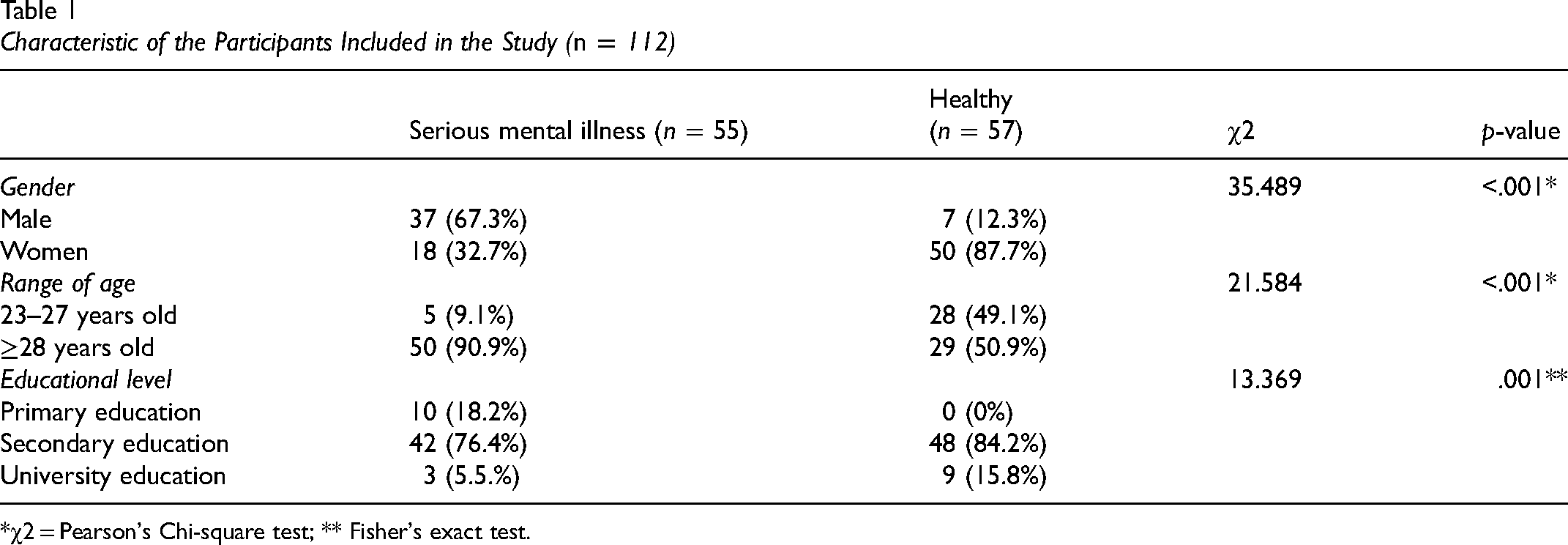
*χ2 = Pearson's Chi-square test; ** Fisher's exact test.
The reliability of ERQ was good, with a Cronbach's alpha value of 0.82, and for the OBQ-E it was excellent, with a Cronbach's alpha value of 0.92. There were statistically significant differences between the two groups in age (χ2 = 21.584; df = 1; p < .001), gender (χ2 = 35.489; df = 1; p < .001), and educational level (χ2 = 13.369; df = 1; p = .001) (Table 1).
Non-normal distribution was followed by occupational balance (Kolmogorov–Smirnov test = 0.084 df = 112; p = .048), emotional regulation (Kolmogorov–Smirnov test = 0.153 df = 112; p < .001), cognitive reappraisal (Kolmogorov–Smirnov test = 0.091 df = 112; p = .023), and expressive suppression (Kolmogorov–Smirnov test = 0.121 df = 112; p < .001). The healthy group showed statistically significant higher scores in occupational balance (Mann–Whitney U-test = 1132.5; p = .011), and in cognitive reappraisal (Mann–Whitney U-test = 867; p < .001), and as well as a slightly significant lower score in expressive suppression (Mann–Whitney U-test = 1240.5; p = .057) (Table 2).
