
Abstract
Digital platforms are often characterized as enablers of new ecosystems. However, platforms are sometimes introduced into pre-existing ecosystems, where a platform’s ability to harmonize with the ecosystem is critical for its success. This article draws on the case of digital healthcare platforms and introduces the concept of platform grafting, which denotes the process of integrating a new platform into a pre-existing ecosystem, leading to a coevolutionary process of adapting both the platform and the surrounding ecosystem. Dynamic capabilities are critical for successfully integrating the platform into the ecosystem, and this article provides a capabilities framework for understanding platform grafting.
Keywords
Digital platforms are currently reshaping almost every sector of the economy. These platforms commonly create new ecosystems, connecting different types of users and/or complementary products and services. By leveraging the value created by such connections, successful platform ecosystems have repeatedly managed to compete with and disrupt existing value chains. For example, Uber introduced a platform that connects passengers directly to a new group of drivers, efficiently circumventing the need for conventional taxi companies. 1 Similarly, Airbnb facilitates coordination and transactions between homeowners and short-term tenants, introducing a new type of competition with established hotel chains. Housing stock that was previously isolated from the rental/hotel markets suddenly became accessible in a convenient manner. Much of our current understanding of digital platforms has been shaped by these success stories, where the creation and growth of new ecosystems connecting previously disconnected parties has been central to platform success. In this setting, addressing the so-called chicken-or-egg problem to generate growth of new users and complementors has been identified as one of several challenges. 2
However, some digital platforms are introduced into pre-existing ecosystems, leading to distinct managerial challenges that differ from those associated with the creation of new platform ecosystems. The introduction of a platform within an established ecosystem requires the platform owner to carefully integrate, navigate, and co-evolve across several dimensions of the ecosystem to harness and strengthen complementarities across existing users and components in the ecosystem. This process is significantly different from the establishment of new platform ecosystems.
In this article, we introduce the concept of platform grafting to denote the process of integrating new digital platforms into pre-existing ecosystems that provide necessary and complementary components, activities, products, and/or services, and with pre-existing governance mechanisms that must be navigated. Our aim is to explore the process of platform grafting and to better understand the related challenges and managerial solutions. To accomplish this, we provide an in-depth case study of digital platforms in healthcare, based on rich primary and secondary data.
The platforms we focus on utilize platform business models that digitally match patients and medical professionals, and integrate platform technologies, data analytics, artificial intelligence, telemedicine, 3 and electronic health records 4 to enhance various aspects of healthcare. They are highly dependent on pre-existing ecosystems, since healthcare services are strictly regulated, and digital services cannot fully replace in-person consultation and treatment but must often be complemented with physical care. Thus, digital platforms in healthcare cannot substitute for—but rather need to integrate into—the pre-existing ecosystems, making it a suitable extreme case for studying platform grafting.
The potential benefits of healthcare digitalization are considerable, making it a highly relevant context in its own right. 5 Digital platforms in healthcare can be powered by AI technologies that contribute to increased speed and quality of the offered services. They efficiently connect patients with medical professionals and coordinate access to complementary services. For healthcare providers, digital platforms reduce the need for costly physical facilities; simplify matching and communication between patients, physicians, and nurses; and even out vicissitudes in demand across geographies. For patients, digital platforms may allow convenient access to healthcare without the need to travel to distant care centers and spend hours in waiting rooms with other patients, potentially transmitting contagious diseases.
About the Research
We use an embedded case study approach to explore the process of digital platform grafting. Embedded cases are suitable for studying complex phenomena, where multiple units of analysis are of importance to describe and explain the phenomena. 6 In our case, the introduction of digital healthcare platforms in Sweden is the main unit, and the individual platforms introduced are subunits of analysis, allowing us to compare and contrast strategies across platforms in the same context.
Sweden provides an ideal setting for our purpose: The Swedish Government was a pioneer in allowing medical diagnoses and treatments to be delivered (including e-prescriptions) via digital platforms. Consequently, Sweden has witnessed the early emergence, growth, and success of digital healthcare platforms. Many Swedish digital platforms are among the most well-funded firms in the industry and feature some of the most downloaded e-health apps, the highest number of consultations, and the highest number of users across Europe. 7
Part of the explanation is that the Swedish market was ready to adopt digital health solutions. The Swedish population is one of the most digitally mature in the world, and the digital ambition of the Swedish Government and the Swedish Association of Local Authorities and Regions was high already in the 2010s, with the bold target for Sweden to, by 2025, become: The best in the world at using the opportunities offered by digitalization and eHealth to make it easier for people to achieve good and equal health and welfare, and to develop and strengthen their resources for increased independence and participation in the life of society.
8
This study focuses on the four major digital healthcare platforms in the Swedish market and draws on both primary and secondary data sources. The primary data includes 35 interviews (30-90 minutes each) carried out with the major digital platform firms, established healthcare providers, and Swedish regulators. The secondary data comprises hundreds of articles from the trade press about digital platforms and the regulatory changes in the Swedish healthcare system; dozens of documents and reports from regulators, physical healthcare providers, and digital platform firms; and rich statistical data on all digital primary care consultations, including the types of diseases, patient categories, financial compensations, and professional categories among the digital platforms.
