
Abstract
Background.
The occupational therapy school-based Partnering for Change (P4C) model has mostly been documented in Ontario.
Purpose.
This implementation study describes the implementation of P4C in two Québec elementary schools (P4C-Q), as well as therapy practices, their impacts, factors perceived to influence implementation, and recommendations.
Method.
A sequential mixed-methods design was applied. Therapists (n=2) completed daily journals, describing activities by P4C-Q level. Therapists and other school-stakeholders (n=11) participated in semi-structured interviews, analyzed through a content analysis framework.
Findings.
Daily journals illustrated that the majority of therapy time was spent on activities targeting the entire classroom, and on collaboration with educators. Interviews illustrated how coaching was used across different practices and the impact of these practices for schools (e.g., capacity-building) and children (e.g., increased functioning), and highlighted how relationship-building is key to facilitating the implementation of this model.
Implications.
Lessons learned may be helpful for others implementing P4C in their own contexts.
Introduction
Best practices suggest that occupational therapists working in Canadian schools should collaborate with educators to promote all students’ success and participation (Hanft & Shepherd, 2016; Villeneuve, 2009). This means that occupational therapists should support not only students with formal diagnoses but also students without a diagnosis who are experiencing challenges with school-functioning ranging from fine motor skill difficulties to participation-related issues (Bolton & Plattner, 2019). Positive outcomes related to occupational therapy services include increased family and educator satisfaction, and improvement in students’ skills, functioning, participation, and well-being (Bazyk & Cahill, 2015; Missiuna et al., 2012).
Despite positive outcomes, challenges have been reported with school-based occupational therapy services in Canada, including long wait lists and inadequate amounts of service (Deloitte & Touche, 2010). These difficulties may stem from historical expectations about occupational therapists and their service delivery models, where pull-out services are expected and common, requests for detailed assessments are numerous, and occupational therapists receive limited support to work towards participation-related goals (Benson et al., 2016; Bolton & Plattner, 2019). Such challenges lead to other issues reported with school-based services in Canada and beyond, including the lack of support provided to educators to help them support children’s inclusion (Kalubi et al., 2015).
Increasing understanding of the roles occupational therapists can play in schools is one recommended strategy to maximize the impact they can have when supporting students (Bolton & Plattner, 2019). Moving away from pull-out, individually based, service delivery approaches to more universal design and health promotion approaches has also been suggested (Ball, 2018). In the United States, there is currently a push towards the use of Response to Intervention (RtI) and Universal Design for Learning (UDL) approaches (Garfinkel & Seruya, 2018). The same trend has also been observed in Canada, but it has been less formally documented. RtI refers to providing high-quality education through the use of multi-leveled services, aimed at supporting academic learning (Ball & Trammell, 2011; Burns & Ysseldyke, 2005). These models generally use three service levels, where Level 1 refers to universal services for many children such as an entire classroom, Level 2 to greater involvement with small groups of children, and Level 3 to more intense, individual services. UDL is a specific framework that can be employed when providing Level 1 services as part of an RtI model. Specifically, UDL can foster collaboration between health and education professionals to support the inclusion of students with disabilities into general education classrooms (Kennedy et al., 2018). It is only relatively recently that RtI and UDL have begun to influence occupational therapy practice, for instance, to support children with autism in schools (Grandisson et al., 2019; Missiuna et al., 2012). Indeed, there is a growing recognition that RtI- and UDL-based models might be more effective than traditional models in supporting students’ inclusion; however, there is still relatively little evidence supporting these beliefs.
One specific model developed in Ontario, Canada, known as Partnering for Change (P4C) (Missiuna et al., 2012), incorporates important aspects of RtI and UDL approaches and provides guidance to occupational therapists practicing in schools. P4C is a school-based service delivery model that promotes four core “C” principles: collaboration, coaching, and capacity building in context. In this approach, three levels ranging from more classroom-wide interventions (Level 1) to interventions for small groups of students (Level 2) to specific one-on-one interventions with students (Level 3) are included. Examples of Level 1 activities include workshops for students or educators, classroom observations, and the provision of classroom recommendations to educators, often known as “teacher coaching.” Through dynamic observation, when occupational therapists observe students struggling with Level 1 activities, they are encouraged to create small groups of students to trial problem-solving strategies. Level 3 includes individualized interventions with students that require more guidance. Specific health care consent is required to work with students requiring Level 3 interventions. These students will often also have an adapted education plan.
The P4C model, and its practices and impacts, have mostly been documented in Ontario schools, the context in which P4C was originally developed Campbell et al., 2016; Pollock et al., 2017). The only example of a published Canadian adaptation of P4C outside of Ontario comes from British Columbia describing the learning process, implementation challenges, and satisfaction with the implementation of an adapted P4C model in a primary school from the perspective of classroom educators (Wilson & Harris, 2017). However, the process of adapting P4C for that provincial context is not described in detail. The context in Quebec is very different from Ontario or British-Columbia, in that, in Quebec, no health care or education teams provide rehabilitation support in schools. In the few schools where occupational therapy services are provided, most interventions are provided on a traditional, one-on-one model directly to children (Jasmin et al., 2019).
Since educational and health care contexts vary greatly from one Canadian province to the other, and from one country to the other, it is important to explore how to maintain the core P4C principles and the effectiveness of the model while adapting the model to fit diverse contexts. Specifically, researchers who developed the P4C service delivery models have identified 16 attributes that support the implementation of the four core “C” principles (see Table 1 as well as https://www.partneringforchange.ca/p4c-in-practice/different/ and Hodson et al., 2014; Missiuna et al., 2015) could be implemented in different contexts (e.g., to explore how supporting educators in designing educational activities consistent with universal approaches, which is an attribute of building capacity, could be implemented in different contexts). Additionally, more information is required to document exactly how occupational therapists spend their time, describe what their practices look like, and generate recommendations to advance practice within this model. A better understanding of how the P4C model principles translate into concrete occupational therapy practices in different contexts would help support ongoing international efforts to implement and adapt P4C in a variety of countries and contexts.
