
Abstract
Background.
Client-centred practice has been part of occupational therapists’ identity for several decades. However, therapists have begun to question whether the term obstructs critical relational aspects of therapy.
Purpose.
The purpose of this article is to summarize critiques of the use of the term client-centred and propose an expanded descriptor and a fundamental shift in how occupational therapists engage with individuals, families, groups, communities, and populations.
Key Issues.
Three themes summarize critiques of how client-centred practice has been envisioned: (a) the language of client-centred, (b) insufficient appreciation of how the therapist affects the relationship, and (c) inadequate consideration of the relational context of occupation. We propose collaborative relationship-focused practice that has key relational elements of being contextually relevant, nuanced, and safe, and promotes rights-based self-determination.
Conclusion.
We argue that these essential relational elements, along with a focus on occupations, are required to promote occupational participation, equity, and justice.
Introduction
Canadian occupational therapists were among the first health professionals to embrace client-centred practice as a key feature of their work. Since 1983, client-centredness has shaped professional identity in Canada (Department of National Health and Welfare & the Canadian Association of Occupational Therapists, 1983), and has been endorsed internationally (World Federation of Occupational Therapists, 2010). However, occupational therapists have begun to question whether the term obstructs critical issues for relational aspects of occupational therapy. The purpose of this article is to propose an expanded descriptor of the relational qualities necessary for occupational therapists to provide high-quality and ethical therapy. We will review the introduction of client-centredness as a descriptor of how occupational therapists engage with the people receiving their services and highlight the key concepts of client-centredness espoused in occupational therapy literature. Next, we will describe how client-centred practice has been critiqued. Finally, we will propose collaborative relationship-focused practice as a descriptor that signals a fundamental shift in occupational therapy practice. We will conclude by identifying implications for practice.
History of Client-Centred Practice in Occupational Therapy
The Guidelines for the Client-Centred Practice of Occupational Therapy, published in 1983, was seminal in identifying occupational therapy as a client-centred process that conceptualizes clients as integral parts of their environments and social systems (Department of National Health and Welfare & the Canadian Association of Occupational Therapists, 1983). Influenced by the work of Carl Rogers, the Guidelines described occupational therapy as client-centred practice. Rogers (1977) asserted that the quality of the therapist–client relationship in psychotherapy is characterized by a strengths-focused appreciation and acceptance of clients, listening, and supporting movement toward their aspirations. The Guidelines reinforced the importance of a humanistic and holistic view of people as active participants within therapy relationships.
Additional clarification of occupational-specific client-centred practice identified in the Guidelines appeared in the 1990s. Townsend et al. (1990) cited foundational beliefs underlying client-centred practice including the worth of individual and collaborative assessment with clients. Sumsion (1993) noted that client-centred practice includes assessments that focus on “client identified problem areas rather than those identified solely by the therapist” (p. 7). Law et al. (1995) drew upon occupational therapy literature, to propose a definition of client-centred practice that included concepts of client strengths and autonomy, partnership, and accessible services. Sumsion (2000) emphasized the importance of participating “actively in negotiating goals which are given priority and are at the centre of assessment, intervention and evaluation” (p. 308).
Key Features of Client-Centred Practice in Occupational Therapy
Since the introduction of occupational therapy-specific descriptions of client-centred practice, key features have been highlighted. These features include respect, collaboration, and power-sharing. Respect for client values, perspectives, knowledge, abilities, and experiences has been endorsed as a core value underpinning client-centred practice (Canadian Association of Occupational Therapists, 1997; Hammell, 2013a; Law et al., 1995; Sumsion, 2000; Townsend et al., 2013). Building on ideas of respect, collaboration has also taken a prominent place as a key feature of the therapy relationship. Collaboration aligns with client-centred principles that recognize clients’ right to make choices and decisions about their needs and occupational therapy services (Law et al., 1995). In particular, collaborative goal setting has been embedded in occupational therapy practice models (Fearing et al., 1997; Polatajko et al., 2007) and outcome measures (Law et al., 1991).
