
Abstract
Introduction
Over decades, a picture has emerged of the costs of caregiving for a child on the autism spectrum. These include intensive time demands, high levels of stress and depression, and poor physical health (Hayes & Watson, 2013; Miodrag & Hodapp, 2010; Sawyer et al., 2010). Research using theory-based well-being measures, rather than those of ill-being such as stress or depression, demonstrate that the impact of caregiving on well-being for mothers of children with disabilities is a complicated picture. Caregiving parents have been shown to experience higher levels of eudamonic well-being in dimensions of personal growth, positive relations with others and purpose in life, for example, at the same time as they experienced diminished subjective well-being with reduced satisfaction with their job, standard of living, family income, and advancement in life (Larson, 2010).
Caring for a child with a disability requires a long-term commitment, managing complex needs often over many years (Dillenburger & McKerr, 2009). In many countries, the cultural expectation is that parents will care for minor children regardless of the intensity of medical and behavioral needs (Murphy et al., 2007) and will continue caring if the child cannot independently transition to adult life. Many North American healthcare systems rely heavily on unpaid family caregivers (Feinberg et al., 2011). U.S. family caregivers of those over 18 years of age with limitations in daily activities are estimated to provide 34 billion hours of care valued at $470 billion (Reinhard et al., 2019). Given the expectations that parents will care for their child, financial analyses for careers of children do not examine the value of their care to health networks but rather examine their losses in maternal employment and additional out-of-pocket costs for the family (Stabile & Allin, 2012).
Wellness promotion programs are needed to support caregivers’ long-term health, and to decrease premature morbidity and mortality of stressed caregivers (Epel et al., 2004; Murphy et al., 2007). Stressed caregivers have been shown to dramatically age more quickly according to cellular level analyses of telomeres (Epel et al., 2004). If caregivers are expected and depended upon by healthcare systems to sustain unpaid care from childhood through adulthood, they need support to have the mental and physical capacity to be responsive caregivers—which is a novel aspect of their own definitions of well-being (Larson, 2010). These caregivers often prioritize family needs over their own, neglect their own healthcare, and curtail participation in health-promoting activities (Larson & Bishoff-Miller, 2014). Parents with the most challenges in managing care and daily life may have the least capacity to engage in wellness-promotion programs; they may be too tired (Giallo et al., 2011). Effective wellness programs need to be tailored to these parents’ unique life circumstances, specifically addressing issues of fatigue and motivation.
Most currently available programs for parents of children on the autism spectrum are problem-focused, aimed at improving parenting skills, coping with caregiving issues, or stress reduction (Singer et al., 2007; Singh et al., 2007; Tétreault et al., 2014). A few have begun to address caregiver wellness. For example, mindfulness-based programs for these parents have shown promise as indicated by diminishing parent stress and depression, and improving child behavior (e.g., Dykens et al., 2014; Ferraioli & Harris, 2013; Rayan & Ahmad, 2017). Two recently developed programs, Healthy Parent Carers Workshop Intervention and Healthy Mothers Healthy Families (HMHF), specifically focus on promoting health using group formats. The first provides programming addressing eight health behaviors in a six-week program (Borek et al., 2018). Participants in the feasibility study found the program's educational content satisfactory; however, they noted it did not support their setting and achieving of realistic individual goals afterwards. The HHMF program has been delivered in an in-person and online format; modules focus on healthy eating, physical activity, psychoeducation, help seeking behaviors, stress reduction, empowerment, self-esteem, family cohesion, and shared leisure (Bourke-Taylor et al., 2019). In the HMHF in-person group format, significant improvements were noted in health behaviors and mental health over time, and significant changes in well-being were maintained 3 months post intervention (Bourke-Taylor et al., 2019). However, in the online format, there was a 61% attrition rate, and only 37–40% of mothers reported changes in mental health, and physical activity and leisure (Bourke-Taylor et al., 2022). These programs focused broadly on the issues mothers manage when parenting a child with a disability and had positive outcomes. Still, each had limited individualized goal setting or lifestyle change content to create and support sustainable health-promoting participation in desired occupations.
Caregivers are best positioned to identify desirable elements for a wellness program that fits their lives. And, in keeping with the focus of occupational therapy and the World Health Organization focus on health being derived from engagement in a range of desired and meaningful everyday activities, we believed such a program should take an occupation-based approach (Larson, 2019; World Health Organization, 1984), congruent with one's desired time-use in a range of occupations that meet the needs for health, safety, rewarding relationships, competence, engagement, and achievement of vital goals (Matuska, 2012; Matuska & Christiansen, 2008; Sheldon et al., 2010). Viable wellness programs must be tailored for caregivers’ complex lives, if they are to be able to engage in it and derive benefit from it. Caregivers may identify priorities and tradeoffs in daily activities that are necessary for them to access and participate in a wellness program, as well as desirable features of wellness program that fit their lifestyles. The aim of this work was to work collaboratively with caregivers to design a wellness program tailored to their lives that would be both practical and sustainable.
