
Abstract
Introduction
Driving can enable social participation, provide access to essential community-based services, and symbolizes identity and independence (Finestone et al., 2010; Mountain et al., 2020). Within occupational therapy and occupational science literature, driving has been framed as a significant occupation throughout the life course (Liddle et al., 2009; Patomella et al., 2009; Vrkljan & Polgar, 2007). However, changes in medical status can call driving ability into question. In the event of stroke, individuals can experience sensorimotor and cognitive-perceptual impairments that may influence driving ability (Perrier et al., 2010). Accordingly, many jurisdictions recommend a period of driving restriction following stroke, including within Canada (Canadian Council of Motor Transport Administrators [CCMTA], 2020), Australia (Austroads, 2017), the United Kingdom (Driver and Vehicle Licensing Agency, 2021), and various parts of the United States (Winstein et al., 2016). While a review conducted by Perrier et al. (2010) indicated that stroke carries a twofold increased risk of motor vehicle collision (MVC), a more recent systematic review by Rapoport et al. (2019) did not find a significant increase in MVC risk. Based on their findings, Rapoport et al. (2019) suggested healthcare professionals (HCPs) use a combination of evidence-based assessment tools alongside their clinical judgment when evaluating driving risk, rather than recommending driver restrictions based only on a diagnosis of stroke. Nonetheless, as stroke does have the potential to impair driving ability, it is important this occupation is assessed by HCPs due to the potential consequences to both personal and public safety.
Within Canada, initial fitness to drive determinations following stroke can occur in acute stroke settings (Mountain et al., 2020). Although the occupation of driving is addressed along the continuum of care, it is within acute care that discussions about driving may first arise. In accordance with Canadian Stroke Best Practice Guidelines, it is recommended that individuals with stroke be advised in acute care to abstain from driving for 30 days and only resume driving in the absence of functional impairments or medical conditions that could influence their fitness to drive (CCMTA, 2020; Mountain et al., 2020). Consequently, it can be the responsibility of the interdisciplinary acute stroke team to provide clients with initial education about return to driving following stroke. In this context, occupational therapists can play an important role in communicating recommendations for driver cessation post-stroke, which is a contentious issue for many clients (Patomella et al., 2009) and may create tensions for occupational therapists if systems do not provide resources that address the occupational implications of driving cessation.
As many countries worldwide stipulate a 30-day driving restriction post-stroke, research examining client adherence to abstain from driving has emerged (Frith et al., 2015, 2020; Frith et al., 2017b; Yu et al., 2016). More specifically, this body of research seeks to estimate the extent to which individuals contravene the 30-day driver restriction, with recent studies suggesting between 26% and 38% of clients return to drive against medical advice (i.e., before 30 days post-stroke) (Frith et al., 2015; Frith et al., 2017b; Yu et al., 2016). Given the potential risk to personal and public safety, research investigating adherence to driving restrictions and the efficacy of practice initiatives that support adherence is warranted.
Adherence is often conceptualized as an individual behaviour, understood through a dichotomous framing, that is, as a correct decision reflecting appropriate understanding and rational compliance or an incorrect decision reflecting misunderstanding or wilful resistance (Dennhardt & Laliberte Rudman, 2012). Alternate perspectives that attend to the complexity of conditions that inform return to driving post-stroke may provide useful insights for research and occupational therapy practice
In parallel to other papers calling upon occupational therapists to be critically reflexive regarding how policies might affect clients (e.g., Aldrich & Rudman, 2020; Pereira & Whiteford, 2013), this paper explicates the dominant ways driving against medical advice has been conceptualized and examined, and the implications for occupational therapy practice with clients facing driving restriction in the first 30 days following stroke. This critical reflexivity is informed by an analysis of research addressing driving adherence, as well as the first author's practice in acute stroke care. We propose that a transactional perspective of occupation can create space for understanding driving after stroke as a situated occupation. This reconceptualization provides a productive basis for reconfiguring how occupational therapists must consider recommending driver restrictions following stroke, and outlines directions for advocacy to support system changes that address conditions shaping differential possibilities for adherence. Although the focus of the paper is on the 30-day period driver restriction that is recommended by driver standards and stroke best practice guidelines (CCMTA, 2020; Mountain et al., 2020), given the limited amount of research focused on this period, we draw on research addressing client experiences of driving along the care continuum to conceptualize driving as a situated occupation. By considering driving as an occupation, the complex transactions that can shape return to driving post-stroke are discussed. In doing so, this paper illustrates how concepts from occupational science can generate new insights for scholarly inquiry and occupational therapy practice.
