
Abstract
Introduction
Suicide safety planning (SSP) is an individualized approach aimed at reducing suicide risk by helping individuals to recall coping strategies and resources that can be drawn upon when suicide ideation occurs (Zonana et al., 2018). This approach is known by a range of names including “safety plan,” “crisis response plan,” and “coping cards,” and is typically a written document developed collaboratively between a service user and provider based on the person's own unique coping strategies and resources (Nuij et al., 2021). The most commonly known SSP has been developed by Stanley and Brown (2012) and includes six primary elements: (1) identifying warning signs of a suicide crisis; (2) internal coping strategies; (3) social supports that can distract from the current crisis; (4) contact information for these social supports; (5) contact information for health care services; and (6) reducing access to lethal means (Stanley & Brown, 2012). SSP was developed as a response to growing recognition that “contracting for safety,” an approach involving a verbal contract in which a service user agrees to avoid attempting suicide before reaching out for professional support, was largely ineffective for mitigating suicide risk (Bryan et al., 2017; Egan, 1997; Rudd et al., 2006). SSP is closely aligned with the values and culture of occupational therapy through its emphasis on collaboration and person-centered care (ACOTRO et al., 2021; Egan & Restall, 2022). As such, its use has been encouraged by occupational therapy scholars and the Canadian Association of Occupational Therapists (CAOT) (Hewitt et al., 2019).
Suicide and Its Impacts in Canada and Internationally
Suicide is a serious public health problem internationally and a leading cause of mortality worldwide (WHO, 2021). At least 700,000 individuals die by suicide annually and many more try suicide (WHO, 2021). In Canada, approximately 11 Canadians die by suicide every day, resulting in an estimated 4,000 deaths per year (Government of Canada, 2021). Suicide is a leading cause of mortality among Canadians and is the second leading cause of death among youth aged 15–34 (Government of Canada, 2021). While these prevalence rates raise alarm, they are particularly concerning when one considers that such estimates are low since suicide rates are often under-reported, and the quality of data internationally is known to be poor (WHO, 2021). The impact of suicide is even more concerning when one considers the deep and lasting impacts on individuals who are personally affected by the suicide of a family member, friend, or service user (Hvidkjaer et al., 2021; Kolves et al., 2020; Sandford et al., 2021). Suicide is a preventable and far-reaching public health problem that reverberates across individuals, families, communities, and societies. The broad scope of this issue highlights the need for prevention efforts to reduce overall suicide rates, and to limit impacts on society more broadly.
The Role of Occupational Therapy in Suicide Prevention and Intervention
Occupational therapists work with a range of individuals who are at increased risk of suicide, and it is imperative that the profession is knowledgeable about the effectiveness of existing approaches aimed at prevention, intervention and postvention. The losses associated with the onset of disability are frequently associated with suicide ideation (Khazem, 2018), and occupational therapists frequently support individuals who have been recently diagnosed. Further, occupational therapists support a range of populations who are at increased risk of suicide, including, but not limited to, persons living with mental illness (Windfuhr & Kapur, 2011), older adults (Holm et al., 2021), Indigenous persons (Ansloos, 2018), persons who experience homelessness (Fazel et al., 2014), veterans (Kashiwa et al., 2017), 2SLGBTQ+ persons (Hottes et al., 2016), youth (Kirby et al., 2020), persons living with physical disabilities (Khazem, 2018), and individuals who experience chronic pain (Racine, 2018). Often a person's health and social circumstances layer over one another to increase the likelihood that suicide ideation can occur. In a recent study exploring the experiences of persons living in low income during the first year of the COVID-19 pandemic, individuals who identified as living with a disability described how the social isolation introduced by the need for physical distancing caused them to feel so hopeless that they thought of pursuing medical assistance in dying to cope (Marshall et al., 2022). The emergent nature of suicide, combined with occupational therapists’ frequent interactions with individuals at risk emphasizes the critical importance that occupational therapists are both comfortable in discussing suicide, and have the foundational knowledge to respond when a suicide crisis occurs.
The role of occupational therapists in suicide prevention, intervention, and postvention has been acknowledged by the profession in Canada, and has resulted in the development of a recent role paper published by CAOT that describes how occupational therapists can support individuals who are at risk of suicide (Hewitt et al., 2019). One of the unique contributions of this document is its emphasis on the important relationship between meaningful activity engagement and suicide risk. Several studies have identified associations between meaningful activity engagement and suicide risk including research focused on youth (Ramey et al., 2010), inmates in correctional facilities (Senior et al., 2007), veterans (Bryan et al., 2015), and older adults (Conti et al., 2020) to name a few. Engagement in meaningful activity can promote resilience by helping to provide purpose and thereby overcome the hopelessness that is frequently a predictor of suicide ideation (Huen et al., 2015). A second key contribution of this role paper is its emphasis on suicide prevention and intervention through SSP.
What Is the Known About the Effectiveness of SSP Approaches?
While systematic reviews have focused on synthesizing literature on a range of strategies for suicide prevention and intervention (Witt et al., 2017; Zalsman et al., 2016), few have focused specifically on the effectiveness of SSP. One recent systematic review identified only six studies evaluating the effectiveness of SSPs, and after conducting a meta-analysis, the authors concluded that SSP reduced suicide behavior by 43% but was ineffective for reducing suicide ideation (Nuij et al., 2021). The inclusion criteria of this review were narrow, however, and included only studies that evaluated SSP as a standalone approach. Further, this study explored the effectiveness of the included interventions on only two key outcomes—suicide attempts and suicide ideation (Nuij et al., 2021). Occupational therapists frequently work in contexts in which complex approaches are required, and there is a need to understand the full scope of effectiveness studies in which SSP is either a standalone approach or a key component of a broader intervention. Further, there is a need to identify the components of a range of SSP approaches, including any occupational components, and their effectiveness on a range of psychosocial outcomes including and beyond suicide ideation and behavior. Identifying the range of approaches in which SSP is a key component, elements of these interventions, and their effectiveness on a broader range of psychosocial outcomes is necessary for informing occupational therapy practice and research within and beyond the profession in this area.