Method
Using a recursive multi-step process, the research team worked with groups of caregivers to develop an occupation-based wellness program that ideally would be individually tailored, manualized, and use approaches rooted in current evidence supporting lifestyle change. Our process included collaborating with caregivers to define lifestyle issues that impede wellness, collaboratively designing a program that was informed by current evidence and caregivers’ preferences, delivering this program to the designing cohort, assessing the program post-participation and repeating this process with a second cohort to refine the program (with the exception of the design step). Focus groups were used, rather than other qualitative methods, to manage participant burden and to understand the degree of group consensus on questions posed. We believed this collaborative research-informed approach promoted a tailoring to caregivers’ lifestyles while being rooted in occupational science principles and lifestyle research. The study was approved by University of Wisconsin-Madison Institutional Review Board (2015-1004); and the Protocol Record NCT03771001 was registered with ClinicalTrials.gov.
Participants
In-person informed consent was obtained prior to participation in the study. Caregivers were recruited at autism conferences and therapy clinics. Interested parents completed informational cards and were screened by phone. Parents were included who: served as a primary caregiver for a child on the autism spectrum 8–21 years of age, were willing to commit sufficient time to participate, and had no major mental health condition except depression. It was expected that caregivers of children older than 8 years of age had established care routines and were therefore able to benefit and manage participation in a lifestyle program.
Collaborative Research-Informed Approach
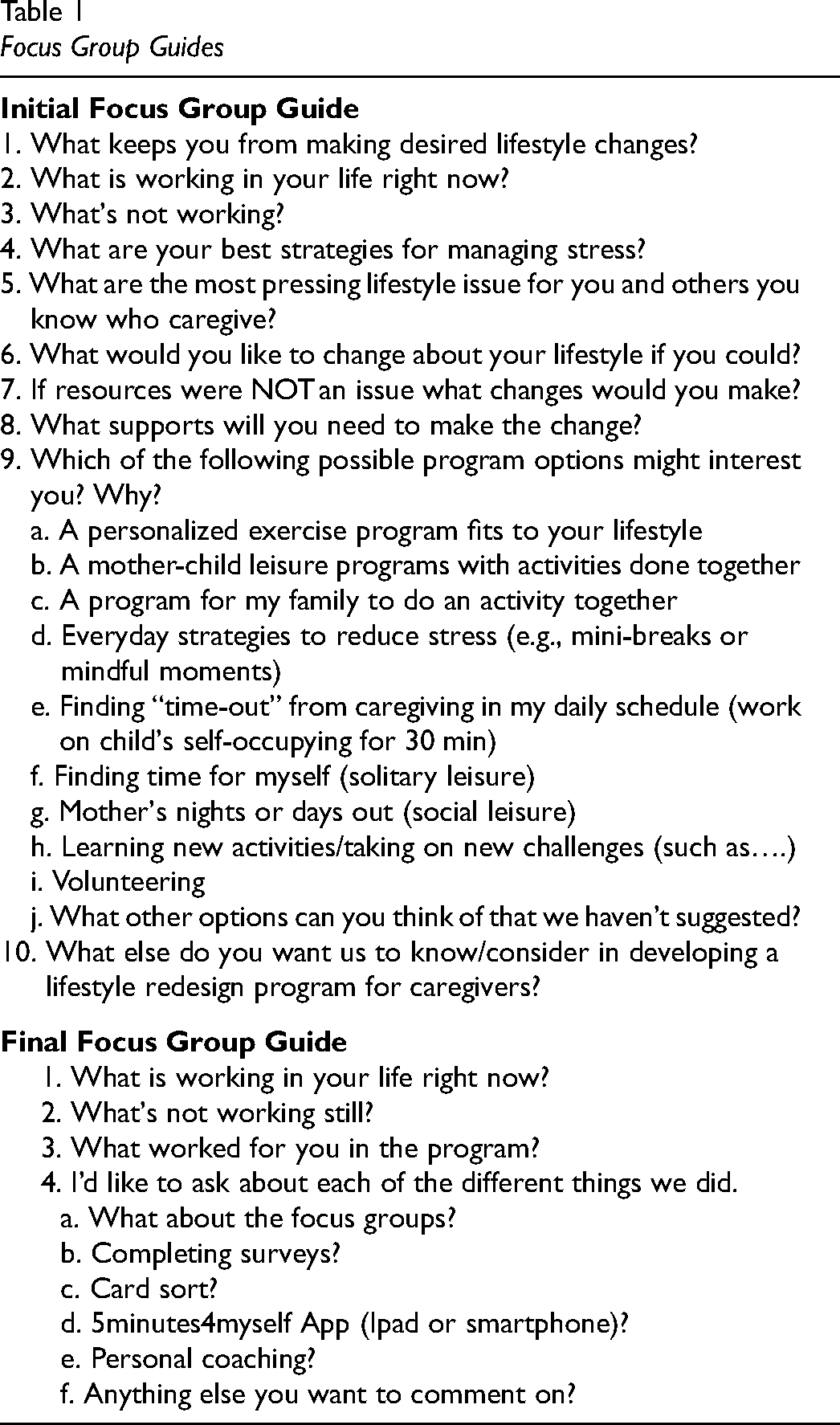
We began by identifying the caregivers’ lifestyle problems, then co-designing a potential program, and after delivering the program, evaluating the quality of the program via a series of focus groups. The principal investigator led focus groups; she had over 30 years’ experience working with families of children with disabilities as well as expertise in conducting focus groups and qualitative methods. (During data collection, participants confirmed that participating in research was easier for them when they had a focused period of time to participate that was free of caregiving responsibilities.) At the initial focus group for the first cohort, we asked all caregivers present “What's working/What's not working in your life?” to identify lifestyle issues impeding wellness and had them complete a form describing demographic information (age, gender, race/ethnicity, marital status, education, family