Reflexivity Statement
The first author is an occupational therapist in acute stroke care and a PhD student studying occupational science. Hence, there is a tension reflected in these respective roles between the pervasive biomedical perspective that is often foundational to clinical practice in a hospital setting, and a central argument in this paper to question its dominance. By occupying the space between these roles and corresponding tensions, the aim is to make the implicit explicit regarding the complexity of addressing driving after stroke (Corbin Dwyer & Buckle, 2018). The second author is an occupational scientist and occupational therapy academic whose work has aimed to raise critical awareness of the boundaries of individualistic conceptualizations of occupation and the practices they promote (Laliberte Rudman, 2021). This paper provided an opportunity to consider how a transactional perspective of occupation as situated, that is, as implicated within social, political, cultural, economic, and other contextual features (Laliberte Rudman, 2021) can inform a particular practice challenge within occupational therapy.
Individualistic, Biomedical Conceptualizations of Driving Against Medical Advice
Immersion in the literature regarding driving against medical advice post-stroke while simultaneously examining paradigm stances in the study of occupation enhanced the first author's awareness of the dominant individualistic, biomedically oriented lens underpinning this research. After explicating this lens, we illustrate how it has dominantly framed research in this area and point to how the questioning of this lens, and its underlying assumptions, can serve to disrupt dominant ways of thinking about and addressing driving cessation post-stroke and create new ways of addressing this issue (Laliberte Rudman, 2021). Finally, we will discuss how an individualistic, biomedical perspective intersects with the first author's research, which lead to critical reflection and revised assumptions.
What is an Individualistic, Biomedical Perspective?
An individualistic paradigm focuses on individual experiences and actions, locating “social issues and phenomena, including occupation, as primarily residing in and being shaped through individuals” (Gerlach et al., 2018, p. 36). For example, in an individualistic perspective, driving is conceptualized as an individual experience and choice with little recognition of social and environmental factors that influence participation. Within an individualistic perspective, driving is framed as something individuals can freely choose to not do, and the ways in which inequities in this choice are constructed through broader contextual features, such as the availability of public transportation, differential distribution of opportunities to work at home, or the design of urban centres, are obscured. Applied to research, individualism can lead to a focus on individual attributes, such as knowledge, attitudes, and behaviours, rather than the larger “experiential whole” (Dickie et al., 2006, p. 82). Individualism is well-aligned with biomedical perspectives of health, given that the unit of study and target of health intervention from biomedical perspectives is the individual (Gerlach et al., 2018). Biomedical perspectives seek to understand person-level facets of health and disease, and like individualistic ideologies, do not wholly consider the broader sociopolitical determinants of health (Gerlach et al., 2018). Given the pervasiveness of an individualistic, biomedical perspective within health care and academia (Gerlach et al., 2018), it is not surprising that one can readily locate such a perspective in stroke and driving research.
