
Abstract
Introduction
Little is known about satisfaction with features of power mobility devices, yet these devices are being recommended in clinical practice to promote learning and overall development in young children. Given the increasing device options available for young children, it is critical to understand parents’ and therapists’ perspectives. Parents’ and therapists’ satisfaction with four early childhood power mobility devices were examined during a two-phased study. Parents and therapists of children 6 years and younger with mobility limitations were recruited from across the province. This paper’s primary objective was to examine parents’ satisfaction with four devices their child trialled during a single introductory session (Trial Phase). Secondary objectives included (i) comparing therapist ratings to those of parents, (ii) contrasting satisfaction among device features, and (iii) examining whether device satisfaction changes following a 6-month equipment loan (Loan Phase).
Independent mobility promotes learning and overall development in infants and children, but when mobility is delayed or impaired, developmental progress may be impeded (Piek, Dawson, Smith, & Gasson, 2008; Huang, 2018). Power mobility may be introduced as early as 12 months of age for children unable to walk or who are anticipated to have inefficient mobility due to a physical disability (Livingstone & Paleg, 2014), such as cerebral palsy, spina bifida or neuromuscular diseases (Livingstone & Field, 2014). Young children with mobility limitations can use powered devices such as switch-adapted ride-on toys, wheelchairs or other mobility devices to explore and learn about their environment, play, and interact with others (Huang, 2018; Feldner, Logan & Galloway, 2016).
A recent mixed-methods evidence synthesis found strong support for a positive impact of power mobility on children’s movement and mobility, and moderate support for impact on participation, play and social interaction (Bray et al., 2020). The highest level of evidence supporting power mobility use for children aged 6 years and younger is a randomized control trial including 28 children with complex disabilities (Canadian Agency for Drugs and Technologies in Health, 2015; Jones, McEwen, & Neas, 2012). After one year, statistically significant differences in overall development between the intervention and control groups were found, along with no negative impact on motor development from power wheelchair use (Jones, et al., 2012). Another recent systematic review also suggested a potentially positive impact from power mobility interventions on young children’s social skills (Cheung, Meadan, & Yang, 2020).
Research is beginning to evaluate the different types of power mobility devices available for young children with mobility limitations. A scoping review evaluated impact of modified ride-on toy cars (James, Pfaff, & Jeffries, 2019) while individual studies have investigated other novel powered devices (Evans & Baines, 2017; Plummer, Logan, & Morress, 2021). Research has contributed insights into parents’ and therapists’ perspectives on device features affecting young children’s power mobility use (Livingstone & Field, 2015; Gudjonsdottir, & Gudmundsdottir, 2021). Limitations such as price, size and weight, transportation requirements, maintenance, social acceptance and aesthetics have been reported in the literature and continue to be problematic (Feldner et al., 2016). Similarly, a mapping review of inclusive paediatric mobility design over the last 50 years identified problems related to desirability, feasibility and viability of wheeled mobility interventions for children (O’Sullivan & Nickpour, 2020).
The Quebec User Evaluation of Satisfaction with assistive Technology (QUEST) was developed to measure satisfaction with assistive technology devices (Demers, Weiss-Lambrou, & Ska, 2002; Demers, Weiss-Lambrou, & Ska, 2000). QUEST 2.0 consists of two subscales: Assistive Device (8 items evaluating device features) and Services (4 items evaluating service delivery) (Demers, Weiss-Lambrou et al., 2002; Demers et al., 2000). Several studies have used the QUEST to examine adults’ satisfaction with their wheeled mobility (Barlow, Liu, & Sekulic, 2009; Arthanat, Wu, Bauer, Lenker, & Nochajski, 2009; Demers, Monette, LaPierre, Arnold, & Wolfson, 2002; Chan, & Chan, 2007; Weiss-Lambrou, Tremblay, LeBlanc, Lacoste, & Dansereau, 1999), yet fewer have examined satisfaction with paediatric power mobility devices (Gudjonsdottir & Gudmundsdottir, 2021; Benedict, Lee, Marrujo, & Farel, 1999; Tefft, Guerette & Furumasu, 2011). Limited research comparing features and acceptability of powered mobility devices for young children raises questions regarding the features most important to consider.
Given the advances in power mobility technologies and increasing options available for young children, it is critical to understand parents’ and therapists’ perspectives. The primary objective of this paper was to report parents’ satisfaction with four devices their child trialled during a single exploratory session (Trial Phase). Secondary objectives included (i) comparing therapist ratings to those of parents, (ii) contrasting satisfaction among device features, and (iii) examining whether device satisfaction changes following a 6-month equipment loan (Loan Phase). To our knowledge, this is the first study to explore parent and therapist impressions using QUEST 2.0 of four different power mobility devices designed for young children.