income, full/part-time work status, children's ages and diagnoses) and a number of surveys including the Perceived Stress Scale (Cohen et al., 1983) and Center for Epidemiologic Studies Depression Scale (Eaton et al., 2004; Radloff, 1977). From a literature review of wellness promotion and occupation-based principles for lifestyle change developed by our team (see Larson, 2019), we created a PowerPoint of potential program principles and elements. This PowerPoint presented three main focuses: 1) Doing (activities promoting pleasure/leisure or social connection, e.g. Lyubomirsky & Layous, 2013) and strategies for lifestyle change to support Doing (usefulness of habits, ecological slots for changing low-valued activities with high-valued ones, starting small, considering personal energy/times of day for occupations, e.g. Bernheimer & Weisner, 2007), 2) Thinking practices (positive emotions fueling resiliency and well-being; benefits of gratitude, e.g. Van Cappellen et al., 2018) and 3) Goal Visioning or pursuit to increase lifestyle balance (enhanced well-being from goal attainment). We also queried caregivers for their preferences for program elements (see Table 1, Focus Group Guide). Based on this information, the team drafted and presented the program at a second focus group eliciting caregivers’ feedback. We then delivered the wellness program to this group of caregivers. After participation in the program, we asked these caregivers about their views of the program in a focus group. The first group participated in three focus groups (initial, design approval and program evaluation). As a research team we reflected on this data to make decisions about program changes for the next version of the program (V2). The revised program (V2) with companion mobile app, designed based on the first cohort's feedback and developed by a local software startup company, was then delivered in three waves to a second cohort, who similarly evaluated the program in focus groups. These data were again reviewed and reflected on by the research team to make decisions about program revision (3 initial and 3 program evaluation focus groups).
Focus Group Guides
Data Analysis
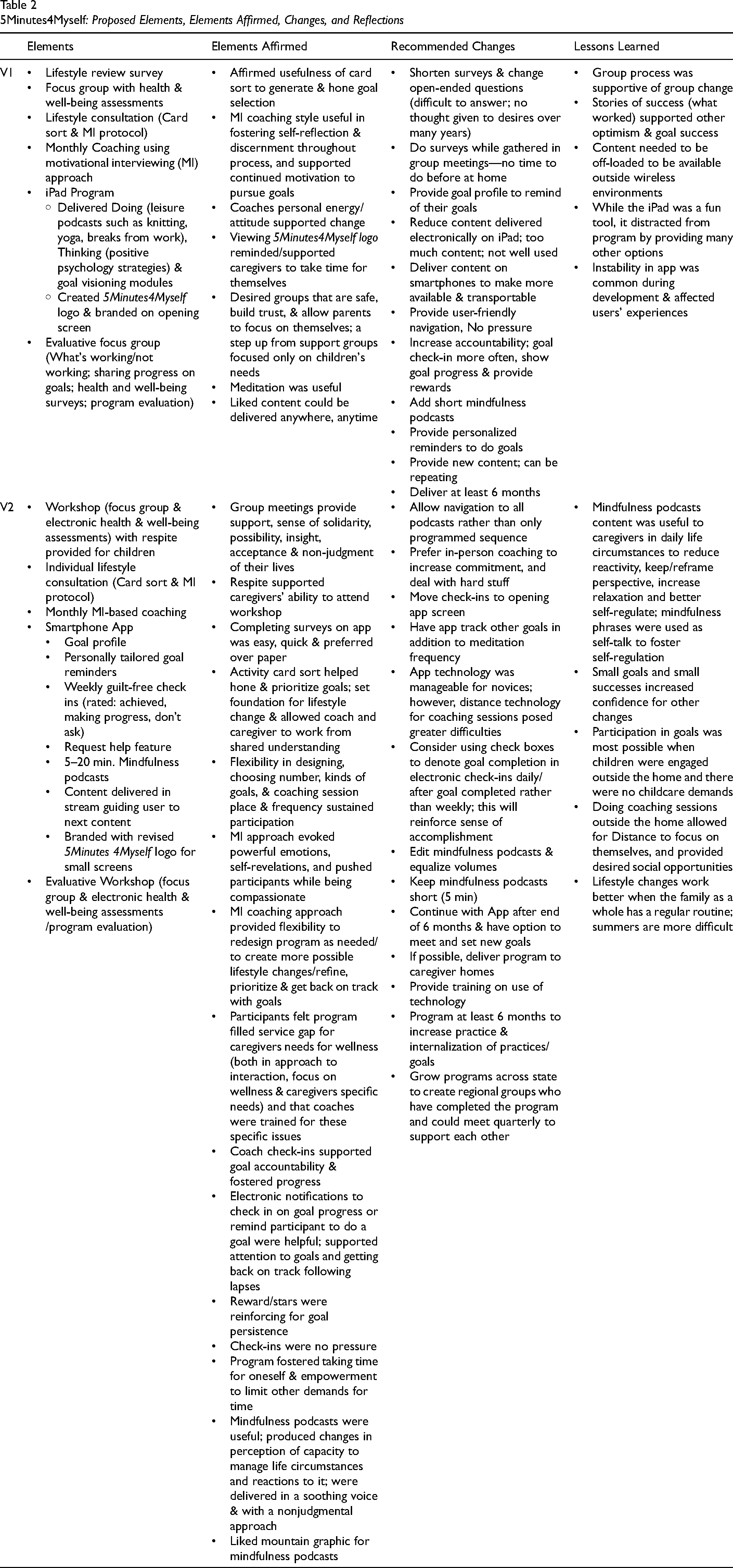
To characterize the participant group, demographic data were analyzed descriptively. Next, recorded data from the series of focus groups was transcribed verbatim and reviewed for accuracy, producing a total of 190 single-spaced pages. At each phase, data segments representing the focus of the analyses (e.g., lifestyle issues or program evaluation) were selected and entered an excel spreadsheet, coded to identify themes in the data (Braun & Clarke, 2006). First, transcribed data was read, emic codes to describe caregivers’ key lifestyle issues that needed to be addressed in a wellness program were generated and