Swedish digital primary care is dominated by four platforms: Kry (with a 41% market share in terms of the number of consultations), Doktor.se (17%), Min Doktor (15%), and Doktor24 (12%). These platforms together provided 85% of the digital consultations conducted in 2020. The Swedish platforms we study are also of international relevance. For example, Kry attracted significant amounts of funding from investors such as Fidelity Management and Research, Index Ventures (e.g., Skype and MySQL), Ontario Teachers’ Pension Plan, CPP Investments, Creandum (e.g., Spotify), and Daniel Ek (CEO and founder of Spotify). The Swedish platforms are also major actors in the European market. As of 2021, Kry was considered the largest digital healthcare provider in Europe, together with the British platform firm Babylon Health, which had the highest cumulative number of consultations in Europe at the time. Both Kry and Babylon Health expanded to the United States (as well as to other non-European countries); but the U.S. market was dominated by the publicly listed platform firm Teladoc Health (Babylon Health filed for chapter 7 bankruptcy on August 9, 2023). Teladoc Health also operates in other markets under the brands Teladoc, Advance Medical, Best Doctors, Livongo, BetterHelp, HealthiestYou, and MédecinDirect.
A Brief Introduction to Platforms
Research on platforms falls into two streams. 9 The first is the economics stream, which focuses on platforms as “markets” (or transactional platforms 10 ) that facilitate exchange. In this perspective, network effects are central, be they same-side (direct) or cross-side (indirect). With network effects, the platform becomes more valuable to users when the number of other users on the same side or on other sides of the platform increases, leading to economies of scale. Consequently, quickly building a user base is central for competitive advantage.
The second stream is the engineering design stream. It focuses on platforms as a collection of common design elements (or innovation platforms 11 ) that can be reused across different products. Economies of scope are central to this perspective, 12 typically enabled by a modular technological architecture. 13
A number of success cases have implicitly shaped the discourse on platforms to date, such as Apple, Facebook, Amazon, eBay, and Airbnb. These platforms enable new use cases and connect different sides of markets that were not previously connected. The platform provides the core of the ecosystem, through which various actors, products, and services connect. 14 Hence, the introduction of such a platform can lead to the emergence of a new ecosystem, which creates value by enabling complementarity. 15 Network effects are central to these platforms, and they substitute and disrupt, rather than complement, previous solutions. 16 This emphasis on network effects for platforms has become central to the economic perspective of platforms, saying that platforms create value by connecting two or more categories of users that would otherwise not have been able to connect. 17 For digital platforms, this connection is created through digital technologies. 18 The emphasis on the creation of new connections has led most previous research to implicitly assume that platforms are predominantly creating new ecosystems around their platforms. 19
Why Healthcare Is Different
To some extent, digital healthcare platforms can be understood and explained by established conceptualizations, vocabulary, and taxonomies. They are primarily transaction platforms, connecting patients with medical professionals; but they also include aspects of innovation platforms to which various complementary services and technologies can be linked. Some healthcare platform firms, such as the 24Health group in Europe, have even organized themselves around these two perspectives by separating the transaction platform business (Doktor24), on which services are provided and exchanged between patients and medical professionals, from the underlying technological innovation platform (Platform24), which develops and supplies a technical platform that is used across different (types of) healthcare providers, including by traditional public primary care organizations.
However, the established view of platforms is also at odds with digital platforms in the healthcare sector, where platforms are introduced into pre-existing ecosystems and where platforms both complement and substitute for parts of the old ecosystems. This integration process is a key challenge, as the Director of Policy at Europe’s largest digital healthcare platform, Kry, explained in an interview with us: “The biggest challenge is finding how these digital platforms can fit into the existing healthcare system as a whole.”
The magnitude of the challenge was recently exemplified by another major digital healthcare platform, namely, the U.K.-based Babylon Health. Synergies were slow to materialize when the firm expanded to the U.S. market, and in the U.K. home market, the platform technology was questioned by other actors in the healthcare ecosystem, all in all leading up to the platform’s subsequent bankruptcy.
There are various reasons why digital platforms in healthcare need to integrate with existing ecosystems rather than create new ones. First, healthcare services are strictly governed by rules and regulations. Thus, new platforms need to adapt and adhere to pre-existing institutions and governance forms. Second, healthcare services have a stable and controlled set of potential users and providers (i.e., patients and medical professionals) compared with, for example, Uber or Airbnb, where one side of the platforms is completely different than for the rival incumbent firms, such as taxi companies and hotel chains. Third, digital platform firms cannot offer all the services that the physical healthcare providers offer. Hence, digital platform firms in healthcare remain dependent on the physical assets and actors.
Many healthcare providers operate in different nations, with different healthcare systems, and such differences may impact opportunities and challenges when introducing healthcare platforms. In Europe, healthcare is generally available for free for the patients (or at a low consultation fee) and it is typically tax-funded by the national governments (a system called “the Beveridge model”). However, some European countries have adopted a mandatory premium-funded insurance model where the governments control the pricing (“the Bismarck model”). This stands in contrast to the United States, which mainly uses a private insurance model, supplemented with access to government-subsidized affordable health insurance for whoever wants to buy it. Affordable care has in turn supplemented publicly provided care through Medicare and Medicaid.
It is important to note, that most nations do not have a single model for providing healthcare services but use a combination or hybrid form of the Beveridge model, the Bismarck model, the private health insurance model, and an out-of-pocket model. In Europe, for example, healthcare has shifted toward more market-based systems. While the specific design of a national healthcare system clearly plays an important role when healthcare platforms enter that specific market, there are still ample opportunities to draw more general conclusions from studying specific markets..
What Is Platform Grafting?