Method
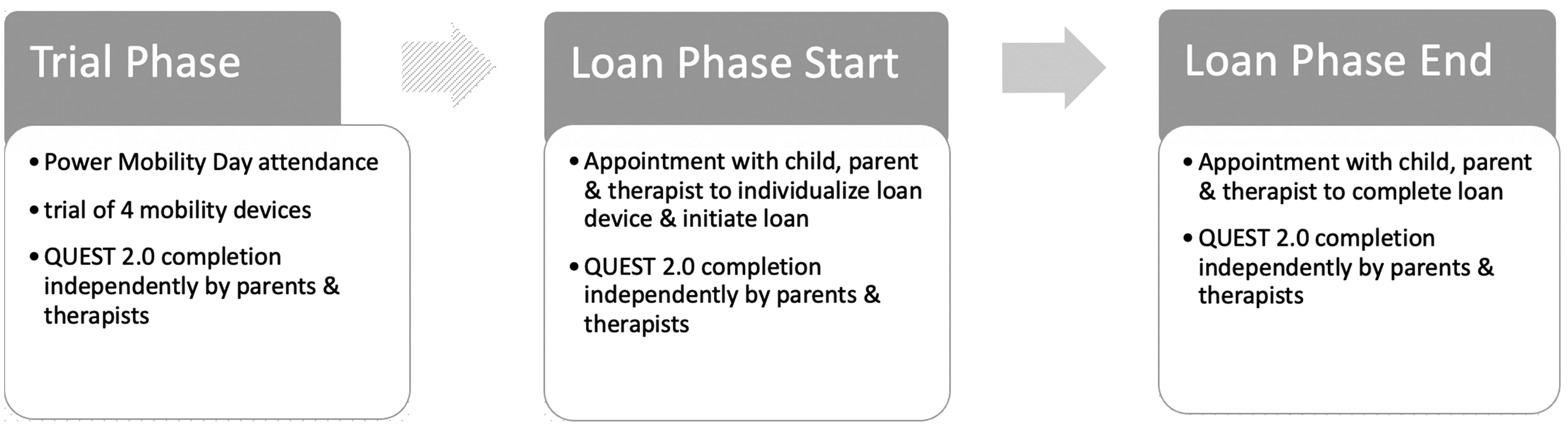
Study design diagram.
consider power mobility for use by their child/client aged 6 months - 6 years with a diagnosis or clinical presentation suggesting inability or inefficient mobility in early childhood; participate in one Power Mobility Day, a novel, 1–1½ hour play-based session; participate in a 6-month power mobility device loan.
For ease of reading, ‘parent’ will be used to imply primary caregiver (e.g., foster parents and grandparents) who were included with written consent of the legal guardian.
University and Institutional Ethics Review Boards granted ethics approval and all participating parents and therapists provided written informed consent.
At the end of the Power Mobility Day session, researchers facilitated independent completion by parents and therapists of the QUEST 2.0 Assistive Device subscale (Demers, Weiss-Lambrou et al., 2002; Demers et al., 2000) (hereafter referred to as QUEST8) to rate satisfaction with each of the four devices trialled. The eight items included dimensions, weight, ease of adjustment, safety and security, durability, ease of use, comfort and effectiveness. The subscales can be scored separately and evidence supports their reliability and validity (Demers, Weiss-Lambrou et al., 2002; Demers et al., 2000; Demers, Monette et al., 2002; Tefft et al., 2011; Kenny & Gowran, 2014). Items were rated on a 5-point ordinal scale ranging from 1 (not satisfied at all) to 5 (very satisfied). Since literature and our clinical experience suggests that aesthetics may be an important feature that parents and therapists consider (Feldner et al., 2016; Livingstone & Field, 2015; Gudjonsdottir & Gudmundsdottir, 2021; O’Sullivan & Nickpour, 2020), we also asked participants to rate satisfaction with device Aesthetics. QUEST developers acknowledge that additional questions can be added if scored separately using the same 5-point ordinal scale (Demers, Weiss-Lambrou et al., 2002). Summary satisfaction scores include total and average scores (total score/items completed).
During Loan Phase, the QUEST8 along with the additional question rating Aesthetics were again independently completed at device loan start and end by each parent and therapist. Device loaned was based on parents’ first or second choice during the Trial Phase, dependent on device availability and their child’s functional abilities. The device was individualized for each child with appropriate postural supports and access method (joystick/switches). Parents and therapists were trained in device use and training suggestions were provided. Researchers provided additional support as needed during the loan. Additional details can be found in related publications (Livingstone, Bone & Field, 2020; Livingstone & Field, 2020; Livingstone & Field, 2021). Power analysis for a one-group sample Wilcoxon signed-rank test (matched pairs) was conducted using G*POWER to determine a sufficient sample size using an alpha of 0.05, a power of 0.80, a medium effect size (d = 0.5) and two tails (Faul, Erdfelder, Buchner, & Lang, 2009). Based on these assumptions, the desired sample size was 35.
To compare parent and therapist scores, Mann Whitney U test, 2-sided with continuity correction, tested the null hypotheses that parent and therapist median satisfaction would be the same across devices for Trial Phase QUEST8 and Aesthetics scores (McCrum-Gardner, 2008). Effect size, estimated using the formula z/sqrt(n) (Tomczak & Tomczak, 2014), was interpreted as follows: <0.3 = small; 0.3–0.5 = moderate; >0.5 = large (Cohen, 1988). To address our secondary objective comparing device features, we examined frequency counts of those rated as 4 (quite satisfied) and 5 (very satisfied) for each device. To address our secondary objective examining satisfaction change over time, Wilcoxon signed-rank test for dependent samples compared Loan Phase QUEST8 and Aesthetics scores from loan start to end. Significance levels for all analyses were p ≤ 0.05, unless otherwise noted.
Findings
Of those families approached to participate in the Trial Phase, 75/81 consented to participate. Seventy-five children aged 9 months to 5 years 8 months (mean 32.45 months; SD 14.08) were enrolled in Trial Phase, with 38 males and 37 females. Cerebral palsy was the most common child diagnosis. Although all 75 parents signed consent forms, one child did not try any devices so their data (along with their parents’ and therapists’ data) was not included in our analyses. Seventy-four children, their parents and therapists took part in one of 18 Power Mobility Days in nine communities.