Townsend et al. (2013) associated collaboration with power-sharing between the therapist and client. Acknowledgment of the power structures inherent in therapy relationships has been identified as a key principle of client-centred practice (Townsend et al., 2013). This acknowledgment extends beyond the therapist–client relationship to consideration of the social, political, and institutional structures in which occupational therapy is positioned. Social, political, and institutional rules and norms can dictate the nature of the therapist-client relationship and constrain the possibilities for occupational therapy processes and interventions. These ideas have prompted critical reflection on enacting client-centred processes in everyday practice including what occupations are valued, by whom, and in what context (Gupta & Taff, 2015).
Argument and Critical Discussion
Client-centred practice has retained a prominent place in occupational therapy guidelines, textbooks, and competency documents in Canada (Association of Canadian Occupational Therapy Regulatory Organizations, 2011; Canadian Association of Occupational Therapists, 1997, 2012; Fearing & Clark, 2000; Townsend & Polatajko, 2007) and internationally (World Federation of Occupational Therapists, 2010). As elements and processes of client-centred occupational therapy have been experienced and defined, critiques of the concept as it is used in contemporary occupational therapy practice have been forwarded. These can be summarized in three major themes: (a) the language of client-centred, (b) insufficient appreciation of how the therapist affects the therapy relationship, and (c) inadequate consideration of the relational context of occupational participation.
Language of Client-Centredness
For Rogers (1977), movement from the language of patient to client was necessary to direct the focus away from the biomedical problem to the person’s potential for growth. Unfortunately, the growth of neoliberal approaches to health care has caused the term to become associated with the commodification of health services which can lead to stigmatization (Costa et al., 2019). Viewing health services as a commodity negates the real differences in power and types of knowledge held between a person seeking health care and a health care provider, obscuring the potential for a collaborative relationship. Commodifying occupational therapy also raises ethical issues related to the ability to pay versus the need for therapy.
Although “clients” have been defined as individuals, families, groups, communities, organizations, and populations (Townsend et al., 2013; World Federation of Occupational Therapists, 2010), conceptualizations of clients as individuals persist. A large body of literature on family-centred care (Cunningham & Rosenbaum, 2014) and efforts to frame communities as clients (Hyett et al., 2019) acknowledge a broader perspective of the social units with whom therapists work. However, occupational therapists continue to be grounded in an individualistic perspective (Gerlach et al., 2018).
Insufficient Appreciation of How the Therapist Influences the Therapy Relationship
Grounded in biomedical models of “professionalism,” there is a prevailing view that within therapeutic relationships, therapists are expected to “bracket” their histories and identities so these do not influence therapy decisions. However, the therapist’s race, gender, abilities, culture, history, and other factors have profound influences on their knowledge, beliefs, and attitudes, which affect their moment-to-moment therapy decision-making and relationships with the people who access their services (Hammell, 2013b). Therapists’ taken-for-granted assumptions about people, occupations, occupational therapy, health, wellness, abilities, and society influence how they interpret the behaviours and the legitimacy of the goals and aspirations of the people, families, groups, communities, and populations they work with. With the exception of a few scholars who have advocated for critical self-reflection by occupational therapists (Beagan, 2015; Duggan, 2005; Hammell, 2013b; McCormack & Collins, 2010; McCorquodale & Kinsella, 2015), the discourse about client-centredness is relatively silent on therapists’ acknowledgment of their own social positionality and how their social positions affect therapy relationships.