grouped into themes. Exemplars of themes, quotations from participants, are provided to support interpretations (Cordon & Sainsbury, 2006). In our next step, post-participation evaluation, segments of focus group data describing similar perspectives were grouped, paraphrased to capture the core idea, and sorted into categories of elements affirmed and recommended changes for each version of the program (see Table 2). Key quotes supporting the program elements are provided (Cordon & Sainsbury, 2006). The research team, the principal investigator, project assistant, and undergraduate and occupational therapy master's students, met after each post-program evaluation focus group to review the focus group data, reflect on the process, and decide upon program revisions. Reflections from this process are described in the Lessons Learned column in Table 2 and summarized in relevant sections.
5Minutes4Myself: Proposed Elements, Elements Affirmed, Changes, and Reflections
Findings
Twenty-eight participants were recruited and participated in the study. They were mostly female (89%), Caucasian (97%), aged 30 to 63 years of age (M = 49.75), varied in education (50% graduate, 28% bachelors, 11% associates, 7% high school, 4% not reported), paid employment (32% full-time, 16% part-time), and income ($10,000 to $140,000, M = $65,481; poverty level for family of 4 = $25,100 in 2018). Prior to participation, 60% of caregivers had scores > 16 as measured by either the CESD or CESD-R (M = 19.7; SD = 9.9; range 8–43), which suggest they were at risk for clinical depression (Eaton et al., 2004; Radloff, 1977). They were parenting boys who ranged in age from 9–21 years (Mean = 14.6); two families had two autistic boys. On the Perceived Stress Scale-10 item, the group scored 23.8 (SD = 5.3; range 14–35; Cohen et al., 1983). Using population averages range from 2009 for the PSS-10, 48% scored between the mean to + 1SD, 48% of the group scored > 1SD above this mean for their age, and an additional 4% scored > 2 SD above the mean (Cohen & Janicki-Diverts, 2012). This suggests that slightly over half of the group were experiencing high levels of stress. Five participants dropped out after the initial focus group; of those remaining 56% attended the post-intervention focus groups.
Through the caregivers’ narratives and a detailed data table, we present our collaborative work with the two cohorts, to design and refine a caregiver program intended to promote wellness, that could be individually tailored, and fit the constraints of their lives. Caregivers were clear that their time was limited and that they were desperately in need of wellness in their lives. In the following sections, key lifestyle issues, program design, program evaluation, and research team reflections that informed choices for revisions are presented.