As a second phase of our research, 49/74 parents were approached to participate in the Loan Phase and 46 consented along with their therapists. Children’s mean age at loan-start was 40.43 (SD 15.66) and ranged from 13 to 68 months. Cerebral palsy was again the most common diagnosis (n = 33; 71.74%). Mean loan-length was 192.4 days (SD 42.79), ranging from 92 to 294 days. Table 1 describes parent and therapist characteristics. Parent respondents were primarily mothers and the majority had post-secondary education. More occupational therapists than physical therapists participated, with the majority having greater than 5 years paediatric rehabilitation experience. Twenty-two therapists in Trial Phase and six in Loan Phase had more than one child in the study. One parent did not complete all demographic information in Trial Phase, while some children had a change of therapists between Trial Phase and Loan Phase, and/or within Loan Phase, resulting in sample size differences across analyses.
Participant Characteristics.
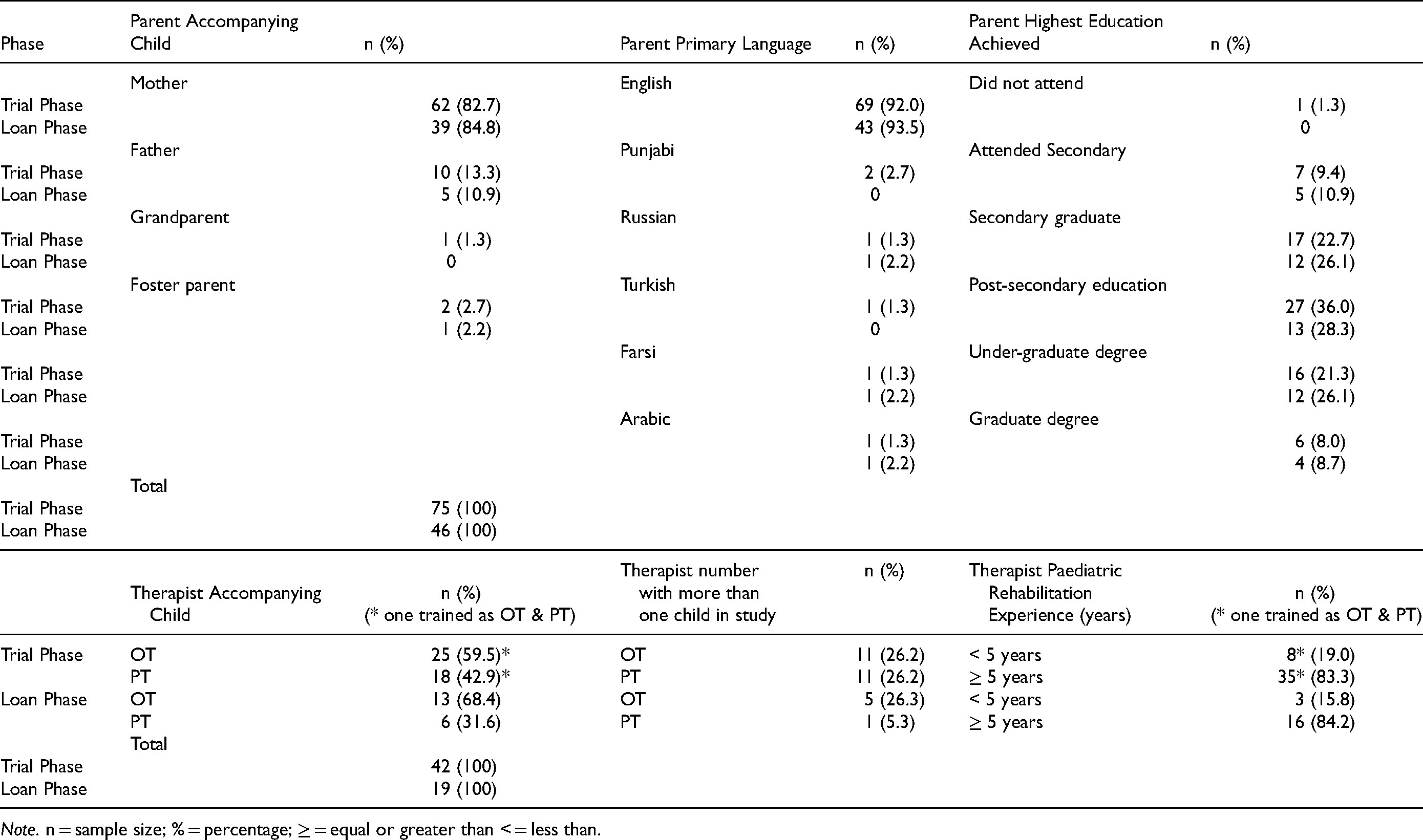
Note. n = sample size; % = percentage; ≥ = equal or greater than < = less than.
Table 2 presents Trial Phase summary scores for the 8-item device subscale and the additional Aesthetics question for parents (primary objective) and therapists (secondary objective). Figure 2 illustrates boxplot comparisons of parents’ and therapists’ QUEST8 and Aesthetics median scores by device for Trial Phase. For QUEST8 median total scores parent scores ranged within 3.5 points, while therapist scores ranged within 4.5 points. Distribution of Aesthetics median scores ranged from 3 to 5 for both groups. Table 2 presents Kruskal-Wallis test results and large effect size estimates providing support for the alternate hypothesis that median QUEST8 total scores and Aesthetics scores were not equal across devices. Conover Test results with Bonferroni correction for pairwise comparisons of devices identified statistically differing QUEST8 and Aesthetics median scores for both parents and therapists.