The Current Study
We conducted this review to synthesize the findings of effectiveness studies that have evaluated SSP, to summarize their various components, and report the effectiveness of these interventions on a range of psychosocial outcomes. Further, given the focus of existing occupational therapy literature on the relationship between meaningful activity engagement and suicide risk, it is important to understand how meaningful activity engagement has been incorporated in SSPs that have been evaluated in existing literature. This information is not only important for occupational therapists, but for the range of health and social care providers who may wish to consider incorporating meaningful activity in their support of individuals who experience suicide ideation. As such, the research question used to guide this review was: What are the effectiveness, quality, and components of SSP interventions evaluated within the existing experimental literature?
Methods
To synthesize the findings of existing empirical research, we conducted a systematic review of effectiveness studies using the method advanced by the Joanna Briggs Institute (JBI) (Tufanaru et al., 2017) following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2010). This method involves designing a search strategy, conducting a title and abstract screening and full-text review, critical appraisal, and narrative synthesis (Aromataris & Munn, 2017). Our review was registered prospectively with PROSPERO (CRD42020216597).
Search Strategy
We developed a search strategy in collaboration with an Academic Research Librarian, an author on this study (RI). We initially deployed our search in November 2020 and updated this search in December 2021. Following PRISMA guidelines (Moher et al., 2010), we searched five databases: Medline, PsycInfo, CINAHL, EMBASE, and Sociological Abstracts. We translated the search strategies using each database platform's command language, controlled vocabulary, and appropriate search fields using terms related to the concept of suicide (i.e., suicide, hopelessness, suicidal ideation), combined with terms pertaining to SSP (i.e., safety plan, crisis response plan, crisis plan) with a Boolean “AND.” In addition to this search, we hand searched the reference lists of all included articles to identify any additional studies not captured using our search strategy. A sample of our Medline search is provided in Appendix 1.
Study Selection
Acting as two independent raters, several members of our research team (CM, PC, DC, RG, JH, CE, and SM) conducted a title and abstract screening and full text review using Covidence, a cloud-based systematic review software program (VeritasHealthInnovation, 2016). A summary of inclusion and exclusion criteria used to guide the selection of studies is provided in Figure 1. Any conflicts emerging at the title and abstract screening and full-text review were resolved through discussion and consensus using at least two independent raters including the principal investigator (CM) and at least one other member of the research team.
Inclusion and exclusion criteria.
Critical Appraisal
Three members of our team (CM, JH, CE) acted as two independent raters and conducted a critical appraisal of each included study using the JBI Critical Appraisal Checklists for Randomized Controlled Trials (RCT) and Quasi-Experimental Studies (Tufanaru et al., 2017). We assigned a score of one to each criterion rated “yes,” and zero to items rated as “no” or “unclear.” After rating each study independently, we compared our ratings and through discussion, arrived at a consensus score. We converted the scores on each rating form to a percentage score between 0 and 100 to facilitate comparison as the total criteria scored on each form differs based on the form used and study appraised. When a criterion was not applicable to the study that we were appraising, we calculated a percentage based on a reduced number of overall criteria.
Data Extraction
Using a custom data extraction form developed in Covidence, three members of our team acted as two independent raters (CM, RG, JH) and extracted the following information for studies included in our review: study design; sample country; sample size, gender, age, race, sexual orientation; intervention name; comparator(s); outcome measures; and the reported effectiveness of the intervention on measured outcomes. Once data was extracted by two raters, we compared information entered, and resolved any conflicts through discussion and consensus.
Narrative Synthesis
The principal investigator (CM) arranged each intervention evaluated in included studies into like categories and presented these categories to other members of the research team. These categories were then refined further in response to these discussions. Included studies were: (1) arranged into tables corresponding to each intervention category; (2) summarized in a descriptive table; (3) described in detail narratively according to intervention type; (4) presented in a table according to their various components; and (5) presented visually according to the reported effectiveness of each intervention.
Findings
A total of 5,897 titles and abstracts remained following the removal of duplicates, of which 76 were subjected to full-text review. A total of 22 studies were included in our analyses and narrative synthesis. A summary of the study selection process and reasons for exclusion are provided in a PRISMA flow diagram in Figure 2.
PRISMA flow diagram.
Study Characteristics
The majority of studies included in this review represented samples of participants residing in the USA (n = 15; 68.2%), followed by Taiwan (n = 2; 9.1%). Of these, 12 were RCTs (54.5%), nine were quasi-experimental studies (40.9%), and one was a systematic review of effectiveness studies (4.5%). A summary of the characteristics of included studies is provided in Table 1.
Description of Included Studies (n = 22).
Note. Percentage sums do not all equal 100 due to rounding.
The number of participants identified in this table should be regarded as an estimate. Small inconsistencies in reporting race characteristics across studies resulted in a surplus of 45 participants beyond the reported sample sizes. These participants were removed from the “unspecified” category as they were assumed to have been reported more than once in the included studies. Otherwise, the total number of participants according to race would equal an additional 45 participants over the reported number of participants across studies.
Participant Characteristics
The studies included in this review represented 2,388 participants. A full summary of the characteristics of participants in included studies can be found in Table 1.
Critical Appraisal
Critical appraisal scores ranged from 38.5 to 92.3 (m = 63.7) representing a moderate-high quality of evidence overall. See Tables 2–4 for scores assigned to individual studies included in this review.
Standard and Enhanced Safety Planning Interventions (n = 11).
Note. I = intervention group; C = control group; RCT = randomized control trial; TAU = treatment as usual.
Electronically Delivered Safety Planning Interventions (n = 5).