Key Lifestyle Issues to Be Addressed
A number of complex lifestyle issues arose in our discussions with caregivers. One issue that emerged was surprising—the caregivers’ difficulty in even identifying a wellness goal Other issues caregivers noted have been previously described—such as the delicate balancing and tension between the caregiver's and family's needs or the caregiver's social isolation and need to rebuild social connections—yet this data provided a deeper and more nuanced understanding of the impact of these issues on lifestyle change for wellness promotion. Three themes emerged: Where to begin?, All on me/risks of stepping away from caring to pursue wellness, and So many pieces need to fall into place.
Where to begin?: The first cohort repeatedly expressed their difficulties in reflecting on and identifying potential wellness-promoting occupations that they could pursue. As one mother noted when trying to answer questions about wellness promotion, “I feel like I don't really know what I'm doing anymore . . . I don't know what brings me joy. I don't know what brings me stress” (P5). In the focus group, caregivers began by talking about their child's needs, rather than their own lives when describing what worked or didn’t work in their lives. An intentional mental shift was necessary for caregivers to focus on their own wellness; this was evident in the next theme as well—the need to have permission to pursue wellness. One mother of teens had begun to engage in occupations essential to her sense of self, “I took snowboard lessons . . . I feel like I'm getting back to the person that I was 12 years ago. . . before [my son] was born” (P2). Addressing this difficulty that many family caregivers expressed, in even generating one wellness goal, was essential to developing this program for caregivers. There were also other challenges noted by caregivers that they believed limited participating in a wellness program as noted in the next theme.
All on me/Risks of stepping away from caring to pursue wellness: Recuperative activities, exercise, mindfulness and social outings, including returning to interests or friends from decades ago were desired options. When asked what kept them from these occupations, caregivers listed guilt, time, energy, and need for oversight of family routines. There was a tension between taking time to care for self and risking the whole family's peace and harmony spiraling out of control in their absence. One mother explained, “It's just so much easier to do everything for yourself and make sure you are in control of the situation rather than let it get out of control” (P3).
So many pieces need to fall into place: Several mothers noted a desire to have or reengage in a fuller and fulfilling social life: “I really want to reconnect with some of my past friends. I really only have work friends right now. [Interviewer: And what would that take to do that?] It would take me calling them up and have a conversation and reconnect ‘cause it's been 15 years. . . [So you need time or motivation to do it?] I need the permission to do it. The commitment to do it, and then the time to do it, and then after that to meet with them so then the energy to go and do it” (P2). Another mother commented, “And that's a lot of pieces. That's the problem” (P5). Creating lifestyle change required a belief that they could make time and space apart from their complex family demands, and that they could act on their long-neglected desires for leisure and rebuild social connections.
Program Design (Version 1)
A detailed description of the elements of this first version of the program is described in Table 2. To assure the program was rooted in current evidence, we presented and caregivers affirmed the use of coaching and positive psychology approaches for fostering behavioral change and wellness (Martins & McNeil, 2009; Sin & Lyubomirsky, 2009).
We addressed the unexpected key issue that arose from the initial focus group data: caregiver's (lack of) capacity to generate wellness goals and strategies for delivering occupation-based wellness-promoting content that fit within caregivers’ constrained schedules. It was clear from our data that a process was needed to facilitate caregivers’ generation and selection of meaningful wellness goals. First, we created a generative process to prompt caregivers’ consideration of a range of occupations. We choose to use an activity card sort that provided physical prompts, sorting cards into piles of desired and non-desired activities, to promote consideration of a wide range of possible health-promoting lifestyle changes. The Adolescent and Young Adult Activity Card Sort (Berg et al., 2015) was paired with a step-by-step Motivational Interviewing-based Road Map. This manualized process included: open-ended questions about each card selected, a query to strengthen motivation (e.g., “How do you think this would change your life?”), an assessment of confidence of goal achievement, prompts to explore ambivalence, and queries about next steps aimed at increasing commitment to change.
Second, an iPad app was created to host goal generation reflections, as well as other content requested. The iPad app was developed to deliver program content anytime and anywhere and provided three content streams: Doing, Thinking, and Goal Visioning. Thinking content included gratitude practices, and links to meditations. Doing content promoted participation in leisure and exercise such as links to yoga videos, at your desk exercise breaks, knitting tutorials or exercise tracking. Lastly, it hosted the Goal Visioning exercises. The iPad program was branded with a 5Minutes4Myself logo developed by a team member. This name reflected our micro approach and emphasized caregivers’ needs for restoration.
Caregivers learned to operate iPads and the 5Minutes4Myself IOS iPad app. Trained coaches scheduled times to meet with caregivers for a lifestyle consultation (activity card sort/manualized MI Road Map) to design individually tailored goals and plans. Each coach and participant decided how, when and where they would meet for monthly coaching sessions and if they would meet with greater frequency than monthly. At the end of the program, we met again as a group for program evaluation.
Program Assessment (V1)
The post-participation evaluative focus group examined participants’ perceptions of the program's impact and usefulness. Participants were again asked What was working/not working in their lives?, and about each program element (focus groups, activity card sort/lifestyle consultation, coaching & iPad app and provided links to leisure occupations).