Differences in Occupational Balance and Emotional Regulation by Groups
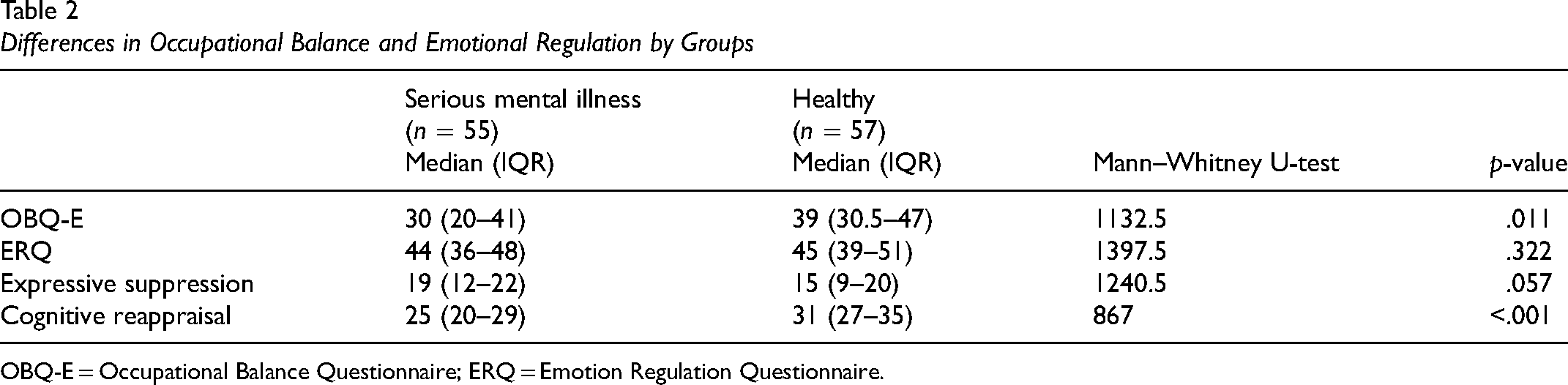
OBQ-E = Occupational Balance Questionnaire; ERQ = Emotion Regulation Questionnaire.
When analyzing the answers between the comparison groups for each item of the OBQ-E, differences were observed in three of them. Serious mental illness group, compared to healthy group, perceived that they had fewer meaningful occupations (Fisher's exact test = 17.279; df = 5; p = .004), a lower balance between doing things alone/with others (Fisher's exact test = 13.504; df = 5; p = .019), and a greater disagreement with having enough to do during a regular week (Fisher`s exact test = 28.120; df = 5; p < .001) (Table 3).
Differences in Occupational Balance (OBQ-E) Between Healthy and Serious Mental Illness