Core Attributes of the P4C Service Delivery Model, Organized According to the 4 Cs
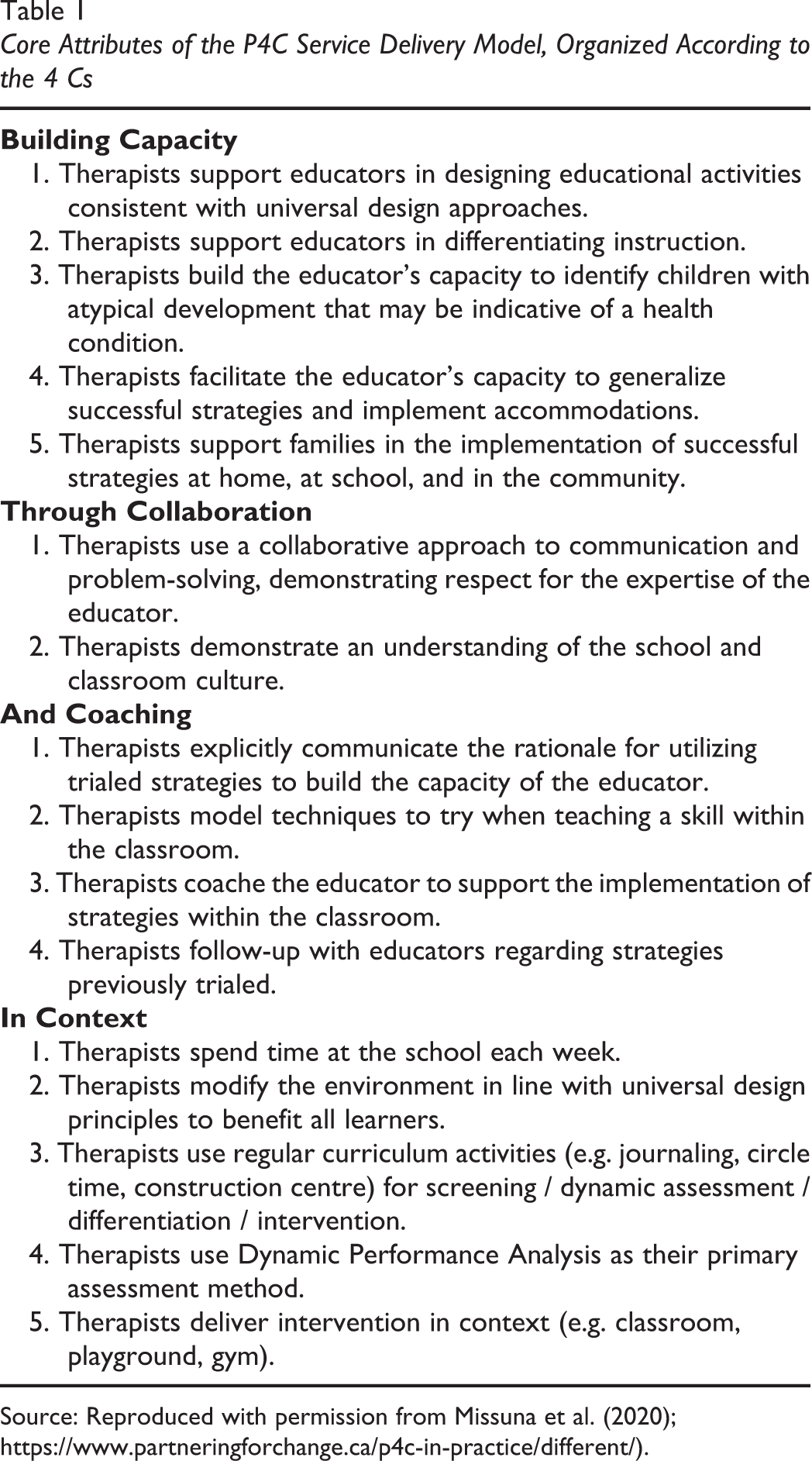
Source: Reproduced with permission from Missuna et al. (2020); https://www.partneringforchange.ca/p4c-in-practice/different/).
Our aim was to explore and describe how P4C could be adapted to, and applied in, the Québec school-based support services context (P4C-Q). Specifically, we sought to describe (a) the daily activities undertaken by occupational therapists applying the P4C-Q in two Québec elementary schools from different school-boards and (b) therapists’ and school-stakeholders’ (parents, educators, and school administrators) perceptions of the newly-introduced practices, perceived impacts of these practices, factors perceived to influence implementation, and recommendations. We also explored inter-school differences and similarities in implementation to generate lessons learned that could be helpful for others when implementing P4C.
Methods
Study Design
This study was undertaken following a participatory-action research (PAR) project to increase support for students with special needs in regular classrooms in Québec, Canada. Specifically, according to PAR principles where non-researchers define the research problem and engage in a problem-solving process (Camden & Poncet, 2014; Tandon, 2002), educational partners expressed the desire to better understand the roles of school-stakeholders in supporting children with special needs. A participatory approach guided the entire study, which comprised three specific research projects. In the first project, education- and health-system researchers worked with school-based partners to identify the roles of stakeholders working with students with special needs and to determine the supports needed to implement an RtI model to assist these students (Anaby et al., 2020, accepted). The second research project described how the RtI model was currently being employed in the province of Quebec. This research identified that the main barriers to the implementation of RtI models in Quebec were the lack of clarity in the expected roles, the lack of support for educators, and the limitation of the scope of current RtI models to behavioral or academic concerns, without taking into account underlying health or occupational issues that could be addressed by collaborative, tiered, school-based rehabilitation models such as P4C (Camden et al., 2020, submitted). These initiatives informed the third research project, proposed by the research team and described in this paper, which involved the adaptation and the implementation of P4C and explored how this model could support both school teams and students.
