
Abstract
Technology is no longer optional in our work, play, and self-care occupations. Clearly, occupations include technology … (Smith, 2017, p. 5).
Introduction
Technologies are embedded in all occupations and directly impact how people live, where they work, how they spend their time, and even what they wear (e.g., smart watches) (Liu, 2018). Assistive technology (AT) includes widely available mainstream technologies and their derivatives (e.g., voice recognition, screen enlargement, automatic door openers), adapted commercial technologies (e.g., adapted mobile technology, hand controls for mobility devices), and custom-designed technologies that enable people with disabilities to engage in occupation (Cook et al., 2020; Liu, 2018; Smith, 2017; World Federation of Occupational Therapists [WFOT], 2019). Technologies present important and innovative means to enable and support occupation, and technology is an important aspect and core competency of occupational therapy assessment and intervention (Liu, 2018; Smith, 2017; WFOT, 2019); however, the proliferation of commercially available technologies have blurred the lines between what can and cannot be characterized as AT (Mirza & Hammel, 2009).
Adults with intellectual disability 1 (ID) have a long history of occupational challenges and can benefit from the therapeutic and functional use of AT and other technology supports (Johnson et al., 2019). Technologies to support participation for adults with ID include the common applications of information and communications technologies, computerization, artificial intelligence, and virtual reality (VR) (Liu & Mihailidis, 2019; Mirza & Hammel, 2009), which can aid in participation in daily life activities, community living, and social inclusion. Additionally, technologies may enhance functional independence, self-determined decision-making, employment, educational opportunities, and leisure and social activities (Boot et al., 2017).
A recent scoping review of the evidence for occupational therapy-related intervention with adults with ID found technology training and technology support as key intervention methods (Blaskowitz et al., 2021). While scoping reviews are useful for identifying the available evidence, they are, in general, limited to a broad synthesis and description of data without nuanced exploration of the review results. Secondary analysis–a review of existing data that was collected for a particular area of interest–allows for a more focused examination and is particularly relevant when reviews yield a significant number of articles for inclusion. For example, Moore et al. (2021) conducted a secondary analysis of their scoping review on the economics of abortion services to ascertain how stigma related to seeking and providing abortion care influenced economic-related outcomes (i.e., cost, benefits, impact, value) at multiple societal levels. White et al. (2011) employed secondary analyses of their scoping review of health promotion interventions to further examine the impact of physical activity-specific health promotion programs on mobility impairments. While the number of secondary analyses of scoping reviews remains limited in the literature, the aforementioned studies demonstrate how this type of analysis provides a more nuanced understanding of the findings (Moore et al., 2021; White et al., 2011).
To further inform occupational therapy practice with adults with ID, this secondary analysis study sought to characterize evidence of the range of technologies available to support occupational engagement of adults with ID. The types of technology, including their form and function, that occupational therapy practitioners and researchers use with adults with ID can influence technology-based assessments, interventions, and supports for adults with ID.
Methods
To ascertain the types of AT used as occupation and AT employed to enable occupational engagement for adults with primary or comorbid ID, the authors performed a secondary analysis of a scoping review aimed at identifying and characterizing literature to inform OT assessment and intervention with that population (Blaskowitz et al., 2021; Mahoney et al., 2021).
Scoping Review Procedures
The authors followed scoping review procedures as outlined by Arksey and O’Malley (2005) and determined the research question for the larger scoping review to be: What is the scope of the evidence related to OT practice with adults with ID? Keywords and controlled vocabulary terms (e.g., “cognitive impairment,” “intellectual disability,” “mental retardation,” “occupational therapy”) were developed by a consulting librarian and custom searchers were completed in PubMed, CINAHL, PsycINFO, and Scopus (Blaskowitz et al., 2021; Mahoney et al., 2021). Citations and abstracts from the searches were maintained in Covidence (Veritas Health Innovation, 2019), a web-based review management system. Inclusion criteria were as follows: (1) articles published in English between January 2002 and January 2018; (2) articles printed in a refereed publication; (3) articles that included content on adults with primary or co-occurring ID; and (4) articles that contained information applicable to occupational therapy practice (citation redacted for peer review). In addition to original research studies, this review included any relevant article in a peer-reviewed publication (e.g., literature reviews, position papers, etc.). Literary criticism, gray literature, and articles that included participants with disabilities without co-occurring ID were excluded.