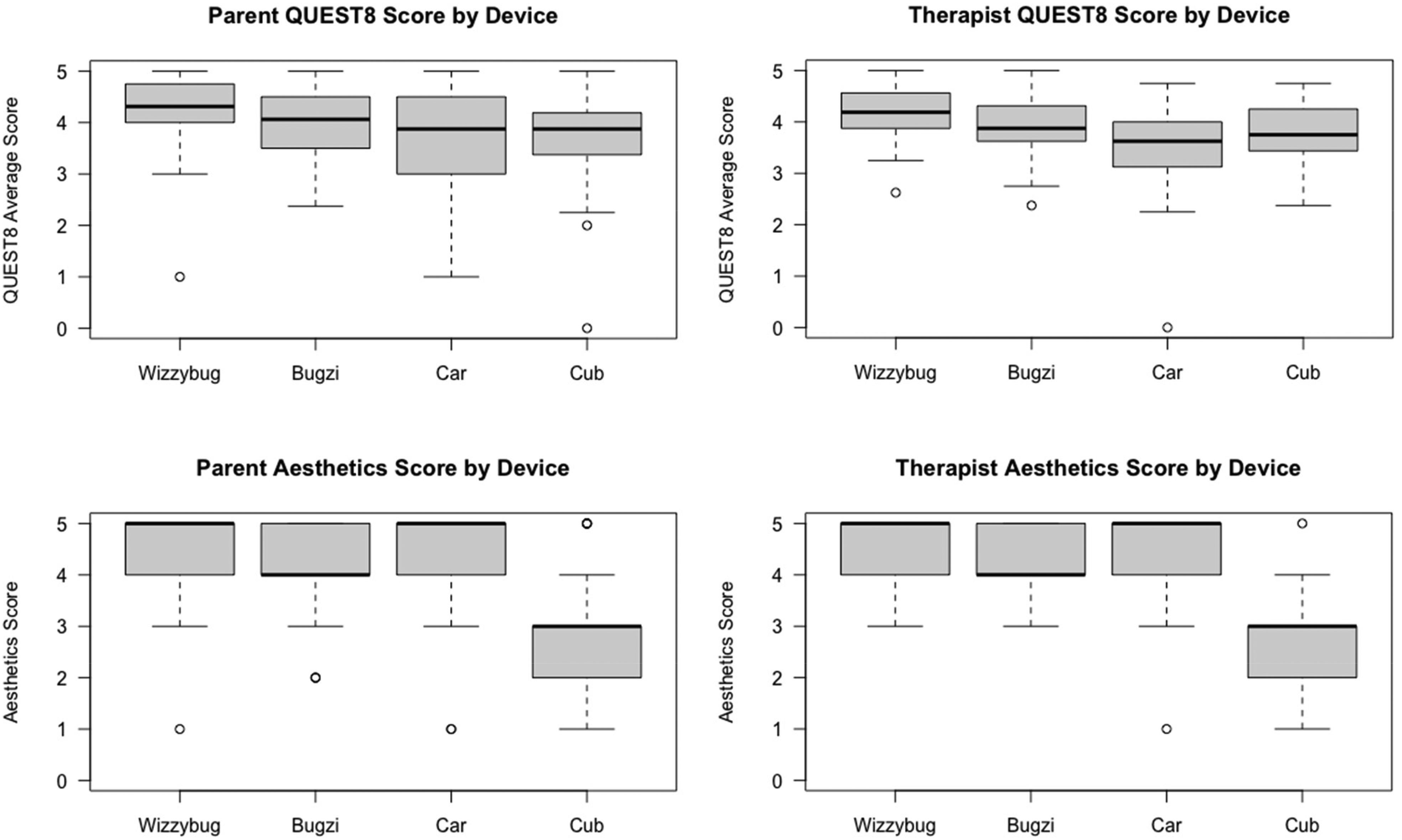
Comparison of Trial Phase parent and therapist QUEST8 and aesthetics scores by device.
Trial Phase Parent and Therapist QUEST8 and Aesthetics Summary Scores.
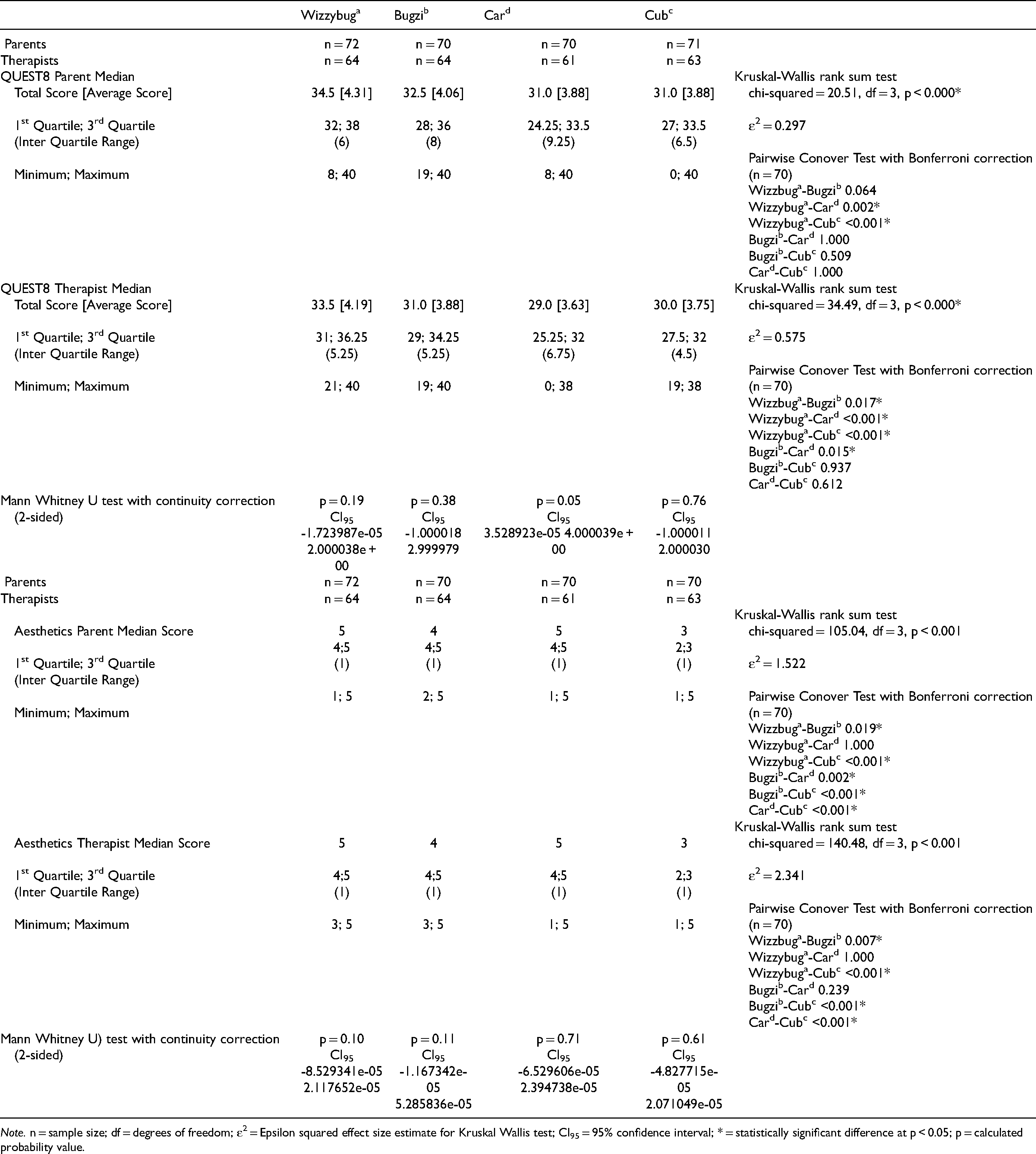
Note. n = sample size; df = degrees of freedom; ε2 = Epsilon squared effect size estimate for Kruskal Wallis test; CI95 = 95% confidence interval; * = statistically significant difference at p < 0.05; p = calculated probability value.
Table 3 identifies device features with which parents were most satisfied, including Wizzybug’sa