Caregivers reported a new belief that their wellness was a worthy priority, and that such a priority was beneficial to the whole family, despite competing demands. “It made me also remember the importance of planning to keep myself alive and happy and able to function. Not only so I feel good but also for my family … It's not okay for me to feel miserable … Sometimes I'd have to choose not to do what my son needed because the greater good was doing for me … It had broader implications” (P3). Overall, caregivers noted positive changes from participation: “It made a difference. I feel more in control of my life than I did before. It always felt like I was playing catch up and now I'm more proactive” (P4).
We discovered that the focus groups served the caregivers by allowing them to share their lives without feeling judged, and built community. “Groups like this, I think it steps it up from a support group. That's why I kind of like this because I didn't want a support group of gripes, feeling sorry for myself … but at the same time … it's like you can just talk” (P2). Caregivers noted other groups for families of children with disabilities did not focus on their needs but led to additional “homework”—reading a recommended book on autism or pursuing new services. Leaving them to feel the need to do more caregiving rather than engage in health promoting occupations.
The Adolescent and Young Adult Activity Card Sort addressed that core issue of where to begin their wellness pursuits. “I think that exercise with all the little cards, that was really, really helpful (‘Yeah that was’, others echoed on the recording). Because I think it's just you don't know what's working and what's not, and what you want and what you don't want. Because you're just trying to get through the day” (P2). In contrast, the multiple goal generation exercises delivered on the iPad app were not well used or found to be useful.
The motivational interviewing coaching approach was well received. The coaching sessions were noted to provide support, focus on goals, accountability and encouraged persistence. “What was probably the best was meeting with [my coach] on a regular basis. And having that one-on-one relationship face-to-face … just having her bringing me back to ‘What are the issues?’ Because we do, we absolutely get taken off on these tangents” (P2). And another, “I liked having [my coach] periodically [meet with me]. I'd have to summarize it, what was working and what wasn't working [in my life] … I don't take time to do that … I think that was the biggest thing, it was kind of like accountability” (P3). One noted how it felt to be really heard, “I felt it … she really, really listened. Which is kudos, because it's really hard to listen to somebody and pick out the important parts” (P2). These quotes support that coaches effectively evoked caregivers’ focusing and problem solving to address their own issues, provided needed accountability, and employed the spirit of motivational interviewing (Miller & Rose, 2009). Coaching sessions supported persistence, “I'd go back after that meeting and say ‘Oh, okay, I can focus on this, this is something I should do.’ So, I like that a lot” (P2).
The iPad app and links were not well used; only one participant used it frequently. This was reportedly due to time scarcity and technophobia. For the one high-usage caregiver the app worked as intended in our program principles. She noted, “You could do [meditation videos] when you wanted to and it was almost live in a way. And so it seemed really real to me and you didn't have to go anywhere to do it … I think that was the most convenient thing” (P2). Yet others, who did not use the mindfulness videos, expressed a strong interest in mindfulness but only if it was delivered in short sessions and a more easily accessible format.
Surprisingly, the logo inspired self-caring. “I like the name of it … 5 min to myself. Have I been taking 5 min to myself? Just the idea, the name” (P3). And another, “The concept is great. The concept of just five minutes” (P5). Caregivers suggested modifications of this electronic support: use a smartphone so it is consistently available, create a goal profiles to remind caregivers of their goals, have a graphic to show progress, make navigation simple, add reminders to engage in goals, and have “no pressure” more frequent check-ins for accountability. “It would have [been] helpful that it kind of gauged what you said you were going to do and if you did it. If it had some kind of a chart or some data … some accountability measure” (P2). They noted a new app would need to strike a balance between accountable and not inducing guilty if caregivers lapsed in pursing their goal.
A number of lessons were learned from this cohorts’ experience when our research team reflected on the process. First, focus groups served a purpose beyond what we intended, creating a community that met needs that support groups did not. The focus on the parents’ wellness, rather than the child, was experienced as unique, and yet having a group that understood how their lives were shaped by parenting a child on the autism spectrum was essential to sharing their vulnerabilities and feeling supported. Believing they were in this together supported optimism for pursuing long neglected wellness goals. Second, a number of iPad app issues disrupted program delivery: content that was not available outside of wireless environments, and app instability. We recognized the need for off-loaded content that could be delivered outside of wireless environments, especially for those in rural areas, and additional refinements to assure app stability.
Program Design Version 2
The second caregiver cohort was provided with the revised program (see V2 Table 2). The first group meeting was redesigned to include the community-building focus group, survey completion, and provided instruction on using the newly designed smartphone app. Respite was provided to families to make attendance as convenient as possible. The individual lifestyle consultation and monthly coaching sessions remained the same since no changes were suggested by the previous participants.