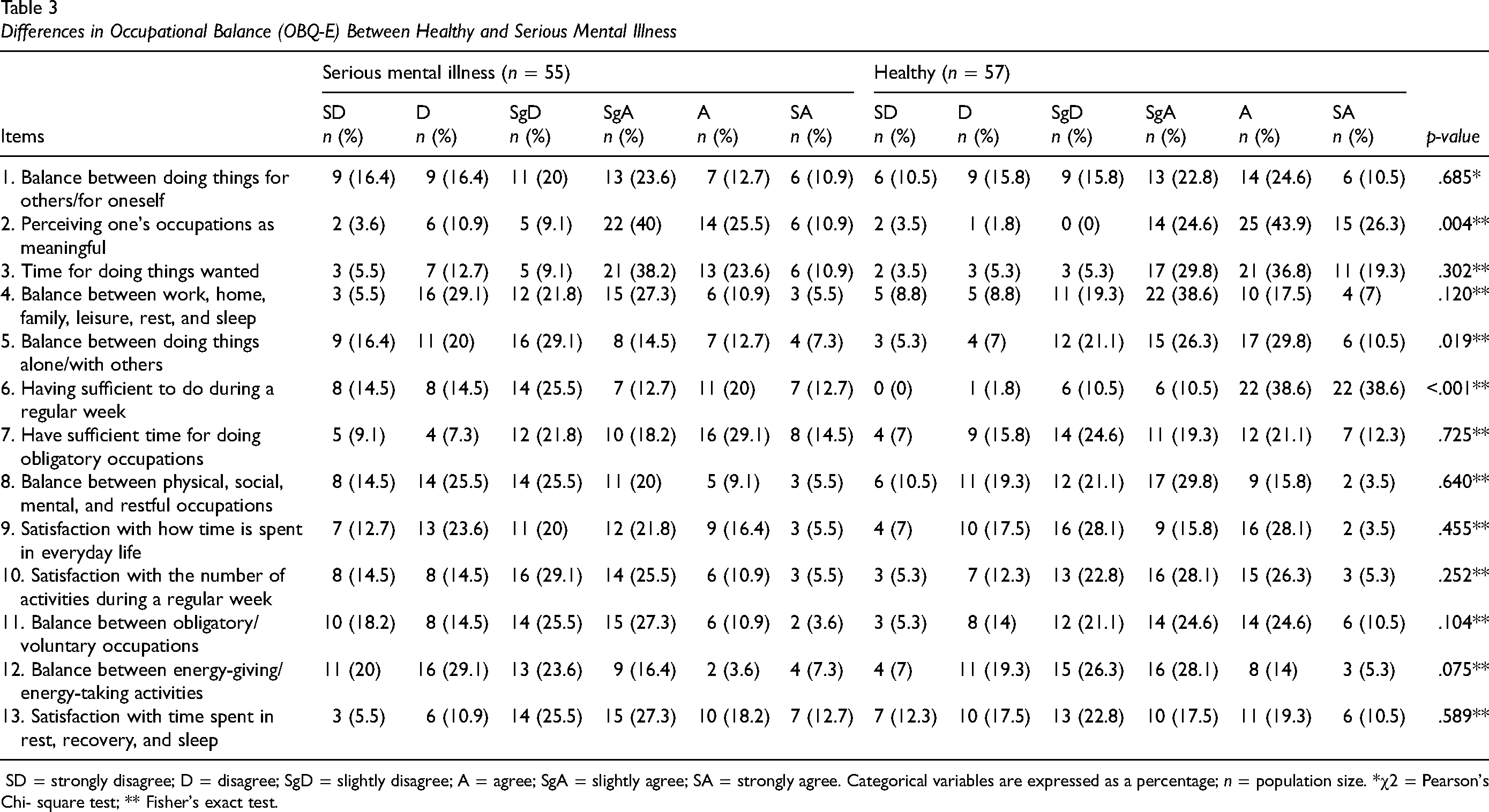
SD = strongly disagree; D = disagree; SgD = slightly disagree; A = agree; SgA = slightly agree; SA = strongly agree. Categorical variables are expressed as a percentage; n = population size. *χ2 = Pearson's Chi- square test; ** Fisher's exact test.
Regarding the correlation analyses, occupational balance showed a statistically significant positive relationship with cognitive reappraisal (rs = .365; p < .001) and a negative relationship with expressive suppression (rs = −.332; p < .001) (Table 4).
Correlations Between Occupational Balance and Emotional Regulation
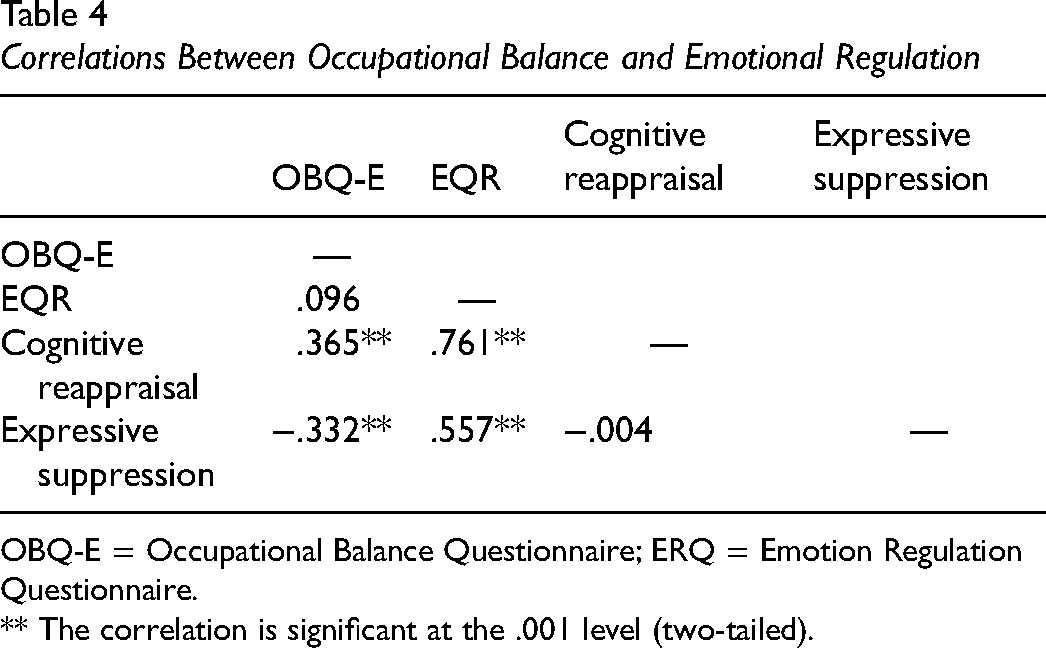
OBQ-E = Occupational Balance Questionnaire; ERQ = Emotion Regulation Questionnaire.