dimensions and safety, Bugzi’sb and Cub’sc safety, and Car’sd aesthetics. Table 4 identifies therapists’ highest-rated features as Wizzybug’sa, Bugzi’sb and Car’sd aesthetics, and Cub’sc safety.
Trial Phase Frequency Count Comparison by Device of QUEST8 and Aesthetics Items Rated 4 (Quite Satisfied) or 5(Very Satisfied) by Parents.
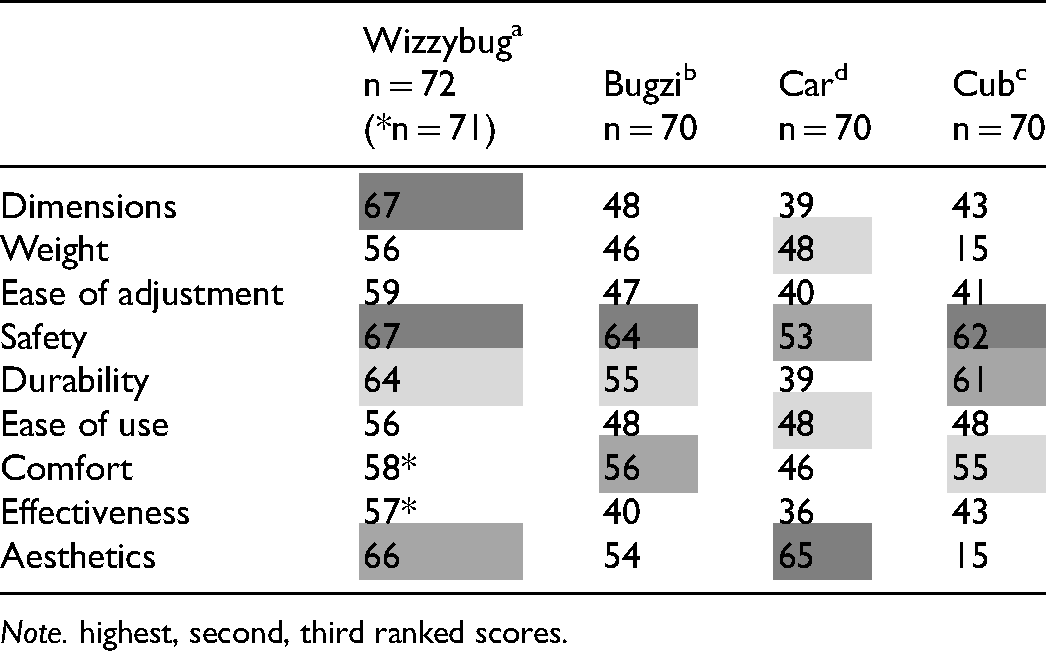
Note. highest, second, third ranked scores.
Trial Phase Frequency Count Comparison by Device of QUEST8 and Aesthetics Items Rated 4 (Quite Satisfied) or 5(Very Satisfied) by Therapists.