Examples of Individualistic, Biomedically Located Research: Advice and Adherence
Driving against medical advice conceptualized and studied from an individualistic, biomedical perspective often leads to a focus on adherence to driving cessation and individually focused solutions to increase compliance. While the research to enhance client and public safety are vital, a narrow focus on individual factors to understand adherence can perpetuate partial understandings and contribute to incomplete and ineffective solutions. For example, in a study including 359 participants aged 18–65 years of age within 28 days of experiencing stroke, Yu et al. (2016) primarily focused on individual-level factors to examine correlates of lack of adherence among stroke survivors. These authors found that several individual-level factors, such as male gender, cognitive impairment, previous employment as a primary income earner, independence in activities of daily living, and no recollection of advice to abstain from driving, were associated with driving against medical advice (Yu et al., 2016). While some contextual factors were included; for example, geographic location, availability of health insurance benefits, marital status, and number of financially dependent children, the majority of explanatory factors examined were individual-level characteristics. Moreover, the suggested recommendations were similarly focused on individuals, namely, enhancing adherence by ensuring appropriate client education in acute care (Yu et al., 2016), which frames the problem as a lack of knowledge and understanding on the part of individual clients. The systematic review by Frith et al. (2015) which addressed adherence to driver cessation post-stroke, identified that less than 50% of clients are informed in acute care to abstain from driving post-stroke (Frith et al., 2015). The authors posited that a lack of education provided by health professionals influences return to driving against medical advice. In their follow-up study that addressed the knowledge of health care providers (the majority of which were occupational therapists), these authors found that only 22% of respondents were aware of the driving restrictions post-stroke, and that a lack of role clarity resulted in professionals deferring the responsibility of addressing driving to others (Frith et al., 2020). A key recommendation from the study was that better education of health care providers can improve client education, which in turn, affects adherence to driving cessation. Their focus on the education of individual therapists, while moving beyond a focus on individual clients, still locates the problem within individuals and their lack of knowledge. This focus is exemplified in the development of an e-learning module designed to arm health professionals with best practice guidelines to encourage clients to maintain the 30-day driver cessation post-stroke (Frith et al., 2017a). Certainly, supporting the practice of clinicians is vital, and such interventions are warranted. However, providing education to clinicians and focusing on ensuring clients are educated, we suggest, will not necessarily or automatically resolve issues of adherence. Attention must also be paid to the complex contextual conditions surrounding driving adherence.
Assumptions and Shortcomings of an Individualistic, Biomedical Perspective
An assumption embedded in an individualistic, biomedical perspective is that if health care providers are aware of the restrictions and communicate them to the clients, clients would not drive against medical advice. A client does need to be aware of a restriction to abide by it, but there is an underlying assumption about risk in this perspective, often labelled a techno-scientific perspective on risk (Dennhardt & Laliberte Rudman, 2012), that can perpetuate partial understandings. Namely, once a risk is identified and understood, there is a universal, logical way to mitigate that risk that is processed and understood the same way by all individuals. In this example, the risk is a MVC following stroke, and the mitigation is well-informed health professionals providing education to clients, who will in turn, abstain from driving. This notion of education to prevent driving against medical advice assumes that individuals aware of risk will act as independent, rational agents and make decisions removed from any sociocultural and historical-political influences. It also assumes that all individuals have equitable access to the resources and conditions to make such decisions, or at least neglects how differential distribution of resources and conditions might create inequitable access (Dennhardt & Laliberte Rudman, 2012). An individualistic, biomedical perspective also posits that driving against medical advice is located within individuals; that is, if one drives against medical advice, it was an oversight of a health professional or the personal choice of a wilfully defiant client (Dennhardt & Laliberte Rudman, 2012).
Through a process of critical reflexivity, the first author identified the same assumption—that if health care providers and clients were given appropriate education, driving against medical advice would “naturally” reduce—underlying her own research. In a pilot study, evaluating an occupational therapy practice resource for addressing driving after stroke, clients were provided with detailed information about driving restrictions both verbally and in writing (Vander Veen et al., 2021). At follow-up, the vast majority (90%) of participants recalled instructions provided in acute care. Unfortunately, recall did not appear to translate into increased adherence. After receiving the best practice education and driving advice, 29% of clients drove earlier than 30 days (29%; n = 4/14), which corresponds to the lower range of previously published estimates (Frith et al., 2015, 2017; Yu et al., 2016). While these results are from a pilot study and cannot be generalized to other contexts, it was a catalyst for critical reflection. Moreover, another insight from that study was the impetus for broadening perspectives on driving after stroke. Clients were asked why they returned to driving against medical advice. The answer was almost unanimous, “I didn't have another choice”. This single finding highlighted the need to reflect on notions of “choice” and how it intersects with abstaining from driving.
Transactional Perspectives in Occupational Science
Drawing on transactional perspectives on occupation developed through occupational science scholarship can provide a way to expand beyond an individualistic, biomedical perspective on driving against medical advice. Dickie et al. (2006) introduced a “transactional perspective on occupation” as a way to move beyond individualistic conceptions of occupation. Over time, diverse aspects of pragmatism, particularly as forwarded by Dewey, have been taken up to develop transactional perspectives on the occupation that extend beyond person-context dualisms pervasive in individualistic perspectives and attend to the “continuity of humans and their environments” (Cutchin & Dickie, 2013, p. 2). Occupations are conceptualized as situated, that is, as embedded within and contributing to dynamic, complex contexts and analysed from “a holistic view of people acting in the world” (Cutchin & Dickie, 2012, p. 27). Transactional perspectives of occupation suggest a continuity of individuals and environments, such that they are necessarily shaped and shaped by each other. Within these ongoing transactions, occupations are an important form of “functional coordination” of person and world (Cutchin et al., 2008; Cutchin & Dickie, 2012, 2013). Accordingly, occupations are inherently transactional, as they are the product of coordinated, ongoing restructuring of the relationships of the person and context (Cutchin & Dickie, 2012).