** The correlation is significant at the .001 level (two-tailed).
After controlling for age, gender, educational level, and group, the results of the ANCOVA showed that, for every one-point increase in expressive suppression, the total OBQ-E score decreases by an average of 0.70 points (p < .001); and for every one-point increase in cognitive reappraisal, the total OBQ-E increases by an average of 0.47 points (p = .002) (Table 5).
Multivariate Model (ANCOVA) of Occupational Balance Adjusted for Age, Gender, Cognitive Reappraisal, and Expressive Suppression
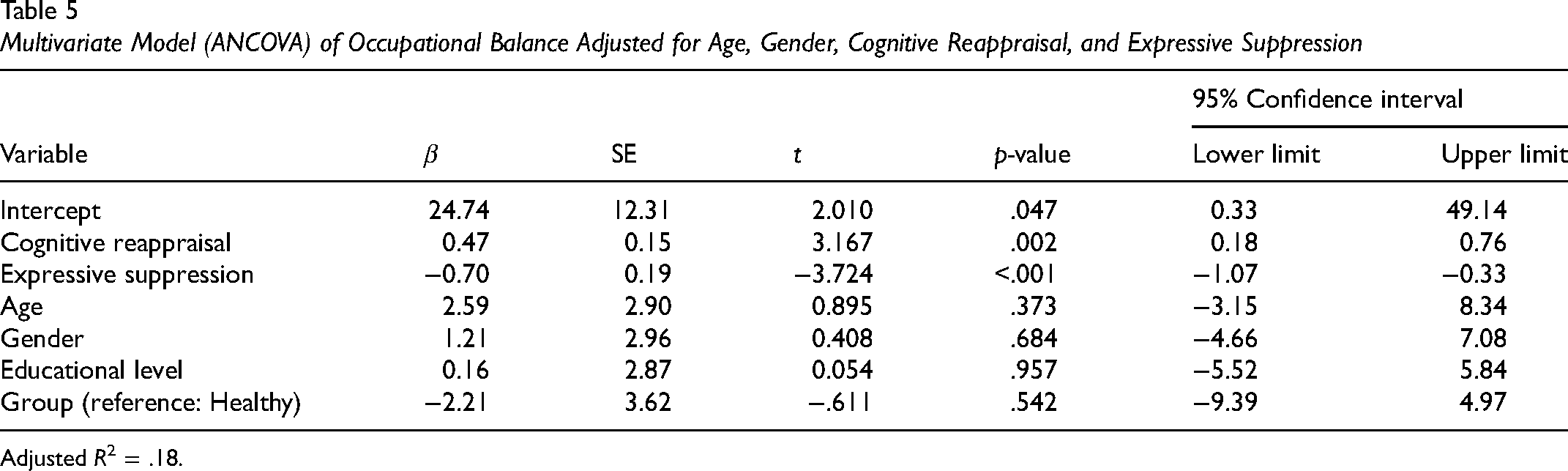
Adjusted R2 = .18.
Discussion
Differences in Occupational Balance
The first aim of this study was to analyze the perceptions of occupational balance in people with serious mental illness and to study if there were differences by group. The results of our study support our first hypothesis, which states that people with serious mental illness reported lower occupational balance than the healthy population. The cut-off points set for the OBQ-E for the general population (Peral-Gómez et al., 2022) are also consistent with these results. Previous studies have shown that lack of occupation is a problem for people with mental illness (Bejerholm & Björkman, 2011) which may have an impact on their quality of life (Wagman et al., 2021). In addition, these results could be related to the findings of other studies that showed occupational engagement facilitates the reduction of negative symptoms in people with serious mental illness (Bejerholm & Björkman, 2011) and it has even been found that participation in social activities helps in reducing delusions (Myin-Germeys et al., 2001).