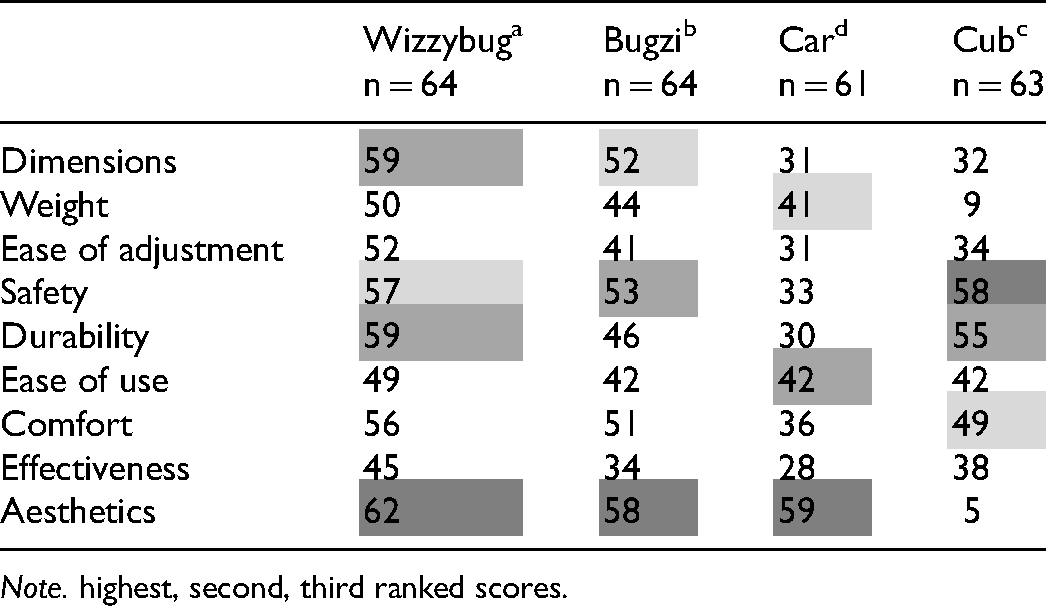
Note. highest, second, third ranked scores.
Table 5 illustrates change in satisfaction over the course of the Loan Phase loan. There were no statistically significant differences between Loan Phase parents’ and therapists’ ratings at each time point, although over the course of the loan parent QUEST8 scores decreased while therapist QUEST8 scores remained stable, as did parent and therapist Aesthetics median scores. Figure 3 illustrates Loan Phase boxplot comparisons at loan-start and end.
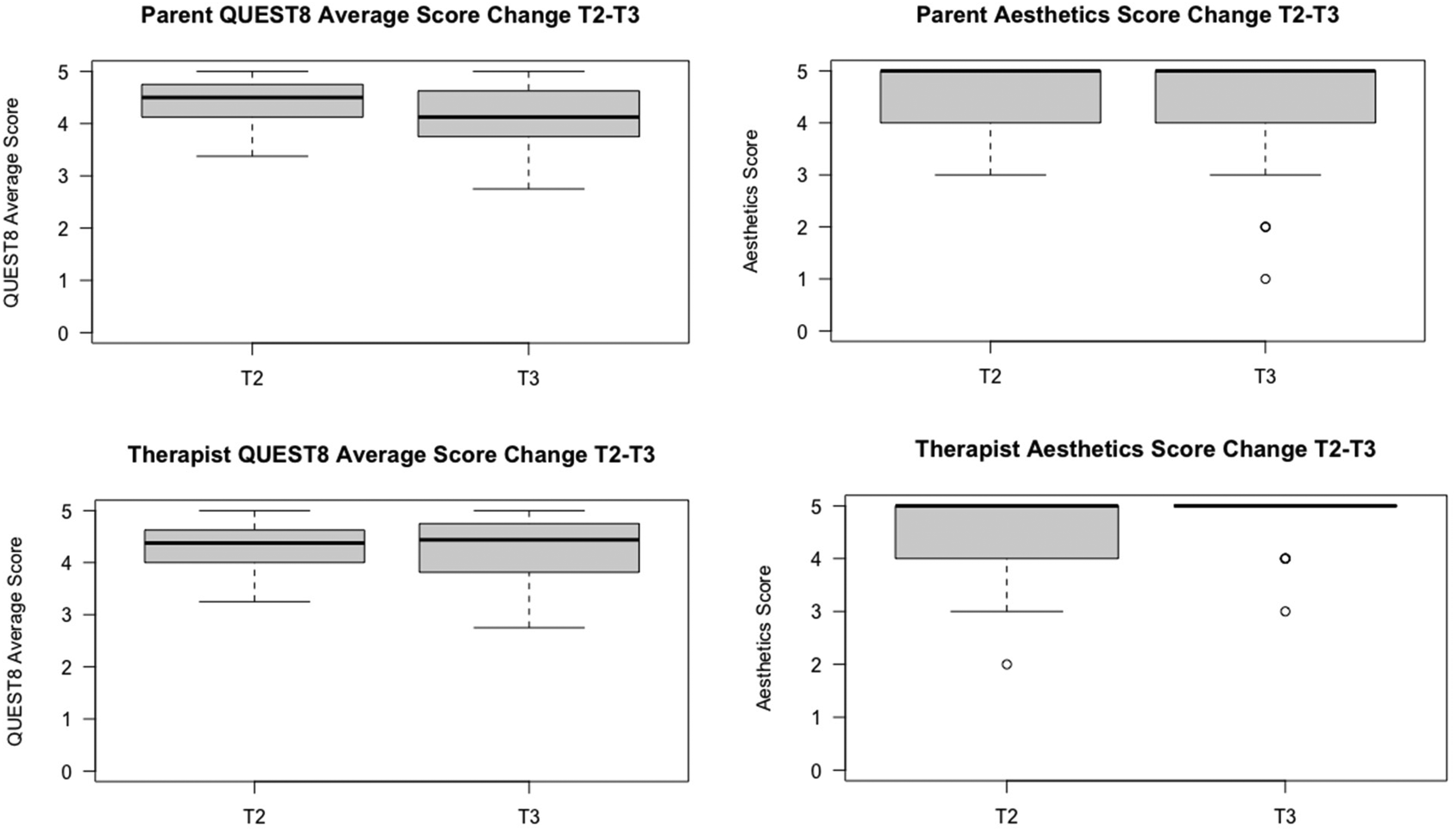
Comparison of Loan Phase parent and therapist QUEST8 and aesthetics scores.