Clearly, the characteristics of a sector like healthcare push new platform entrants to introduce their digital platforms by integrating them into a pre-existing ecosystem of healthcare services, providers, and users. As noted, platform grafting is the process of integrating a new platform into a pre-existing ecosystem, leading to a coevolutionary process of adapting both the platform and the surrounding ecosystem for successful integration and performance.
The concept is borrowed from biology and medicine. In biology, grafting refers to the process of adding one plant to the roots and/or stem of another plant to benefit from their complementary characteristics. In medicine, engraftment is when a body accepts stem cells or bone marrow and new healthy cells start being produced.
Similar to grafting in biology and medicine, platform grafting folds a platform in an existing ecosystem, and the platform both substitutes and complements the existing components of the system—all in all to improve the ecosystem as a whole. Platform grafting is currently common in healthcare, since digital entrants typically do not control all the complementary assets 20 needed to provide healthcare services, and they require the established ecosystem to provide complementary services, such as specialist care. Thus, digital healthcare platforms do not fully substitute for the traditional and physical healthcare ecosystems but rather contribute to their evolution by providing both substitute and complementary products and services. It is clearly different from platform entry that creates a new ecosystem (see Figure 1a).
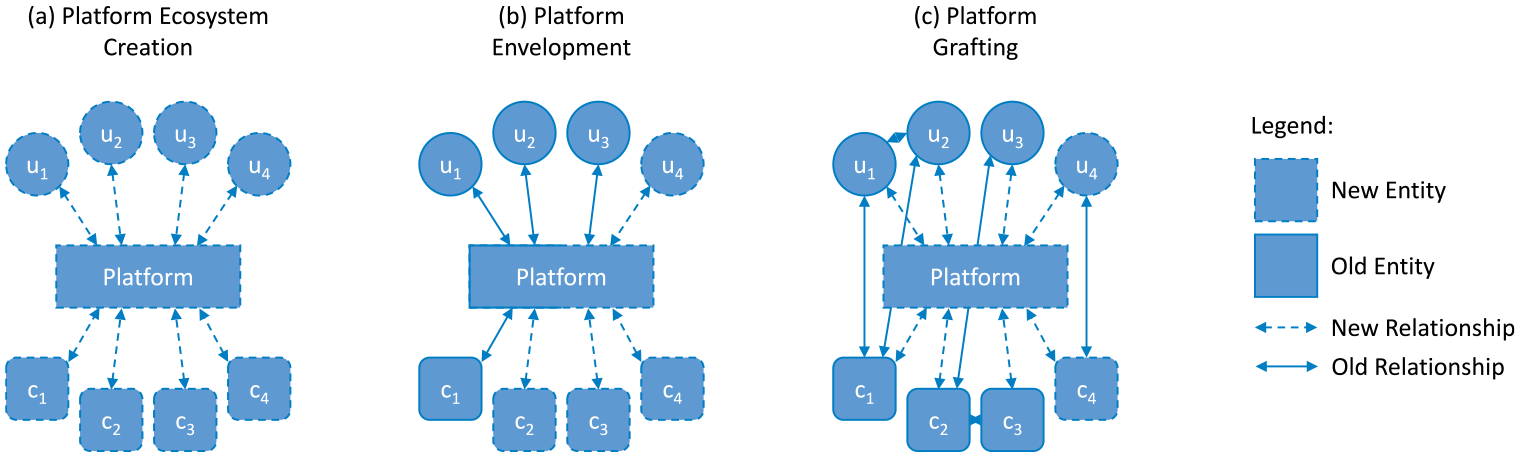
Different types of platform entries with ecosystems of users (u) and complements (c).
Platform grafting has some similarities to what Ozalp and coauthors 21 call digital colonization—that is, when Big Tech firms explore their superior data and data analytics capabilities to provide services to old and regulated industries such as education and healthcare—but platform grafting is limited neither to Big Tech actors nor to data services. Platform grafting also has some similarities to what Eisenmann and coauthors 22 denote as platform envelopment—that is, when a platform leverages its user base and/or complements in one market to successfully enter another market—but platform grafting is different in that the new platforms integrate with established ecosystems, which provide necessary and complementary components, activities, products, and/or services (see Figures 1b and 1c, respectively). Introducing digital platforms and finding viable strategies is particularly challenging in this context of established ecosystems—where ecosystem governance is already established and where new platforms are dependent on old components of the ecosystem, including services, technologies, users, and firms.
Dynamic Capabilities for Platform Grafting
Digital platform firms entering established ecosystems need to address different challenges than those met by platforms creating new ecosystems. Previous research has identified several dimensions of ecosystems, and each dimension may present an integration challenge for a new platform entrant. For example, an ecosystem has been described as “a set of actors with varying degrees of multilateral, nongeneric complementarities that are not fully hierarchically controlled.” 23 Research has also emphasized the tasks or activities that are performed in the ecosystem, 24 and the complementary assets of the system. 25 On top of these actors, tasks, and assets, the governance mechanisms add an institutional layer to the ecosystem. 26 Introducing a platform in such an ecosystem transforms it from a general type of business ecosystem to a platform ecosystem. 27 The platform provides an additional way of coordinating the members, tasks, and assets of the ecosystem, 28 but it may also interfere with pre-existing coordination and governance. This can lead to significant turbulence across the different dimensions of the ecosystem when transforming it into a platform ecosystem in the grafting process. As we will show based on our case of digital healthcare platforms, managing this grafting process for long-term success requires specific capabilities.