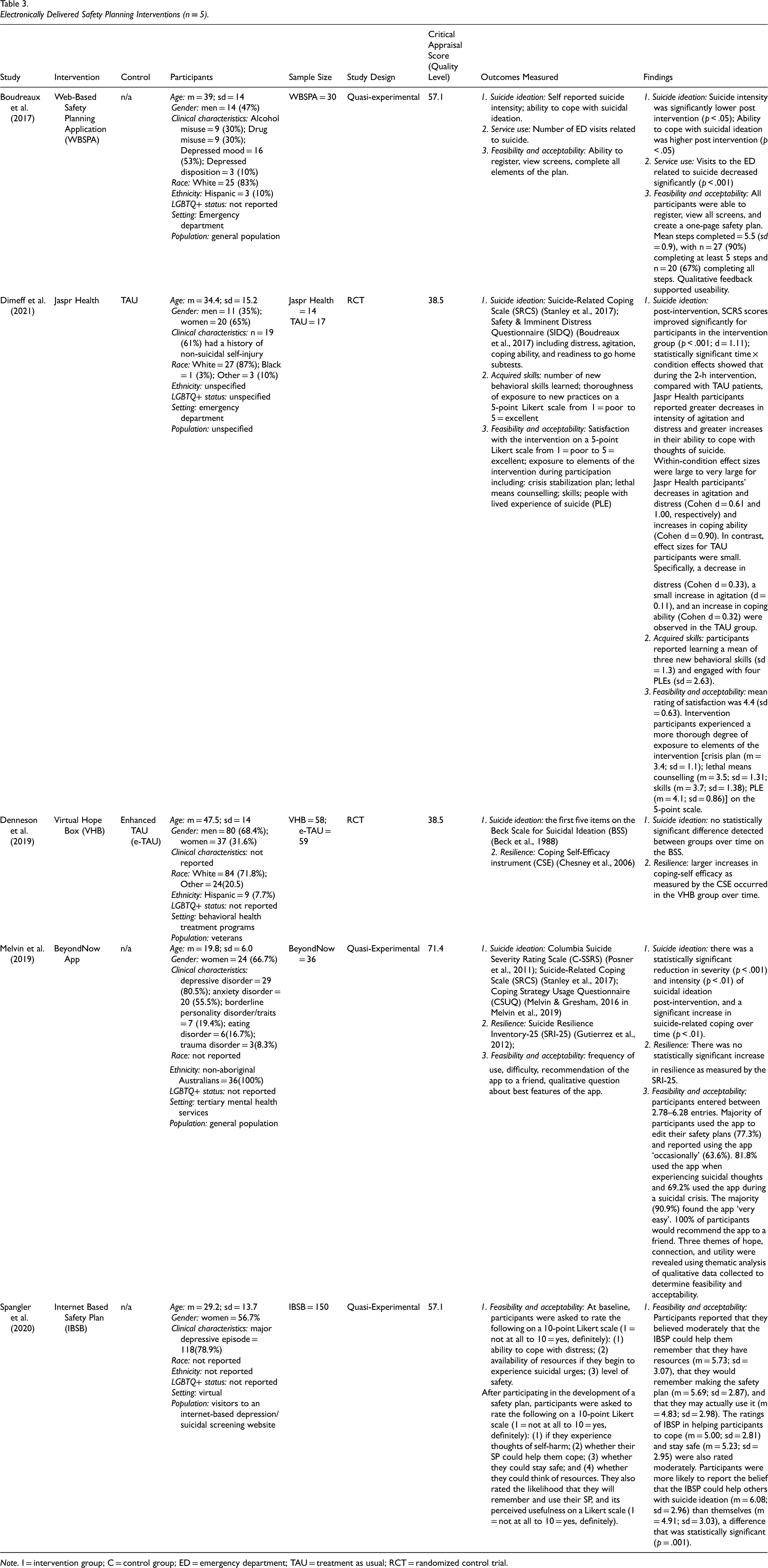
Note. I = intervention group; C = control group; ED = emergency department; TAU = treatment as usual; RCT = randomized control trial.
Safety Planning Integrated Within Complex Approaches (n = 6).
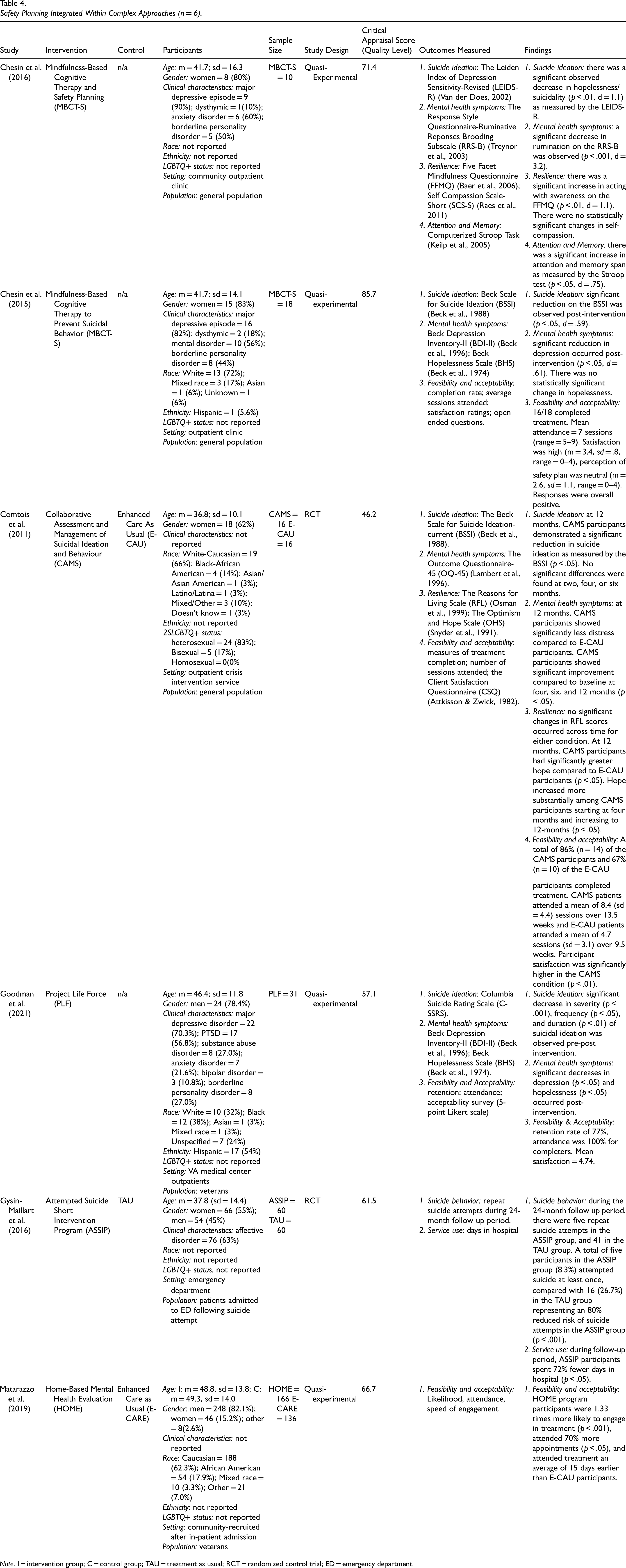
Note. I = intervention group; C = control group; TAU = treatment as usual; RCT = randomized control trial; ED = emergency department.