Changes in the person-place whole that disrupt harmonious functional coordination, that is, problematic or undetermined situations, can lead to a need to reconfigure transactions through changes in occupation and contexts to re-establish functional coordination (Cutchin et al., 2008; Johansson et al., 2013). From this perspective, driving cessation can be viewed as creating a problematic situation that disrupts functional coordination, in which engagement in the occupation of driving previously enabled functional coordination between person and context. “Adhering” to medical advice to abstain from driving becomes more than an individual choice, but rather creates a “threat of disintegration of the person-place whole” (Johansson et al., 2013, p. 109). In turn, following medical advice to cease driving is not merely an individual choice, but requires a complex reconfiguration of the coordination of transactions of person and context through problem-solving and alterations in occupation.
The hierarchical model of driving provides a conceptualization that recognizes the connection between person and environment, thus moving away from an individualistic perspective. The hierarchy describes five levels, the first three “technical levels” relate to skills and knowledge for driving (Keskinen, 2014, p. 16). The fourth level refers to “goals for life and skills for living” related to factors such as personal motives, lifestyle, social background, gender, and age that influence driver behaviour (Keskinen, 2014, p. 16). The fifth level, termed the social environment, refers to cultural and social group norms, goals and values, legislation, and law enforcement (Keskinen, 2014). Although the hierarchical model of driving begins to address interactions between person and environment, particularly in relation to the fourth and fifth levels, it describes the social environment as an entity separate from individuals. A transactional perspective suggests that drivers and context are inseparable, co-constituted, and simultaneously shaped and shaped by one another. Transactional perspectives provide an opportunity to reconceptualize driving more generally, which in turn, can be a catalyst to reflect upon driving against medical advice.
Driving Against Medical Advice as an Occupation: Occupational Choice
Rethinking driving against medical advice as an occupation from a transactional perspective reframes the “choices” surrounding driving after stroke, whether according to or against medical advice. Returning to the first author's pilot study, participants reported driving against medical advice because they did not have another choice. A transactional perspective moves away from an individualistic conceptualization of “choice”, situating choice within the transactional, constant coordination between person and context.
Drawing upon a transactional perspective, Galvaan (2012; 2015) critiqued individualistic conceptualizations that locate “occupational choice” within individual volition and as solely resulting from individual reasoning. Her transactional analysis of adolescents’ occupational choices in a marginalized community in South Africa highlighted how these choices were contextually bound within historical occupational patterns, socio-economic conditions, and political factors. In other words, occupational choices and context are inseparable, such that occupational choice is a complex, situated process involving transactions of humans as agents and contexts (Galvaan, 2012). Moreover, Galvaan (2012) suggests that occupational choice may serve as a mediating factor connecting person and occupation, providing a means to maintain or re-establish functional coordination. Thus, from a transactional perspective, understanding choices regarding driving post-stroke needs to go beyond a focus on an individual's knowledge or attitudes, towards attending to how person and context transact to shape such choices.
Central to occupational choice from a transactional view is the recognition that choices are not equally available to all. Socio-economic, political, historical, and other contextual conditions transact in ways that enable or constrain choices available to individuals on the basis of characteristics such as gender, age, ability status, urban/rural location, or race (Galvaan, 2012; 2015). Consequently, differential access to occupational choices can create occupational injustices in participation (Galvaan, 2012; 2015). Occupational injustices encompass restrictions in occupational rights to “experience meaning and enrichment in one's occupations; to participate in a range of occupations for health and social inclusion; to make choices and share decision-making power in daily life; and to receive equal privileges for diverse participation in occupations” (Townsend & Wilcock, 2004, p. 75). As it relates to driving, the existence of unequal access to participation in the occupation of driving may constitute an occupational injustice if rights to community mobility are not supported, particularly for clients whose contextual conditions constrain alternatives to driving and for whom ceasing driving threatens functional coordination. Attending to the complex transactions that shape access to driving and the consequences of not driving can, in turn, inform efforts to challenge occupational injustices that arise for clients whose right to community mobility is inadequately supported within current systems.