The major V2 innovation was development of the cross-platform (IOS or Android) smartphone app. App content was simplified from the iPad, with additions of habit building features to support goal persistence, and mindfulness podcasts. New features included a goal profile, customized goal reminders, weekly guilt-free check-ins, easy “stream” navigation, micro-mindfulness content, and new 5Minutes4Myself branding. Our micro-mindfulness program content was designed for caregivers’ needs (e.g., a specially tailored introduction for mothers of children on the autism spectrum, and loving kindness meditation for parents of children with disabilities). Content included sequentially longer 5–20 min podcasts prepared by a clinical psychologist who was also a trained Mindfulness Based Stress Reduction instructor. Podcasts included a mini-introduction to the instructor and mindfulness, “dropping in” to the present experience, breath awareness and deep breathing, body scans, and loving kindness meditations. Podcasts narration included elements of non-judgment, observing what is, being present in the moment, and loving kindness toward self and others. The intention was to easily fit mindfulness practices into caregivers’ schedules to allow them to derive the health benefits of this intervention.
Program Assessment (V2)
Post-participation, caregivers again affirmed the usefulness of the group meetings, the activity card sort/MI consultation for goal generation, and the MI coaching (see Table 2). They again noted that group meetings were community building, creating a supportive non-judgmental environment, sense of solidarity, and possibility to launch into lifestyle change. “You see other groups of friends … you have this group where they’re all dance moms and this group they’re all soccer moms [laughs] and you know like we didn’t know each other before. And so we’re not judging on anything, we’re just moms of children, autism moms. Yeah so the groups are solidarity, you know, unspoken, and neutral. You know we share a life. I mean we walk similar walks. And nobody will be like judging. And I will be like yeah I totally get it” (P22). Similarly: “At least for me, it just showed that I wasn't alone … we have some of the same struggles … different families might have different struggles, but a lot of them really are related and kind of the same. So, you didn't feel like, even as I was working on my goals, even though so and so might have different goals, but we were all working on kind of the end goal of having a better quality of life” (P16). This confirmed again the importance of these groups in community-building that supported lifestyle change.
This group provided more detailed comments about the impact of motivational interviewing-based coaching in providing flexibility for lifestyle programs and in delving deeply into the emotions driving lifestyle choices. They commented on the usefulness of the MI approach in allowing them to feel free to adjust their lifestyle programs to allow them to prioritize or get back on track after lapses. One mother said, “I think what was helpful to me was picking three goals that seemed really do-able, you know, so they were smaller than what I would usually choose as a goal. And then just keeping a focus on those three things week after week after week. I mean normally I would do something like twice and then be you know ‘check’ [laughs] … I think having some continuity to it was really helpful because it's giving me enough time to make things really happen” (P22).
Caregivers confirmed that the features of the app were very useful: notifications were helpful in attending to goals and getting back on track, check-ins were indeed no pressure and rewards reinforced goal persistence. Mindfulness podcasts were seen as useful and produced changes in their perceptions about their capacity to change their life, altered their reactions to previously anxiety producing life circumstances, and were pleasant in their visual and auditory features. For example, this mother recalled phrases to help her cope with daily challenges: When I'm in those moments where things are really frustrating or I'm at [work] and things are just not going right, I do try to think back to some of the … little phrases …‘let it go’… I can just take a deep breath or just walk away for a few minutes … I don't feel like I'm as reactive at the end of the day as I used to be with my family … So, I think that part helped. (P18)
Some wanted only five minute podcasts: “It's a lot easier to fit in.” This short format was suggested to provide greater sustainability of the practice, “Then I can see it do-able for the rest of my life because at some point your mind is trained so we can do it without the lady coaching you through. Because you catch yourself thinking ‘Ok, I’m stressed let's concentrate on that’… I can hear her advice of ‘Just breathe and pause’ … in my head, so after a long time I think the five minutes would be perfect” (P19).
The program as a whole was described as flexible and produced small successes, which increased confidence for other changes. The caregivers also noted that lifestyle change was best promoted during the school year when family schedules were more structured; those coached over summer months felt it was much more difficult to pursue their goals and had less success. Caregivers suggested app modifications: flexibility in selecting podcast sequence, change app flow (placement of options on opening screen, additional goal tracking), increase frequency of check-ins, audio editing of podcasts to reduce background noise, and allowing continued app usage after the program was completed (See Table 1).
Caregivers felt this program filled a significant service gap. They expressed dissatisfaction with prior mental health services that failed to get at the nub of their issues, or which stopped on strict schedules. “So, there was something about feeling like this person is trained for my specific issue in life …You just feel like there was a specific goal we were working on and they understand where I'm coming from” (P19). Caregivers noted that having completed the activity card sort/MI Roadmap with their coach, they started with a shared understanding to work from. Caregivers desired that the program be readily and widely available, longer in length of time, and extended to include regional support groups for program completers to sustain lifestyle change.