Inadequate Consideration of the Relational Context of Occupational Participation
There is limited acknowledgment in current client-centred practice discourse about consideration of the diverse ways that individuals and collectives relate to each other, and their physical environments, histories, ancestors, cultures, knowledge, and social, political, and economic structures. Health disparities related to social, political, and economic disadvantages experienced by individuals and collectives are well documented (Public Health Agency of Canada, 2018). In particular, Indigenous people in Canada have experienced a plethora of legally and socially sanctioned injustices and oppressions that continue to affect all aspects of their lives including health, well-being, and relationships with family, community, culture, traditional knowledge, and the land (Reading, 2015). Although the experiences of Indigenous people are unique, injustices and disadvantages are also accrued on additional individuals and groups according to socially determined identities such as race, ethnicity, being an immigrant or refugee, socioeconomic status, sex, gender, sexual orientation, ability, and age. Despite knowledge about these impacts, the social, political, and economic influences on people’s autonomy and occupations have received inadequate attention in the education of occupational therapists (Fleming-Castaldy, 2015) or current client-centred practice (Fransen et al., 2015).
Racism and stigma have been identified as major public health concerns (Tam, 2019). Discrimination related to race, sexual identity, and a variety of health conditions, including but not limited to, HIV, mental illness, obesity, and substance use is experienced by people both outside and within the health system (Tam, 2019). However, there has been little acknowledgment of occupational therapists’ practices or complacency that perpetuate racist and oppressive practices and structures.
The principles of client-centred practice (Law et al., 1995) are a starting place for an approach to respectful, collaborative, and power-sharing therapy relationships. We advance the argument that current conceptualizations of client-centred practice have failed to address adequately the justice and equity challenges embedded in the delivery of occupational therapy education, clinical practice, and research. Some authors have argued that claims of client-centred practice have become rhetorical (Hammell, 2013c) while the fundamental effects of structural and systemic issues that affect people’s occupational participation are ignored (Restall et al., 2016).
The Case for Collaborative Relationship-Focused Practice
Given the above critiques, we assert that it is time for an evolution in both lexicon and practice to collaborative relationship-focused practice. We argue therapists’ interactions with the people they serve need to explicitly focus on the development of collaborative relationships. To build on the key principles of respect, collaboration, and power-sharing and to address critiques of client-centred practice, we draw on literature and experiential evidence to identify the essential relational elements of developing a collaborative relationship-focused practice that fosters peoples’ occupational participation and engagement. The goal for therapists is to develop collaborative relationships that are contextually relevant, nuanced, and safe, and that promote rights-based self-determination. We argue that these essential relational elements, along with a focus on valued occupations, are required in collaborative therapy relationships to work in partnership with individuals, families, groups, communities, and populations to promote occupational participation, justice, and equity.
Contextually Relevant Relationships
Collaborative relationship-focused practice requires critical reflection on the contextual and relational elements of developing therapy relationships. It begins with the acknowledgment that therapists are an integral part of the relational context of therapy. As in any relationship, the therapist’s critical self-awareness is essential (Duggan, 2005; McCormack & Collins, 2010; McCorquodale & Kinsella, 2015). One of the greatest barriers to accepting the goals and preferences of people who use occupational therapy services is conflicting values and beliefs (Cameron et al., 2018; Óladóttir & Pálmadóttir, 2017). An oft-cited example is the tension created when the therapist’s ideas of safety and therapy recipient’s rights to make informed decisions about risk clash (Kessler et al., 2019). This tension is enacted in pressure to relocate to supervised settings on hospital discharge or accept unwanted services or equipment (Durocher et al., 2015). It also is enacted when therapists decline to engage service recipients in goal setting (Cameron et al., 2018) or, when engaged, prioritize some goals over others based on their own perceptions of what is best for the service recipient (Kessler et al., 2019; Levack et al., 2011).
These documented tensions do not tell the whole story. The values, beliefs, decision-making, words, and deeds of therapists within therapy relationships are scripted from many places, experiences, and information sources, and often are outside of therapists’ awareness. A collaborative relationship-focused practice requires therapists to be continuously aware of their own social positionality and the privileges and disadvantages accorded by their social identities including, but not limited to, race, sexuality, gender, and ability. They also need to be aware that the imposition of dominant worldviews about occupational choices can result in implicit or explicit aggression toward individuals or collectives (Bailliard et al., 2020).