Narrative Synthesis
Studies were assigned to three intervention categories including: standard and enhanced SSP interventions (n = 11; 50%); electronically delivered SSP interventions (n = 5; 22.7%); and SSP integrated within complex approaches (n = 6; 27.3%). See Tables 2–4 for a detailed description of each study included in these categories.
Standard and enhanced SSP interventions
The most common interventions evaluated in the studies included in this review were standard (S-SSP) and enhanced (E-SSP) SSP interventions (n = 11). The critical appraisal scores of these studies ranged from 46.2–92.3 (m = 68.2) representing moderate-high quality evidence. See Table 2.
S-SSP and E-SSP interventions included in this category were called “crisis response plans” (Bryan et al., 2017, 2018a, 2018b; Rozek et al., 2019) and “safety plans” (Green et al., 2018; Stanley et al., 2015, 2020). S-SSPs included identification of warning signs, self-management and coping strategies, and social supports and healthcare professionals who could help during a suicide crisis. Four of these plans also included identifying crisis services (Bryan et al., 2017, 2018a, 2018b; Rozek et al., 2019), three included a component of reducing access to lethal means (Green et al., 2018; Stanley et al., 2015, 2020), and one included a component of identifying places that could serve as a distraction (Green et al., 2018). E-SSPs included the components included in S-SSPs, while also including verbal contracts for safety and identifying reasons for living (Bryan et al., 2017, 2018a, 2018b; Rozek et al., 2019).
SSPs in this category also included a crisis postcard intervention (CPI), in which participants collaborated with a case manager to identify individualized coping strategies, healthcare services, and crisis services on a wallet-sized postcard that they could refer to when thoughts of suicide emerged (Chen et al., 2013). They then received support from a case manager as they worked through a suicide crisis (Chen et al., 2013). In a similar intervention, individuals were provided with case management services and then engaged in sessions delivered over six weeks that helped them to develop individualized “crisis coping cards” (CCC) (Wang et al., 2016). These cards were small enough to be folded so they could fit into a wallet or pocket and consulted when a person had thoughts of suicide. Individuals engaged in this intervention received follow-up by phone or in-person depending on their preference (Wang et al., 2016). A final intervention called the Contract and Safety Planning (CASP) intervention was developed for use with individuals living in refugee camps (Vijayakumar et al., 2017). This intervention involves the use of community volunteers who meet with individuals who are at risk of suicide in refugee camps to engage them in the development of SSPs with added follow-up.
Electronically delivered SSP interventions
A total of five studies included in this review evaluated the effectiveness of electronically delivered SSP interventions (21.7%). The critical appraisal scores of these studies ranged from 38.5 to 71.4 (m = 52.5) representing moderate-high quality studies. See Table 3.
Interventions forming this category are newly developed approaches given that technology has enabled the development of research and practice in this area in recent years. These included: Web-Based Safety Planning Application (WBSPA) (Boudreaux et al., 2017); Jaspr Health (Dimeff et al., 2021); Virtual Hope Box (VHB) (Denneson et al., 2019); BeyondNow App (Melvin et al., 2019); and Internet Based Safety Plan (IBSP) (Spangler et al., 2020). All of these approaches included elements of SSPs designed to be delivered in-person, but in a virtual environment. While a range of SSP apps are available, WBSPA and Jaspr Health were designed for delivery in clinical settings (Boudreaux et al., 2017; Dimeff et al., 2021). The WBSPA integrates elements of the SSP developed by Stanley and Brown (2012) into a format that could be self-administered via computer within an emergency department rather than by clinical interview (Boudreaux et al., 2017). Jaspr Health integrates both a crisis stabilization plan and psychoeducation modules pertaining to suicide and mental health that are aimed at reducing reduce suicide risk while a person is accessing support in an emergency department for suicide ideation (Dimeff et al., 2021).
The BeyondNow App and IBSP similarly included the six elements typically included in the SSP designed by Stanley & Brown (2012), yet the BeyondNow app is designed to be self-administered via cell-phone app (Melvin et al., 2019), and the IBSP is designed to be self-administered over the internet (Spangler et al., 2020). A final intervention, VHB, aims to replicate the Hope Box intervention, an intervention that engages individuals in compiling items that enable recall of reasons for living and coping with suicide ideation (Denneson et al., 2019). The VHB replicates the physical Hope Box by providing an app in which the individual can save reminders of strategies for coping during periods of suicide ideation or emotional dysregulation. The benefit of a VHB over its physical counterpart is that a virtual hope box is portable, and is therefore easily accessible across multiple locations in which suicide ideation can occur (Denneson et al., 2019).
SSP integrated within complex approaches
A total of six studies included in this review evaluated the effectiveness of SSP interventions that were integrated within other approaches (27.3%). Critical appraisal scores ranged from 46.2 to 85.7 (m = 64.8) representing moderate-high quality evidence. See Table 4.