Rethinking Driving Against Medical Advice
Equipped with re-configurated concepts of occupation and occupational choice informed by transactional perspectives, how can understandings of driving against medical advice be reframed? Answering this question from a transactional perspective requires an acknowledgement of a multitude of intersecting factors, which, within the scope of this paper, cannot be addressed in satisfactory detail. Instead, we have chosen to illustrate how transactional perspectives can be drawn upon to reframe considerations of risk and issues of equity involved in occupational choices related to driving after stroke.
To acknowledge the complex transactions implicated in driving after stroke, Figure 1 presents examples of some of the intersecting personal and contextual factors cited in the literature pertaining to driving against medical advice, driver cessation, and maintenance of driver cessation. This figure illustrates the interconnectedness and complexity of factors that encompass a transactional perspective of driving after stroke. Importantly, this figure represents only examples of factors relevant to driving after stroke, as from a transactional perspective, the scope of factors that are possibly implicated is vast.
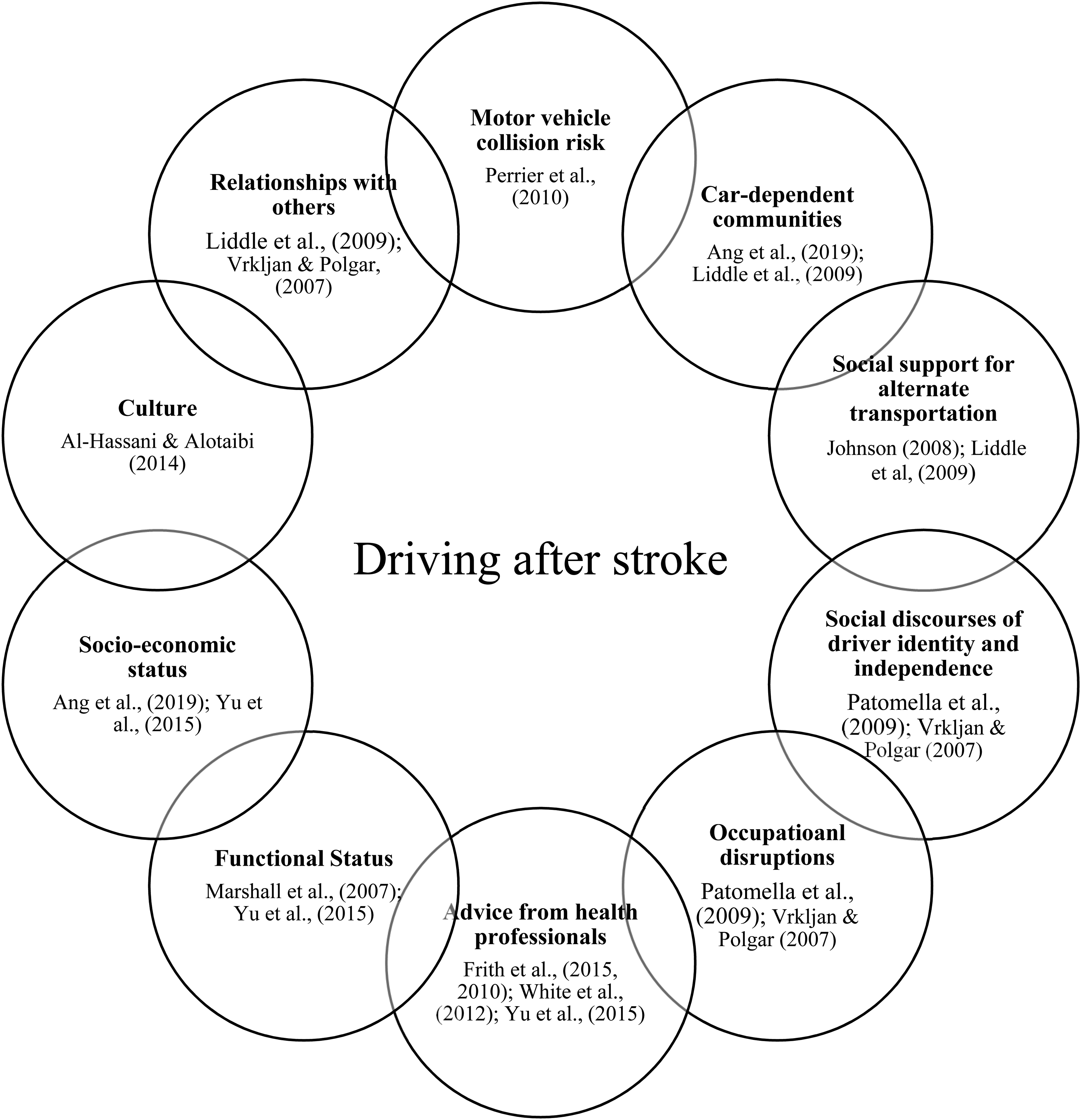
Driving after stroke as a transactional process.