The conscious and implicit biases held by a therapist can have devastating effects on the people who use their services, creating health inequities (Tam, 2019), and limiting the possibilities for collaborative relationships. Therapists have a moral and ethical duty to understand their own biases, and how their biases and stereotypes influence therapy relationships (Krupa, 2008). Ongoing life-long critical self-reflection by health care providers of social positioning, bias, and structural allotment of privilege and oppression was coined “cultural humility” by Tervalon and Murray-García (1998). Commitment to cultural humility has an important contribution to creating a better relational context in occupational therapy (Beagan, 2015; Hammell, 2013b). Expressing humility recognizes one’s own biases and respectfully acknowledges the importance of diverse worldviews, values, and ways of being.
The influence of coloniality and White race and Western epistemological dominance combined with a prevailing history of exclusion, discounting, and structurally violent efforts to erase other ways of doing and being—such as has been experienced by Indigenous people in Canada—has been profound (Allan & Smylie, 2015). These macro-level forces have shaped the institutions and communities in which occupational therapy relationships occur, yet their influence has been made largely invisible and accepted as the norm in a cloak of White supremacy of knowledge, theories, and ways of being (Grenier, 2020). Increasingly, occupational therapists have been encouraged to critically reflect on current models of occupational therapy practice (Hammell, 2009) and how the policies and processes of organizations and institutions facilitate or constrain therapy relationships (Restall et al., 2003). Better relationships and outcomes are possible when therapists critically reflect on how collaborative relationships are built or undermined within the institutions and structures in which they work. As suggested by Hyett et al. (2019) in describing case studies of community development work, mapping power relations both inside and outside therapy relationships can illuminate opportunities for redistribution of power within social structures.
Relationship-focused practice means that therapists must do the hard work of understanding the micro-, meso-, and macro-level influences on themselves and on the individuals, and collectives who use their services and the forces that facilitate or constrain relationship building. It requires therapists to examine how issues like stigmas, ableism, and racism are enacted in systemic, intrapersonal, epistemic, and interpersonal practices and structures (Allan & Smylie, 2015; Krupa, 2008). It requires therapists’ active engagement in addressing equity and justice issues in everyday practice.
Nuanced Relationships
Collaborative relationships are nuanced contextually and temporally. Contextually, the therapist needs to understand what, from the client’s perspective, is needed in the therapy relationship and to what outcome. Variability in individual and contextual factors are important considerations in building collaborative relationships. Relationships with individuals are different from relationships with communities (Janse van Rensburg, 2018). It is incumbent on the therapist to be critically conscious of how to build and evolve respectful collaborative relationships with the people and collectives with whom they work.
All relationships, whether short or long term, require time and attention to build. How time is allocated in everyday practice can create ethical tensions for therapists as time spent meeting institutional demands often takes time away from other activities including spending time with people receiving services (Motta-Ochoa et al., 2019). Although time has been cited by therapists as a barrier to developing collaborative relationships (Mortenson & Dyck, 2006), therapists can build relationships, even within very short-term services, by listening carefully to people’s experiences and concerns (Trudelle, 2016). Based on an auto-ethnography of three therapists (speech and occupational therapists) who were in the process of changing their practices to spend more time developing therapy relationships, Bright et al. (2012) concluded that spending the time to determine a person’s story was vital to achieving meaningful outcomes. Likewise, therapists in Leclair et al.’s (2019) study identified the importance of taking the time to be present and interact in nuanced formal and informal interactions to build relationships in community development work.
Relationships are also nuanced over the length of time in which therapy occurs. For example, what is relevant and valued can change over the course of recovery from a serious injury or illness (Hunt & Ells, 2011). In addition, the role of the therapist in the therapy relationship may need to change. For example, results of Van de Velde et al.’s (2016) study suggested that, in the early stages of rehabilitation, a more therapist-directed role was important when bio-medical concerns were central to survival. A less directive role was important when psychosocial concerns and longer-term planning needs were paramount in the later stages of recovery. Thus, a nuanced relationship requires therapists to adjust their approach according to the perspectives and goals of the people using services that can change over time (Cott, 2004).