Our findings showed that people with severe mental illness perceived their occupations as less meaningful. These findings support previous literature showing that this population is characterized by low participation in significant occupations and maintains low occupational engagement (Bejerholm & Björkman, 2011). Similar results have been reported in other studies, showing that people with schizophrenia participated in significantly fewer activities than healthy people (Lipskaya-Velikovsky et al., 2015) and with impoverished daily life with few meaningful occupations and a sedentary style (Eklund et al., 2017). Also, other authors with the Spanish population showed differences in occupational satisfaction when comparing people with mental illness and the healthy population using another useful instrument to assess occupational balance and satisfaction with occupations (SDO-OB) (Vidaña-Moya et al., 2020). In community mental health intervention programs, beyond the distribution of time in self-care, work, leisure, rest, etc., it has been suggested that a broader perspective, of temporal adaptation, should be taken (Kielhofner, 2007) emphasizing one's qualitative perspective about the relevance of one's occupations (Crist et al., 2000). This point of view is consistent with the results obtained by a previous study in which the healthy group showed greater enjoyment, competence, and relevance from occupations than people who had mental health problems. Furthermore, the healthy group became more aware of the relevance of play/leisure and its relationship with their well-being (Crist et al., 2000). Moreover, other studies have shown a relationship between occupational balance and emotional well-being (Eklund & Argentzell, 2016). Consistent with our findings, people with severe mental illness reported having lower occupational balance. Considering the results of the previous authors, occupational therapy interventions that promote occupational balance and awareness of it, could help generate greater well-being in people with serious mental illness. Furthermore, it has been suggested that one of the most important challenges for occupational therapists is to understand the meaning that activities have for the client and their impact on the reconstruction of their occupational identity, through engagement in different occupations (Crist et al., 2000). Other authors have mentioned that this important task should start by helping people with mental illness understand their participation in occupations in a harmonious way (Eklund & Argentzell, 2016) fostering their sense of competence, belonging, enjoyment and autonomy (Crist et al., 2000). In this sense, it has been described that people with severe mental illness tend to consider meaningful activities those activities that are pleasant and allow them to enjoy and to be in connection and interact with other people and their environment, productive activities that lead to the development of a sense of competence, activities that allow them to have routines and develop projects as well as activities involved with personal and health care.
On the other hand, our findings showed statistically significant differences for “the balance between doing things alone with others.” It has been indicated that people with mental illness are characterized by being under-occupied, which affects their recovery and well-being (Eklund & Argentzell, 2016). It has been pointed out that there is a cultural and gender pattern in the occupational balance, in such a way that people who have children perceive that they perform a higher number of activities in their daily life, such as occurs with women who assume more responsibilities in raising children and in household chores. This pattern could be related to less participation in work and leisure activities, where spaces are shared and where they interact with other people (Eklund & Argentzell, 2016). These differences are greater in the population with mental illness, in which a lower socio-labour integration has been reported, associated with the stigma of mental illness and the difficulty for employers to understand it. Likewise, the lack of balance between doing things alone or with others may be related to the well-being perceived by some patients with mental illness when doing things alone, such as walking (Jivanjee et al., 2008).
Moreover, our results showed that the serious mental illness group, in comparison to the healthy group, reported a greater disagreement with “having sufficient to do during a regular week,” that is, they perceived to be under-occupied, been these differences statistically significant. The under-occupation or lack of occupation is another key element in the occupational balance in people with mental illness that coincides with the findings of a previous research (Eklund & Argentzell, 2016). It is interesting to mention that when it has been compared over-occupied versus under-occupied users, the occupational balance is greater in the last. This has been explained because, in the case of people with serious mental illness, the mere fact of having a job does not mean having more occupational balance if the job is not flexible enough to adapt to the evolution of their disease (Eklund & Argentzell, 2016). Our research is consistent with other author's results, which suggest that people with severe mental illness should be encouraged to find a balance between occupations and rest (Eklund & Sandlund, 2014) even if they do not have a job, providing opportunities to be active and break the pattern of being under-occupied (Eklund & Argentzell, 2016).
Differences in Expressive Suppression and Cognitive Reappraisal
Our first aim also included analyzing the perceptions about emotional regulation in people with serious mental illness and studying if there were differences when compared with the healthy group. Related to emotional regulation in people with serious mental illness, one of the key symptoms is reduced emotional experience, understood as emotional withdrawal, passive social withdrawal, active social avoidance, or social withdrawal (Al-Halabí et al., 2016; Silberstein et al., 2018). In the serious mental illness group, compared to the healthy group, we found a statistically significant lower cognitive reappraisal and a higher expressive suppression, although in this case the difference was marginally significant. Poor emotional awareness can lead to difficulties in identifying and describing feelings, with fewer social contacts (Kimhy et al. 2012). In people with mental illness, it has been observed that they use emotional suppression to a greater extent, related to poor social functioning, compared to cognitive reappraisal, which allows modifying the way in which they think about a certain event to alter its emotional impact and it is more related to a positive emotion and general feelings of well-being.