Loan Phase QUEST8 and Aesthetics Satisfaction Ratings from Loan Start to End.
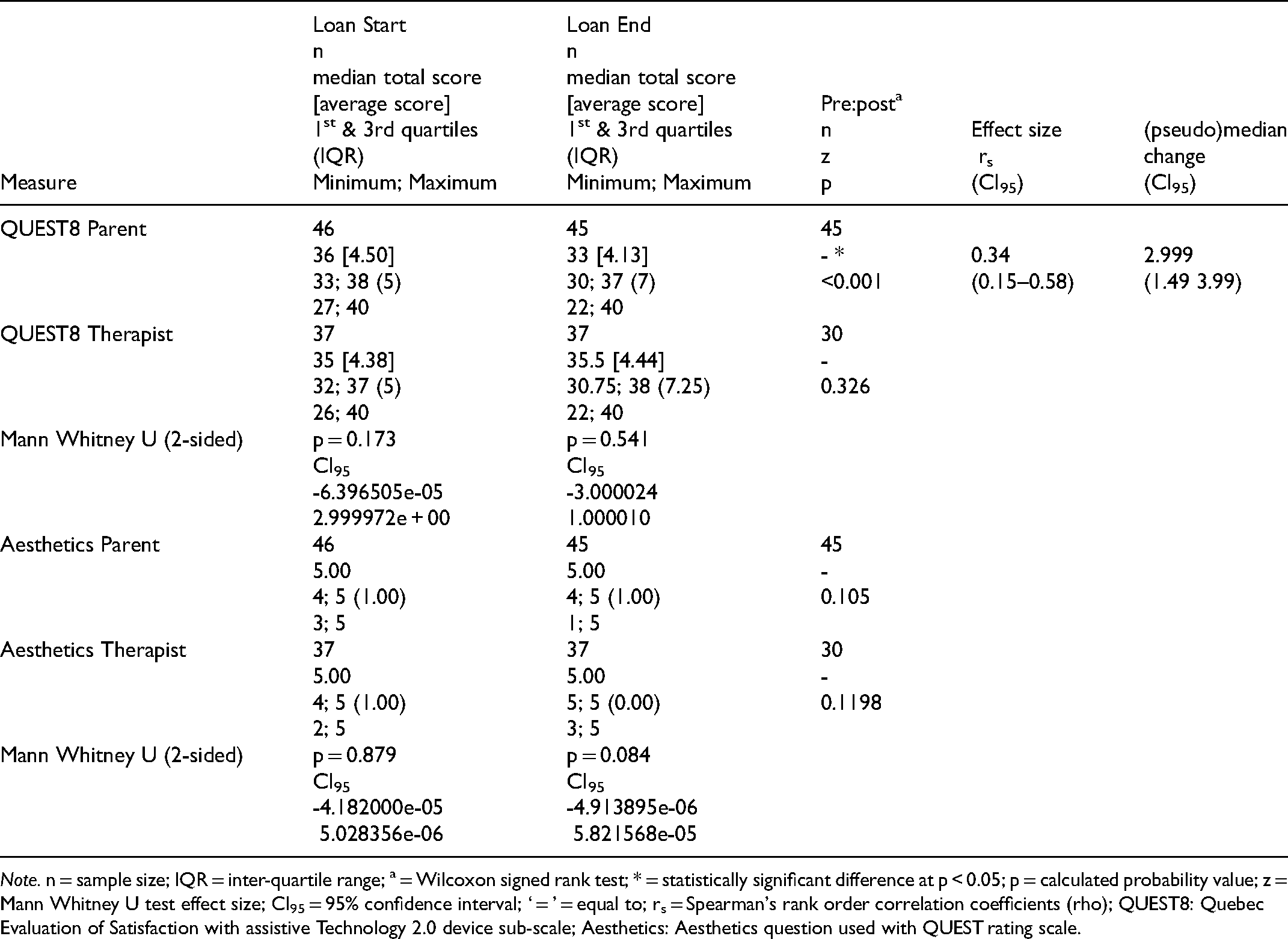
Note. n = sample size; IQR = inter-quartile range; a = Wilcoxon signed rank test; * = statistically significant difference at p < 0.05; p = calculated probability value; z = Mann Whitney U test effect size; CI95 = 95% confidence interval; ‘ = ’ = equal to; rs = Spearman's rank order correlation coefficients (rho); QUEST8: Quebec Evaluation of Satisfaction with assistive Technology 2.0 device sub-scale; Aesthetics: Aesthetics question used with QUEST rating scale.
Discussion
To address our primary objective, most parents were satisfied with device features for QUEST8 and Aesthetics ratings of Wizzybuga, Bugzib, Card and Cubc after participating in an introductory trial session, although satisfaction ratings were variable across the four devices. In regards to our first secondary objective, therapist satisfaction ratings for QUEST8 and Aesthetics were similar to parent ratings. Although QUEST8 score spread was somewhat less, differences in therapists’ Aesthetics median ratings mirrored parents’ ratings.
Our QUEST8 scores are in line with other studies, although equipment and measurement approaches differ somewhat. In a study evaluating different service delivery models, mean QUEST 12-item total scores included both Device and Services subscales and ranged from 3.89 (CI95 3.48–4.30) to 4.18 (CI95 3.62–4.74) (Barlow et al., 2009). A recent survey of children 7–18 years and parents, compared QUEST 12-item scores across walkers, manual and power wheelchairs but reported only percentage of those quite/very satisfied (Gudjonsdottir, & Gudmundsdottir, 2021). Adult studies reported QUEST 2.0 Devices subscale values (Arthanat et al., 2009, Demers, Monette et al., 2002), with one reporting a slightly lower mean device satisfaction total score of 27.69 (SD 4.57) (Chan, & Chan, 2007). Variation between study results may be expected with differing measurement approaches; our study had parents rating their child’s device features, bringing in another difference. Given our positively skewed data, parents and therapists in our study were generally satisfied with the four devices. This aligns with the developer’s statement that average scores ≥4.0 for mobility devices suggest an acceptable level of device satisfaction (Demers et al., 2000).
For our secondary objective contrasting feature satisfaction, parents rated safety and durability most highly across devices although aesthetics and comfort were also important; while therapists rated aesthetics highly (for all but Cubc), along with safety, durability and device dimensions. Our results are comparable to a study of caregiver satisfaction with assistive technology device use (including powered mobility) for preschool children, where appearance, safety, effectiveness, and durability were most highly rated (Benedict et al., 1999). Similarly, safety, durability, and appearance were rated highest in another study (Weiss-Lambrou et al., 1999) while a further rated size, safety and ease of use highest (Gudjonsdottir, & Gudmundsdottir, 2021). Weight and ease of adjustment were rated least satisfied in that same study (Gudjonsdottir & Gudmundsdottir, 2021).
Interestingly, for our secondary objective examining change in satisfaction from loan-start to end, there was a statistically significant difference in parent QUEST8 satisfaction scores with a moderate effect size, although this change was not observed for therapists, nor did Aesthetics ratings change in either group. The slight decrease in parent QUEST8 satisfaction likely represents a more practical appreciation of the device following real-life experience, although the loan-end median score of 4.13 indicates that parents were still ‘quite satisfied’. Devices were predominantly selected by parents, and access method and postural supports were individualized for child abilities, suggesting the device was suitable for each child.
Our results are similar to another pre-post study involving 23 children under 6 years of age: after 4–6 months of powered wheelchair use, parents’ average QUEST 2.0 satisfaction ratings were quite satisfied (score of 4) and very satisfied (score of 5), for six of eight device-related items although weight and ease of adjustment ratings were lower (Tefft et al., 2011). Our study’s therapists’ (unchanged) ratings may have been influenced by prior device experience or reduced device interactions throughout the loan in comparison with parents (Livingstone & Field, 2020; Livingstone & Field, 2021). Curiously, when QUEST8 and Aesthetic satisfaction ratings were compared between parents and therapists both at loan-start and at loan-end, scores did not differ statistically from each other, perhaps because both groups were generally satisfied with device features. This perhaps may be explained partly by the loaned device being of the parents’ own choice.
Our respondents’ satisfaction with Aesthetics may be attributed somewhat to the novel device designs, as discussed in a qualitative paper highlighting parents’ and therapists’ perspectives of their Power Mobility Day (Trial Phase) experience (Livingstone, Field, Sanderson, Pineau, & Zwicker, 2020). Others have described how parents appreciated that the toy car avoided the attention associated with specialized equipment, because it was much like typical children’s toys (Pritchard-Wiart et al., 2019). A similar sentiment was suggested with Wizzybuga: that it was ‘designed to invoke fun and play associated with children’s ride-on toys as opposed to the medical aesthetic of some mobility devices’ (Evans & Bains, 2017, p.144). Our quantitative results regarding satisfaction with device features are (for the most part) supported by parents’ and therapists’ perspectives reported in paediatric qualitative literature (Bray et al., 2020; Evans & Bains, 2017, Livingstone & Field, 2015; Livingstone, Field et al., 2020; Pritchard-Wiart et al., 2019). Of note, is the differing priorities that our parents and therapists placed on features across the four devices in regards to suitability for their child. This reinforces the importance of fit between child, device and environment when learning to use a power mobility device and integrating it into the child’s and family’s life (Bray et al., 2020; Benedict et al., 1999; Tefft et al., 2011).
Conclusion
Findings suggest that parents’ and therapists’ initial satisfaction with device features were positive, although there was some variability across the four powered mobility devices. Parents’ and therapists’ priorities across devices varied, although safety, durability, aesthetics, comfort and dimensions were most valued. Despite variability among parents’ and therapists’ satisfaction ratings, median score differences between these two groups for each device did not differ significantly. Over an extended device loan period, parents’ satisfaction with some features decreased as they began using the devices in everyday life. However, parent & therapist QUEST and Aesthetics ratings remained favourable. Device features are an important consideration when introducing power mobility for young children, in order to optimize its fit with the child’s and family’s life. Trial and loan opportunities may enhance parent satisfaction and engagement with power mobility use for children with delayed or limited mobility. This is the first study to explore quantitatively similarities and differences between parent and therapist impressions of four different paediatric power mobility devices.
Key Messages
Device feature satisfaction is important to consider when providing power mobility devices for young children as they may influence device acceptance and use in daily life.
Parents’ and therapists’ perspectives of device features may differ, yet both perspectives are valuable when determining suitability of device for young children.
Satisfaction with power mobility device features may vary depending on child, family and therapist experiences.
There are benefits of trialing several different devices, and considering parents’ choice before providing a mobility device for a longer loan period.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, of this article: This work was supported by the Posture & Mobility Group (UK), Sunny Hill Health Centre for Children, British Columbia Children’s Hospital Research Institute, Sunny Hill Foundation for Children,