Our study shows that to successfully introduce and integrate a platform in a pre-existing ecosystem in the platform grafting process, the platform owner must sense opportunities to improve the ecosystem by means of platform design and technologies. Moreover, such opportunities must be seized by developing a platform offering that is folded in the ecosystem and accepted by various stakeholders, typically requiring technological capabilities, data analytics, and novel process capabilities, on top of an in-depth understanding of the specific sector and market. As the platform and the ecosystem co-evolve, the platform owner must transform and reconfigure its business and the ecosystem for long-term success. For example, managing co-specialization over time, enabling learning effects, and reconfiguring governance to align incentives are all critical activities in transforming the business and the ecosystem. 29
These processes of sensing, seizing, and transforming are the main components of the dynamic capabilities framework. 30 Consequently, platform grafting can be understood through the dual lenses of ecosystem dimensions and dynamic capabilities, together providing a framework for managerial guidance in the platform grafting process (see Figure 2).
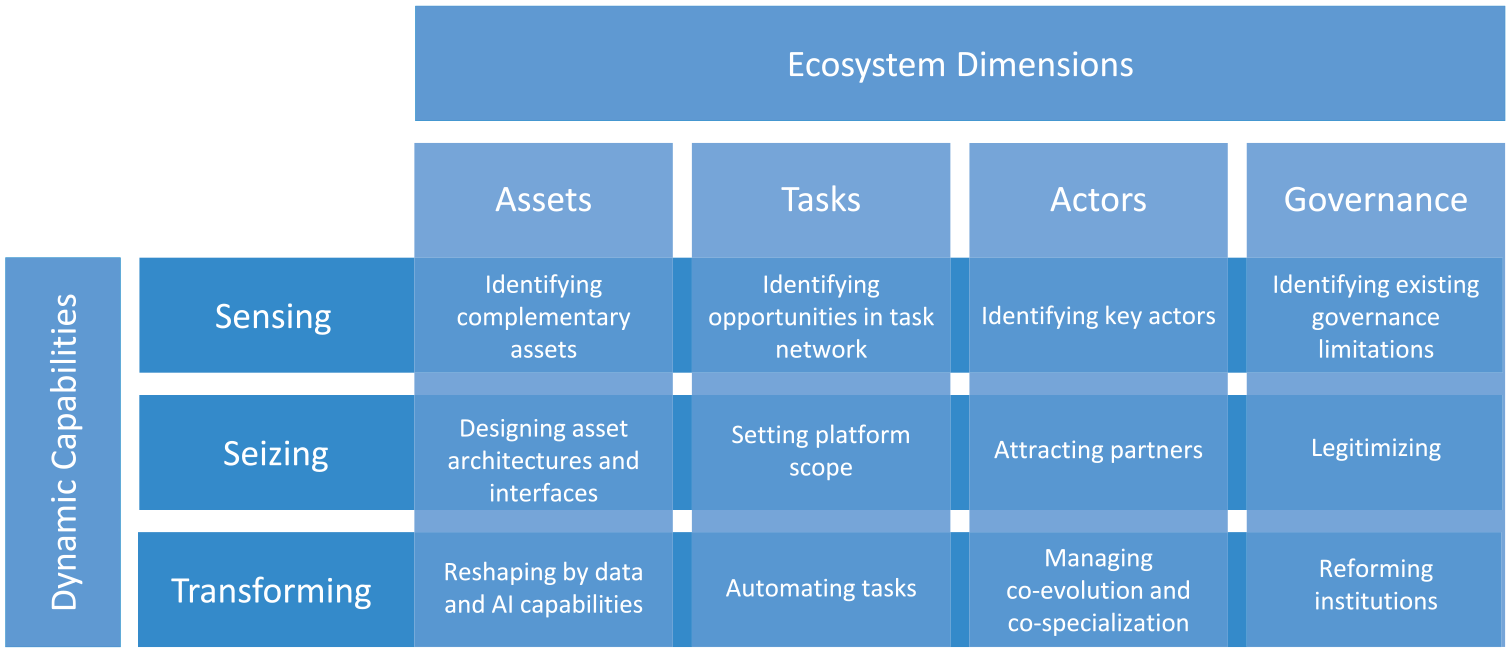
Dynamic capabilities for platform grafting.
Managing Asset Integration
A key challenge in platform grafting is that platform entrants do not control all necessary complementary assets, 31 since their ownership and control are distributed across pre-existing ecosystem actors. Platform entrants must initially identify the central complementary assets, define and design interdependencies and interfaces between the new platform and the pre-existing resources of the ecosystem, and possibly develop and/or acquire some of these assets. The platform technology and business model enable productive use of data and AI capabilities, and over time platform entrants must build such capabilities and ensure they are well-aligned—possibly even co-specialized 32 —with other assets in the ecosystem.
In general, asset integration plays out differently depending on the type of platform that is introduced. For innovation platforms, the integration with pre-existing technical assets and components by means of technology and interface design is critical, while for transaction platforms other types of assets—such as distribution assets—are central, and the means of integration may rather be contractual and organizational.