A quantitative-qualitative sequential mixed methods design (Creswell et al., 2003) was used. Specifically, a descriptive design was used both for quantitative and qualitative data to document the implementation (Palinkas et al., 2011; Sanelowski, 2000) of P4C-Q and the perceptions of the therapists and school-stakeholders’ (parents, educators, and administrators). Specifically, quantitative data were collected first through daily journals completed by the occupational therapists throughout the school year, while qualitative data to better understand the practices documented in the journals were collected at the end of the school year. Ethics approval was granted by the ethics committee of the research centre of the CHUS.
Context
In collaboration with our school-based partners, we chose two elementary schools with different sociodemographic profiles and experiences implementing RtI models, and who did not have any experience with the P4C model or with having an occupational therapist present at their school prior to the project. School A, from a Francophone school board, was a large school situated within an affluent community, but with a student population with very diverse ethnic and socioeconomic backgrounds. According to the provincial socioeconomic classification of schools, School A was considered to be a high socioeconomic school, even if important disparities existed within school neighborhoods, some of which comprised very low-income families. This school also had an important proportion of immigrant families. School A had been implementing some RtI specific interventions to foster academic achievement for a few years (e.g., learning French and mathematics) but had never had a school-based occupational therapist. School B, from an Anglophone school board, was located in a small Francophone city and had a smaller, less ethnically-diverse student population than School A, and was considered to be a middle-income school. School B was only beginning to implement RtI approaches, and only for literacy. Neither of these schools had defined special needs classes. Both schools included students with special needs in mainstream classes.
Adaptation of the Model
Several modifications to the model were needed to fit the Québec educational system, and our school-based partners’ expectations, as there are important differences in how services are delivered in Ontario and Québec. These differences are outlined further, along with our modifications to the four core P4C principles, based on these differences.
Differences in Service Delivery in Ontario and Québec schools
There are several important differences between the Ontario and Québec school health support services contexts. First, there are typically no rehabilitation professionals working in Québec schools. Most Québec schools have never had an occupational therapist providing services to their schools. Most Québec school boards provide Speech-Language and other health professional services for a few hours each month to respond to assessment and/or consultation needs, unlike the Ontario context where rehabilitation teams provide services to several schools. In P4C-Q, we maintained the same intensity of occupational therapy services as in P4C (seven-hour day once per week), and we asked therapists to use the core P4C principles focusing on collaboration with school teams, coaching, and capacity-building, and providing most of the intervention in context (Missiuna et al., 2012). We also provided therapists with mentoring, as recommended (Missiuna et al., 2012). Therapists completed the seven P4C training modules (about 14 hours), participated in mentoring meetings with the principal investigators monthly to discuss their practices and problem-solve together, foster the development of their competency, and ensure fidelity in the implementation of the model. Therapists were encouraged to reach out to each other or the research team whenever they had questions.
Second, P4C was originally designed to be used only with children with Developmental Coordination Disorder (DCD). More recently, the model is being adapted and applied in other contexts and with other populations (Blumenstock & Drew, 2017; Corelli & McClelland, 2017; Wilson & Harris, 2017). We instructed therapists to respond to the needs of all students, not just those with DCD, and according to their school-specific priorities that could come from the schools themselves and the needs they would observe. In the original model, evidence-based information was provided to therapists about DCD best practices. P4C-Q therapists were provided with the same DCD information, but it was not feasible to provide them with best practice information on all potential situations they might encounter. They were asked to explore best practices according to need when responding to specific student requests (behavioural issues as an example), or while designing an in-class/in-context activity, such as classroom management.
Third, we decided to place a greater emphasis on a continuum of care to foster collaboration between health and education sectors. In Québec, rehabilitation services are provided primarily in rehabilitation centres. Centre therapists may be contracted to provide support to schools, but only for specific students also receiving centre services (i.e., meeting eligibility criteria, and having significant participation restrictions). In addition, P4C-Q therapists were perceived as potentially having a key role in linking with community and health and social services to best support children. As a result, the therapists were encouraged to design activities in collaboration with external partners, and, if needed, to assess students to support the diagnostic process, or facilitate access to resources or services. This included removing students from the classroom for assessment when necessary. These assessments were not an aspect included in the original P4C. Therapists were, however, instructed not to emphasize assessment, but rather only to complete a formal assessment when it was deemed to be the best way to support students/families/schools. Occupational therapists were specifically asked to work as much as possible in context, and to respect the P4C approach and core principles.
Finally, in P4C-Q, a greater emphasis was placed on family engagement. In P4C, therapists were encouraged to contact families when students were receiving Level 3 interventions, but not necessarily at other levels. However, despite not being formally described in the original model, we are aware from the P4C research team that parent workshops were also implemented as initiatives in Ontario. Following discussions with our school partners, and to improve family-school collaboration for all students more globally, we decided to use a similar tiered approach with families. Specifically, therapists were explicitly encouraged to design general workshops for parents, to discuss different aspects of children’s development and the skills required to perform various school activities, as well as their roles in the school.
Participants
Two occupational therapists, both female, were recruited and delivered P4C-Q in their respective schools. The therapist at School A was already working for the research team as a research coordinator and the therapist at School B was already working part time in School board B (but was not providing services specifically in School B). School-stakeholders were recruited to take part in stakeholder interviews and included parents, educators, and administrators from the two school boards. In collaboration with school partners, a purposeful sample was used to select a variety of stakeholders who had significant interactions with the therapists, or who had opportunities to observe the therapists providing P4C-Q. The final pool of participants included the two occupational therapists, as well as one mother, six educators, one special educator, and three administrators.