Full-text screenings of 569 articles were completed, of which 159 articles met the inclusion criteria. Refer to Figure 1 for details on the number of manuscripts identified, included, and excluded for review (Blaskowitz et al., 2021; adapted with permission). In their initial review, the authors noted the frequency with which technology emerged in their analyses; consequently, a secondary analysis was conducted to determine the form and function of technology in relation to OT assessment and intervention with adults with ID.
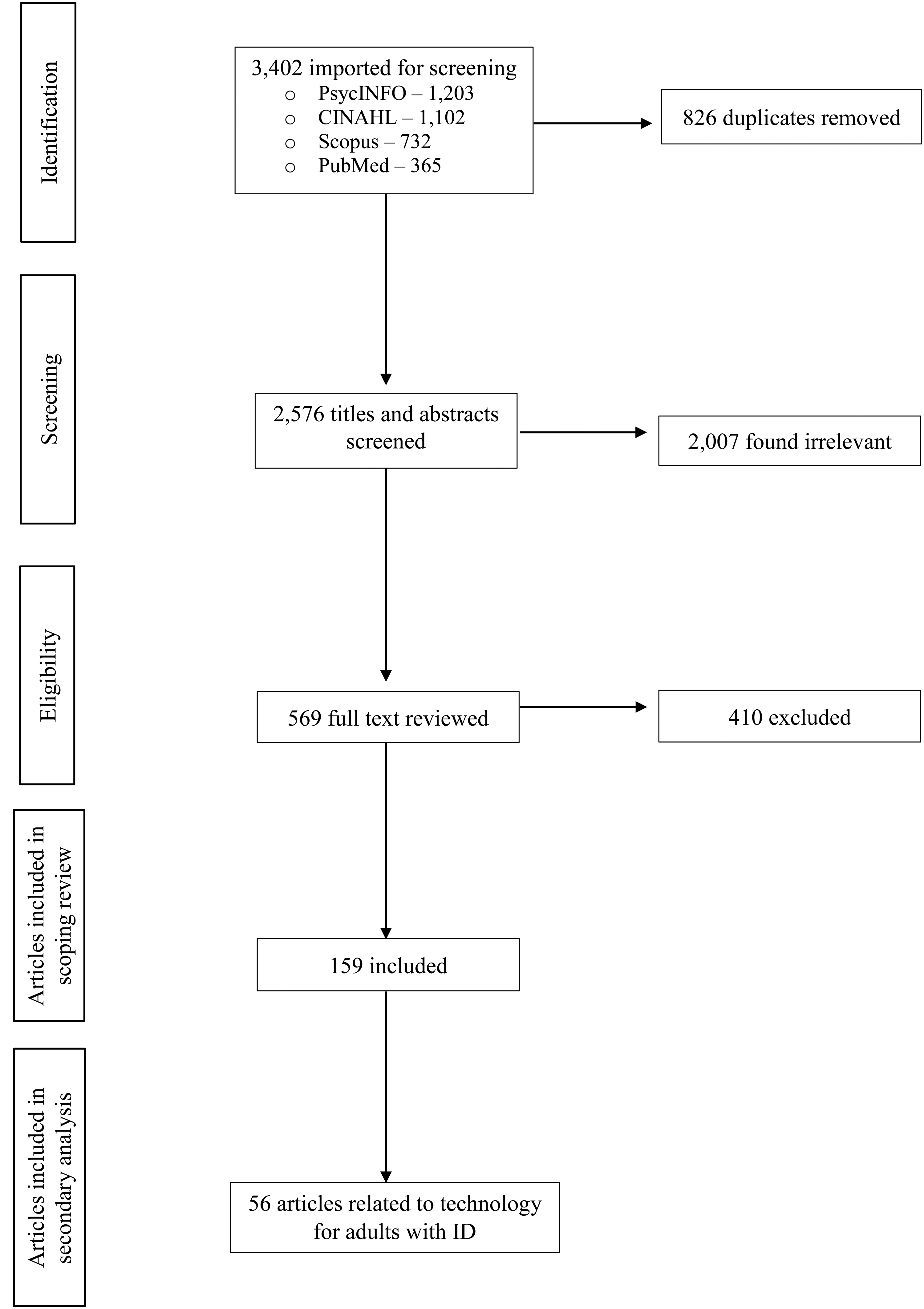
Flow diagram for inclusion and exclusion of articles in the secondary analysis.