Relationship Between Occupational Balance and Emotional Regulation
The second hypothesis of our research was that people with greater occupational balance would show better emotional self-regulation, with greater cognitive reappraisal and expressive suppression. In this sense, this study partially confirms it. Our findings showed that the higher cognitive reappraisal, the higher occupational balance, and the higher expressive suppression, the lower occupational balance. According to Kimhy et al. (Kimhy et al., 2012), less suppression and a greater cognitive reappraisal have been associated with better social functioning in people with serious mental illness. Other studies have shown that people with mental illness who use suppression as an emotional regulation strategy, showed greater negative emotions, a reduction in positive emotions, a decrease in social interaction in their daily life (Moran & Kring, 2018) and fewer prosocial activities (Lopes et al., 2005). Likewise, it has been indicated that greater use of suppression is associated with poorer social functioning, lower quality of friendships, lower interpersonal sensitivity, fewer prosocial activities, and more social conflict in young adults (Kimhy et al., 2012).
Our findings could have implications for the clinical practice. The assessment of occupational balance in people with serious mental illness could help occupational therapists to optimize the design of therapeutic approaches for this population. Occupational Therapy intervention in patients with serious mental illness should give opportunities for these people to get involved and engage in occupations that are meaningful. On the other hand, implementing programs that include meaningful occupations and that allow these people to improve their cognitive reappraisal, could improve their occupational balance. Negative emotions can trigger psychotic symptoms, which makes it even more relevant for them to learn effective regulation strategies (Grezellschak et al., 2015). In addition, it has been found that people with schizophrenia can modulate their emotional regulation following explicit instructions (Moran & Kring, 2018). The development of emotional skills in outpatients could be crucial for their recovery since it has been observed that the improving of social cognition, such as empathy and emotional understanding skills are good predictors of treatment success (Rus-Calafell et al., 2013). In addition, the results suggest that it could be relevant to promote occupational balance and involvement in social occupations that encourage these patients to relate to others and their environment. It may be of interest to consider the most important social occupations for each person (i.e., team sports, dance), extending participation beyond the therapeutic intervention, such as weekends. In addition, incorporating interventions aimed to improve time management to avoid, for example, procrastination, excess or deficiency of some type of specific occupation, could allow the gradual development of a viable, regular and sustainable occupational pattern, and help prepare for discharge (Holmefur et al., 2019, 2021).
Limitations
Our study has several limitations. First, the selection of patients was conducted by means of a non-probabilistic convenience sampling. This might limit the extrapolation of the results, although the usefulness of this method has been demonstrated in exploratory studies like ours (Hernández et al. 2010). Second, there is a small number of participants. Therefore, it would be advisable to design new studies that include a greater number of participants. Third, the type of cross-sectional design does not provide knowledge about causality. It would be of interest to conduct longitudinal studies to establish causal relationships and to verify whether interventions in people with severe mental illness that try to increase group activities manage to improve their social participation and occupational balance. Fourth, nowadays, there are two instruments available for use in the Spanish population: the SOD-EO and the OBQ-E. SOD-EO assess satisfaction with occupations and occupational balance in the Spanish population with mental illness (Vidaña-Moya et al., 2020). OBQ-E is validated in the Spanish population but not in mental health. However, the use of the OBQ-E could be justified by wanting to compare people with and without mental illness and because the OBQ-E has normative data that also allows a better assessment of the results (Peral-Gómez et al., 2022).
Conclusions
People with serious mental illness reported a lower occupational balance compared to healthy people. Furthermore, our findings showed that the higher cognitive reappraisal, the higher occupational balance, and the higher expressive suppression, the lower occupational balance. These findings give reasonable support to the idea that patients with severe mental illness can benefit from occupational therapy intervention based on meaningful occupations, especially those required an interaction with others and with the environmental and not only the number of activities.
Key Messages
People with serious mental illness had significantly lower occupational balance concerning meaningful occupations, the balance between doing things alone/with others, and having sufficient to do during regular work.
The higher cognitive reappraisal, the higher occupational balance, and the higher expressive suppression, the lower occupational balance.
Patients with severe mental illness can benefit from occupational therapy intervention based on meaningful occupations, especially those requiring interaction with others and with the environment and not only the number of activities.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universidad de Granada. Vicerrectorado de Responsabilidad Social, Igualdad e Inclusión, Programa 45. Impulso de investigación en materia.