Data Collection
Occupational therapy activities
Throughout the implementation process, therapists completed daily journals. The daily journal was developed by the research team and adapted from the P4C journals, which follow a RtI structure (i.e., asking information about activities done in Levels 1, 2, and 3 (Missiuna et al., 2015). Small modifications were made to reflect our adaptations, and to further capture information such as time spent by therapists on collaboration not perceived to be related to any leveled activities. Therapists responded to close-ended questions and reported on the number of different activities per day, time spent, and who participated in each activity as well as any additional information. Therapists were encouraged to include details such as the number of students seen in Level 3 activities (not relevant/feasible for Level 1 and 2). Time spent per day was recorded for each of the three levels and the collaboration activities, as well as communicating with community partners and performing research-related activities. The latter could include time spent completing journals, during mentoring meetings and when seeking evidence-based information. As an example, therapists were asked first “How many Level 1 activities did you do today?.” Then for each activity, they identified whether the activity occurred within the classroom or was intended for the broader school/community. They were then asked to determine the type of Level 1 activities among several options, and to report how much time they spent (in minutes) on this specific activity. Therapists were also asked to provide comments to describe the activities they conducted.
Therapists’ and school-stakeholders’ perceptions of therapy practices, impacts, and factors influencing implementation
At the end of the school year, individual, semi-structured interviews were conducted by two members of the research team who were independent of the targeted school. Interviews lasted between 25 minutes and 1 hour. Interviews were conducted either by a trained research assistant or by occupational therapists (i.e., the occupational therapist who worked in School A helped conducted interviews in school B, and vice versa). The interviewers used a semi-structured guide covering four main topic areas. First, parent, educator, administrator, and therapist participants were asked to describe their observations of the activities undertaken by the therapist (or self-perceptions for therapists), according P4C-Q level. Second, they were asked about their perspectives regarding the impact of these activities on their professional roles as well as any direct student impacts. Third, interviewers asked participants about the factors that they believed influenced implementation of this new model. And then fourth, they explored participants’ satisfaction with the project as a whole, and asked for suggestions to improve the project and/or future projects.