Secondary Analysis of Scoping Review Procedures
Literature outlining the process for secondary analyses of scoping reviews is limited; however, scholars in library science have indicated the analytic process involves (1) developing the research question(s); (2) identifying the data set to be investigated; and (3) completing a thorough evaluation of those data (Johnston, 2014).
Secondary analysis: inclusion procedure
For this secondary analysis, the authors reviewed all 159 full-text articles included in the initial scoping review for inclusion and analysis (Blaskowitz et al., 2021; Mahoney et al., 2021). The authors sought to address the question: what are the types and purposes of technologies identified in the articles? The authors included articles in the secondary analysis that explicitly named the use of technologies with adults with ID in any section of the article, regardless of its focus. Articles previously coded for technology-related intervention were initially included in the secondary analysis. All other articles were reviewed twice by the authors to determine if technology information was present. All authors discussed and resolved any inclusion conflicts.
Secondary analysis: data analysis procedure
After determining which articles met the inclusion criteria for the secondary analysis, the authors developed a coding structure for analysis with technology and occupation categories. The authors created technology categories with definitions adapted from Cook et al. (2020), a commonly used assistive technology textbook, and occupation categories adapted from the Occupational Therapy Practice Framework 4th Edition (AOTA, 2020). For example, initial technology categories were mainstream technologies and control interfaces.
To establish reliability in their coding structure, the authors reviewed 10 articles each and discussed their application of the codes. They adapted the technology codes and refined definitions to ensure clarity and consistency. For example, they created a category for “preparatory technologies” that helped individuals develop skills and was not reflected in the predetermined AT category codes. They also combined separate codes for reading, writing, and verbal communication supports into one category of “supplemental communication” for clarity. Multiple codes were assigned to articles, as appropriate, to represent the type of technology discussed. The authors met regularly to discuss data analysis processes and reach consensus.
Further, the authors added technology-related information to previously extracted data (i.e., type of article, purpose of the study, location of study, population demographics, research design, areas of occupation addressed, descriptions of technologies used) into an Excel spreadsheet used in the original scoping review. One author reviewed each article with a second author confirming extracted information and technology codes applied. Authors continued synthesizing the results through discussion and writing.
Results
The authors found 56 articles that met the inclusion criteria for the secondary analysis (Figure 1; Supplemental Table 1). Literature supporting technology use among adults with ID included representation from 10 countries and several international collaborations beyond those. The majority of included articles were research studies (n = 45); other articles were case descriptions, literature reviews, or position papers. There was a range of emphasis on technology in included articles. For example, 35 articles specified technology as part of the purpose with detailed descriptions, and eight articles only included brief mentions of technology, often in the article discussion (e.g., Lancioni et al., 2015; Williamson et al., 2017). The analysis yielded the following categories of technology: cognitive supports, mainstream technologies, supplemental communication, aids for daily living, seating and mobility, control interfaces, and preparatory technologies.
AT for Cognition
Adults with ID used AT devices to support cognition in 27 articles. Cognitive augmentation AT subcategories, adapted from Cook et al. (2020), included technology for prompting or cueing, tracking and identification, and time management.
Prompting cueing
The most common AT to support cognition for adults with ID was prompting or cueing technology that provided guidance for procedural or sequencing tasks. Seventeen articles included technology connected to activity analysis and routines to provide cues to initiate the next step or activity through visual or auditory prompts. Technology consisted of smart phones or PDAs with specialized apps such as video modeling, paper-based picture support, door sensors with alerts, or customized prompting systems (e.g., Cannella-Malone et al., 2017; Stock et al., 2011). Specialized prompting systems involved custom-made devices with sensors, lights, and pre-recorded verbal messages to enable adults with profound ID and multiple physical disabilities to engage in productive tasks with minimal staff support (e.g., Lancioni et al., 2015). The most common occupations for prompting technology were job performance and community mobility including using public transportation (e.g., Lancioni et al., 2015; Stock et al., 2011).
Time management
Four articles identified technology to assist with managing time, such as written or electronic schedules (e.g., Wennberg & Kjellberg, 2010). In addition to general schedule management, time management technology supported ADL, home management, and job performance including managing break time.
Tracking/identification
Three articles included adults with ID using devices to support problem-solving and safety through tracking and identification. Global positioning systems and location-tracking applications on mobile phones were the primary technology used to provide this type of cognitive support (e.g., Stock et al., 2011).
Mainstream Technologies
Adults with ID used mainstream technologies, defined as everyday technologies that are mass-produced and widely used by the general public, to support occupation in 22 articles (Cook et al., 2020). The most common occupations supported by mainstream technologies were health management (physical activity), leisure, work, and home establishment and management.