For digital health entrants, a critical challenge was the interdependence between the new digital platforms and the old, and still necessary, physical healthcare assets. The leading European healthcare platform Kry estimated that they could digitally handle roughly 50% of all typical visits to a physical health center, and they realized that for the remaining ones, they needed to find ways to give their patients access to complementary physical care resources. One solution, adopted by several platforms, was to acquire complementary assets already in the system. Many platforms acquired physical primary care units to be able to provide combined digital and physical healthcare, as exemplified by Kry: With Kry’s [expansion into physical care], our patients can continue to seek care from Kry digitally, whilst also receiving face-to-face care at more physical care centers . . . than we have previously been able to offer. This enables us to treat more symptoms whilst continuing to provide high-quality care that puts patients’ choice first. (Swedish General Manager, Kry
33
)
Another solution was to partner with other types of actors in the ecosystem, such as pharmacies, whose access to well-positioned physical facilities was useful for opening physical care centers. For example, the platforms Doktor24 and Min Doktor opened physical healthcare centers in connection to local pharmacies, where digital visits could be complemented with testing, vaccination, or physical examination. 34
Hence, digital healthcare platforms are integrated into physical healthcare assets to provide a seamless interface in the patient journey across upstream digital and downstream physical care. By controlling both digital platforms and complementary physical assets, platform firms may create value by designing a better customer (patient) journey: We will blur the line between what is digital and physical, instead of dividing it, we will see how different activities can strengthen each other . . . At Min Doktor, we work to ensure that care is provided as needed and at the right level of care, but no one should have to give up needed care because the care staff is not enough. Digital care meetings are suitable for many problems and make both the physician and the care process more efficient, but of course, it is up to each patient to decide for themselves when they want to visit us online and when they want a visit to our health center. (Chief Medical Officer, Min Doktor
35
)
However, scaling an offering based on a combination of physical and digital assets is much more costly and challenging than scaling a purely digital platform. Several platforms had to raise additional capital to fund investments in physical assets. 36 And even then, the physical assets were not available with nearly the same geographic reach as the digital offerings, meaning that the digital platforms and their users remained dependent on the provision of services of incumbent actors controlling complementary assets.
Over time, as platforms grow and profit, they will continue to transform and reconfigure the ecosystem by introducing data and AI capabilities. The introduction of new technologies impacts the evolution of ecosystems. 37 But the implementation of data and AI capabilities is challenging. Recent evidence suggests that challenges persist even among mature actors, and that processes of experimentation, learning, and capability development remain relevant and critical even among the most advanced implementors of AI. 38 In the case of healthcare, some successful platforms, such as Platform24, built and utilized growing datasets to develop automated triage engines, which to some extent replaced the need for human resources in the triage process (i.e., the process of prioritizing and channeling new patients to medical professionals). Such asset development also led the platform to transform its business model so that it was more like a technology provider.
Managing Task Integration
Central to any economic system, including ecosystems, is the range of activities or tasks being performed. 39 When platforms enter an existing ecosystem, the platform replaces other actors in performing certain tasks. Therefore, the platform owner must set the scope of what activities the platform will take on. Initially, this entails the identification of tasks that can be performed better and/or cheaper on the platform, and related tasks that are so tightly interdependent that they need to be integrated within the platform firm, setting the scope of the platform offering. As the platform grows and develops, the task network will continue to be reconfigured by vertical/horizontal integration, automation, and adaptation of certain tasks (e.g., by employing novel data and AI capabilities).
In the healthcare case, we identified two different strategies for the initial integration of the platforms in the task network. The first strategy focused on digitally mimicking parts of the physical task network in order to improve the patient journey. The platforms using this strategy, including Doktor.se and Doktor24, identified a set of tasks that could be better performed on the digital platform than in physical care centers, and they moved such tasks onto the platform. By doing so, the patient journey—and the task network—on the platform remained similar to the physical care center. For example, patients were channeled first to nurses for initial screening and triaging, and only after that to physicians. According to the Head of medical innovation and development at Doktor24 “there was a need . . . for a platform that reflected the usual way of working.” Despite similarities to the physical patient journey, the platforms could enjoy advantages relating to both costs (including fewer physical assets and maintenance) and value (including easier access for patients).
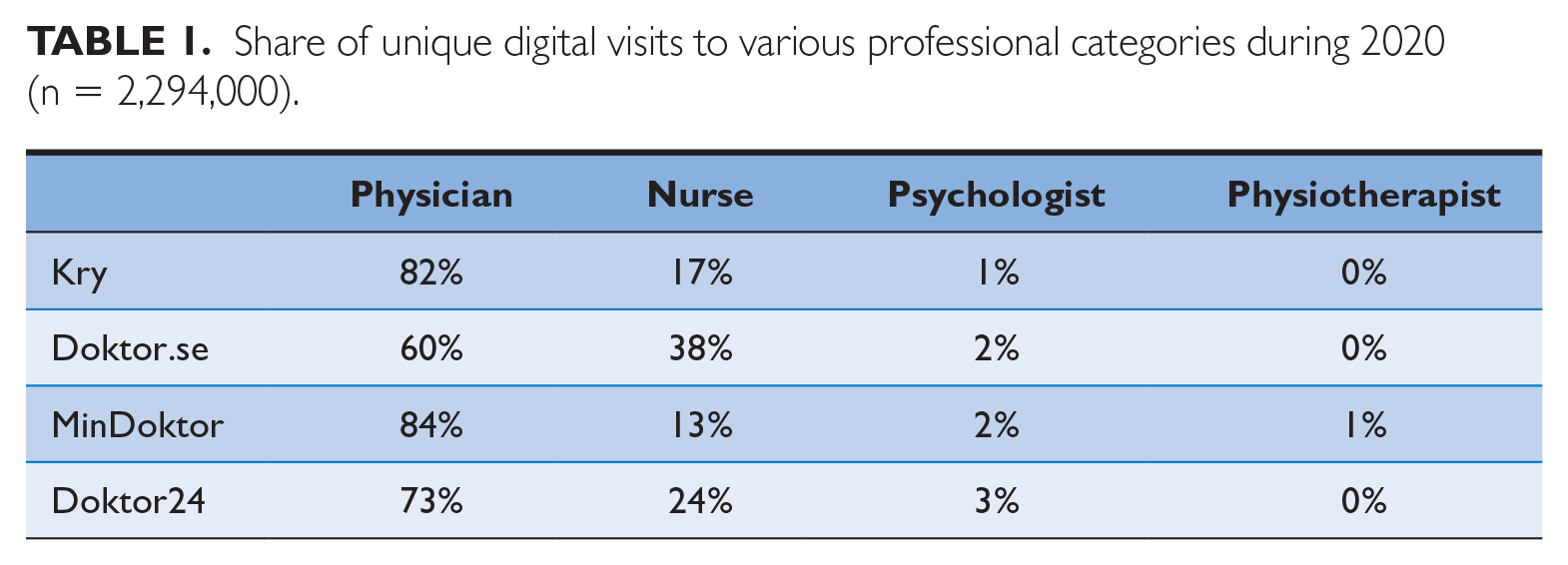
The second strategy focused on utilizing the efficiency of digital platforms to increase the amount of the most value-adding tasks while reducing others, leading to a changed task network from the outset. For example, Kry initially focused on giving patients’ direct access to physicians and eliminated some tasks that had been necessary in a physical patient journey, such as screening meetings with nurses. Consequently, such platforms had high shares of digital visits handled by physicians (see Table 1).