Data Analysis
Occupational therapy activities
At the end of the implementation process, we used SPSS software (IBM) to analyze the quantitative journal data descriptively, calculating frequencies and mean results for each journal item (e.g., “How may Level 1 activities did you do today?”), and analyzing the data separately by school.
Therapists’ and School-Stakeholders’ perceptions of therapy practices and impacts
All qualitative interview data were analyzed using NVivo software (version 12). Interviews were transcribed verbatim by one research assistant (CG). Transcriptions were analyzed following the thematic analysis process described by Braun and Clarke (2006), which is consistent with a descriptive qualitative design (Sandelowski, 2000). First, all research members became familiar with the data. At this stage, discussion between the occupational therapists, research assistants, and researchers led to the identification of key emerging ideas. The research assistant (CG) generated initial codes and, together with another research assistant (RD) and the principal investigator (CC), began to identify preliminary themes. As reflexivity plays a key role in thematic analysis (Braun & Clarke, 2019), researchers’ assumptions relating to the probable feasibility and effectiveness of the P4C model were shared upfront, and all team members were encouraged to stay true to the data and explore alternate explanations and criticisms of the model. This was fostered through regular, iterative discussion between the therapists who implemented the model and were part of the research team, the research assistants who were familiar with the data but less so with the day-to-day activities, and the researchers who knew the model. These discussions also fostered trustworthiness, to ensure all perspectives were represented and a consensus was achieved in the final interpretation of the data. Moreover, quotations from different stakeholders were selected to illustrate a varied range of perspectives.
Findings
Occupational therapy activities (journal data)
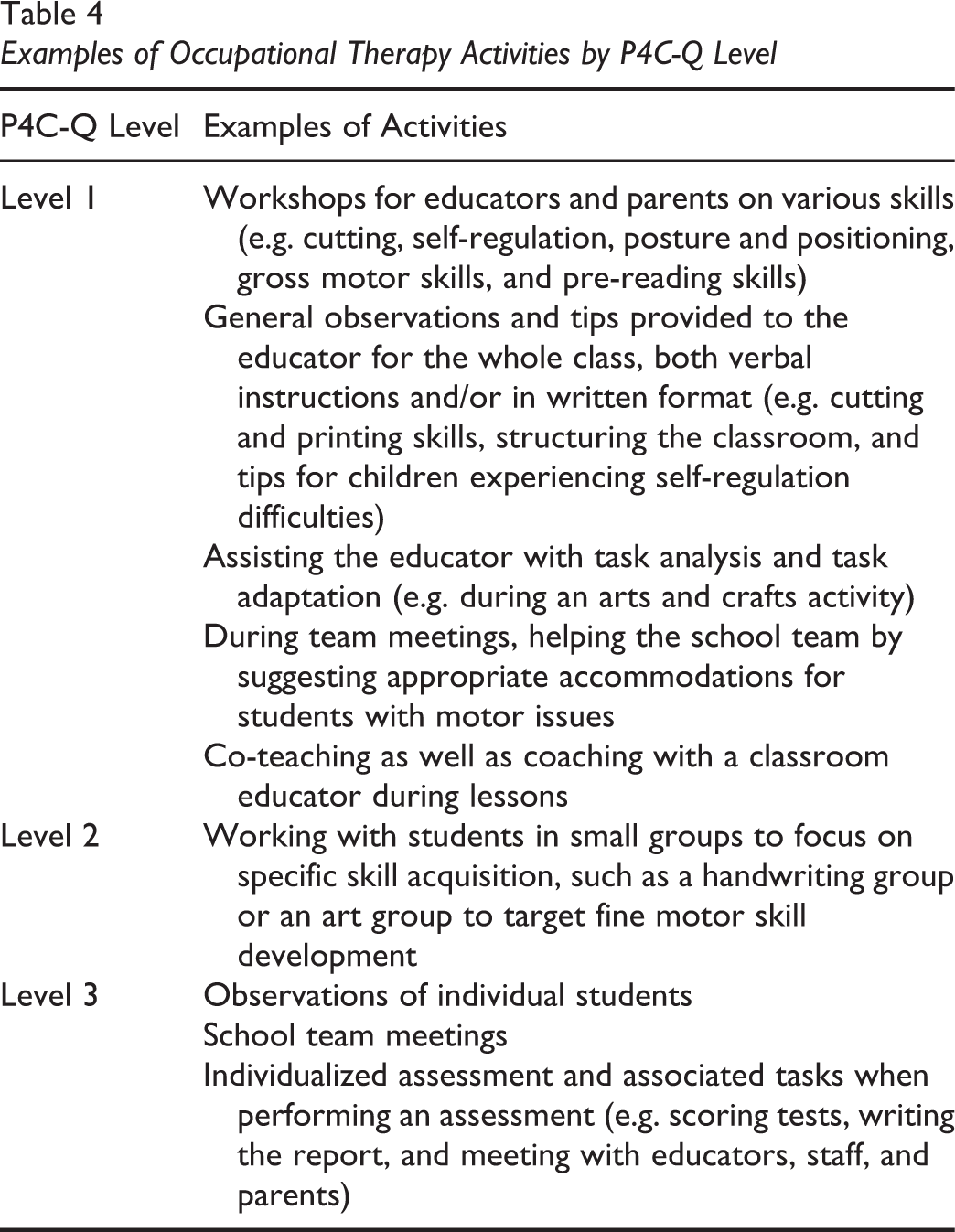