More than half of the articles in this category (14/22) incorporated the use of personal computers or smartphone technology, applications, and the internet. Adults with ID used computer software programs and internet applications (e.g., online bill pay) to establish and maintain their home (e.g., Waight & Oldreive, 2012). Smartphone applications and video modeling supported adults with ID to travel to/from work and school (Gentry et al., 2012). Video conferencing and telecommunication platforms (e.g., Skype™) were especially useful in helping adults with ID manage their health and social participation with peers remotely (e.g., Dew et al., 2013; Kramer et al., 2018).
Adults with ID used VR to promote exercise and leisure exploration in six articles (e.g., Lotan et al., 2011). Commercially available VR systems were most frequently employed.
Supplemental Communication
Adults with ID used supplemental communication technology to support expressive and/or receptive communication in 10 articles. Health management occupations were the most common purpose of supplemental communication technology for adults with ID in the literature. Specific technology, such as health advocacy tools, was only briefly mentioned (e.g., Williamson et al., 2017). Plain language translation to decrease the complexity of information was a mechanism to support receptive language (e.g., Yalon-Chamovitz, 2009). Photovoice to support expressive language involved providing adults with ID cameras to take photographs to answer questions during a research study (e.g., Jurkowski et al., 2009).
Aids for Daily Living
Aids for daily living refer to devices or tools that support participation and completion of daily life activities (e.g., activities of daily living (ADL) and instrumental activiites of daily living (IADL) including electronic and non-electronic AT and environmental modifications for the home (Cook et al., 2020). Of eight articles in this category, two articles focused on the use of various electronic technologies to enhance ADL safety and support transition from institutional settings to community living (Hammel et al., 2002; Naick, 2017). For example, adults with ID used sensors or other technology to assist with nighttime incontinence or request assistance.
Six articles described non-electronic technologies that supported ADL, home management, and mobility safety (e.g., falls prevention and injury reduction) in congregate and community-based settings (e.g., Finlayson et al., 2014; Pal et al., 2013). Examples of non-electronic assistive devices to improve safety with functional mobility included alarm mats, chair lifts, various types of walkers, helmet, transfer belts, and supportive footwear. To support participation in ADL, scholars noted adults with ID and their carers utilized technology such as adaptive shower equipment, emergency alerts and water temperature gauges, and raised toilet seats (Finlayson et al., 2014; Pal et al., 2013).
Control Interfaces
Seven articles described adapted interfaces that provided adults with ID with greater access to equipment and/or devices to support their occupational performance. Four articles provided detailed descriptions of switches and/or joystick systems installed on power wheelchairs to enhance functional mobility (e.g., Nilsson et al., 2011). An additional three articles included switches, mouse adaptations, or symbol recognition systems (combined with support from a facilitator) to help people with severe and profound and multiple intellectual disabilities gain greater access to their computers and engage in occupations (e.g., Waight & Oldreive, 2012).
Seating and Mobility Technologies
Technologies used to support the postural control, positioning, and mobility of adults with ID and physical disabilities were discussed in five articles. These articles highlighted the importance of providing power wheelchairs with customized trays, armrests, and seating systems to provide trunk stabilization for improved functional mobility and to increase community, social, and leisure participation (Hammel et al., 2002; Nilsson et al., 2011).
Preparatory Technologies
Seven articles described technologies used to support learning prior to engaging in occupations. These preparatory technologies included examples such as Snoezelen or other sensory systems or devices used to create or assess change to prepare for occupations including ADL, IADL, community mobility, and social interaction for play and leisure. More specifically, three articles described sensory interventions aimed to enhance attention and adaptive behaviors (e.g., Castehlhano et al., 2013). Two articles characterized assistive navigational devices, VR travel training, and other computerized video instruction to improve information access in preparation for personal and public transportation (e.g., Stock et al., 2011). Two articles illustrated how photographs, video clips, computer-based video games, and multisensory environments can be used to teach adults with ID socialization skills (e.g., Virji-Babul et al., 2011).