Safe Relationships
Safety is a cornerstone of a collaborative relationship-focused practice. It involves preventing harm and keeping risks to people receiving services to a minimum (World Health Organization, 2021). In this context, safety does not preclude the right of people to determine their own level of acceptable risk but rather refers to the prevention of harm created by the occupational therapist, either intentionally or unintentionally. Physical risks, errors, or omissions in the delivery of occupational therapy can cause harm, as can ineffective, inappropriate, or missed opportunities for intervention (Canadian Association of Occupational Therapists, 2011). Safety requires therapists’ lifelong commitment to ensuring currency in critical thinking and the technical aspects of their areas of practice. In addition, they need to be vigilant about the ways they may be unintentionally creating unjust inequities in access to, and quality of, occupational therapy service (Restall et al., 2018).
Emotional safety is also important. Discounting of cultural and spiritual beliefs of people receiving services erodes trust and opportunities for mutual respect and collaboration. Safe collaborative relationships require therapists to be attentive to the verbal and nonverbal ways they demonstrate respect through humility and openness to understand cultural practices, spiritual beliefs, and ways of being that are different than their own and the dominant society. In addition, personal boundary crossing and violations can create emotionally unsafe spaces for therapy relationships. Boundary violations occur when relationships change from a therapy alliance to a personal alliance, with the therapist’s actions, consciously or unconsciously, motivated by meeting their own needs, rather than those of the person receiving services. Therapists have an ethical responsibility to be aware of these dynamics and be vigilant about reducing the effects of transference and countertransference issues on themselves and the people receiving services (College of Occupational Therapists of Ontario, 2015). This does not preclude the development of reciprocity in human relationships that enhances, rather than harms, the wellbeing of individuals and collectives using occupational therapy services.
Cultural safety is an important component of collaborative relationship-focused practice. Originally described in the context of culturally safe health care that addresses the needs of Indigenous people in Western colonial health care systems (Papps & Ramsden, 1996), it has been advocated as an important component of occupational therapy relationships for many years (Gerlach, 2012; Gray & McPherson, 2005). Overall, cultural safely incorporates practices that consider the social, political, and historical contexts in which health care occurs (Tam, 2019). It requires emphasis on power relationships and resulting inequities that are embedded in the underlying forces of historic and current social and political contexts (Curtis et al., 2019). The First Nations Health Authority (n.d.) described culturally safe health care professionals as adopting “a humble, self-reflective clinical practice that positions them as respectful and curious partners when providing care” (p. 3). Anti-racist, anti-oppressive, and trauma-informed approaches that recognize root causes of historic, intergenerational, and contemporary trauma are important (Tam, 2019). Cultural safety involves therapists’ consideration, analysis and reduction of systemic power imbalances, discrimination, and colonization (Baba, 2013). Occupational therapists have a duty to address these systemic issues that create barriers to safe occupational therapy practices (Restall et al., 2016).
Safety is essential in collaborative relationship-focused practice and includes physical, emotional, cultural, and spiritual dimensions. It requires attention to what makes practice environments safe overall, and a more nuanced understanding of what makes a practice context and relationship safe or unsafe for the people or collectives with whom therapists work. For example, a White older adult man being admitted to a health institution may feel confident in the health system and care providers, and relatively safe in that environment. In contrast, an Indigenous man admitted to the same institution may feel very unsafe with the health system and care providers due to historic traumatic experiences with health or other institutions such as residential schools. A transgender woman with a disability may feel unsafe due to past experiences in the health system in which providers disregarded her accounts of her life, symptoms, or goals. Occupation therapists have an imperative to understand trauma in its many forms and its effects on occupations (Edgelow et al., 2019), and an obligation to create safe spaces that avoid retraumatizing the people who use their services. Safe practices must be defined from the perspective of the person or community receiving services (Baba, 2013; Curtis et al., 2019; First Nations Health Authority, n.d.; Tam, 2019).