Share of unique digital visits to various professional categories during 2020 (n = 2,294,000).
Over time, digital platforms and healthcare ecosystems were transformed in several ways. First, data and AI capabilities were employed to automate tasks, including triaging, to match patients with the right healthcare professional faster and better. Second, platform scope changed within the same healthcare vertical, by adding specialist care to handle more elements of care, thus broadening platform scope by adding more sides (specialists) to the platform.
40
Platforms also began targeting different patients, specifically attracting patients with chronic diseases, which accounted for approximately 85% of the healthcare expenditure.
41
Third, platform scope changed and expanded to new verticals, including international technology licensing. For example, Doktor.se began monetizing platform technology through the largest Brazilian digital healthcare provider, ViBe, and Belgium’s largest telco, Proximus Group. In several cases, the platform technology was licensed to other types of businesses as well, such as veterinary services. For example, Doktor.se provided its platform technology to the European veterinary giant, Anicura, with over 3 million consultations per year and an annual growth rate of approximately 40% to 50%: As a company, we are extremely driven by digital growth in combination with the fact that we are physical care providers. The opportunity to be able to sell and license something purely digital means an incredible deal to the business model. It is a diversification and a stronger foundation to stand on. (CEO, Doktor.se
42
)
Task integration is difficult, however. Moving some tasks from incumbent actors onto the platform changes the task network in ways that incumbents may oppose (which they did), and in ways that may change the structure of “transaction-free zones.” Transaction-free zones are “spaces where . . . transfers occur freely—undefined, uncounted, and uncompensated,” such as organizations. 43 For example, physical primary care units perform multiple tasks without the need for transacting and compensating between these different tasks, as long as they are performed within the same organization. When digital platforms were introduced, they could only bring some of these tasks to the digital setting. Consequently, the structure of transaction-free zones changed, which generated new transactions (and transaction costs) that were to some degree misaligned with the established compensation system, causing even more opposition among incumbents.
Managing Actor Integration and Partnering
It has already been noted that when a platform enters a pre-existing ecosystem, it needs to integrate into an existing network of actors. These actors include the different types of users that the platform connects. They also include suppliers and providers of complementary assets and services. Successful platform entrants must identify the central actors, enable partnerships, and over time manage coevolution and co-specialization.
In the healthcare case, and more specifically the major actor Kry, the users of the platform were relatively easy to attract initially. Answering the question of whether it was more difficult to get traction on the patient or professional side (cf. chicken-or-egg problem), Kry’s Director of Policy said: Neither. There are, of course, different degrees of digital maturity in different countries. But over the years, at Kry, the problem has not been to make patients like it or make the professionals like it. We have never had a problem attracting professionals to the platform.
Increasing competition from both digital platform entrants and incumbents developing digital offerings eventually made it much more challenging to retain this growth, however. In addition, there were central assets and tasks in the ecosystem that were controlled by other actors, and platform entrants needed to partner with others to access these. However, the physical healthcare providers were reluctant to partner with digital entrants, who were perceived as making easy profits from simple cases (low-cost tasks) while the established physical healthcare providers had to deal with difficult and costly cases.
Instead, many platform entrants partnered with providers of complementary services, namely, pharmacies. Such collaborations aimed at offering patients a seamless digital experience with fast home delivery of medicines, potentially locking in patients to an individual platform. First, a large pharmacy chain, Apoteket Hjärtat, acquired 42% of Min Doktor shares in September 2018. Following this acquisition, the companies’ services were, to some extent, integrated, and the patients could order prescription medicines on the healthcare platform and have them delivered to their home by the pharmacy. In a similar fashion, Doktor24 began collaborating with another pharmacy firm, Apoteket, providing access to the digital platform from the physical pharmacy and focusing on prescription renewal. Subsequently, Apoteket acquired 20% of the shares in Doktor24, leading to even closer integration, with a direct link from the platform to the pharmacy to simplify the ordering of prescribed medicines with home delivery. Doktor.se offered similar integrated services with another large pharmacy, Kronans Apotek, both of which also had the same owner. This cross-ownership received criticism from the Swedish Medical Association due to the risk of increased patient costs and over-prescription of medicines. However, to date, no regulatory limitation has been imposed on such collaborations.