Occupational Choice: What Risks are Considered?
What if considering the risks of driving against medical advice after stroke involved simultaneously considering the opposite, the risks of abstaining from driving? Attending to both the consequences of driving and abstaining from driving after stroke, begins to address the complexity of the person-context transactions shaping this occupational choice. As previously outlined, in a transactional occupational choice perspective, choices are inseparable from social, cultural, historical, and economic conditions. Thus, when an individual is provided with the medical advice not to drive for 30 days, material realities, social ideologies or discourses, and other contextual features can bind, permeate, and influence choices.
Attending to broader social discourses related to driving as part of the transactional process of occupational choice can illuminate unintended consequences and challenges of driver cessation. One does not have to look hard to find examples of Western social discourses surrounding driving, such as archetypal coming-of-age films purporting the freedom-giving and independence-signaling driver's license. The centrality of driving as a marker of valued identity characteristics tied to independence and freedom within a pop culture are also evident in the driving literature. In research conducted with individuals after stroke beyond the 30-day driver restriction, participants described driving as an important and enduring part of their identity, even after driver cessation (Liddle et al., 2009; Patomella et al., 2009). Driving maintains participation in valued activities, and is perceived as a symbol of freedom, flexibility, and spontaneity to engage in occupations (Liddle et al., 2009; Patomella et al., 2009). Furthermore, driving is a taken-for-granted occupation, such that when driving ability is called into question it is perceived as an untenable situation that challenges identity and valued occupational patterns (Patomella et al., 2009). Related to injustice, driver testing is perceived as a violation of the right to self-determination that is imposed after sustaining a stroke (Patomella et al., 2009). In this way, discourses have symbolic, social, psychological, and material consequences which pose other forms of risk connected to personal identity, social identity, and occupational engagement.
Reflecting on the occupation of driving as integral to identity raises the “stakes” associated with abstaining from driving. Driving after stroke is not just a means of accessing the community and engaging in occupations following stroke (Finestone et al., 2010; Liddle et al., 2009; Mountain et al., 2020), but may also be a threat to the self, informed by social discourses of driver identity and independence (Vrkljan & Polgar, 2007). After driving cessation, clients report depression, isolation, loss of freedom, fear, blame, anger, helplessness, and lack of control (Liddle et al., 2009; Patomella et al., 2009). Thus, the “risks” to abstain from driving are also high. Acknowledging the situated nature of occupational choice challenges researchers and occupational therapists to consider the transacting personal and contextual elements involved. The advice from health professionals to abstain and the social discourses of driver identity to drive exist in a transaction and influence occupational choices. Consequently, not abiding by medical advice is more than an individual act of non-compliance based on a lack of understanding of risks as defined by a biomedical perspective. Rather, it is a complex process of considering various intersecting risks (Patomella et al., 2009; Vrkljan & Polgar, 2007).