Promotion of Rights-Based Self-Determination of the Individual, Family, Groups, Community, or Population
The Cambridge Dictionary (n.d.) defines self-determination as “the ability or power to make decisions for yourself, especially the power of a nation to decide how it will be governed” (para. 1). We adopt a rights-based definition grounded in the idea that people have the power to make decisions that affect one’s life and community. The Declaration on the Rights of Disabled Persons (United Nations, 1975), the Declaration on the Rights of Indigenous Peoples (United Nations, 2007), and the Declaration of First Nations (Assembly of First Nations, n.d.) are examples of this rights-based approach. Gibson et al. (2015) have asserted that “self-determination should be central to both occupation and occupational therapy” (p. 215).
We argue that the concept of promoting individual and community self-determination incorporates elements of power-sharing, facilitating participation in decisions about therapy goals and interventions, and encompasses a broad perspective of people as embedded within their rights and responsibilities to themselves, their families, and their communities. People using health and social services often need to make complex decisions and choices, including their level of participation in decision-making. Collaborative relationship-focused practice includes processes through which therapists co-create, along side the individuals and collectives they work with, opportunities that facilitate shared decision-making about goals, interventions, processes, and outcomes. This requires therapists to acknowledge the diverse worldviews that influence decisions about health, wellbeing, survival, and responsibilities to family and community and how these conceptualizations may differ from those of the dominant culture and the therapist’s own worldviews. Acceptance of peoples’ worldviews, along with respect and trust, set the stage for individuals and collectives being more likely to engage in shared decision-making processes toward self-determination (Groot et al., 2020; Jull et al., 2015). The relational aspects of choice and decision-making are also important to take into account (Durocher et al., 2015; Hunt & Ells, 2011). Social, political, cultural, economic, and environmental factors facilitate or constrain choices. Adequate information is a necessary prerequisite to making informed choices (Stefánsdóttir & Thóra Egilson, 2016). Thus, cultural and health literacy factors in knowledge translation communication are also important to building trust and collaborative engagement (Jull et al., 2015; Groot et al., 2020).
Constraints to people’s opportunities imposed by social, economic, and political structures are important considerations for practice and it is therapists’ responsibility to work within their circles of influence to address barriers (Restall et al., 2018). We advance an approach to collaborative relationship-focused practice that includes an attitude of respect for the rights, strengths, and capacities of people and communities for self-determination, demonstration of acceptance of diverse worldviews, and attention to creating opportunities for culturally and health literacy appropriate collaboration.
Implications and Conclusion
Client-centred practice has been a cornerstone of occupational therapists’ identity for several decades. We have argued that the individuals and collectives that occupational therapists serve must continue to be at the centre of doing occupational therapy. However, occupational therapists can no longer ignore the effects of colonization on the creation and perpetuation of health and social inequities for Indigenous Peoples, and additional groups who experience structural violence and marginalization. We propose that the collaborative relationship-focused practice of occupational therapy better captures the appropriate way forward to promote occupational participation, equity, and justice.
We acknowledge that therapists may face challenges when putting the principles of relationship-focused occupational therapy into practice. Barriers are embedded in institutional social structures that give preference to biomedical approaches (Sumsion & Smyth, 2000) and the goals and expectations of practice environments that limit time for relationship building and choices about therapy (Phoenix & Vanderkaay, 2015). As well, therapists may internalize biomedical ideas and Western-based social norms resulting in difficulty identifying possibilities for moving beyond them (Townsend, 1998). Lack of attention to the broader social structures that limit clients’ occupational possibilities has also been identified as barriers (Rudman, 2005; Sauvé-Schenk et al., 2019). Despite a recognition that social and structural factors affect the identification, pursuit, and achievement of goals identified by individuals and collectives, many therapists report that they do not address these systemic issues in their practices (Pitonyak et al., 2015; Restall & Ripat, 2008). However, therapists can make a positive difference by addressing these issues. Creating collaborative relationships is an essential step in that process.