In our reflections, we observed several ways caregivers gained from the program as designed and some insights into future options. Caregivers quoted mindfulness content to one another and described how they used these phrases as self-talk to reduce their reactivity to everyday stressors. It was clear even small doses of mindfulness appeared to be useful to caregivers. They noted that achieving small goals increased their confidence to pursue other changes. The school year was an easier time to engage in the program, due to its regular schedule for childcare, whereas summer didn’t work.
Discussion
A collaborative research-informed approach allowed the research team and users to co-create an intervention that fit caregivers’ lives. Through this approach, we developed and honed a micro-, portable, tailored, evidence- and occupation-based wellness program for caregivers. This was an advancement in its occupation-based approach (using an activity card sort to elicit occupational goals), personalization, and elicitation of small workable goals. The program developed here used fewer group sessions than other current programs, although recognizing the importance of group support, and provided individual consultation and coaching to achieve wellness goals which caregivers found useful. Adding health promoting occupations using a “small goal” approach is well supported as reasonable approach to change and a potential steppingstone to additional changes (Zinn et al., 2012).
Given that caregivers felt it critical to be present to manage the interactions between family members to promote harmony and reduce disruption, the program design needed to support the caregivers’ shift in thinking that their own wellness was a priority (DeGrace, 2004; Larson & Bishoff-Miller, 2014) and that stepping away from caregiving to have time for their wellness-promoting occupations was possible. The app logo and micro-approach, just 5Minutes4Myself, seemed to support this shift in thinking and willingness to restructure their schedules in small ways to include wellness-promoting occupations. The mindfulness component seemed to foster this as well, allowing them to feel more in control and less reactive to challenging family circumstances. For this population, experiencing benefits from mindfulness practices has been shown in other programs as well but in this program the time commitment was significantly smaller with shorter meditations and no 1–2 hour weekly in-person meetings required(Rayan & Ahmad, 2017; Shapiro et al., 2007; Zautra et al., 2012).
Although evidence-based elements were useful in developing the program, unexpected issues led to useful innovations. For example, caregivers’ difficulties in identifying wellness goals led to the development of a generative process for goal selection. While intended for data gathering, focus groups became community-building meetings that inspired and supported participants in pursuing wellness. Motivational interviewing facilitated personal insights that circumvented beliefs and thoughts that were barriers to wellness promotion. The development of a smartphone app with a mindfulness program and its habit-building features arose from participants’ desires for greater program portability and accountability. Caregivers’ requests for adding this specific positive psychology intervention to the program are well supported (Sin & Lyubomirsky, 2009) and was well received in this project. Most importantly, caregivers felt the program filled a crucial unmet need for wellness promotion for parents of children with disabilities.
This program was developed with a small number of caregivers yet based on the data provided here we believe it may have social validity for a larger group of caregivers, but this will need further research to confirm (Seekins & White, 2013). In addition, further manualizing the program and creating training protocols to assure coaches are sufficiently trained are additional steps needed in the development of this intervention. To assure that later the program outcomes can reliably be assessed, additional procedures assessing the fidelity of the MI coaching are needed.
There are limitations to this work. The wellness program was developed largely with and by white mothers, many who were well-educated, at risk for depression, moderately stressed, and with modest financial resources. Caregivers with fewer social and economic resources, more severe depression or stress may need additional supports. In addition, cultural tailoring for specific groups and contexts is known to increase the use and effectiveness of programs (Smith et al., 2011), so such adaptations should be developed. Even the most efficacious treatment interventions are improved through cultural adaptation especially when adapted for needs of underserved communities (Benish et al., 2011).
Conclusion
Similar to other findings, for most mothers in our study it had been years since they considered finding time to engage in wellness promotion (Hoogsteen & Woodgate, 2013). This project confirms that for caregivers an integrated approach of peer group support, and in-person coaching with smartphone app is useful in an occupation-based wellness program. The 5Minutes4Myself program delivers a tailored individualized program and leverages group and technology-mediated support. Mobile technology, used to supplement rather than replace quality healthcare, is predicted to revolutionize healthcare in the coming decades (Steinhubl et al., 2015). This model of extending in-person occupational therapy interventions via mobile technologies is viewed as a promising avenue to increase access to care for underserved groups, reduce travel time and costs.
Key Messages
A collaborative research-informed approach was a useful method to invite caregivers to co-design a wellness intervention that was tailored to their lifestyle, constraints and resources, as well as caregiving demands.
The co-designed wellness program developed was personally-tailored via a lifestyle consultation that used an activity card sort and motivational interviewing protocol to elicit small workable occupation-based wellness goals, and supported caregivers’ lifestyle change via coaching and a companions’ smartphone app.
The app logo (5Minutes4Myself) and micro-approach supported caregivers’ beliefs that it was possible to attend to their wellness and restructure schedules in small ways to include wellness-promoting occupations.
Footnotes
Acknowledgements
The contributions of the co-researchers, study participants who shaped and informed this work, are deeply appreciated as are those of the undergraduate and MSOT students serving on the research team.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.