Interventions in this category included Mindfulness-Based Cognitive Therapy with Safety Planning (MBCT-S) (Chesin et al., 2015, 2016), Project Life Force (PLF) (Goodman et al., 2021), Attempted Suicide Short Intervention Program (ASSIP) (Gysin-Maillart et al., 2016), Home-Based Mental Health Evaluation (HOME) (Matarazzo et al., 2019), and Collaborative Assessment and Management of Suicidal (CAMS) ideation and behavior (Comtois et al., 2011).
MBCT-S and PLF are both group-based interventions. MBCT-S is a structured approach developed by Chesin et al. (2016) that combines Mindfulness-Based Cognitive Therapy (MBCT), an evidence-based intervention integrating both principles of mindfulness and cognitive behavioral therapy, with the six-component SSP intervention introduced by Stanley & Brown (2012). PLF was developed to assist veterans to manage suicide risk by developing five key skills: (1) managing aggression and impulsivity; (2) managing medication and adhering to treatment; (3) emotion regulation to alleviate psychological distress and hopelessness; (4) reducing access to lethal means; and (5) asking for support and help (Goodman et al., 2021). Six of the 11 sessions included in this group intervention are dedicated to each of the six components of the SSP developed by Stanley et al. (Stanley & Brown, 2012), making SSP a core component of this intervention.
ASSIP, HOME, and CAMS are designed to be delivered individually. ASSIP was developed as a 3–4 session brief protocol for supporting individuals through a suicide crisis (Gysin-Maillart et al., 2016). In the first session of ASSIP, a health professional conducts a narrative interview with the person at risk of suicide to understand their experience and factors related to suicide ideation. This interview is video recorded. In the second session, the health professional plays back parts of the video recorded session to reactivate the person's psychological state at the time of the suicide crisis. During this time, the health professional supports the person to emotionally process their experiences and to begin planning to manage thoughts of suicide. In the third session, the person develops a structured SSP with the health professional that includes long-term goals, warning signs, and safety strategies (Gysin-Maillart et al., 2016). A fourth session is added for ongoing support should the health professional or service user deem that this is necessary (Gysin-Maillart et al., 2016).