Altering language and re-conceptualizing occupational therapy practice may be celebrated by some and criticized by others. The health care system has increasingly adopted the language of client-centred care and there is a risk of not falling into step with inter-professional language. The unique perspectives of occupational therapy should make obvious the need to think about relationships with the people and communities in new, more expansive, and critical ways. To promote equity and justice, building truly collaborative relationships that are contextually relevant, safe, nuanced, and promote rights-based self-determination is the way forward.
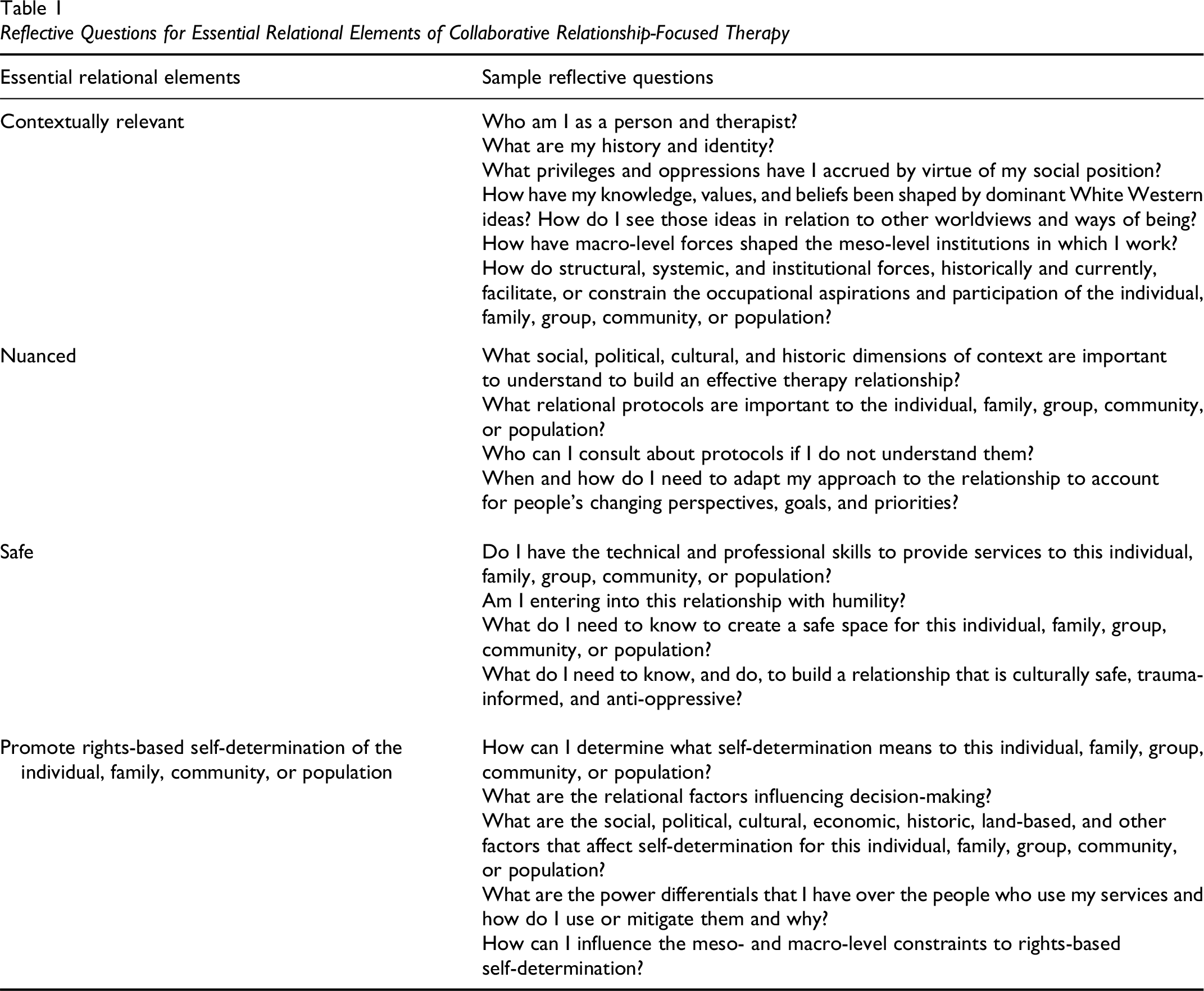
Relationship-focused occupational therapy has implications for individual therapists, researchers, and organization leaders. Individual therapists must earn their place within a relationship. Personal and collective stories are sacrosanct. Therapists must earn the gift of hearing the stories of people’s occupational aspirations and being in the relationship (Smith, 2006). Therapy relationships can come more easily when context and commonalities align but can be hard work when social structures, social positions, and an array of sources of diversity create chasms and challenges that must be crossed for therapists to be effective in their everyday practice. There are many layers to relationship-focused practice. Relationships require therapist self-knowledge and the ability to build relationships with diverse people and collectives. There is no entitlement under the guise of professionalism or having a particular knowledge base, and the work of building collaborative relationships is not optional. Truly collaborative relationships are demanding for everyone involved (Bjørkedal et al., 2016; Phenix & Valavaara, 2019). Table 1 provides reflective questions for each of the essential relational elements of collaborative relationship-focused practice to help guide therapists in working in this way.