Table 2 outlines the journal activities, regarding time spent on broad categories of activities. The therapist providing services at School A (Therapist-A) worked 41 days and the therapist providing services at School B (Therapist-B) worked 46 days. Table 3 provides the average number of activities per year for both therapists, according to each of the P4C-Q levels. Therapist-A reported many more occasions of Level 2 activities than Therapist-B (46 and 6, respectively), including screening by observation, personalised teaching, and consultations. However, Therapist-A reported spending less time, nearly half, collaborating with other stakeholders. Therapist-B reported more time, on average, per day on Level 3 activities (75 minutes) compared with Therapist-B (29 minutes). However, the therapists reported seeing a similar number of students individually in Level 3 (seven and ten, respectively). In addition to reporting time performing Level 1, 2 or 3 activities, both therapists reported a substantial proportion of time spent on other informal activities related to collaborating, developing relationships, working with community partners, or performing task-related research. Both therapists described specific examples of activities performed at each P4C-Q level and these are found in Table 4.
Time Spent (in minutes) on P4C-Q Level Activities, by Activity Level and Per Day, Separated by School
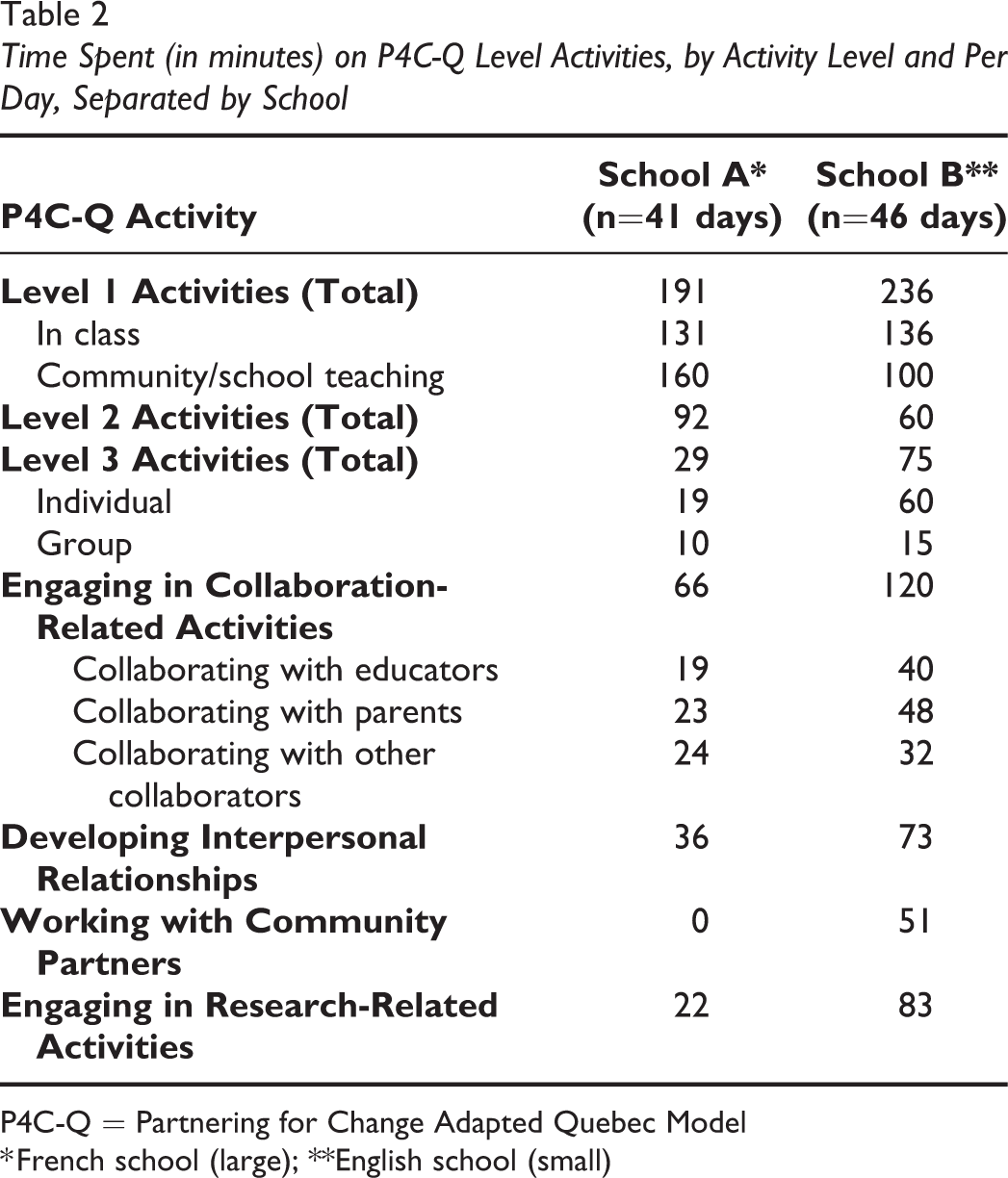
P4C-Q = Partnering for Change Adapted Quebec Model
* French school (large); **English school (small)
Number of Activities (or Children Seen) at P4C-Q levels, Per Year, Separated by School
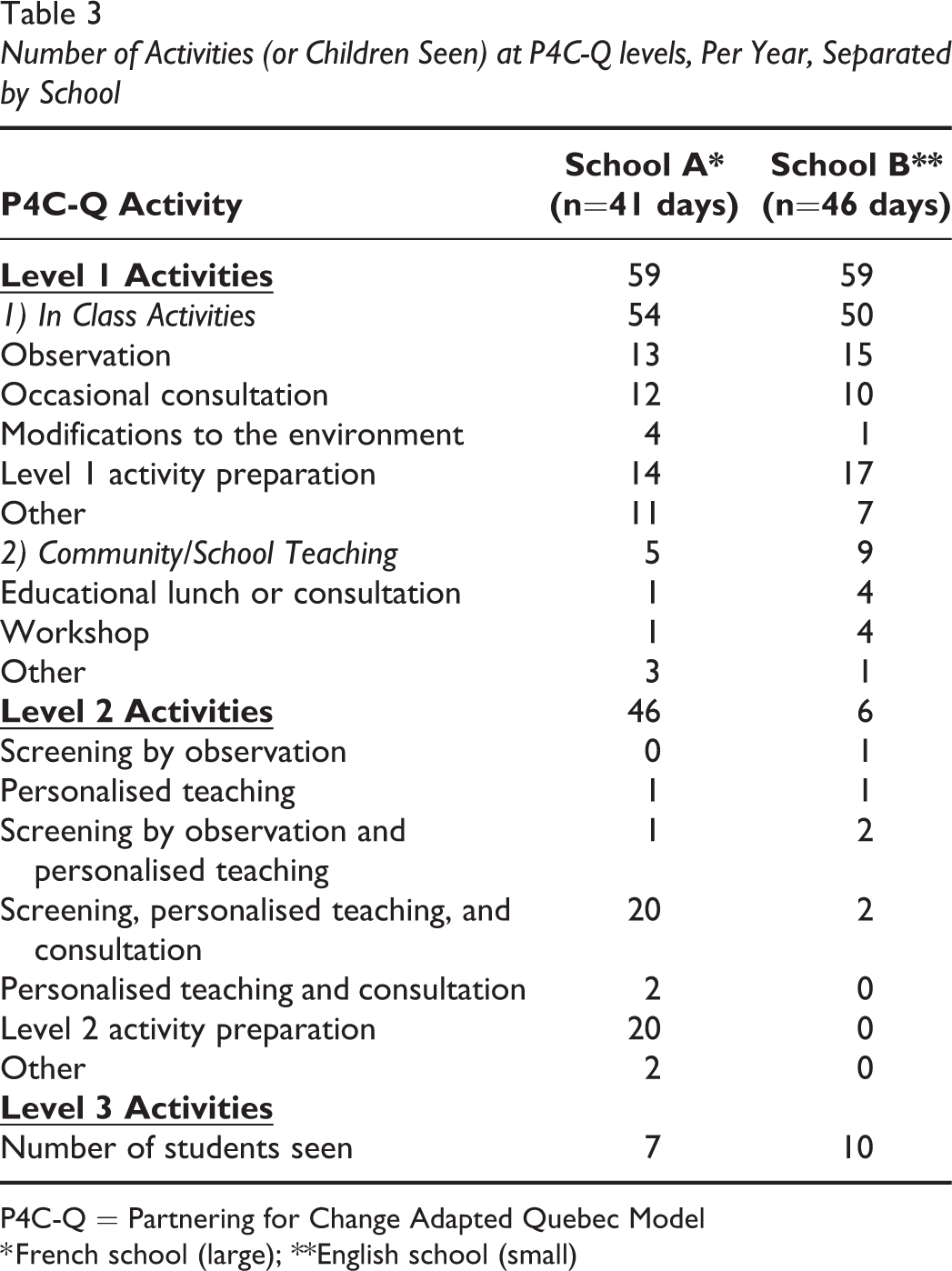
P4C-Q = Partnering for Change Adapted Quebec Model
* French school (large); **English school (small)
Examples of Occupational Therapy Activities by P4C-Q Level
Therapists’ and School-Stakeholders’ perceptions of therapy practices and impacts (interviews)
Since categories were similar across the two schools, results are presented for both schools simultaneously, and when present, differences are discussed. Results are presented according to perceived practices, impacts and factors influencing the implementation, with selected quotations freely translated from French to illustrate participants’ perspectives.
Perceived occupational therapy practices
Emerging themes illustrated practices at the three levels, and they demonstrated how collaboration and developing trusting relationships were interwoven throughout the descriptions: (a) A diversity of Level 1 services grounded in collaboration and coaching, (b) Fewer Level 2 activities using small-group interventions, and (c) Level 3 activities for individual interventions and assessments.