HOME is an intervention designed to assist veterans who have been hospitalized for suicide attempts and/or ideation (Matarazzo et al., 2019). In this intervention, a health professional meets with the person in hospital, and provides support during and following discharge. The health professional introduces SSP using the six components introduced by Stanley et al. (2012), and collaborates with the service user to ensure that information on the plan is updated throughout the intervention process (Matarazzo et al., 2019). Finally, in CAMS, a mental health clinician provides counseling to support a person through a suicide crisis. This support is accompanied by identification of individual triggers that elicit suicide ideation. These triggers are captured on a suicide status form (SSF), which is used for collaborative and ongoing assessment and treatment planning (Comtois et al., 2011).
Intervention Components
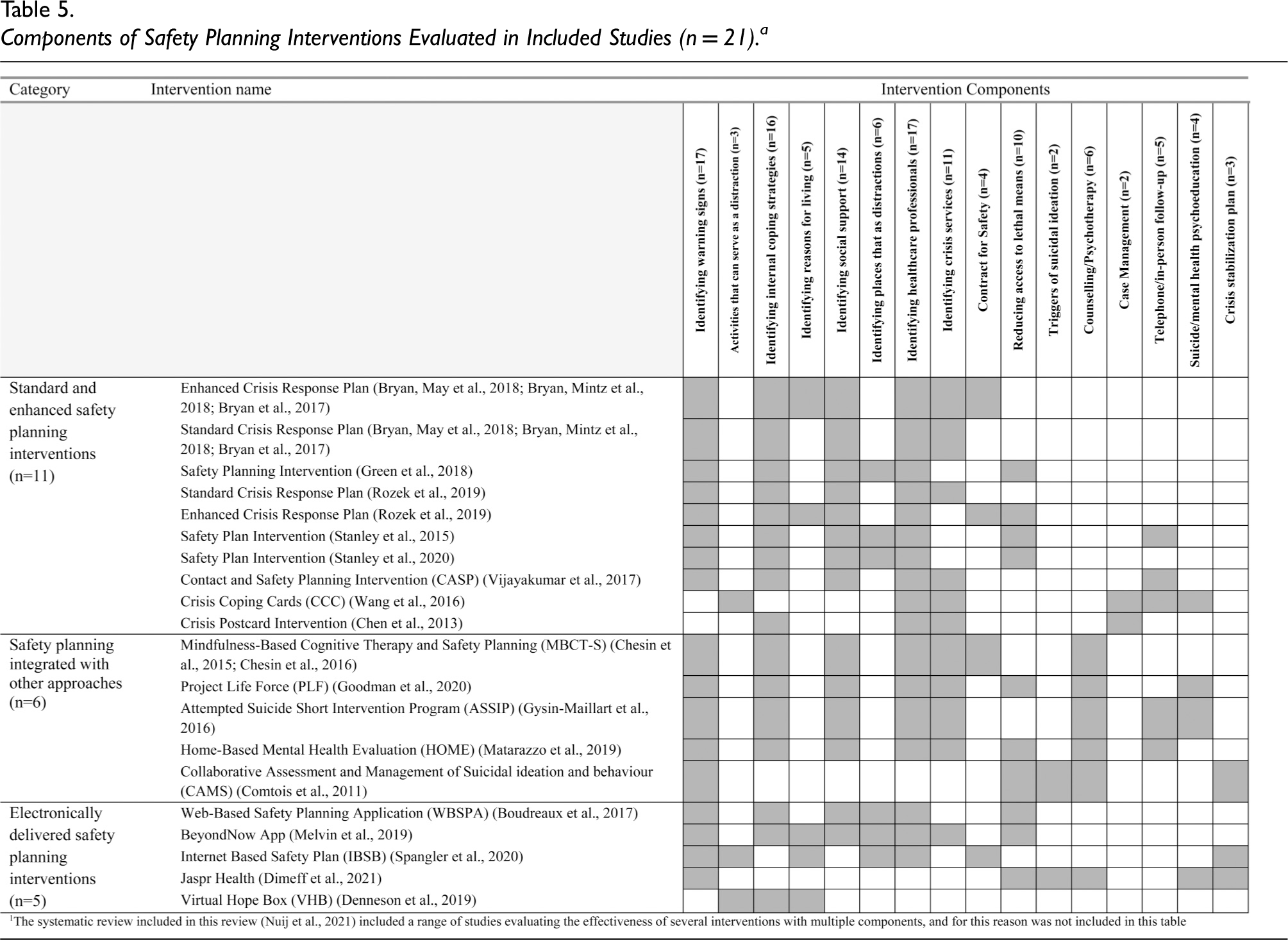
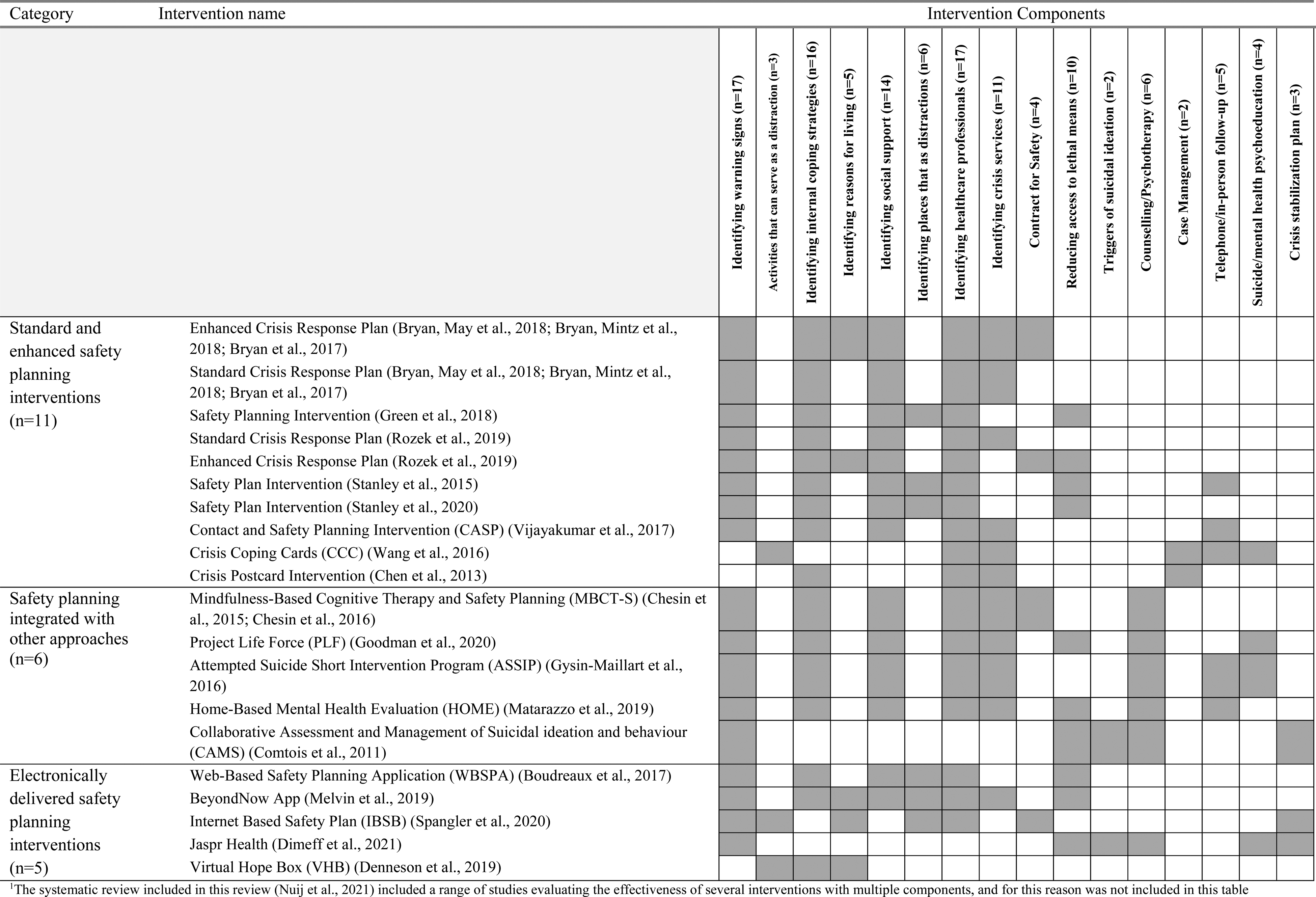
To describe the various components of each included intervention to inform practice and future research, we summarized the various components of each intervention in Table 5. Of the 16 components of safety planning in the included studies, the most common component used was “identifying warning signs” of a suicide crisis (n = 17 interventions) and “identifying healthcare professionals” that could be accessed (n = 17 interventions). The least common components were “case management” (n = 2 interventions) and ‘triggers of suicide ideation’ (n = 2). Only three interventions evaluated in the included studies involved a component related to meaningful activity engagement (i.e., “activities that can serve as a distraction”): CCC (Wang et al., 2016); IBSB (Spangler et al., 2020); and VHB (Denneson et al., 2019).
Components of Safety Planning Interventions Evaluated in Included Studies (n = 21).a
Effectiveness of Included Interventions on Key Outcomes
In addition to our narrative synthesis of included studies, we have provided a visual summary of the effectiveness of these interventions in terms of key psychosocial outcomes in Table 6. Overall, existing moderate-high quality studies that have evaluated the effectiveness of suicide safety planning interventions have demonstrated effectiveness for suicide ideation (n = 7 studies), suicide behavior (n = 7), mental health symptoms (n = 5), resilience (n = 2), and service use (n = 4). Table 6 details the specific studies and their effectiveness on each of these outcomes.
Summary of Intervention Effectiveness on Suicide Ideation and Behavior, Mental Health Symptoms, Resilience, and Service Use (n = 22).
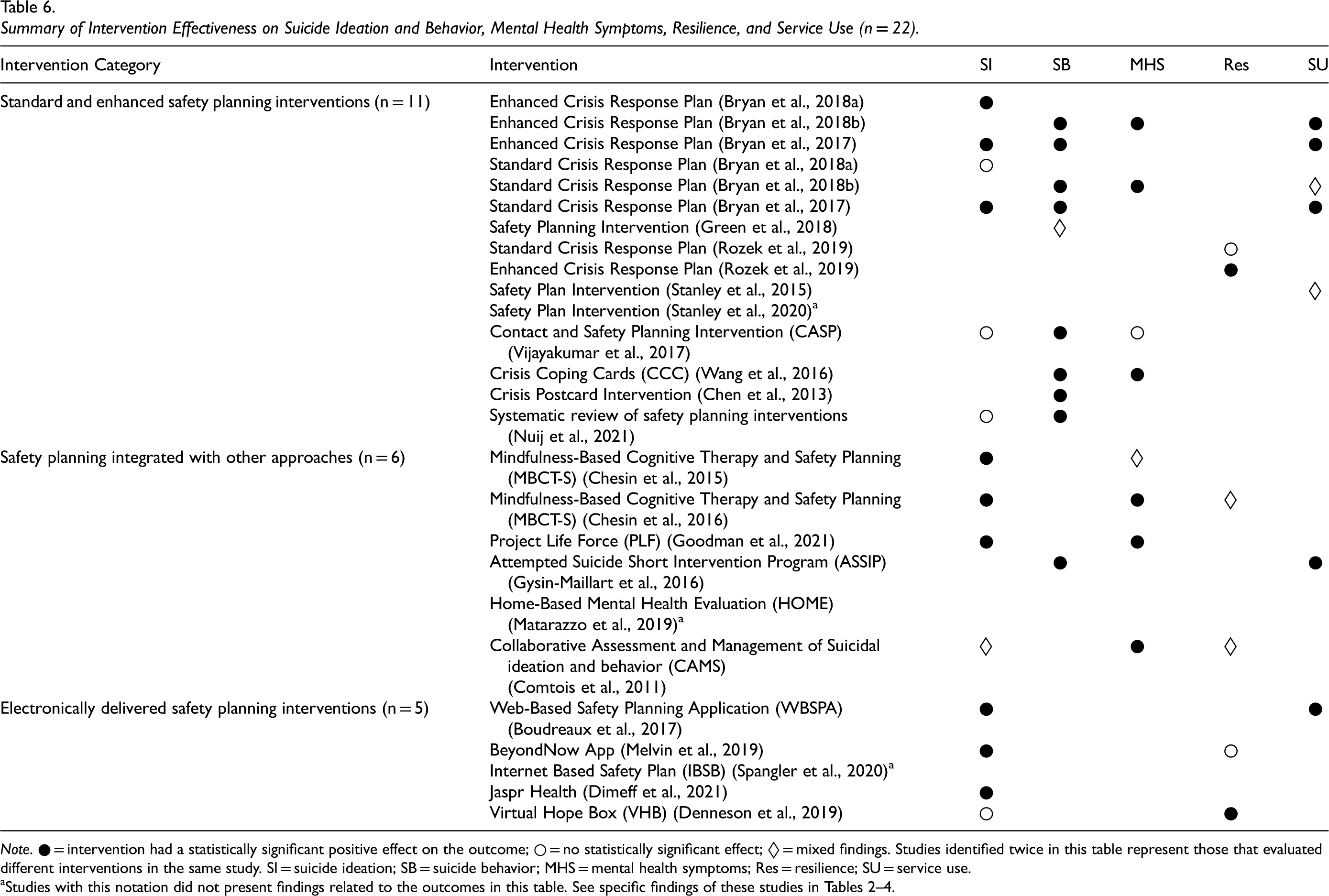
Note. ● = intervention had a statistically significant positive effect on the outcome; ○ = no statistically significant effect; ◊ = mixed findings. Studies identified twice in this table represent those that evaluated different interventions in the same study. SI = suicide ideation; SB = suicide behavior; MHS = mental health symptoms; Res = resilience; SU = service use.
Discussion
Occupational therapists support individuals who experience suicide ideation in a range of practice areas (Hewitt et al., 2019). For this reason, developing and maintaining competence as an occupational therapist in the use of evidence-based interventions for mitigating suicide risk is important across practice settings. By conducting this review, we identified and evaluated a range of studies that addressed standalone SSP interventions, electronically delivered SSPs, and complex interventions that include SSP. The findings from the current review indicate that SSP is an established evidence-based approach for reducing suicide behavior; a finding that also emerged from another systematic review (Nuij et al., 2021). While Nuij et al.'s (2021) meta-analysis suggested that suicide ideation is not effectively targeted by SSP, results from our review indicate that a range of SSP interventions are effective for targeting suicide ideation (Boudreaux et al., 2017; Bryan et al., 2017, 2018a; Chesin et al., 2016; Chesin et al., 2015; Dimeff et al., 2021; Goodman et al., 2021; Melvin et al., 2019). Other outcomes, however, including resilience and service use, have yet to be studied extensively, and therefore, we cannot draw conclusions concerning their effectiveness at this time.
The majority of studies included in this review were published in the United States, followed by Taiwan. Only one of the included studies was conducted in Canada, and none were conducted with or by occupational therapy researchers. Researchers in Canada and other countries may consider conducting effectiveness studies of SSP interventions that reflect the unique cultural and service contexts of their countries to generate data on the effectiveness of these approaches across a range of contexts. Conducting this research will provide critical data for informing both policy and practice for mitigating suicide risk, and will lead to the development of SSP approaches that reflect the cultural and service contexts in which they are used.
Although the profession of occupational therapy has encouraged the use of SSP for mitigating suicide risk (Hewitt et al., 2019), none of the included studies were published by occupational therapy scholars. Only three of the included studies incorporated activity engagement in their SSP, and these studies identified activities as a “distraction” (Denneson et al., 2019; Spangler et al., 2020; Wang et al., 2016). While it is encouraging from an occupational therapy perspective that this component was included in some studies, little is known about the contribution of meaningful activity engagement for mitigating suicide risk. While we recognize that activity could be an important distraction from SI, future research exploring the inclusion of meaningful activity in SSPs should account for the meaning attributed to the activity itself, and the ways in which it may mitigate SI and SB. Theoretically, it makes sense that meaning might be a remedy for the hopelessness that is a frequent precursor to SI (Baryshnikov et al., 2020). Occupational therapy researchers should consider the framing of meaning within future occupation-focused research in this area. While we recognize that components of the interventions included in this review might implicitly incorporate a focus on meaningful activity engagement (e.g., coping), future occupational therapy research on SSP should make these components explicit to enable scholars and practitioners within and beyond the profession to evaluate the contribution of meaningful activity on key psychosocial outcomes.
Seven of the included studies incorporated existential components, including reasons for living (Bryan et al., 2017, 2018a, 2018b; Denneson et al., 2019; Melvin et al., 2019; Rozek et al., 2019; Spangler et al., 2020). In at least one of these studies, suicide ideation was more effectively targeted by E-CRP, which added the component of identifying reasons for living (Bryan et al., 2018a). This evidence suggests that including such existential elements are an important and worthy direction for future research to enhance the effectiveness of SSP for addressing SI (Nuij et al., 2021). For example, an SSP called the “Living Safety Plan” has been developed by an author on the current study (DC), which includes collaborating with a service user on developing a mission statement of one's life (Carmichael, n.d.). This plan has been adapted by another occupational therapist, who developed the “Suicide Safety Plan for Occupational Engagement and Recovery” (SSP-OEAR) (Straathof, 2022). These plans have yet to be formally evaluated empirically. Further, research aimed at identifying associations between meaningful activity engagement and suicide risk is needed to inform ongoing development of SSP interventions.
Practice Implications
The findings of this review indicate that SSP is an important and evidence-based intervention for addressing SI and SB. Occupational therapists who currently use SSP should be reassured that their use of this approach is supported by evidence, and those who are unfamiliar with this intervention may consider training opportunities to deliver SSP as part their practice. University educators in entry-level occupational therapy programs should be aware of the need for incorporating SSP in their curriculum to prepare graduates with the skills needed to intervene when service users express thoughts of suicide. Occupational therapists who are familiar with SSP and have been developing these plans with service users in analog format (paper and pencil) may consider incorporating electronically delivered SSPs based on evidence of their effectiveness from this review. Using electronically delivered approaches, such as software applications, may be more amenable to some service users and provide additional options for person-centered care. Finally, incorporating an occupational perspective and existential components into one's SSP approach may enhance its effectiveness, while aligning more closely with the core occupational values of the profession (Egan & Restall, 2022).
Policy Implications
Policymakers should be aware of existing evidence that support the use of SSP for mitigating suicide risk. While only a handful of the included studies explored service use as an outcome, two studies identified that individuals who were supported using SSP spent fewer days in hospital and had shorter inpatient stays than those using the traditional CFS (Bryan et al., 2017; Gysin-Maillart et al., 2016). While more research is needed to determine whether the use of SSP decreases the need for inpatient services across a range of studies, policymakers should be aware of the potential for decreasing the overall cost of care, while improving the lives of persons who experience suicide ideation through implementing the use of SSP across programs. Policymakers at provincial and federal levels may consider: (1) allocating funding for training health and social care professionals, including occupational therapists, in SSP; and (2) dedicating funding for the conduct of effectiveness research in a Canadian context.
Limitations
While our search was comprehensive, there is a possibility that with any scoping or systematic review that our search strategy may have missed some studies. Readers should be aware that the findings of this review primarily represent the effectiveness of SSP primarily in a US context, and findings should be interpreted accordingly. Further, the findings of existing studies represent the effectiveness of these approaches primarily for individuals who identify as men and women. Persons identifying with other genders have been largely underrepresented by the findings of this review. Similarly, included studies represent the effectiveness of SSP for persons who are primarily White and who have not explicitly identified as 2SLGBTQ+. As such, the findings of this review should be interpreted with caution.
Conclusion
SSP is an evidence-based intervention for mitigating suicide risk. Such interventions need to be encouraged in occupational therapy (Hewitt et al., 2019). Occupational therapists support individuals who are at risk of suicide in range of practice contexts, and for this reason, SSP should be incorporated into education and practice. SSP interventions that incorporate existential and occupational components may be promising additions for improving effectiveness on addressing suicide ideation. Researchers may consider designing novel interventions that incorporate these components and evaluate their specific contributions on indices of psychosocial well-being. Given this evidence, policymakers should ensure that occupational therapists and others working with at risk populations receive the training and support needed to deliver SSP within their practice.
Key Messages
Occupational therapists support persons at risk of suicide ideation (SI). Competence in the delivery of evidence-based approaches that address SI is critical.
Suicide Safety Planning (SSP) is an evidence-based approach that reduces suicide behaviors, yet evidence is mixed regarding its effectiveness for managing SI.
Occupational therapy researchers and practitioners should consider strategies for incorporating meaningful activity engagement in SSPs and evaluating the respective contribution of occupation-focused approaches with at-risk populations.
Supplemental Material
sj-docx-1-cjo-10.1177_00084174221132097 - Supplemental material for Effectiveness of Suicide Safety Planning Interventions: A Systematic Review Informing Occupational Therapy
Supplemental material, sj-docx-1-cjo-10.1177_00084174221132097 for Effectiveness of Suicide Safety Planning Interventions: A Systematic Review Informing Occupational Therapy by Carrie Anne Marshall, Pavlina Crowley, Dave Carmichael, Rebecca Goldszmidt, Suliman Aryobi, Julia Holmes, Corinna Easton, Roxanne Isard and Susanne Murphy in Canadian Journal of Occupational Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an internal grant provided to the principal investigator by Western University (Grant number: R5840A03).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.