Reflective Questions for Essential Relational Elements of Collaborative Relationship-Focused Therapy
Researchers can promote critical reflection on the ideas presented here. Research can help define the ways that the essential elements of collaborative relationship-focused practice are taught in educational programs and enacted in diverse practice settings. Understanding the experience of this approach from the perspectives of the people who use occupational therapy is essential.
Leaders in occupational therapy organizations have a role in supporting change to further this vision of collaborative relationship-focused practice. Real change will occur when the institutions that guide and govern occupational therapy support occupational therapists in doing the full extent of collaborative relationship-focused practice. Occupational therapy educational programs need to prepare graduates for critical reflection on themselves, occupational therapy practices, the systems in which they practice, and the structures that promote and constrain occupations and occupational therapy practice (Hammell, 2015). Understanding colonization and its sustained negative impact on the health and wellbeing of Indigenous Peoples needs to be an integral part of every program, as does understanding the origins and effects of racism and stigma. Curricula needs to include a focus on developing knowledge of the systemic and structural determinants of health, well-being, and occupational participation. There needs to be widespread education for developing the knowledge, skills, and attitudes to disrupt systems and structures that create inequities and to act in solidarity with equity-seeking groups. Leaders of professional organizations have a role in decolonizing occupational therapy practice and supporting leaders and therapists from communities experiencing structural violence and oppression to have a greater role in promoting change. Leaders can influence systems and structures, including educational program accreditation standards, by placing a greater emphasis on relational dimensions of practice that are contextually relevant, nuanced, safe, and promote rights-based self-determination. Regulatory organizations need to change existing approaches to regulatory requirements that currently rely heavily on rules that govern individual behaviour within Western colonial health systems, to take into account alternate understandings of relationships, collectivity, and worldviews (Silcock et al., 2016).
In this article, we have proposed that it is time to evolve how we conceptualize occupational therapy practice. We have argued that describing occupational therapy as client-centred is no longer adequate for effective practice with individuals, families, groups, communities, and populations. We propose that occupational therapists embrace collaborative relationship-focused practice as a means to attend to the relational aspects of practice including the self, and the individuals, families, groups, communities, and populations who use occupational therapy services within the context of the social and structural factors that promote and constrain occupations. To enact the full extent of relationship-focused practice needs action within and by the institutions that guide and regulate occupational therapy to support therapists to be leaders in practices that promote health, wellness, equity, and justice.
Key Messages
Limitations in conceptualizations of client-centred practice suggest a change to collaborative relationship-focused practice as an expanded descriptor and fundamental shift in occupational therapy practice.
Collaborative relationship-focused practice is contextually relevant, nuanced, and safe, and promotes rights-based self-determination.
This shift is needed to forefront the relational aspects of practice including the self, the individuals, families, groups, communities, and populations who use occupational therapy, and the social and structural factors that promote and constrain occupational participation.