Collaboration and coaching were explicitly integrated into seven types of interrelated therapy practices identified for Level 1: (a) workshops for educators, (b) workshops for parents, (c) school-wide physical activities, (d) supporting educators, (e) informal discussions with educators, (f) specific observations in the classroom, and (g) providing recommendations. The following quotation illustrates an example of school-wide physical activities demonstrating how occupational therapists’ competences were valued for designing activities targeting large groups of students: We were working together on an active corridor and on the active corridor procedure, so we worked on the procedure, we were still working on it this week and we set up a corridor, she and I. I used her added value in occupational therapy for everything that is related to the motor skills of hands, feet, legs for first year students. (Special Educator, School A) She [the therapist] has provided extensive support to teachers in their understanding of children’s behaviour, both by coming into the classroom and by discussing outside the classroom. It has brought a new vision of children’s development. (Educator 1, School B) She [the therapist] also supported me a lot this year in relation to the questions I had about some students. I thought we were capping with some very young ones. She was able to give me a few more tools. There are things I already knew a lot about, but despite that, it was useful to have a second opinion with a perspective [in the classroom] that is not ours. She is an occupational therapist, so it brought another vision, it’s very interesting. I found her very relevant as a resource person in the school. (Educator 4, School A) I know that she also did small group workshops in class on certain topics. That’s one more service we were able to give to the students. (Administrator, School B) We noticed that having regular interventions responded to the needs of some children, some problems were resolved, and children developed ways to compensate for particular difficulties (Administrator 1, School A)
Perceived impacts
Emerging themes were the following: (a) building capacity in schools, (b) building relationships and supporting families, and (c) improving children’s functioning. Building capacity at the school level included improvements at the macro level, such as how schools organized support services. The therapist was perceived to be an important team player who could bring all school personnel and outside stakeholders to work together (e.g., having a common approach to support learning for a student with communication, motor, or behavior difficulties). As a consequence, participants described how their school was able to provide a new type of support services, and better identify children with special needs, as illustrated below: The occupational therapist provided additional support and we were able to go and evaluate other things we had never evaluated before. Without the expertise of an occupational therapist we are not able to make these connections there, because we don’t have the knowledge for it. (Administrator, School B) Discussions with the occupational therapist, both about a particular student and in general, made me think about how I approach student difficulties and classroom dynamics. She brought new ways of analyzing things (e.g., the student doesn’t listen because he didn’t move enough in the morning, he should move because it helps him concentrate). (Educator 2, School B) So it opened my eyes to a lot of things that I wonder now if I was failing to observe before. We now have lots of questions. I think that the first goal of the occupational therapist, it is to equip the educators so that we become more autonomous. (Educator 1, School A) Parents are sometimes more open to listening to recommendations that come from a healthcare professional. They also accepted that the occupational therapist works with other occupational therapists from another institution outside of the school, so it [increased continuity of services]. (Special educator, School A) But just one thing. It’s with communication. I had no idea what’s going on, what they’re going to do. I think communication is important. It might be nice to have the paper…you know the summaries with the smiley faces? You know? Like it went well or it didn’t go well, just the things that they did, how long was it, just a few things like this. Just a little something so we understand. (Parent, School A) Children really improved. I do see differences between the beginning of the school year and the end of the year, for their writing skills, for their motricity. (Educator 3, School A) Working with an occupational therapist helped [me] to pay attention to things we do not normally pay attention to. For posture, for instance. I have a child who[se] [feet] do not touch the floor. I hadn’t thought of modifying that. (Educator 3, School A) There is a child with whom the occupational therapist worked. I calculated at the beginning of the year that he could not stay seated more than 30 seconds on his chair. The occupational therapist provided me with recommendations, and the child really improved. (Educator 2, School A) Occupational therapy recommendations were provided at home, and the mother took it seriously. After a month, use of scissors was greatly improved. So it did have an impact at home too […] Something happened, it’s not only maturity. (Educator 1, School A)
Factors influencing implementation
Emerging themes illustrating factors influencing implementation included (a) Developing trusting relationships and creating openness, (b) therapists’ collaborative attitude and competency, and (c) ensuring appropriate resources and understanding of the model. Developing trusting relationship appeared to be influenced by characteristics of individuals, especially of educators and therapists. For educators, being open to having a therapist in the classroom to give them advice and understanding how the model worked were noted to be important factors to facilitate collaboration. Creating openness took time in both schools and it was necessary for the therapists to build a relationship of trust with all school staff, including administrative workers, educators, and administrators in order to get all the necessary materials, and for them to be able to go into classes and give advice that the educators themselves wanted. This quotation illustrates the importance of relationships:
First task I actually gave myself was to establish relationships and find my place, to establish relationships with everyone. Make everyone feel comfortable coming to see me, let them know who I am. Also with the janitor because I knew I was going to have to set up tables, for example. Then also with the administrators, but that was already well underway. The secretaries too, very important. It was not opportunistic. It was to be just friendly and not to have a professional status apart. I wanted to be part of the team. (Occupational Therapist, School A)
The therapists’ collaborative attitude and competency were highlighted in comments from other school-stakeholders, which reflected perceptions that both therapists were readily available and competent, which facilitated the implementation of P4C-Q. However, some perceived challenges were mentioned with regards to how therapists spent their time, with the caveat that many stakeholders mentioned that one day a week was not enough to follow up and complete all three model levels. As they perceived it, with more time came the possibility of addressing more classrooms, especially in schools with large numbers of students and classes. In the settings where this was a perceived factor, only some kindergarten and first grade classes had access to occupational therapy services and not necessarily every week. Many participants said that they would have appreciated more time with the therapist in class to get the most from her expertise. It was believed that if the therapist had more time, they would have liked for her to provide more Level 3 interventions, but more importantly, to support all educators in the school. The therapists started where they saw the greatest needs, or where educators were the most proactive in inviting her into their classrooms, but for some, it created inequities in how only some educators, some classrooms, and some students were supported. The two following quotations illustrate that both administrators and educators perceived that more therapist time was needed:
She went to class to do workshops with some targeted students, do other exercises, and there was not so much level 3 rehabilitation because a day a week was not necessarily ideal. (Administrator 1, School A)
I think it’s a shame, but I also understand that with the time that’s available, it’s not easy either. I think that all the teachers would deserve to have interventions in occupational therapy. It can help at the level of their time, but also at the organizational level, etc. (Educator 1, School A)
When appropriate resources and understanding the model are limited, it appears to negatively impact on the implementation of the model and on its perceived effectiveness, as illustrated earlier. Limited school budget to hire therapists more than one day a week was perceived not to be enough compared to the time required to deliver complete interventions. All school-stakeholders wished the model would be sustained, but that more time would be available to ensure greater service equity and enough time for students needing the most. Recommendations were also made with regards to better explaining, at the beginning of the year, what the therapist could do inside and outside the classroom, for students, educators, and families. Many school-stakeholders stressed that they felt they now had a clearer idea of the benefits of P4C-Q long-term to better understand students’ difficulties as well as learn how to modify and improve their teaching skills. Some stakeholders in School B mentioned their school decided to hire an occupational therapist for the following year as a result of this greater understanding of how therapists can support schools and students.
Discussion
This article described the occupational therapy activities and the perceived practices and impacts following the implementation of an adapted P4C model in two elementary schools in Québec, Canada. Results highlight the feasibility of implementing a model such as P4C in Québec, and provide clear descriptions of the modifications made, as well as the rationale underlying these modifications.
Despite the fact that several model modifications were made, similar results were obtained to those reported with the original P4C model, in particular, the high satisfaction from school stakeholders (Campbell et al., 2016; Missiuna et al., 2012). This might be explained partially by the fact that we made explicit modifications that had already been made by occupational therapists implementing the original model. For instance, we explicitly extended therapy service to all children within a school experiencing challenges. This may explain stakeholders’ perceptions that there was not enough time for the therapist to see all students needing service, potentially contributing to service inequities. Lack of time was noted as a concern with the original P4C model, and this may be exacerbated when therapists are asked to increase the number of children seen without increasing the dosage (i.e., available for seven hours, one day per week). Potential equity issues with occupational therapy and support services are well described in the literature, and can be influenced by many factors, including personal characteristics of professionals and educators, but also school characteristics and service expectations (Bose & Hinojosa, 2008). As recommended by others, clarifying what therapists can and cannot do, not only regarding their scope of practice (Shasby & Schneck, 2011), but also with the time and resources allowed, and setting clear priorities with school teams (not only with administrators), may be a way to ensure all stakeholders share a common understanding of the proposed services and can identify realistic expectations.
Regarding therapy activities, both quantitative and qualitative results contribute to our understanding of how therapists spend their time in daily multi-leveled activities. A strength of our findings for clinicians includes the very specific activities described at each level of the model in the daily therapy journals, which can be very useful for others wishing to implement a model, assisting with suggestions that are readily applicable “on the ground.” Next steps might include more support for therapists, as already suggested, but also more materials or resources, training on multi-level service delivery models, pre-service training for occupational therapists and/or educators on collaboration (Casillas, 2010; Dettmer et al., 2005; Shasby & Schneck, 2011; Vincent et al., 2008) and to building upon the repertoire of additional concrete examples of therapy activities in practice.
Our quantitative results indicate that therapists spent the majority of their time on Level 1 activities, as would be expected in this new model of service delivery, and based on the model’s core principles. The therapists used practices inspired by UDL approaches, and performed observations and conducted workshops as previously reported (Kennedy et al., 2018). Qualitative results highlight, however, the difficulties for therapists when determining which of their actions are associated with what specific activity level, given how integrated activity levels may be within the model and how often actions overlap with collaboration and relationship-building activities. This is actually seen as a positive, for it is a strong tenet of the model that collaboration and relationship-building should be continually used as strategies, regardless of activity level. In fact, while some might assign collaboration and relationship-building activities to Level 1, these principles are also used at Level 2 and Level 3, with the presumed distinctions related to the concepts being applied to group work or work with individual children (Camden et al., 2020, submitted). Combined with the qualitative results demonstrating how collaboration eventually led to the development of concrete activities, these findings stress the importance, but also the time that is required, to develop the building blocks necessary for the successful implementation of collaborative multi-level models such as P4C.
Even though study therapists functioned in different school environments, we found more similarities than differences across the two schools. In addition, the principles of the model were the same in both schools, suggesting the applicability of P4C-Q across different school settings. It aligns nicely with Jasmin and colleagues’ (2019) recommendations to use collaborative practices to develop school-based occupational therapy in Quebec. As such, the P4C-Q should be considered as a serious option for therapists and managers responsible for developing support services for children with special needs in Quebec.
One of the limitations of this study is the fact that it was undertaken in only two schools, thus limiting the generalizability of study findings. Moreover, although informal discussions helped to validate the interpretation of the data, no formal member checking was performed due to stakeholders’ time constraints, which might have limited trustworthiness. Another limitation is the fact that the perspective of students was not directly explored. Moving forward, it will be important to seek more evidence of what works, and in what ways, across contexts and potentially across teams of professionals. In addition, conducting effectiveness studies with larger numbers of schools and involving standardized outcome measures, including of performance and of satisfaction for educators and students, will be useful. In addition, it will be critical to investigate ways in which to make implementation of models such as P4C-Q sustainable. Finally, one of the two therapists had worked as a research assistant for the research team, which may have introduced a bias when describing her perceptions of the implementation and impact of P4C-Q. This was addressed as much as possible by the training and the support mechanisms that were put in place, and by exploring the perceptions of other stakeholders associated with the school where she worked.
Conclusions
Adapting and implementing P4C in Québec was feasible and increased perceived satisfaction among key stakeholders including educators, parents, and school administrators. Occupational therapists devoted substantial time to identifying their schools’ needs and to building trust and rapport with their school teams. This relationship-building was reported to be related to the positive outcomes described by stakeholders. Recommendations provided here by stakeholders will be useful to guide the next steps in implementation and to promote long-term sustainability of this new service delivery model.
Key Messages
A key aspect of the Québec P4C model, as in the original model, is the emphasis on identifying the needs of educators, parents, and school stakeholders prior to school interventions.
Collaboration and relationship-building are key factors in model success.
While substantial time must be spent on building rapport and trust, in addition to universal and individual approaches in therapy, these are essential for effective implementation.
Footnotes
Acknowledgements
We want to thank all study participants, and in particular, our partners from the school boards who made this pilot feasible. We also want to thank all members of the GOLD research team.
Funding
This study was funded by a grant from the Fonds de Recherche du Québec – Société et Culture. The first author is funded by a salary award from the Fonds de Recherche du Québec – Santé.