Balancing techno-scientific and socialcultural notions of risk were raised by Galvaan (2015) when exploring the occupational choices of adolescents in South Africa. Adolescent participants recognized the health risks of smoking tobacco and admonished adults for smoking, but at the same time took up the occupation of smoking. Within their sociocultural context, smoking was an expected, socialized and patterned occupational choice, regardless of health consequences (Galvaan, 2015). In this way, smoking despite known biomedically defined risks is analogous to driving against medical advice; both are occupational choices that are heavily embedded within social contexts. Therefore, techno-scientific notions of risk, wherein “good” clients act rationally to make “safe” choices, are inconsistent with the complexities of driving against medical advice following stroke. In fact, in addition to risks to personal and public safety, there can be significant legal and insurance ramifications of driving against medical advice. In Ontario, for example, a client's license could be suspended as a result of a physician or occupational therapist's report to the Ministry of Transportation. Any person found guilty of driving with a suspended license is liable to a fine up to $5,000 with repeated offenses leading to higher fines and/or imprisonment (R.S.O. 1990, c. 53 (1); 1997. C.12, s. 7 [1]). Moreover, sustaining a MVC while driving against medical advice can invalidate some insurance coverages and benefits (Financial Services Commission of Ontario, 2021). While legal and insurance implications might be viewed from a techno-scientific perspective as rational reasons that ought to lead to a decision to not drive, a transactional perspective does not assume that any form of risk necessarily takes precedence. Rather, a transactional view turns attention to how various risks, including material, practical, social, and symbolic transact within particular contexts and influence occupational choices.
Occupational Choice: Are all “Choices” After Stroke Equal and Available to all?
Considering driving after stroke as an occupational choice arising through transactions of person and context also brings issues of justice to the fore. If occupational choices can be constrained by contextual factors, then choices for driving after stroke, or more importantly, not driving, can similarly be constrained. From an individualistic, biomedical perspective, one simply must make the rational “choice” not to drive given risks to health and safety, regardless of other consequences or the availability of an acceptable mobility alternative. But do all clients after stroke have the same access to choices to abstain from driving? From a transactional perspective, do all clients have the same access to resources and conditions that enable them to negotiate the threat to “possibilities for action” (Johansson et al., 2013, p. 111) resulting from the absence of driving?
Most communities in the developed world are car-dependent and built on the assumption of universal car use (Mattioli et al., 2020). Car dependence, or the prioritization of car travel to meet human needs over other transport alternatives, is pervasive and reinforced by social, political, and economic facets of “car culture” (Mattioli et al., 2020). Consequently, accessing alternatives to car travel to support driving cessation can be difficult not only symbolically, but also practically. In a recent systematic review of the challenges of driver cessation, access to alternative methods of transportation was a significant barrier, both in rural and urban settings (Ang et al., 2019). In many regions, public transportation is not available, and when it is, it is perceived as inconvenient, restrictive, unaffordable, and time consuming, compared to car travel (Ang et al., 2019; Liddle et al., 2009). Another obvious alternative is accessing a ride from another driver. Often individuals call upon family and friends for rides, and not surprisingly, those who have social support of an alternate driver more easily maintain driving cessation (Ang et al., 2019; Johnson, 2008; Liddle et al., 2009). However, even when social support is available, individuals may fear becoming a burden to those who are driving them (Liddle et al., 2009; Vrkljan & Polgar, 2007). Another significant predictor of driving against medical advice is related to income and employment. Workers who are the primary income earner are more likely to drive against medical advice within the first 30 days post-stroke, which may be required to maintain job and financial security (Yu et al., 2016). While these findings represent just a window into how contextual conditions can create barriers to driving cessation, they highlight the complexities of the transactions shaping possibilities for action and complicate education-based best practice guidelines.
Taken together, alternatives to driving are not equally available and accessible to all. The “choice” to abstain from driving is situated in the physical, social, and economic contexts. As such, where you live, who you live with (or don't), your socio-economic status, among other uncountable factors, enable or constrain choices that are available and therefore, options to abstain from driving. Viewing driving after stroke as a transactional occupational choice seeks to go beyond a rational-choice narrative to foreground the transactional nature of the person in their context and acknowledges the inequities that exist in the possibilities for driving cessation.