Over time, some platforms also initiated partnerships to enable learning from new markets. Sometimes the learning itself is sufficiently valuable to offer the platform technology to other healthcare providers free of charge. For example, during the COVID-19 pandemic, Kry quickly developed a version of its platform, named Care Connect and Livi Connect, for the European and U.S. markets. While it first was a way to facilitate digital contacts between patients and healthcare providers during the pandemic, it also allowed the company to gain new insights that were useful in its international expansion, which however met other challenges.
Managing Ecosystem Governance
A final key challenge for platforms entering established ecosystems is that governance and coordination mechanisms are already developed and in play, and they may not be well-designed for digital platforms. Therefore, platform entrants must identify niches in the market and ecosystem where they can successfully enter, given the existing governance, and where the mechanisms at play give enough room to create and capture value by means of a digital platform. They must also legitimize the platform 44 and the business model in relation to pre-existing users and actors in the ecosystem, and over time, they need to transform and reconfigure ecosystem governance to enable the full potential of the digital platform.
In the healthcare case, governance integration posed several challenges for platform entrants. First, compensation mechanisms were based on a physical healthcare logic and were not well-designed for digital platforms. The cost efficiency, increased quality of services, and easy access of digital platforms were contrasted with the migration of physicians from physical to digital care, the overconsumption of medical consultations and treatments due to the simplified access, and skewness in terms of easy and higher-margin consultations taking place on digital platforms.
45
While physical healthcare providers were primarily compensated based on the number of listed patients at their units, digital platforms were primarily compensated based on the number of consultations. Therefore, digital platforms were accused of a skewed focus on easy and cheap consultations with high margins, such as cases when patients needed “sick notes” for simple illnesses such as the flu, while patients were referred to physical care units whenever the diagnosis or treatment could not be performed digitally and remotely. Consequently, established actors and regulators pushed for changes leading to drastically decreased compensation rates to digital platforms (by about 75%) and thereby a very different business case for investors. The Swedish Association of Local Authorities and Regions argued that the new compensation rates were appropriate for delivering services on digital platforms: [This] is based on a weighted assessment that takes into account, among other aspects, data on costs, the need for the continued development of new working methods and improved availability, and the need for healthcare offered at the lowest effective level of care.
46
Second, legitimacy issues arose when some platforms increasingly automated specific tasks with AI, such as the triage process. To mitigate this, platforms used and analyzed data to provide evidence of the benefits of their automated processes. For example, Platform24 spent significant efforts countering critique related to its triage engine by providing evidence of its performance.
Third, the pre-existing governance models were not well-aligned regionally and internationally, since traditional healthcare was primarily a local matter, creating significant obstacles for the necessary scaling to profit from heavy investments in digital platforms, as explained by Kry’s Director of Policy: There are scaling challenges in that it is an enormously complex sector with various regulatory obstacles. The primary care system is not built to act on a large scale . . . In Sweden alone, we have 21 regions, and all regions have different regulations. And it is similar in other countries as well . . . In every region, differences exist in administrative regulations . . . There are hundreds of examples of operational variations to relate to. It is very difficult to have a scalable solution in such a fragmented system.
In the United States, Babylon Health had similar experiences, as expressed by Babylon’s senior managing director of commercial strategy and revenue growth: [In the U.S.], healthcare is a very local business in the way that it’s set up. States all have their virtual care and telemedicine laws and regulations that you abide by, and all of that goes along [to make] a very complex environment.
47
Hence, scaling a new platform in a pre-existing ecosystem with fragmented governance mechanisms requires careful consideration on when and how to scale. It may require internal managerial capabilities with local governance know-how in a given ecosystem or local partners with such capabilities. 48 Several European platforms, including Babylon Health, Kry, and Min Doktor, invested heavily in international expansions of their platform-based service offerings, but it turned out to be difficult to profit from these investments.
Instead, some platforms scaled by licensing their platforms to digital healthcare providers internationally, physical healthcare providers nationally, and new verticals, such as veterinary and dental providers, through technology offerings—a type of scaling that is quite different from how non-platform healthcare firms scaled. The main reason for choosing a licensing strategy instead of entering new markets with a service offering was the fragmented regulatory environment. The chief marketing officer at Doctor.se explains: When you want to internationalize, you have to do it in a smart way . . . Either you enter into a platform collaboration, like we did together with ViBe, a company that really understands how healthcare works in that country [the largest Brazilian digital healthcare provider]. Or you need to have a very good understanding of how healthcare is organized [to do it yourself]. Because there are very large differences between countries. It is not like having a streaming app for music, for example, where you can just offer it on the global market and expect it to work in pretty much the same way everywhere . . . In healthcare, you need to have the resources to reach out to users, and you have to make it work with the governments and insurance companies . . . This is not easy, so you have to be very careful before choosing to enter a new national market.