Discussion
The evidence on technology to support adults with ID most frequently identified AT to support cognition, mainstream or everyday technologies, and supplemental communication technologies. It was unsurprising that AT for cognition was the largest category of this secondary analysis given the characterization of ID as a cognitive disability. Adults with ID can use AT to enhance or supplement caregiver support (Lancioni et al., 2015; Naick, 2017). For example, Lancioni et al. (2015) created a specialized technology prompting system for adults with profound ID and multiple physical disabilities to engage in productive work tasks while minimizing the amount of direct support needed. Supplemental communication technologies, such as pictures and health passports, can help adults with ID manage their own health care and engage in social occupations (Hammel et al., 2002; Williamson et al., 2017). In addition to supporting cognition and communication for a variety of occupations, technology provides a means to participate in technology-focused occupations, such as using a smartphone or computer (Gentry et al., 2012; Waight & Oldreive, 2012).
In this secondary analysis, mainstream or everyday technologies supported multiple daily living categories. Adults with ID used combinations of high (e.g., smartphone applications, computers, virtual communication technologies) and low (e.g., visual schedules, picture exchange communication systems) technologies, contemporary and older technologies, technologies that had adapted interface capability, and those that did not (Jurkowski et al., 2009; Lotan et al., 2011; Waight & Oldreive, 2012). When recommending AT devices, occupational therapy practitioners should consider the accessibility of the technology and potential services to enable technology use (Canadian Association of Occupational Therapist [CAOT], 2012). The CAOT (2012) also affirmed occupational therapy practitioners should take stock of the contextual demands on AT use, and ethical issues in the application of AT including its potential to restrict participation and promote the use of AT to enhance occupational engagement, health, and well-being. Adults with ID may experience challenges learning and applying new technology and require additional support for its use due to cognitive impairments (Burke, 2017); therefore, occupational therapy practitioners should leverage their expertise to facilitate occupational performance with adults with ID through the selection, learning, and intentional application of AT (CAOT, 2012).
Due to the expeditious reproduction of commercially available technologies, mainstream AT devices have become more accessible to adults with ID and the occupational therapy practitioners who support them. However, recently developed technologies may be overly complex or overwhelming for adults with ID, which could inadvertently limit information access. Adults with ID may incur additional costs with the use of Smartphone devices, tablets, and computers (e.g., support applications, adaptations), leading them to use these ATs to a lesser degree or not to their full operability. A survey conducted in the U.S. in 2016 found that less than half of adults with ID (44.6%) used a tablet, smartphone, or another computer, and only 13.2% used social media (Patrick et al., 2020). Additionally, the perpetual evolution of mainstream technologies also means they become quickly outdated, as indicated by the technologies identified in this secondary analysis. Not only were the technologies used within the articles often antiquated but they were in some cases obsolete (e.g., iPod Touch).
While mainstream technologies (e.g., iPhone, Zoom, smart home technologies) are more available in high-income countries, inequities in access and funding for assistive technology still exist for adults with ID (World Health Organization [WHO], 2018). Only 1 in 10 people globally have access to the AT they need (WHO, 2018). A Pew Research survey (2021) administered prior to the coronavirus disease 2019 (COVID-19) pandemic found that only one in four US adults with disabilities had reliable access to WiFi, a smartphone, desktop, laptop, or tablet. Time delays and complexities with navigating the funding system are major barriers for adults with ID and their care communities, as well as occupational therapy practitioners. For example, U.S. federal programs that fund cell phone technologies for those with low incomes do not fund smartphones (Federal Communications Commission, 2021). The COVID-19 pandemic only deepened disparities in technology access making it nearly impossible for people with ID to connect virtually with necessary health care and therapy services, direct support services, and day, community, and social activities (Constantino & Sahin, 2020; Layton et al., 2021).
In the U.S. and Canada, a lack of federal legislation specific to AT has led to inconsistencies in obtaining much-needed AT for many adults with ID (National Academies of Sciences, Engineering & Medicine, 2017; Schreiber et al., 2017). In particular, adults with ID with limited financial resources and Black adults with disabilities experience challenges in procuring AT (Friedman & Rizzolo, 2017; Ward-Sutton et al., 2020). AT funding is also likely to exclude mainstream technologies, which means that only those adults with ID who can pay for these technologies out of pocket can access them. This “digital divide” contributes to employment disparities for these populations. With the passage of the U.S. Assistive Technology Act of 2004, most states now operate AT loan programs, and the Office of Vocational Rehabilitation and Medicaid Home and Community-Based Services (HCBS) Waiver increased AT funding (Braddock et al., 2015; Kitchener et al., 2008); however, provision of AT is still inconsistent from state to state. A national review of Canadian AT policy and funding similarly found inconsistent eligibility criteria and funding across federal, provincial and territorial governments for those with cognitive AT needs (Schreiber et al., 2017). Occupational therapists must become proficient in negotiating funding systems to connect adults with ID and their care communities to technology supports. Further, occupational therapy practitioners must take a strong role in advocating for consistent and potentially increased access to funding across states or provinces (CAOT, 2012).
Occupational therapy practitioners play an important role in supporting adults with ID to access and use AT devices. Major barriers to accessing AT for adults with ID include funding, decreased awareness of potential AT, and professionals not adapting assessment to the needs of adults with ID (Boot et al., 2018). Occupational therapy practitioners can address these barriers as our scope of practice includes assessing clients’ need for AT, making recommendations for AT devices that maximize occupational performance in a variety of contexts, and linking them with funding streams to obtain necessary AT (AOTA, 2010; CAOT, 2012). While evidence from this analysis suggests there is a role for occupational therapy in AT support, this role is not always explicitly discussed in the literature (e.g., Boot et al., 2018; Lancioni et al., 2015). It is imperative that occupational therapy practitioners access a range of resources, in addition to peer-reviewed research, to stay abreast of the newest available technologies to utilize in practice and to better understand their function to support people with ID.
Limitations
Inherent to secondary analyses of existing data, the available data are not collected to address the research question for the analysis; rather, the search terms and data addressed the original research question for which it was collected. While this means that some relevant articles were not included, this review captured articles with brief mentions of technology applicable to occupational therapy practice with adults with ID that likely would have been missed with technology-focused search strategies. Although articles published since 2018 were not included in this secondary analysis, the categories of technology support for adults with ID in the results will likely provide a useful structure to organize evidence from newer research and as new technology emerges.
Future Research
This secondary analysis demonstrates that there is likely sufficient research evidence to warrant a systematic review focused on technology supports for adults with ID. Research on AT for people with ID may not be keeping up with the production of new and evolving technologies. Consequently, these delays can quickly render research outdated or irrelevant, or miss the newest and best available technology options. Delays in publishing peer-reviewed research may also give the impression that older technologies are being used more frequently in research and clinical practice.
In wake of the evolving pandemic, there remains an opportunity for occupational therapy scholars to investigate the lasting impact of COVID-19 on technology use and accessibility. The pandemic not only underscored existing disparities in healthcare, it also emphasized differences in technology use and accessibility related to telemedicine and telerehabilitation.
Conclusion
This secondary analysis provides a snapshot of the current usage and availability of technologies for adults with ID and the occupational therapy practitioners who provide therapeutic services with this population. Literature suggests practitioners should include AT as part of the individual planning process, as technology-based interventions have demonstrated a benefit in improving the participation of adults with ID in a range of daily life activities. Likewise, environmental modifications, coupled with AT and related supports, enhanced participation for adults with severe/profound intellectual and multiple disabilities. While the articles included in this secondary analysis demonstrated that technology is a key support for occupational participation overall, specific implications remain for advancing technology use in occupational therapy practice, research, and policy and advocacy.
Key Messages
AT is an important way to support participation for adults with ID. In addition to traditional adaptive equipment, occupational therapy practitioners need to consider cognitive support, supplemental communication, and mainstream technologies.
The rapid reproduction of technologies can render tools utilized in occupational therapy assessment and intervention obsolete. That is, the assessments and interventions used by practitioners must evolve to include readily available technologies that adults with ID will use in their everyday lives.
Inaccessible funding for technology accessibility persists. Inclusive of connecting adults with ID to AT funding, occupational therapy practitioners should advocate for new funding mechanisms and policies that improve access through public and private reimbursement streams.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174231160975 - Supplemental material for Technology for Adults with Intellectual Disability: Secondary Analysis of a Scoping Review
Supplemental material, sj-docx-1-cjo-10.1177_00084174231160975 for Technology for Adults with Intellectual Disability: Secondary Analysis of a Scoping Review by Khalilah R. Johnson, Meghan G. Blaskowitz and Wanda J. Mahoney in Canadian Journal of Occupational Therapy
Footnotes
Acknowledgments
This paper was accepted as a poster presentation for the 144th annual meeting of the American Association on Intellectual and Developmental Disabilities which was canceled due to COVID-19. (1) Consulting librarians (David Nolfi and Ted Bergfelt, Duquesne University) for their work on the original scoping review. (2) Graduate assistants: Lindsey Wethington (Washington University St. Louis), Amy Castagnino, OTD (Duquesne University), and Emma Naegler, BS, OTD student (Duquesne University).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.