A way Forward for Research and Occupational Therapy Practice
Applying concepts from transactional perspectives on occupation raises awareness of the complexity of negotiating a 30-day driver restriction post-stroke and can inform re-imaginings of how to approach this issue in research and clinical practice. While the shortcomings of an individualistic, biomedical perspective of driving after stroke have been raised here, we are not suggesting abandoning such research on driving and stroke. Conversely, the dominance of this approach needs to be challenged, creating space to conduct research located in other perspectives that can also inform practice. Although individualistic, biomedically framed research provides vital knowledge about the health and safety risks of driving after stroke, it has also led to a predominant tendency to conceptualize, study and address driving as an individual experience and choice. In addition to obscuring contextual conditions shaping driving, only studying driving from an individualistic perspective can lead to research being complicit in framing driving against medical advice following stroke as an “individual problem”, thereby invoking labels of “noncompliance”. Researching and considering the complex transactions implicated when addressing the occupation of driving after stroke can broaden understandings and create opportunities for new insights and foci of inquiry. Specifically, using mixed and qualitative methods informed by a transactional perspective to explore contextual facets in tandem with individual factors, we can better understand the complex coordination of the person and environment in the occupational choice of driving.
In clinical practice, if we consider driving from a transactional perspective, occupational therapists can develop more nuanced understandings of driver cessation to inform client-centred care that optimally supports possibilities for continued functional coordination of the person-context whole. Understanding the complexities of driving after stroke can attenuate occupational therapists to the stakes of abstaining from driving after stroke. With this understanding, occupational therapists in acute care can approach initial counselling with clients about mandatory driver cessation following stroke with a more holistic perspective, thus setting the stage for ongoing, open conversations through the continuum of care. Stroke best practice guidelines increasingly underscore the importance of client-centred care but have been criticized for falling short of that goal (Egan et al., 2020). Identifying enablers and constraints by attending to the transactional person-context whole can equip the occupational therapist and client to develop client-centred strategies that facilitate community mobility during driver cessation post-stroke. Such strategies could include (1) approaching driver cessation discussions with empathy and recognition of the occupational “stakes” involved, (2) using active, client-centred, and partnered collaborations to identify and troubleshoot potential options for community mobility, (3) assisting with applications for subsidized transportation alternatives, and (4) easing the burden of accessing medical/therapy appointments (e.g., coordinating appointments to occur at the same place and date, providing in-home services or telerehabilitation). At broader levels, applying a transactional perspective can inform advocacy efforts that change conditions to lessen the disequilibrium that can arise from ceasing driving; for example, advocating for improved services within health regions to reduce travel demands, working to create a greater range of low cost and easily accessible options for publicly subsidized forms of transportation, and contributing an occupational perspective to community planning sessions. While these strategies will not immediately negate the unintended negative consequences of driver cessation, they may represent a way forward and create opportunities to rethink driving after stroke, including against medical advice, in practice and in the communities in which we work
Limitations
The central argument of this paper, to go beyond an individualistic, biomedical perspective of driving after stroke to embrace a more transactional perspective when addressing this occupation, may be at odds with the realities of the systems in which occupational therapists practice (Aldrich & Rudman, 2020). Specifically, within acute care, occupational therapists often experience tensions between the goals of the organization and philosophy of the profession (Murray et al., 2021). With the predominant biomedical model of care and primary focus on rapid discharge within acute care settings, occupational therapists often do not have time, space, resources, or organizational support to address occupational issues from a transactional perspective (Murray et al., 2021). As such, we acknowledge that advocating to address driving from a transactional occupational perspective could be met with a lack of understanding or even resistance. At the same time, optimally supporting clients in their occupational lives and aligning practice with core occupational therapy values requires taking up a collective professional responsibility to work towards system and practice changes (Aldrich & Rudman, 2020; Laliberte Rudman, 2021).
Conclusion
In this paper, we advocate for going beyond individualistic, biomedical notions of risk and choice to deepen our understandings about driving during the 30-day period of mandatory driving restriction after stroke. We have argued for applying concepts from transactional perspectives on occupation to disrupt the dominance of individualistic, biomedical perspectives and create new possibilities for clients and occupational therapy practice. We invite clinicians and researchers to further consider how transactional perspectives can broaden research foci and generate new strategies to support community mobility after stroke.
Key messages
Occupational therapists are encouraged to go beyond an individualistic, biomedical perspective of “driving against medical advice” by analyzing how “choices” for driving after stroke are situated within the transactions of clients in context.
Occupational therapists are encouraged to partner with clients to enact strategies that acknowledge and address the challenges of driver cessation that arise through person-context transactions.
Further dialogues between occupational science and occupational therapy can support practice approaches informed by understandings of occupation as situated.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.