Conclusion
Much research and management advice has covered how digital platforms create and orchestrate new ecosystems. This study has focused on a related but different phenomenon, namely, that of introducing new digital platforms into established ecosystems through platform grafting. We defined platform grafting as the process of integrating a new platform into a pre-existing ecosystem, leading to a coevolutionary process of adapting both the platform and the surrounding ecosystem to achieve successful integration. Ecosystems are multidimensional, and the integration of a new platform in a pre-existing ecosystem creates integration challenges across the different dimensions of the ecosystem, including the interdependent networks of actors, 49 tasks, 50 assets, 51 and governance mechanisms. 52
Our results contrast and expand our extant understanding of platform strategies. We know that strategies aiming at platform ecosystem creation and subsequent ignition focus on building network effects to enable growth and customer lock-in, for example, by solving the so-called chicken-or-egg problem. 53 An effective strategy to address the chicken-or-egg problem is to subsidize one or more sides of the platform. 54 Over time, network effects may create sufficient value for users on all sides of the platform, thereby enabling independent growth. 55 Consequently, subsidies can be turned into profits, at least on one of the sides of a platform. While this is, to some extent, relevant also for strategies aiming at platform grafting, more important are the abilities to adapt, develop, and integrate (graft) platforms and business models to existing entities, thereby enabling a good fit with the ecosystems in which they are embedded. Equally important are the abilities to impact and adapt the ecosystems to achieve congruence between the digital platform and the surrounding complementarities in the ecosystem.
Our framework highlights several challenges and required dynamic capabilities for platform grafting. Platform entrants must sense opportunities by identifying complementary assets, understanding the task network and what tasks to move onto the platform, finding the key actors for integration and partnerships, and exploring the limitations and opportunities in existing governance structures. These opportunities are seized by designing asset architectures and interfaces with relevant complementary assets, setting the scope for tasks on the platform, attracting users and partners, and legitimizing the digital platform in the ecosystem. As platforms mature and grow, they must transform and reconfigure their business models and the ecosystems they are embedded in by reshaping asset structures with data and AI capabilities, automating tasks, managing the coevolution and co-specialization in relation to other actors in the ecosystem, and reforming institutions and governance mechanisms to enable the full potential of digital platforms.
While the concept of platform grafting is new, the phenomenon is not. By introducing the concept into the platform literature, we want to widen the dominant understanding of platform strategy to include the critical challenges of ecosystem integration in addition to ecosystem creation. Managers who focus mainly on how to nurture and benefit from network effects otherwise risk being blindsided by important integration challenges. We studied the case of healthcare—with tight regulations, a defined set of users, and a critical physical asset network—but the integration challenges in platform grafting are relevant also in less regulated cases. In fact, most platform introductions can be characterized as a combination of pure ecosystem creation and platform grafting.
For example, consider the case of Spotify. Spotify introduced a music streaming platform that eventually disrupted the established music distribution industry. One of the most critical challenges for Spotify was to integrate into the actor network in the pre-existing music ecosystem, to get access to the music catalogs of various artists. 56 Another example, showcasing aspects of platform grafting, is console gaming. In every generation shift, console makers such as Microsoft and Sony need to reintegrate into the established ecosystems of the preceding console generation. 57 Hence, backwards compatibility is a way to integrate in the asset network of a pre-existing ecosystem. Yet another example is provided by digital security firm Yubico, which is critically dependent on the established and changing governance structures in the digital security ecosystem. The firm has described how it has managed to “integrate in the broader identity ecosystem,” and how that provides a competitive advantage, but also that the firm is at risk in case of governance changes in the ecosystem. 58
Beyond the managerial implications, our results also have implications for theory. Most importantly, our findings contribute to our understanding of the microfoundations of dynamic capabilities. 59 Previous research has identified microfoundations both on the level of cognitive abilities of individuals and on firm-level capabilities, 60 and here we primarily contribute to the latter by providing a framework of capabilities and specifying managerial activities of relevance for the long-term success of platform entrants. 61
Business historian Alfred Chandler noticed that in major technological transitions, firms and markets co-evolve, 62 and this is certainly the case when digital platforms are introduced into established ecosystems. The platform firms in our study adapted to frequent regulatory changes, and also worked to influence policy, in a form of “regulatory co-creation.” 63 In such a changing regulatory and competitive context, building strong dynamic capabilities is essential. 64 The successful digital platform firms that we observed sensed and seized new opportunities and challenges across the ecosystem, and over time reconfigured and transformed their businesses and the ecosystems they entered. 65 Successful platforms must be proactive and adaptive. 66 Innovation is just as important as optimization for a platform to become and remain successful. 67 In other words, dynamic capabilities are key to success where platform grafting is necessary. Platform firms must be able to anticipate changes, achieve business model adjustments, and effectuate the alignment of complementarities. 68 While economies of scale and scope were relevant driving factors, platform grafting is a more complex process, involving internationalization, diversification, and technology contracting, as illustrated by this case study.
Footnotes
Acknowledgements
Authors in alphabetical order. We thank three anonymous reviewers, Rabih Darwish, Malin Petrén, and the CMR editors for outstanding feedback and constructive comments on prior drafts. Any errors remain ours alone.
Funding
The author(s) disclosed receipt of the following financial support for the research,authorship, and/or publication of this article: Joakim Björkdahl and Marcus Holgersson acknowledge the support of Vinnova (Grant No. 2022-00292).
Notes
Author Biographies
Joakim Björkdahl is Professor of Strategic Management and Innovation at Chalmers University of Technology, Sweden (email:
Marcus Holgersson is Professor of Industrial Management and Economics at Chalmers University of Technology, Sweden (email:
David J. Teece is Professor of the Graduate School, UC Berkeley, and Executive Chairman of the Berkeley Research Group (email: